Abstract
Background
The importance of incorporating quality-of-life (QoL) assessments into medical practice is growing as health care practice shifts from a “disease-based” to a “patient-centered” model. The prevalence of age-related macular degeneration (AMD) is increasing in today’s aging population. The purpose of this paper is: (1) to discuss, by reviewing the current literature, the impact of AMD on patients’ QoL and the utility of QoL assessments in evaluating the impact of AMD and its treatment; and (2) to make a recommendation for incorporating QoL into clinical practice.
Methods
We conducted a PubMed and an open Internet search to identify publications on the measurement of QoL in AMD, as well as the impact of AMD and the effect of treatment on QoL. A total of 28 articles were selected.
Results
AMD has been found to cause a severity-dependent decrement in QoL that is comparable to systemic diseases such as cancer, ischemic heart disease, and stroke. QoL impairment manifests as greater social dependence, difficulty with daily living, higher rates of clinical depression, increased risk of falls, premature admission to nursing homes, and suicide. The National Eye Institute Visual Functioning Questionnaire (NEI VFQ-25) is the most widely used eye disease-specific QoL instrument in AMD. It has been shown to correlate significantly with visual acuity (VA). QoL reflects aspects of AMD including psychological well-being, functional capacity, and the ability to perform patients’ valued activities, which are not captured by a single, numerical VA score.
Conclusion
The literature shows that the adverse impact of AMD on QoL is comparable to serious systemic disease. Eye disease-specific instruments for measuring QoL, such as the NEI VFQ-25, have shown a significant correlation of QoL decrement with measures of disease severity, as well as significant QoL improvement with treatment. The NEI VFQ-25 and other validated instruments provide a wide-ranging assessment of vision-related functioning that is important to patients and complementary to VA measurement. We strongly recommend the incorporation of QoL assessment into routine clinical practice.
Background
Age-related macular degeneration and associated burden of illness
Age-related macular degeneration (AMD) is a chronic, progressive eye disorder that mainly affects people over the age of 50.Citation1 Clinically, there are two types of AMD. Atrophic or “dry” AMD, also known as geographic atrophy, is characterized by fatty deposits behind the retina (drusen), causing thinning and drying of the macula. Dry AMD accounts for about 80% of cases affecting both eyes, but it typically causes only mild loss of vision.Citation1 Neovascular AMD, or “wet” AMD (wAMD), is caused by growth of new blood vessels (choroidal neovascularization). The relative proportions of wAMD and dry AMD cases are dependent on the way they are defined. For example, findings from the Hisayama prospective cohort study in Japan revealed a higher wAMD prevalence, which was threefold (0.67%) that of dry AMD (0.2%).Citation2 Moreover, wAMD is associated with rapidly deteriorating vision and accounts for 90% of cases of severe visual impairment due to AMD.Citation3
In the US, the estimated prevalence of AMD (neovascular and/or geographic atrophy) is 1.47%, affecting approximately 1.75 million individuals.Citation4 The burden of illness of wAMD due to lost wages alone is about $5.4 billion. Other costs, such as those associated with caregiving, injury and provision of other services, drive the economic burden even higher.Citation5,Citation6 In Japan, which has the oldest and longest living population in the world, 1.64 million people are affected by visual impairment, of whom 61% are older than 65 years. Notably, early AMD is highly prevalent (12.7%) in those 50 years and older in the Japanese population, whereas late AMD is less prevalent (0.87%).Citation2 More recently, follow-up from the ongoing Hisayama study showed a 9-year cumulative incidence of 10% for early AMD and 1.4% for late AMD.Citation7 Overall, the economic burden of visual impairment in Japan is substantial, costing about 8785 billion Yen (US $72.8 billion), or 1.7% of gross domestic product.Citation8 Given the high prevalence of early AMD among the elderly Japanese population, it is likely that a significant proportion of this economic burden is due to AMD. In Asia, AMD is a major cause of blindness among the elderly. A high prevalence of AMD has also been documented in Singapore (27% in those over 60 years of age) and Taiwan (9.2% and 1.9% for early and late AMD, respectively, in those 65 years and older).Citation9,Citation10
The importance of quality of life assessment in wAMD
With progressive deterioration of the macula, AMD patients experience a multitude of visual problems that significantly affect their mental health and quality of life (QoL). In this context, it is notable that the World Health Organization constitution describes health as a state of physical, mental, and social well-being, not merely the absence of disease or infirmity. Consequently, the measurement of health should encompass an assessment of mental and social well-being, which can be accomplished by using QoL measures.Citation11 Moreover, as health care continues to evolve from a “disease-based” to a “patient-centered” model, the importance of evaluating the outcomes of health care from the patient perspective is now widely recognized. Thus, in addition to clinical measures, a number of instruments measure patient-reported outcomes that assess patients’ QoL, functional status, and their experiences with care.
“QoL is an individual’s perception of position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.”
From the WHO “Measuring Quality of Life”Citation11
Given the growing importance of incorporating QoL assessments into medical practice in general, and given the increasing prevalence of AMD in today’s aging population and the heavy burden of this disease, it is critical to understand the impact of AMD on QoL and to improve the measurement of QoL in the context of routine ophthalmologic practice. The purpose of this paper is to provide a summary of the available evidence on the impact of AMD on patients’ QoL and the utility of QoL assessments in evaluating the impact of AMD and its treatment, and to make a recommendation for incorporating QoL assessment into clinical practice.
Methods
We conducted an open Internet search and a PubMed search to identify articles (full text only) relating to the effects of wAMD on QoL. The following search criteria were used for the PubMed search: (1) English language, (2) peer reviewed journals, (3) articles published between 2000 and 2012. Search terms included “age-related macular degeneration,” “wet AMD,” “neovascular AMD,” “burden of illness,” “cost,” “cost effectiveness,” “prevalence,” “blindness,” “quality of life,” “health-related quality of life,” “patient-reported outcome,” “questionnaire,” “visual impairment,” “activities of daily living,” and “functional assessment.”
A similar range of search terms was used in the open Internet search to identify other sources of information on vision-related QoL measures, QoL-specific treatment outcomes, guidelines concerning the role of QoL assessment in the clinical care of patients with AMD, and the impact of AMD on QoL. The primary targets of this search were websites representing professional societies and international health care organizations concerned with QoL and wAMD.
Literature from the PubMed and open Internet searches were reviewed and salient information was extracted.
Results
Clinical measurement of AMD severity
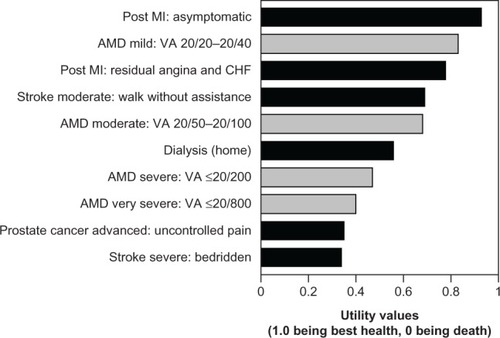
In clinical practice, the severity of AMD can be categorized based on Snellen visual acuity (VA) testing of the better-seeing eye: mild (20/20–20/40), moderate (20/50–20/100), severe (20/200 or worse), very severe (20/800 or worse) ().Citation6 Clinical practice in Japan uses the decimal-point equivalent of the VA. Traditionally, it has been the practice to treat patients with late-stage wAMD in clinical settings. However, with the availability of better diagnosis and effective treatment options, patients are evaluated earlier and those with AMD or even pre-AMD symptoms may receive treatment. Severity of AMD alone is no longer a sufficient criterion for treatment decision making. The impact of the disease on the patient’s QoL is also an important factor. For example, while severe or very severe disease in one eye is an established criterion for treatment, patients with disease in both eyes may be treated regardless of VA to maintain vision-related QoL.
Table 1 Impact of wAMD on QoL, treatment, and goals based on clinical assessments of wAMD severity
Impact of AMD on QoL
Given its increasing importance in clinical treatment of wAMD, it is critical to gauge the magnitude of QoL decrement in wAMD. It has been documented that compared to individuals without AMD and with vision within the normal range, those who are visually impaired experience significantly reduced QoL, which manifests as greater social dependence, difficulty with daily living, higher rates of clinical depression, increased risk of falls, premature admission to nursing homes, and suicide.Citation3 The poor QoL associated with AMD is greatly underestimated by clinicians and the general public.Citation12 AMD patients suffer from a multitude of visual problems including reduced central VA, impaired color vision, decreased contrast sensitivity, and metamorphosia.Citation1 Although peripheral vision is usually retained in AMD, the losses in these multiple parameters of vision can impair proficiency in performing most activities of daily living and can make it more difficult for people to lead independent lives.Citation3 Central vision, in particular, is needed for activities such as reading, driving, and facial recognition. Even in early AMD there is blurring and distortion of central vision, which decreases functional capacity for these activities.Citation12 It is the progressive deterioration of central vision that profoundly impacts disease-specific QoL.
Patients in the earliest stages of AMD experience distorted vision, which has a minimal impact on their QoL (). Patients with moderately severe disease in one eye often experience difficulty reading small print but retain fairly normal distance vision, thereby reducing the overall effect on QoL. On the other hand, those with both eyes affected experience a major reduction in QoL due to poor facial recognition, difficulty writing or reading small print, and compromised ability to perform activities of daily living.Citation1,Citation3,Citation6 Patients with advanced or late-stage AMD experience very poor QoL due to severely affected central vision and reduced VA (). These patients may have difficulty distinguishing between certain colors. Thus, AMD has been found to cause a severity-dependent decrement in QoL ranging from 17% to 63%, which is comparable to systemic diseases such as cancer, ischemic heart disease, and stroke ().Citation6 The impact of QoL is also an important part of patient management, enhancing the clinical assessment based on improvement or stabilization of VA. summarizes the treatment goals for AMD, in conjunction with the corresponding clinical assessments and QoL impact by disease severity.
Figure 1 Impact of AMD on QoL as presented by utility values corresponding to VA in the better seeing eye, compared with utility values for other disease states.
Abbreviations: AMD, age-related macular degeneration; QoL, quality of life; VA, visual acuity; Mi, myocardial infarction; CHF, congestive heart failure.
Value of QoL measures in patient assessments and current use in wAMD clinical research
Change in VA is the standard measure in clinical practice as well as in trial settings for evaluating treatment response in AMD. However, VA or other measures of disease severity (eg, optical coherence tomography) alone do not take into account the impact of all aspects of the disease, including such manifestations as central dark spots, vision-related functioning, the capacity to engage in valued activities, or the psychological effect of changes in these parameters (ie, the patient’s actual QoL).Citation13–Citation15 From the patient’s perspective, improvement in psychological well-being and the ability to perform activities of daily living that are dependent on visual function may be as, or more, important than the clinical assessment of VA itself.Citation13,Citation15 The importance of recognizing disease-specific QoL in AMD is manifold. First, it justifies the need to prevent disease progression with therapeutic interventions. Second, it provides a means of measuring the impact of treatment on what matters most – patients’ ability to function and enjoy life. Third, it encourages the development of low-vision aids and other devices to help patients with activities of daily living by providing a means of quantifying the benefits, in terms of improved functional capacity, of interventions that do not alter unaided VA.Citation12
Although VA and QoL are clearly correlated, the latter is what matters most to the patient and is the ultimate measure of the need for, and success of, treatment.Citation16 Fortunately, there are a number of disease-specific QoL instruments that have been validated in the wAMD population that can be used to directly measure their QoL. The National Eye Institute Visual Functioning questionnaire (NEI VFQ-25), the Daily Living Tasks Dependent on Vision questionnaire (DLTV), the Activities of Daily Vision Scale, and the Visual Function Index are prominent examples of vision-specific QoL questionnaires designed to assess respondents’ health status, functional status, visual function, and well-being.Citation3
The NEI VFQ-25, a 25-item questionnaire, is one of the most widely used of these instruments ().Citation17 Several of the subscales of this instrument have been used as prespecified endpoints in clinical trials: near vision (items 5–7), distance vision (items 8, 9, 14), dependency (items 20, 23, 24), and mental health (items 3, 21, 22, 25). In a noninterventional study of wAMD patients, Orr et alCitation18 used the NEI VFQ-25 total composite score and subscale scores for near activity, distance activity, and vision-specific dependency to correlate with clinical assessment (best corrected VA) and to associate with patient-reported outcomes (restricted activity days), a measure of QoL. Their results showed that the NEI VFQ-25 composite and subscale scores were significantly correlated with best corrected VA of the better-seeing eye (r = −0.48 to −0.54; all P < 0.0001) and with restricted activity days (r = −0.52 to −0.55; all P < 0.0001). Patients with fewer restricted activity days over a 3-month period had a significantly higher NEI VFQ-25 score (eg, patients with 0–1 days of restricted activity had a mean NEI VFQ-25 total composite score of 79.8 compared with a score of 43.5 for those with >9 restricted activity days [P < 0.001]). Subscale scores showed similar results to total composite scores (). In the Age-Related Eye Disease Study,Citation19 NEI VFQ-25 was administered to AMD patients twice within a 1- to 4-year interval to assess the impact of disease progression and loss of VA on health-related QoL. The NEI VFQ-25 composite score was significantly responsive to disease progression (t = 14; P < 0.001) and to loss of VA (t = 16; P < 0.001).Citation20 Subscale scores – including near activities, distance activities, dependency, and mental health scores – were also significantly responsive, though the effect sizes were smaller than those for the overall score. These studies demonstrate that the NEI VFQ-25 is a valid measure of vision-related QoL in AMD.
Figure 2 NEI VFQ-25 composite and subscale scores by number of patient-reported restricted activity days due to AMD over a 3-month period.
Abbreviations: NEI VFQ-25, National Eye institute visual Functioning Questionnaire 25-items; AMD, age-related macular degeneration.
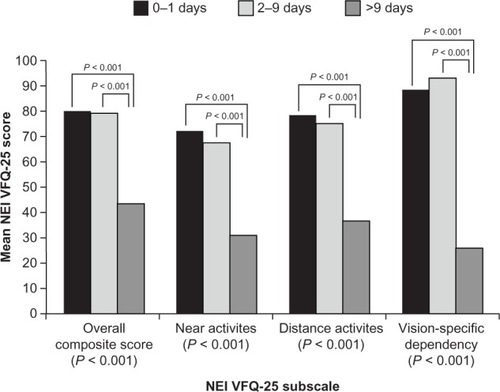
Table 2 Item analysis of NEI VFQ-25
Another example of a vision-specific instrument is DLTV, a 24-item questionnaire that assesses tasks dependent on distance and near vision, depth and contrast perception, light and dark adaptation, and visual fields.Citation22 The construct validity of this instrument was demonstrated by showing a statistically significant correlation of the DLTV total and domain scores while using, versus not using, regular help from caregiving (P < 0.0001).Citation23 For example, patients receiving regular help from caregiving had a mean DLTV total score of 49.8 ± 20.4, while those not requiring regular help had a score of 79.0 ± 18.1 (P < 0.0001).
Although vision-specific instruments provide disease-specific QoL information, generic QoL instruments (ie, do not target a specific age, disease, or treatment group) such as the Short Form-12 or Short Form-36, have also been used to assess QoL in patients with AMD. These instruments provide functional health and well-being scores and a preference-based health utility index, as well as psychometrically based physical and mental health summary measures.Citation24 However, general QoL instruments have been shown only to clearly differentiate between different ophthalmic disease states, but not to be responsive to disease progression or changes in VA in wAMD.Citation24
Most clinical studies depend on quantitative outcome measures, but the value of therapy to the patient and caregiver depends more directly on improvement in QoL. Pharmacotherapy with pegaptanib, ranibizumab, and intravitreal aflibercept have all demonstrated significant improvements in QoL composite score on the NEI VFQ-25, indicating overall improvement in the respondent’s visual health and related functional capacities.Citation13,Citation14,Citation25,Citation26 Other benefits, such as a reduction in the incidence of depression or a decrease in injuries due to falls (a major hazard of vision loss), may also be reflected in improved QoL scores.Citation3,Citation12 More specifically, a reduction in dependency is manifested as improvements in daily activities such as reading, cooking, identifying objects on a crowded shelf, watching television, shopping, doing hobbies such as sewing and fixing things, and being able to walk across streets without assistance ().Citation13,Citation14,Citation25,Citation26 Additionally, improvements in QoL composite score were documented, indicating overall improvement in the respondents’ mental and physical health and reduction in injuries due to falls, a major hazard of vision loss.
Table 3 QoL assessment in clinical trials of antivascular endothelial growth factor therapy for wAMD
Discussion
The literature on QoL in AMD, as briefly reviewed here, has established that the impact of wAMD on QoL is severity-dependent and quantitatively similar to that for other major diseases of the elderly. Second, there are several vision-specific instruments for measuring QoL that have been proven for reliability and validity, and which are superior to general health-related QoL instruments in this population. Third, vision-specific QoL instruments, such as the NEI VFQ-25, have been shown to be sensitive to disease progression, as measured by the worsening of VA. Most recently, and of great clinical importance, clinical trials of antivascular endothelial growth factor treatments of wAMD using the NEI VFQ-25 have demonstrated substantial improvements in QoL that parallel the improvement in VA.
Despite the demonstrated vision-related QoL benefits of treatment observed in research settings and the recurrent recognition by clinical researchers that these benefits are the most meaningful to patients, the measurement of vision-related QoL is quite limited in real-world clinical practice. Integrating the assessment of QoL into clinical practice may increase patients’ motivation to adhere to treatment by providing them with objective feedback on the real-life improvements they have attained. It would also provide the clinician with an additional common language for discussing treatment progress with the patient. In addition, routine QoL assessment will generate outcome data that may help demonstrate the cost effectiveness of this expensive treatment to key stakeholders, including physicians, payers, and regulatory agencies.
Perhaps the major barrier to the implementation of a QoL assessment is insufficient time on the part of the attending ophthalmologist to administer the instrument routinely during clinic visits. For example, in our experience, the interviewer-administered version has typically taken approximately 10 to 15 minutes to complete per patient. Some of the difficulty in accomplishing the task more efficiently is due to patient factors, such as poor VA and/or cognitive impairment. Of equal importance, however, is the extensiveness of the instruments themselves, which were designed primarily for research purposes. With respect to the NEI VFQ-25, for example, it is inevitably time consuming to administer a 25-item questionnaire.
Based on the literature reviewed here, it is clear that some NEI VFQ-25 subscales and their corresponding items have a greater impact on vision-related QoL assessment in AMD patients than others. In recognizing the busy schedules of clinicians, whose primary focus is to assess changes in VA, we recommend that the original NEI VFQ-25 be shortened to include only those items that are most relevant to assessing QoL in wAMD patients in the clinical setting. By shortening the administration time and also making scoring and interpretation easier, an abridged version of the NEI VFQ-25 would be more readily adopted by practicing clinicians. However, further research evaluating the reliability and validity of such an instrument would be required.
Another barrier to adopting a QoL assessment may be that clinicians are not aware that some of the instruments described above have been validated in many regions of the world.Citation17 With regard to eye disease-specific QoL instruments, the NEI VFQ-25 has been psychometrically validated in many languages with minor amendments made to the original instrument in order to accommodate wider usage.Citation15,Citation27,Citation28 For example, there is a Japanese version of the NEI VFQ-25 that was modified to substitute items in the near and distance vision subscales with those that are more relevant to Japanese patients.Citation15 Such amendments minimize missing or inaccurate data and thereby increase measurement precision.
Adoption of a QoL assessment in clinical practice might increase if it were recommended in clinical guidelines for the evaluation and management of wAMD. For example, QoL assessment using a validated questionnaire is specifically discussed and recommended in the Japanese guidelines for allergic rhinitis.Citation29 Treatment for allergic rhinitis is aimed at alleviating symptoms and eliminating difficulties experienced in everyday life, hence resulting in an improvement in QoL. Improvement in QoL was included in the guidelines because allergic rhinitis is manageable when treated, although it resists cure.Citation30
Conclusion
wAMD accounts for 90% of cases of severe visual impairment due to AMD, and epidemiological data clearly show that this form of visual impairment typically causes a significant reduction in QoL and substantial societal burden. Decrements in QoL associated with wAMD can be easily and accurately measured, and research has clearly demonstrated the value of QoL assessment for understanding the natural history of wAMD and its response to treatment. QoL measures additional aspects of the disease, such as the psychological well-being and daily functioning of patients, that cannot be captured by a single clinical measurement of disease severity. However, despite their widespread use in epidemiologic research and clinical trial settings, eye disease-specific QoL measures are seldom used in routine clinical assessment of AMD patients, in part because of barriers to implementation. The present review indicates that efforts to overcome these barriers are warranted. The authors recommend the development of a validated shortened version of the NEI VFQ-25, tailored specifically to wAMD, for use in QoL assessment in the routine clinical care of wAMD patients.
Acknowledgments
The authors wish to acknowledge the contribution of Kim Ullerup Wittrup-Jensen, Kenji Adachi, and Keigo Kudo of Bayer for their insightful comments during the manuscript preparation and discussion. Medical writing assistance was provided by Bagi Ravishankar, PhD, and Bill Kadish, MD, of PAREXEL, and was funded by Bayer HealthCare, LLC.
All authors contributed important intellectual content, including discussions on the manuscript concept and outline, interpretation of the literature review results, clinical insights, and critical revision of all drafts of the manuscript. All authors approved the final draft for submission and take full responsibility for the contents of this article.
Disclosure
MY and KF have received fees for consulting from Bayer Yakuhin, Ltd. ET and EW are salaried employees of Bayer Yakuhin, Ltd. The authors report no other conflicts of interest in this work.
References
- JagerRDMielerWFMillerJWAge-related macular degenerationN Engl J Med2008358242606261718550876
- OshimaYIshibashiTMurataTTaharaYKiyoharaYKubotaTPrevalence of age related maculopathy in a representative Japanese population: the Hisayama studyBr J Ophthalmol200185101153115711567955
- MitchellJBradleyCQuality of life in age-related macular degeneration: a review of the literatureHealth Qual Life Outcomes200649717184527
- FriedmanDSO’ColmainBJMuñozBEye Disease Prevalence Research GroupPrevalence of age-related macular degeneration in the United StatesArch Ophthalmol2004122456457215078675
- AMD Alliance InternationalThe Global Economic Cost of Visual Impairment: Summary Report2010 Available from: http://www.amdalliance.org/amdalliance/AMDAlliance/cost-of-blindnessAccessed May 20, 2013
- BrownGCBrownMMSharmaSThe burden of age-related macular degeneration: a value-based medicine analysisTrans Am Ophthalmol Soc2005103173184 discussion 184–18617057801
- YasudaMKiyoharaYHataYNine-year incidence and risk factors for age-related macular degeneration in a defined Japanese population the Hisayama studyOphthalmology2009116112135214019744734
- RobertsCBHiratsukaYYamadaMEconomic cost of visual impairment in JapanArch Ophthalmol2010128676677120547955
- WooJHAu EongKGDon’t lose sight of age-related macular degeneration: the need for increased awareness in SingaporeSingapore Med J2008491185085319037547
- ChenSJChengCYPengKLPrevalence and associated risk factors of age-related macular degeneration in an elderly Chinese population in Taiwan: the Shihpai Eye StudyInvest Ophthalmol Vis Sci20084973126313318390643
- World Health OrganizationWHOQOL: Measuring quality of life1997 Available from: http://www.who.int/mental_health/media/68.pdfAccessed May 20, 2013
- SteinJDBrownMMBrownGCHollandsHSharmaSQuality of life with macular degeneration: perceptions of patients, clinicians, and community membersBr J Ophthalmol200387181212488253
- BresslerNMChangTSFineJTDolanCMWardJAnti-VEGF Antibody for the Treatment of Predominantly Classic Choroidal Neovascularization in Age-Related Macular Degeneration (ANCHOR) Research GroupImproved vision-related function after ranibizumab vs photodynamic therapy: a randomized clinical trialArch Ophthalmol20091271132119139332
- ChangTSBresslerNMFineJTImproved vision-related function after ranibizumab treatment of neovascular age-related macular degeneration: results of a randomized clinical trialArch Ophthalmol2007125111460146917998507
- SuzukamoYOshikaTYuzawaMPsychometric properties of the 25-item National Eye Institute Visual Function Questionnaire (NEI VFQ-25), Japanese versionHealth Qual Life Outcomes200536516248900
- MiskalaPHBassEBBresslerNMSubmacular Surgery Trials (SST) Research GroupSurgery for subfoveal choroidal neovascularization in age-related macular degeneration: quality-of-life findings: SST report no 12Ophthalmology2004111111981199215522363
- MarellaMPesudovsKKeeffeJEO’ConnorPMReesGLamoureuxELThe psychometric validity of the NEI VFQ-25 for use in a low-vision populationInvest Ophthalmol Vis Sci20105162878288420089878
- OrrPRentzAMMargolisMKValidation of the National Eye Institute Visual Function Questionnaire-25 (NEI VFQ-25) in age-related macular degenerationInvest Ophthalmol Vis Sci20115263354335921282568
- Age-Related Eye Disease Study Research GroupThe Age-Related Eye Disease Study (AREDS): design implications. AREDS report no 1Control Clin Trials199920657360010588299
- LindbladASClemonsTEResponsiveness of the National Eye Institute Visual Function Questionnaire to progression to advanced age-related macular degeneration, vision loss, and lens opacity: AREDS Report no 14Arch Ophthalmol200512391207121416157800
- SuñerIJKokameGTYuEWardJDolanCBresslerNMResponsiveness of NEI VFQ-25 to changes in visual acuity in neovas-cular AMD: validation studies from two phase 3 clinical trialsInvest Ophthalmol Vis Sci20095083629363519255158
- McClureMEHartPMJacksonAJStevensonMRChakravarthyUMacular degeneration: do conventional measurements of impaired visual function equate with visual disability?Br J Ophthalmol200084324425010684832
- SchmierJKHalpernMTCovertDValidation of the Daily Living Tasks Dependent on Vision (DLTV) questionnaire in a U S population with age-related macular degenerationOphthalmic Epidemiol200613213714316581618
- GlobeDRLevinSChangTSMackenziePJAzenSValidity of the SF-12 quality of life instrument in patients with retinal diseasesOphthalmology2002109101793179812359596
- HeierJSBrownDMChongVVIEW 1 and VIEW 2 Study GroupsIntravitreal aflibercept (VEGF trap-eye) in wet age-related macular degenerationOphthalmology2012119122537254823084240
- LeysAZlatevaGShahSNPatelMQuality of life in patients with age-related macular degeneration: results from the VISION studyEye (Lond)200822679279817585313
- ChanCWWongDLamCLMcGheeSLaiWWDevelopment of a Chinese version of the National Eye Institute Visual Function Questionnaire (CHI-VFQ-25) as a tool to study patients with eye diseases in Hong KongBr J Ophthalmol200993111431143619515645
- LabirisGKatsanosAFanariotisMPsychometric properties of the Greek version of the NEI-VFQ 25BMC Ophthalmol20088418325083
- OkudaMOhkuboKGotoMComparative study of two Japanese rhinoconjunctivitis quality-of-life questionnairesActa Otolaryngol2005125773674416012036
- OkuboKKuronoYFujiedaSJapanese Society of AllergologyJapanese guideline for allergic rhinitisAllergol Int201160217118921636965