
Abstract
Purpose
This study assessed the incidence of postsurgical intraocular inflammation after cataract extraction by phacoemulsification and implantation with AcrySof IQ ReSTOR intraocular lenses (IOLs) produced using an updated manufacturing process. Incidence rates were compared with historical rates of postsurgical intraocular inflammation.
Methods
This was a prospective, multicenter, post-approval study at 34 sites. Patients aged ≥22 years received a study lens in at least 1 eye. Postsurgical intraocular inflammation (aqueous cell grade ≥3+ within 14 days after surgery, aqueous cell ≥2+ at 14 to ≤60 days after surgery, or aqueous cell ≥1+ at >60 days) was assessed within a 180-day period after implantation. Rates of toxic anterior segment syndrome (TASS), acute postoperative endophthalmitis, chronic postoperative endophthalmitis, and uncategorized cases of postsurgical intraocular inflammation were assessed. Ocular adverse events (AEs) and ocular adverse device effects (ADEs) were evaluated. Historical rates of postsurgical intraocular inflammation were determined from the 2011–2013 Medicare Limited Data Set files (a 5% sample of the Medicare data set representative of patients aged ≥65 years).
Results
Final safety analysis set included 3357 eyes (1792 patients; mean age, 68.6 ± 7.9 years). Postsurgical intraocular inflammation (any type) rate was 5.1 per 1000 attempted IOL implants (95% CI, 2.95, 8.10). TASS, acute postoperative endophthalmitis, and uncategorized inflammation rates were 0.6 (95% CI, 0.07, 2.15), 0.3 (95% CI, 0.01, 1.66), and 4.2 (95% CI, 2.28, 6.99) per 1000 attempted IOL implants, respectively. There were no events of chronic postoperative endophthalmitis. Ocular AEs and ADEs were reported in 17% and 1.5% of eyes, respectively. Most common ADEs were halo (0.63%) and glare (0.51%). The historical postsurgical inflammation rate from 221,519 cataract procedures was 10.3/1000 cataract surgeries, and the endophthalmitis rate was 1.2/1000 surgeries.
Conclusion
The updated IOL manufacturing process resulted in postoperative intraocular inflammation rates that were substantially lower than the historic rate.
Introduction
Cataract, the leading cause of reversible blindness worldwide,Citation1 can be treated by removing the cloudy natural crystalline lens and implanting an intraocular lens (IOL).Citation2 This common surgical procedure to restore visual function is effective and typically safe and uneventful. However, postsurgical inflammation and other complications can occur in some cases, including toxic anterior segment syndrome (TASS) and endophthalmitis. Both TASS and endophthalmitis can lead to poor visual outcomes.Citation3–5
TASS is caused by a noninfectious substance entering the anterior segment of an eye during cataract surgery and may result from surgical instrument or IOL contamination.Citation3 It is characterized by anterior chamber inflammation during the early postoperative period, causing toxic cellular and extracellular damage.Citation6 Symptoms of TASS may include blurry vision, ocular pain, corneal edema, macular edema, visual deterioration, and eye redness.Citation6,Citation7 TASS is uncommon (incidence of 0.22% based on case series)Citation8 but often occurs in a clustered outbreak at specific surgical sites.Citation6 In patients with TASS, visual acuity was significantly worse after the development of inflammation than before.Citation9,Citation10
Another type of postsurgical inflammation, and one of the most serious complications of cataract surgery, is postoperative endophthalmitis (incidence, 0.012%–1.3%).Citation11 It is most often caused by gram-positive bacteria and is characterized by moderate-to-severe ocular pain and decreased visual acuity.Citation3 In patients with endophthalmitis occurring within 6 weeks after cataract surgery or secondary IOL implantation, 26% were reported to have visual acuity worse than 20/100 Snellen at 9–12 months of follow-up.Citation4 A population-based, 21-year retrospective study in Australia also reported that patients with postoperative endophthalmitis had poor visual outcomes.Citation5
Specific materials and IOL models have been associated with postsurgical inflammation.Citation10–13 In a case series (7 eyes of 4 patients) that evaluated a TASS outbreak at 2 tertiary hospitals between July and November 2020, a Lentis Comfort IOL (LS-313MF15, Santen Pharmaceutical, Osaka, Japan), a hydrophilic soft acrylic IOL, was most likely the cause of TASS. The incidence of TASS in this case series was 4.3% (7/162).Citation12 In a retrospective study of 251 patients who developed TASS between November 2011 and February 2013, a 1-piece acrylic iSert 251 and iSert 255 IOLs (HOYA, Tokyo, Japan) were identified as a likely cause, with an incidence of 0.7% (251/34,239).Citation10 Historically, silicone IOLs were significantly associated with increased risk of postoperative endophthalmitis compared with polymethylmethacrylate or acrylic hydrophobic IOLs (odds ratio, 3.13; 95% CI, 1.47–6.67),Citation14 suggesting that IOL material properties may play a role in postoperative intraocular inflammation.
Between January 2015 and March 2016, a cluster of unusual ocular inflammation cases were reported in 304 eyes at 184 sites in Japan following implantation of AcrySof® IQ ReSTOR® single-piece multifocal (toric and nontoric) IOLs (Alcon Vision LLC, Fort Worth, TX, USA).Citation9 A retrospective observational case series in 201 eyes reported TASS incidence of approximately 2.0% after implantation of the AcrySof ReSTOR and ReSTOR toric IOLs and 0.74% for AcrySof IQ toric IOLs (T6–T9).Citation9 In April 2015, Alcon announced a voluntary product recall in Japan for all AcrySof ReSTOR and ReSTOR toric multifocal IOLs manufactured in and marketed only in Japan.Citation15 The recall in Japan was expanded to include AcrySof IQ high cylinder toric IOLs (T6–T9) in October 2015.
The manufacturer conducted a thorough internal investigation and found residual particles on the surface of approximately 6.8% of inspected unused IOLs.Citation9 The increased residual particles were attributed to the specific manufacturing process for the Japan AcrySof ReSTOR multifocal (toric and nontoric) IOLs (specifically in the oven curing and wet metrology steps). To address these local market TASS events, the updated manufacturing process included a shortened curing cycle, a change from a batch to a tunnel oven, and the introduction of a new wafer molding material.
Although this manufacturing process and these TASS-related incidents were specific to the Japanese market, manufacturing updates and improvements were subsequently introduced in the United States (US) and for global production. With the submission for approval of the AcrySof IQ ReSTOR +3.0 multifocal Toric IOL in the US, a post-approval study was requested by the US Food and Drug Administration (FDA). The purpose of this study was to assess the incidence of postsurgical intraocular inflammation up to 6 months after implantation with AcrySof IQ ReSTOR IOLs manufactured using the updated process and compare it with the historical rate of postsurgical intraocular inflammation.
Methods
Study Design
This was a prospective, multicenter, active-surveillance post-approval study with 6-month follow-up (NCT03733730). The study was conducted at 34 sites in the US between October 2020 and October 2022. Patients received AcrySof IQ ReSTOR lenses that were either +3.0 multifocal toric (models SND1T3–6) or multifocal nontoric (models SV25T0). These IOLs are manufactured using single-piece construction, have a 6.0-mm diameter biconvex optic, and have an overall length of 13.0 mm. The haptics are made of the same materials as the optic with no angulation. The same updated manufacturing process was used for both toric and nontoric IOLs.
Included in the study were patients aged ≥22 years who received the study lens in at least 1 eye. Excluded from the study were eyes with ocular inflammation at the screening visit or on the day of surgery (although slit-lamp examination was not required on the day of surgery, patients were checked for obvious signs of infection and inflammation), patients with a history of any intraocular inflammation (eg, uveitis, choroiditis) within the past year, and patients who had combined procedures introducing an additional medical device during cataract surgery. Visits included the presurgery visit (≤40 days before first eye implantation and ≤60 days before second eye implantation), the operative visit, and postimplantation visits 1–2 days, 7–14 days, 30–60 days, and 90–180 days after implantation of each eye. Attempted IOL implantations were defined as successful or aborted implantations after contact with the eye.
The study was conducted in accordance with the principles of the Declaration of Helsinki and in compliance with the International Council for Harmonisation E6 Good Clinical Practice Consolidated Guideline and ISO 14155:2011 Clinical Investigation of Medical Devices for Human Subjects, code of federal regulations, and standard operating procedures of Alcon and contract research organizations. Study sites received institutional review board (IRB) approval from Sterling IRB or Advarra. All patients provided informed consent before initiation of any screening.
Postsurgical Intraocular Inflammation Assessments
The primary endpoint assessed the rate (per 1000 attempted IOL implants) of all postsurgical intraocular inflammation reported within a 180-day period after implantation. Postsurgical intraocular inflammation was defined as exacerbated intraocular inflammation, including aqueous cell grade ≥3+ within 14 days after surgery, aqueous cell ≥2+ at 14 to ≤60 days after surgery, or aqueous cell ≥1+ at >60 days.
The secondary endpoints assessed the rates (per IOL attempted IOL implants) of postsurgical TASS, acute postoperative endophthalmitis, chronic postoperative endophthalmitis, and uncategorized cases of postsurgical intraocular inflammation within 180 days after implantation. TASS was defined as aqueous cell graded ≥3+, noninfectious etiology, and rapid onset (up to and including 2 days after surgery). Acute postoperative endophthalmitis was defined as aqueous cell graded ≥3+, infectious (positive culture of ocular media) or noninfectious etiology, inflammatory cells in the vitreous or vitreous abscess, and a rapid onset (3–14 days after surgery). Chronic postoperative endophthalmitis was defined as aqueous cell graded ≥1+, infectious (positive culture of ocular media) or noninfectious etiology, inflammatory cells in the vitreous, and a delayed onset (>14 days after surgery). Uncategorized postsurgical intraocular inflammation was defined as aqueous cell graded ≥3+ within the first 14 days after surgery, aqueous cell graded ≥2+ at >14 to ≤60 days after surgery, and aqueous cell graded ≥1+ at >60 days after the surgery that did not meet the definitions for TASS or endophthalmitis.
Additional Safety Assessments
Ocular and non-ocular adverse events (AEs), serious AEs (SAEs), and device deficiencies were collected for patients enrolled in the study. Every AE and device deficiency was assessed as related or not related to the medical device or test procedure by the investigator. The investigator also assessed the severity of the AEs as mild, moderate, or severe.
Best corrected distance visual acuity (BCDVA) was assessed in all patients at all visits except the operative visit. Visual acuity was measured under photopic conditions with dimmed room illumination using standard-of-care equipment. The last line with a majority of letters correctly identified was counted as the final score, and results were documented in Snellen. The same exam room setup and test administration procedures were used consistently throughout the study at each site.
Statistical Analysis
The safety set used in the analysis included all eyes with attempted IOL implantation. The rates of postsurgical intraocular inflammation and exact two-sided 95% confidence intervals (CI) were determined. The event rate was calculated as the total number of reported events divided by the total number of attempted implants × 1000. An eye with multiple reports of inflammation was only counted once. The modified safety set, which included all eyes with successful IOL implantation, was used for sensitivity analysis of the primary safety endpoint.
Historical Rates of Postsurgical Intraocular Inflammation
Data were analyzed from the 2011–2013 Medicare Limited Data Set files (as recommended by the FDA), a 5% sample of the Medicare data set representative of US citizens aged ≥65 years. All cataract surgeries reported in that time period in the database were reviewed to assess the frequency of postsurgical intraocular inflammation within 180 days of cataract surgery. Historical rate (per 1000 surgeries) of postsurgical intraocular inflammation was determined based on the International Classification of Diseases coding of endophthalmitis, uveitis, postsurgical intraocular inflammation, or other related codes within the 180-day period after IOL implantation (specific IOLs were not listed in the Medicare database).
Results
There were 3417 eyes (1827 patients) that underwent attempted implantation with the study lens, and 3416 eyes were successfully implanted. Because of Good Clinical Practice violations, a single site (60 eyes [35 patients] that underwent attempted implantation) was excluded from the study; there were no cases of inflammation in these eyes. The final safety analysis set included 3357 eyes (1792 patients). The modified safety set included 3356 eyes (one 2nd eye was excluded because the IOL was not implanted after touching the patient’s eye). Mean age was 68.6 ± 7.9 years, 64% of patients were female, and 77% were white ().
Table 1 Patient Demographics and Baseline Characteristics (Safety Analysis Set)
Postsurgical Intraocular Inflammation
Postsurgical intraocular inflammation (any type) rate in overall eyes was 5.1 per 1000 attempted IOL implants (95% CI, 2.95, 8.10; ), reported in 17/3357 eyes. There were 19 postsurgical inflammation events in 17 eyes (2 eyes had a reoccurring event). Time to occurrence of inflammation for the first eye events ranged from 1 to 115 days after surgery, and the majority of events occurred during the first 92 days. Duration of inflammation ranged from 6 to 108 days; 1 case of inflammation was “ongoing” at the 6-month visit. In the modified safety set, the Kaplan–Meier cumulative event rate at 6 months after implantation was 0.6% (95% CI, 0.34, 0.90). None of the cases were assessed as related to the study device.
Figure 1 Rates of postsurgical inflammation. Rates were calculated as (n/Total) × 1000. Error bars represent 95% CI.
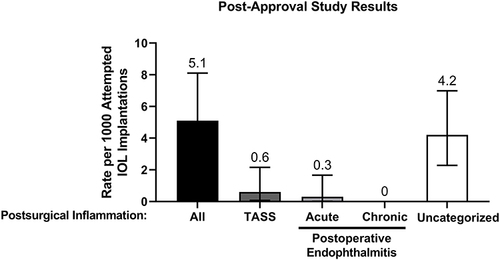
Secondary safety endpoints included postsurgical inflammation rates stratified by type: TASS, acute and chronic postoperative endophthalmitis, and uncategorized (). TASS was reported in 2 eyes; the event rate was 0.6 per 1000 attempted IOL implants (95% CI, 0.07, 2.15). Acute postoperative endophthalmitis was reported in 1 eye; the event rate was 0.3 per 1000 attempted IOL implants (95% CI, 0.01, 1.66). There were no events of chronic postoperative endophthalmitis. Uncategorized inflammation was reported in 14 eyes (2 eyes had a reoccurring event); the event rate was 4.2 per 1000 attempted IOL implants (95% CI, 2.28, 6.99).
Safety
Ocular AEs were reported in 17% (577/3357) of all eyes. The most common ocular AEs included intraocular pressure increase (3.4%; 113/3357), posterior capsule opacification (3.2%; 107/3357), and visual acuity reduction (1.7%; 58/3357; ). Ocular SAEs were reported in 1.2% (41/3357) of all eyes. The most common serious ocular AE was vitrectomy (0.36%; 12/3357; ). Fifteen ocular SAEs were related to the device, including device dislocation (n = 3), IOL repositioning (n = 8), and glare (n = 4). In addition, 3 events of device dislocation were unrelated to the device (2 device dislocations and 1 off-axis device rotation were procedure-related).
Table 2 Treatment-Emergent Ocular Adverse Events with Incidence ≥1% (Safety Analysis Set)
Table 3 Treatment-Emergent Ocular Serious Adverse Events with Incidence ≥0.1% (Safety Analysis Set)
Ocular adverse device effects were reported in 1.5% (51/3357) of all eyes and included 62 events. The most common adverse device effects were halo vision (0.63%; 21/3357) and glare (0.51%; 17/3357). Secondary surgical interventions were reported in 0.98% (33/3357) of all eyes and were caused by IOL repositioning (0.33%; 11/3357), vitrectomy (0.33%; 11/3357), and lens extraction (0.27%; 9/3357). Furthermore, there were 16 device deficiencies reported in the safety analysis set, including scratched materials (0.12%; 4/3357) and failure to fold (0.09%, 3/3357; ).
Table 4 Device Deficiencies (Safety Analysis Set)
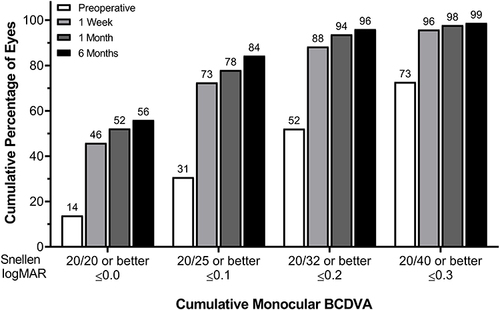
At 6 months after implantation, 56% of eyes in the safety analysis set achieved BCDVA of 20/20 or better, and 99% of eyes achieved BCDVA of 20/40 or better ().
Figure 2 Cumulative distribution of monocular BCDVA in eyes implanted with the study IOL.
Historical Postsurgical Intraocular Inflammation Rate
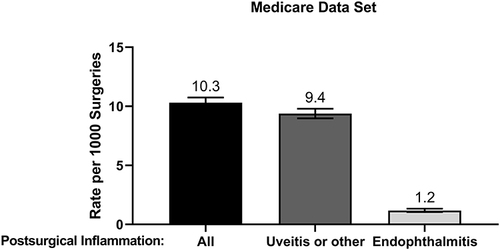
The Medicare data set, which comprised a 5% systematic sample of records of all non-HMO Medicare patients enrolled from 2011 through 2013, included 221,519 cataract procedures. All patients were aged ≥65 years, 60% were female, and 89% were white. At 6 months after implantation, there were 2284 postsurgical inflammation events, and the reported event rate was 10.3 per 1000 cataract surgeries (95% CI, 9.89, 10.74; ). Of these, there were 260 events of endophthalmitis; the event rate was 1.2 per 1000 surgeries (95% CI, 1.04, 1.33). There were 2077 events of uveitis or other post-surgical inflammation; the event rate was 9.4 per 1000 surgeries (95% CI, 8.98, 9.79).
Figure 3 Rates of historical postsurgical inflammation from the Medicare data set. Rates were calculated as (n/Total) × 1000. Error bars represent 95% CI.
Discussion
Optimizing IOL material selection and the manufacturing process may improve IOL biocompatibility and help improve safety outcomes related to cataract surgery, including postsurgical intraocular inflammation.Citation16 This 6-month study assessed the rate of postoperative inflammation in cataract patients who received AcrySof ReSTOR IOLs produced using the updated manufacturing process. An overall rate of postsurgical intraocular inflammation was 5.1 events per 1000 attempted IOL implantations; most of these events were uncategorized, with the TASS and acute postoperative endophthalmitis rates of 0.6 and 0.3 events per 1000 attempted IOL implantations, respectively. Based on an analysis of the 2011–2013 Medicare Beneficiary files, the historical postsurgical inflammation rate was 10.3 events per 1000 surgeries (95% CI, 9.89, 10.74), substantially higher than the rate reported in this study.
It can be difficult to isolate the cause of TASS: some of the causes have been reported to include intraocular irrigation solutions and medications with suboptimal chemical composition or pH, toxic-contaminating residues, and materials contained within or on the IOLs themselves (ie, polishing compounds and cleaning and sterilizing compounds).Citation6 Some studies suggest that IOL manufacturing processes, particularly residual metallic particles on IOLs, may be associated with TASS. One study assessed TASS in patients who received iSert IOLs contaminated with aluminum; in these patients, the most common presenting signs of TASS were the appearance of inflammatory cells in the anterior chamber (affecting 99% of eyes) and conjunctival injection.Citation10 Another study reported an aluminum-related late-onset TASS outbreak in 6 patients implanted with iSert IOLs.Citation17 A case report has also linked iSert IOL contamination with residual metallic particles to TASS; the manufacturing process that was used has been since updated.Citation18 Furthermore, MemoryLens (CIBA Vision) contaminated with metallic particles has been suggested to be associated with TASS in some patients;Citation13 these findings also led to an update in the manufacturing process of MemoryLens IOLs.
Following the postoperative inflammation outbreak associated with the AcrySof IQ Toric (T6–T9) and IQ ReSTOR IOLs in Japan,Citation9 several updates to manufacturing process, including shortened curing cycle, a change from a batch to a tunnel oven, and a new wafer molding material, were implemented and resulted in positive clinical outcomes reported in this study. In 2017, a post-market surveillance study was conducted in Japan, enrolling 3451 eyes at 394 surgical sites. Eyes were implanted with AcrySof IQ ReSTOR or ReSTOR Toric multifocal IOLs manufactured using the revised process, and the rate of postoperative inflammation was assessed for these cataract patients.Citation19 After the successful completion of this study in Japan, all AcrySof IQ ReSTOR, ReSTOR Toric, and high-cylinder Toric IOLs were reintroduced to the Japan market. Additionally, the updated manufacturing process is now used globally for Alcon lenses, including the Clareon family of IOLs.
Adverse device effects such as halo vision and glare reported in this study were consistent with the known risks associated with multifocal IOLs.Citation20 Rates of halo and glare were 0.6% (21/3357) and 0.5% (17/3357), respectively. In comparison, an earlier prospective, randomized clinical trial that assessed effectiveness and safety of the +2.5 D AcrySof ReSTOR multifocal IOL reported glare and halos in 3% (8/310 for both) of eyes at 6 months after implantation.Citation21 A prospective cohort study that assessed visual and safety outcomes with +3.0 D AcrySof ReSTOR toric reported glare and halos in 3.5% (13/372) and 7.5% (28/372) of eyes, respectively, at 1 year after implantation.Citation22
In the current study, 56%, 84%, and 99% of eyes achieved monocular BCDVA of 20/20 or better, 20/25 or better, and 20/40 or better, respectively. An extensive database study of 368,256 cataract extractions demonstrated similar outcomes, with 61% and 94% of patients achieving BCDVA of 20/20 or better and 20/40 or better, respectively.Citation23 In a small study of 32 eyes implanted with Tecnis Multifocal IOL at a single site (ZMB00; Johnson & Johnson Vision, Irvine, CA, USA), 94% and 100% of eyes achieved monocular BCDVA of 20/20 or better and 20/25 or better, respectively (mean follow-up was at 9.4 ± 3.8 months).Citation24 Another small study (n = 19) reported that 79% and 95% of eyes implanted with Tecnis Synergy multifocal IOL achieved monocular BCDVA of 20/20 or better and 20/25 or better, respectively, at 6 months after implantation.Citation25 A 6-month study in patients who received Tecnis Synergy (n = 135) reported that 80%, 97%, and 100% of eyes achieved monocular BCDVA of 20/20 or better, 20/25 or better, or 20/50 or better, respectively.Citation26 However, differences in standardization across sites, methodology (eg, Snellen versus logMAR Early Treatment Diabetic Retinopathy Study charts), patient selection (eg, predefined exclusion parameters), and study design make interpretation difficult and comparison of visual acuity among the studies impractical.
This study has a number of limitations. There were violations related to Good Clinical Practice at one of the sites, resulting in exclusion of the data from the analysis. Furthermore, study design and patient population may have contributed to only 56% of eyes achieving BCDVA of 20/20 or better. Not all the diagnostic criteria of this study matched the diagnostic codes in the Medicare data analysis. Furthermore, the Medicare data analysis used a 5% sample of the database from more than 10 years ago (2011–2013), and standard cataract surgery techniques may have improved in that period. However, a recent analysis of all Medicare beneficiaries from 2016 to 2019 reported an endophthalmitis rate of 0.08% for cataract surgeries and 0.11% for cataract surgeries combined with other procedures, which is consistent with the 0.12% rate from the 2011–2013 Medicare data.Citation27
In conclusion, the updated Alcon IOL manufacturing process results in low rates of postoperative intraocular inflammation. It is important for manufacturers to monitor IOL product performance and safety, implementing timely manufacturing process improvements when appropriate, for continuous outcome improvements.
Disclosure
James Paauw received research support from Alcon. Michael Caplan received research support and consulting fees from Alcon. Mark Gallardo received research support and consulting fees and was a speaker for Alcon. Kristi Rushin is an employee of Alcon. Jeff Horn received research support from Alcon and was a consultant and speaker for Alcon. The authors report no other conflicts of interest in this work.
Acknowledgments
Medical writing assistance was provided by Natalia Zhukovskaya, PhD, of ICON plc (Blue Bell, PA) and was funded by Alcon. The authors would like to thank Val Injev, MBA, PE, for his valuable input in the preparation of this manuscript.
Additional information
Funding
References
- Flaxman SR, Bourne RRA, Resnikoff S, et al. Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis. Lancet Glob Health. 2017;5(12):e1221–e1234. doi:10.1016/S2214-109X(17)30393-5
- Lundstrom M, Barry P, Henry Y, Rosen P, Stenevi U. Evidence-based guidelines for cataract surgery: guidelines based on data in the European Registry of Quality Outcomes for Cataract and Refractive Surgery database. J Cataract Refract Surg. 2012;38(6):1086–1093. doi:10.1016/j.jcrs.2012.03.006
- Sengillo JD, Chen Y, Perez Garcia D, et al. Postoperative endophthalmitis and toxic anterior segment syndrome prophylaxis: 2020 update. Ann Transl Med. 2020;8(22):1548. doi:10.21037/atm-2019-rcs-02
- Endophthalmitis Vitrectomy Study Group. Results of the Endophthalmitis Vitrectomy Study: a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitis. Arch Ophthalmol. 1995;113(12):1479–1496. doi:10.1001/archopht.1995.01100120009001
- Ng JQ, Morlet N, Pearman JW, et al. Management and outcomes of postoperative endophthalmitis since the Endophthalmitis Vitrectomy Study: the Endophthalmitis Population Study of Western Australia (EPSWA)’s fifth report. Ophthalmology. 2005;112(7):1199–1206. doi:10.1016/j.ophtha.2005.01.050
- Mamalis N, Edelhauser HF, Dawson DG, et al. Toxic anterior segment syndrome. J Cataract Refract Surg. 2006;32(2):324–333 doi:10.1016/j.jcrs.2006.01.065
- Park CY, Lee JK, Chuck RS. Toxic anterior segment syndrome-an updated review. BMC Ophthalmol. 2018;18(1):276. doi:10.1186/s12886-018-0939-3
- Sengupta S, Chang DF, Gandhi R, Kenia H, Venkatesh R. Incidence and long-term outcomes of toxic anterior segment syndrome at Aravind Eye Hospital. J Cataract Refract Surg. 2011;37(9):1673–1678. doi:10.1016/j.jcrs.2011.03.053
- Oshika T, Eguchi S, Goto H, Ohashi Y. Outbreak of subacute-onset toxic anterior segment syndrome associated with single-piece acrylic intraocular lenses. Ophthalmology. 2017;124(4):519–523. doi:10.1016/j.ophtha.2016.12.010
- Suzuki T, Ohashi Y, Oshika T, et al. Outbreak of late-onset toxic anterior segment syndrome after implantation of one-piece intraocular lenses. Am J Ophthalmol. 2015;159(5):934–939.e2. doi:10.1016/j.ajo.2015.01.023
- Cao H, Zhang L, Li L, Lo S. Risk factors for acute endophthalmitis following cataract surgery: a systematic review and meta-analysis. PLoS One. 2013;8(8):e71731 doi:10.1371/journal.pone.0071731
- Imamachi K, Sugihara K, Ikeda Y, Matsuoka Y, Tanito M. Report of a cluster of cases of toxic anterior-segment syndrome after implantation of a specific intraocular lens model. Am J Ophthalmol. 2021;228:1–7. doi:10.1016/j.ajo.2021.03.024
- Jehan FS, Mamalis N, Spencer TS, et al. Postoperative sterile endophthalmitis (TASS) associated with the MemoryLens. J Cataract Refract Surg. 2000;26(12):1773–1777. doi:10.1016/S0886-3350(00)00726-4
- ESCRS Endophthalmitis Study Group. Prophylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factors. J Cataract Refract Surg. 2007;33(6):978–988. doi:10.1016/j.jcrs.2007.02.032
- Alcon announces a voluntary product recall in Japan. Alcon. Available from: https://www.alcon.com/media-release/alcon-announces-voluntary-product-recall-japan. Accessed June 19, 2024
- Luo C, Wang H, Chen X, et al. Recent advances of intraocular lens materials and surface modification in cataract surgery. Front Bioeng Biotechnol. 2022;10:913383. doi:10.3389/fbioe.2022.913383
- Miyake G, Ota I, Miyake K, et al. Late-onset toxic anterior segment syndrome. J Cataract Refract Surg. 2015;41(3):666–669. doi:10.1016/j.jcrs.2015.01.002
- Kumaran N, Larkin G, Hollick EJ. Sterile postoperative endophthalmitis following HOYA IOL insertion. Eye. 2014;28(11):1382. doi:10.1038/eye.2014.170
- Alcon Vision LLC. Data on File. Fort Worth, TX: Alcon Vision LLC; 2018
- ACrySof IQ ReStor multifocal IOL. Full Prescribing Information. Fort Worth, TX: Alcon Laboratories, Inc; 2015
- Maxwell A, Holland E, Cibik L, et al. Clinical and patient-reported outcomes of bilateral implantation of a +2.5 diopter multifocal intraocular lens. J Cataract Refract Surg. 2017;43(1):29–41. doi:10.1016/j.jcrs.2016.10.026
- Lehmann R, Modi S, Fisher B, Michna M, Snyder M. Bilateral implantation of +3.0 D multifocal toric intraocular lenses: results of a US Food and Drug Administration clinical trial. Clin Ophthalmol. 2017;11:1321–1331 doi:10.2147/OPTH.S137413
- Lundström M, Barry P, Henry Y, Rosen P, Stenevi U. Visual outcome of cataract surgery; study from the European Registry of Quality Outcomes for Cataract and Refractive Surgery. J Cataract Refract Surg. 2013;39(5):673–679. doi:10.1016/j.jcrs.2012.11.026
- Chang DH, Thompson VM, Christie WC, Chu YR, Vida RS. Clinical evaluation of a modified light transmission short-wavelength filtering intraocular lens compared to a colorless control. Ophthalmol Ther. 2023;12(3):1775–1785. doi:10.1007/s40123-023-00709-w
- Moshirfar M, Stapley SR, Corbin WM, et al. Comparative visual outcome analysis of a diffractive multifocal intraocular lens and a new diffractive multifocal lens with extended depth of focus. J Clin Med. 2022;11(24):7374. doi:10.3390/jcm11247374
- Chang DH, Hu JG, Lehmann RP, et al. Clinical performance of a hybrid presbyopia-correcting intraocular lens in patients undergoing cataract surgery in a multicenter trial. J Cataract Refract Surg. 2023;49(8):840–847. doi:10.1097/j.jcrs.0000000000001205
- Chen A, Dun C, Schein OD, et al. Endophthalmitis rates and risk factors following intraocular surgeries in the medicare population from 2016 to 2019. Br J Ophthalmol. 2024;108(2):232–237. doi:10.1136/bjo-2023-323865