
Abstract
Purpose
To investigate the long-term visual outcome and their determinants after an operation in Thai pituitary adenoma (PA).
Patients and Methods
A retrospective cohort study was conducted on PA patients who underwent surgery at Rajavithi Hospital. Baseline characteristics and visual parameters, including visual acuity (VA) and visual field (VF), were analyzed in relation to the visual prognosis outcome. The outcome was defined as VA improvement at 1-year postoperatively. Visual parameters were measured at each follow-up visit and compared. Factors for improved visual prognosis were evaluated using logistic regression analysis.
Results
A total cohort of 87 patients (64.37% female), 62.07% showed improvement in visual outcome. Most improvement occurred immediately after surgery, evident at the 1-month visit. The mean follow-up time was 47.45 months (±28.49 SD), mean difference in VA improvement at 1-year was −0.56 logMAR (95% CI −0.73, −0.47). In multivariable logistic regression model, prolonged onset duration was associated with a reduced odds of improved visual outcome, with an odds ratio (OR) of 0.946 (95% CI 0.899–0.996, p = 0.034). Baseline characteristics, tumor volume, Hardy and Knops classification, and surgical approaches were not identified as significant predictors.
Conclusion
Both TSS and transcranial approaches are effective for pituitary adenoma. A prompt operation is recommended for patients with prolonged onset duration, with thorough discussion on poor postoperative visual outcomes.
Introduction
Pituitary adenoma (PA) is one of the most common benign tumors in the central nervous system (CNS). The incidence of PA varies from 3% to 25%.Citation1–3 It can be categorized into functioning or non-functioning PA. Functioning PA may present with hormonal hypersecretion, such as Cushing syndrome or prolactinoma. Despite its benign nature in non-functioning PA without hormonal disturbance, the tumor can cause headache, visual impairment, or diplopia due to tumor invasion in the cavernous sinus.Citation4–6 There are several treatment modalities for the tumor, including medical, surgical, and radiotherapy. Typically, patients who present with significant visual symptoms or a neurological deficit with a large tumor are chosen for surgical management.Citation2 Transsphenoidal approach (TSS) is the primary treatment chosen for the majority of pituitary tumors.Citation7 Aggressive pituitary tumors may require multimodal therapy with multiple operations.
Several predictive factors for postoperative visual outcomes in PA have been identified. A shorter duration of symptoms before surgery and younger age are associated with a higher amount of reserved nerve fiber layers.Citation5,Citation8–10 Additionally, large tumor size and suprasellar extension are significantly associated with poor postoperative visual outcomes.Citation11,Citation12 Regarding the prognosis for the visual field, favorable outcomes are observed in patients with a short duration of symptoms, a higher preoperative VF, and a thicker peripapillary temporal retinal nerve fiber layer (RNFL).Citation8 While several researchers proposed the great benefit of TSS, the transcranial approach was found to be a significant predictor of favorable visual field improvement in an Asian study.Citation13,Citation14
The present study aims to identify predictive factors for favorable postoperative visual outcomes in patients with PA at Rajavithi Hospital and to report on long-term visual outcomes in Thai populations.
Patients and Methods
Patients’ Selection and Clinical Characteristics
We conducted a retrospective study of all PA patients who received their first operation at the department of neurosurgery in Rajavithi Hospital, Thailand, between January, 2016, and December, 2020. The inclusion criteria were for PA patients aged 18–80 years who underwent their first surgery at our center. Exclusion criteria included: 1) patients under 18 or over 80; 2) incomplete baseline characteristic data; 3) follow-up time less than 1 years; 4) history of prior tumor operation, chemotherapy, or radiation; 5) recurrent PA; and 6) preexisting eye diseases that could affect the visual field, such as glaucoma or other optic neuropathies.
Demographic and tumor data were retrospectively reviewed, including age, gender, and baseline visual status such as best corrected visual acuity (BCVA), which were converted to the logarithm of the minimum angle of the resolution (logMAR) as the follows;Citation15 no perception of light (NPL), perception of light (PL), hand moment (HM), counting finger (CF) to 3.4, 3.1, 2.9, and 2.6, respectively, presence of relative afferent pupillary defect (RAPD), and disc morphology. The type of functioning adenoma was reviewed based on the endocrinologist’s preoperative diagnosis, determined through serum hormone-level assessments. The visual field defect was measured by the 30–2 Swedish of the Humphrey visual field automate perimetry. Reliable VF value assessment was confirmed when fixation losses or false-positive or false-negative responses were less than 20%.Citation16 Radiological characteristics of PA, including size, extension, and location, were assessed preoperatively using computed tomography scan (CT scan) or brain magnetic resonance imaging (MRI). Postoperative visual status at each follow-up visit was retrospectively reviewed at 1, 6, 12, and 24 months. Outcome of visual improvement was defined as a decrease of at least 0.2 logMAR between baseline and postoperative 1-year. Tumor volume and extension were measured and classified according to Hardy-Wilson and Knosp classifications.Citation17,Citation18
Ethics Approval
The present study was approved by the Ethics committee at Rajavithi Hospital (certificate number 186/66) and followed the Declaration of Helsinki. All participants were received inform and consent before data collection.
Statistical Analysis
Continuous data were expressed as mean, standard deviation (SD) in normal distributed data, or interquartile range (IQR) in non-normal distributed data. Categorical data were expressed as percentages and compared using Chi-square or Fisher exact test. The comparison of continuous data was employed by the Student’s t-test or Mann–Whitney’s U-test. The difference in visual acuity in logMAR and visual field in decibel for each postoperative visit was compared using multilevel mixed-effects model analysis. Potential prognostic predictors associated with improved postoperative visual recovery in univariable analysis with p <0.2 were further included in multivariable logistic regression model. All statistical significances were set at p <0.05. All analyses were done using a standard statistical program.
Result
Clinical Characteristics of Pituitary Adenoma Patients
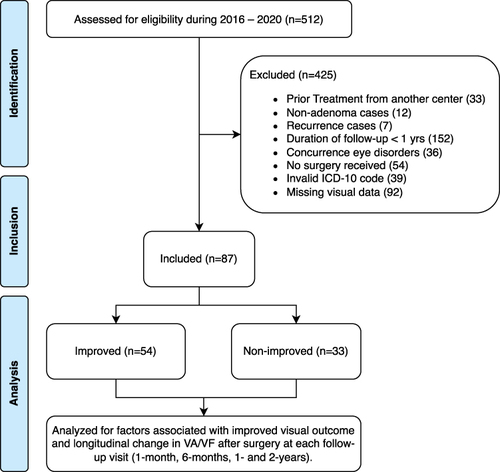
We retrospectively enrolled all patients diagnosed with PA during 2016–2020 at our center. Subsequently, 174 eyes from 87 patients were selected for inclusion in the analysis after being excluded according to the exclusion criteria (). The characteristics of the patients at baseline preoperatively were similar in both improved and non-improved groups, with 62.07% of patients demonstrating improvement (). The mean (SD) age was 50 (12.81) years, with no significant difference between the improved and non-improved groups (p = 0.864). Gender distribution showed no significant disparity between the groups (p = 0.252), with 64.37% females overall. The presenting symptoms were generally unremarkable, with visual blurring being the most common symptom in the entire cohort. Patients in the improved group had a shorter duration of symptoms (p < 0.001). The mean follow-up time for both groups was 47.45 (28.49) months, with no significant difference.
Table 1 Baseline Characteristics in Pituitary Adenoma Patient.*
Figure 1 STROBE study participant’s flow chart.
Functioning adenomas constitute 77.5% of patients with available lab panels (40 out of 87 patients from the entire cohort). No significant differences were observed between the groups regarding the type of functioning adenoma, while prolactinoma was the most common, accounted for 40% (). Macroadenoma was comparable (p = 0.055). Hardy and Knops classifications were similar between the two groups (p = 0.860, p = 0.471, respectively), with the majority of the cohort falling below grade C and below grade 3 in Hardy and Knops classifications, respectively.
Table 2 Baseline Characteristics of Tumor and Imaging Classification.*
Long-Term Visual Outcome in Improved Vs Non-Improved Group
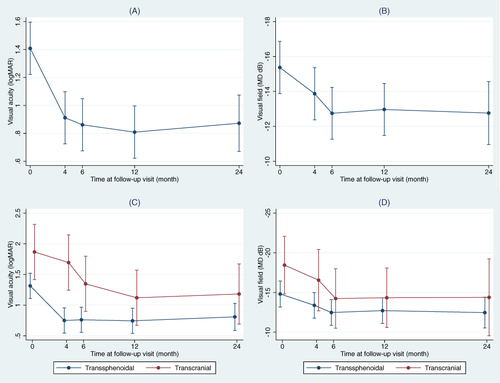
Visual acuity demonstrated a statistically significant improvement after surgery over the follow-up period (, ). Preoperatively, the overall median logMAR in the worse-seeing eye was 1 (range 0.1 to 3.4), which improved to 0.6 (0–3.4) at 1-month postoperatively (p < 0.001). Visual field exhibited a similar trend with a median MD of −15.19 dB (−32.77 to −1.71) and improved to −12.48 (−28.89 to −2.48) at 1-month postoperatively (p = 0.064). From 1-month postoperatively through month 48, both visual acuity and visual field remained stable. The mean difference in VA improvement at 1-year in the worse-seeing eye was −0.56 logMAR (95% CI −0.73, −0.47). The mean difference in VF improvement was 2.40 dB (95% CI 0.82, 3.99).
Table 3 Trend of Baseline and Postoperative Visual Parameters.*
Figure 2 Changes in visual parameters from during each follow-up visit.
Determinates on Visual Outcome
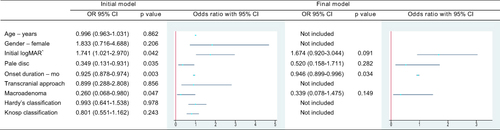
A multivariable logistic regression analysis was conducted to identify factors influencing poor visual outcomes. In the multivariable regression model, age, gender, pale disc, surgical approaches, macroadenoma, and Hardy classification were excluded (). Duration of symptoms remained significant associated factors with an improved visual outcome, with an OD of 0.946 (95% CI 0.899–0.996, p = 0.034).
Figure 3 Multivariable logistic regression model of the initial and final best model for improved visual outcome postoperatively.
Discussion
The present study found that the overall visual improvement of PA post-operation is 62.07% at 1-year postoperatively. The most apparently improved VA and VF were observed during 1–6 months. The significant predictive risk factor for poor visual outcome postoperatively is prolonged duration of symptom.
In our cohort, there was a female predominance, similar to other studies.Citation16,Citation19 Visual blur was the most common presenting symptom, consistent with previous reports.Citation16,Citation20 Regarding the influence of patient age on visual prognosis, its impact differs among each study. Young age has a better visual prognosis in some studies.Citation9,Citation13,Citation16,Citation21 On the contrary, Watanabe et al observed no difference in postoperative visual outcome in Japanese patients in the elderly group (≥70 years) compared to the younger group.Citation22 In our cohort, both improved and non-improved groups exhibited a nearly identical age range. The influence of age on the outcome of the disease remains unclear, probably because various parameters differ among studies including tumor size, tumor extension, or different criteria of visual outcome in each study. Additionally, epigenetic changes associated with aging and age-related vascular changes may contribute to poor visual outcomes.Citation23 However, previous researchers observed that the most substantial improvement in visual field occurs 6 months rather than within the initial 3 months period after surgery.Citation24 Butenschoen VM et al reported a significant improvement at 3 months post-TSS.Citation13 Taghvaei M et al also proposed an improvement in visual status in the PA patients (VA, VF) shortly after 3 months post-TSS.Citation21 In this cohort, we found a notable improvement in visual outcome between the period of 4 weeks and 6 months. This trend in visual prognosis could serve as valuable guidance for advising patients and their families.
However, previous researchers reported the association between tumor size and tumor extension on the visual prognosis.Citation19,Citation25,Citation26 In the present study, neither size nor extension, as classified by Hardy and Knops, influenced the visual outcome. Possibly, a larger tumor size may receive a timely operation, potentially diluting the actual correlation between size and outcomes. Additionally, Ng et al proposed that the tumor height from the supracarotid artery correlated more closely with the visual outcome rather than the absolute height of the tumor.Citation26 Further studies evaluating the influences of all extensions on imaging will greatly expand our comprehensive understanding of this aspect.
Onset duration is only a predictor of poor visual recovery. While vascular density and the ganglion cell complex showed immediate improvement after TSS at 48 hours post-surgery, the RNFL thickness remained unchanged, suggesting permanent structural damage resulting from delayed decompression.Citation20,Citation27 In several cases, improvements eventually occur despite the prolonged onset of symptoms. This apparent contradiction may be linked to the slow growth of these tumors, affording the optic nerve sufficiently adapts to the structural change.Citation28 This suggested role of optic nerve plasticity, a factor intricately linked with genetic factors among patients, has contributed to diverse adaptive responses of the optic nerve and recovery, further influencing postoperative visual outcome.Citation29 Our result is in accordance with the previous studies.Citation9,Citation14,Citation20,Citation30 In Asian population, Sriram et al reported that PA patients with a 1-month onset duration after post-transcranial or TSS operatively achieved better outcome than the longer group.Citation14 Moreover, Jahangiri et al identified a delay onset of 6 months as a risk factor for poor visual outcome in the older age group.Citation31 Therefore, despite the old age patients, postoperative visual outcome can still improve. Hence, we suggest that older patients who are good candidates for surgery should receive a timely operation to increase their chances of achieving good vision.
The initial visual parameters have been investigated as potential determinants of postoperative visual outcomes in various studies.Citation9,Citation16,Citation19 However, inconclusive findings have been reported.Citation32 Our results indicate that the initial VA showed no significant impact on improvement in the multivariable analysis. However, we observe a potential statistically inverse correlation (p = 0.091), suggesting that worse initial VA might be associated with more improvement postoperatively. This could have resulted from misclassification bias of the cut-point for improvement with 0.2 logMAR. Consequently, it is conceivable that a patient with a worse preoperative VA, even with a minute improvement, could result in a substantial improvement in logMAR but may not result in clinically meaningful improvement. For instance, an individual with an initial VA of no perception of light (NPL) – logMAR 3.4 improves to a postoperative VA of perception of light (PL) – logMAR 3.1 demonstrating an improvement of 0.3. This comparison contrasts with another subgroup with a more favorable visual outcome, such as those achieving from 20/25 to 20/20, where the observed improvement is only 0.1 logMAR. While the magnitude of improvement in logMAR may not reflect the clinical significance of visual improvement, and the chosen improvement threshold could potentially skew result interpretation. Moreover, patients with worse initial VA tend to seek earlier medical care. Early intervention for patients with poor initial VA may afford an opportunity for timely surgical management. Lastly, the exclusive inclusion of patients from an ophthalmic outpatient department leads to potential selection bias and over-representing those with initially poor VA in our cohort.
Some previous researchers revealed no different treatment efficacy among the surgical approaches in the Asian PA patients.Citation14 The visual outcome of TSS or transcranial approach groups was unremarkable on the experienced surgeons or centers.Citation33 However, several recent meta-analysis studies of PA reported the significantly better visual outcome of the TSS group.Citation34–36 In our series, most of the patients received TSS. Although TSS did not emerge as a statistically significant variable in predicting a favorable visual outcome in logistic regression analysis, an interesting observation was noted; VA improvement was faster at the 1-month follow-up in the TSS approach compared to the 6-month interval observed in the transcranial approach. Conversely, the transcranial approach demonstrated a slight improvement at 1–6-month period in contrast to TSS approach, which maintained stable VA after an initial improvement at the 1-month visit. This suggests a delayed improvement that can still occur in the transcranial approach. A similar pattern was observed in VF, where improvement persisted beyond the 6-month postoperative period in the transcranial approach, despite lacking statistical significance. In general, transsphenoidal approach is preferred due to lower postoperative complications and is the approach of choice if there are no contraindications and suitable preoperative imaging, such as no large suprasellar extension. In cases with giant adenoma that would be difficult to resect due to suprasellar extension, subtotal resection resulting from choosing the transsphenoidal approach can lead to postoperative swelling of the tumor and infarction, which can be life-threatening.Citation37 This highlights the importance of careful preoperative planning. One explanation for poorer visual outcomes generally observed in the transcranial approach is the more complex and aggressive nature of tumors. However, it allows for superior exposure, enabling more effective separation of the tumor from adjacent structure compared to the transsphenoidal approach.Citation38 The involvement of the optic nerve often requires meticulous resection and careful separation of the tumor while balancing degree of the optic nerve damage. This manipulation of the optic nerve could account for the delayed improvement in visual parameters observed in our cohort. We proposed that conducting a subsequent study with larger sample size would be valuable for comprehensively evaluating the impact of surgical techniques on visual outcome across short- and long-term period.
Several limitations should be addressed in the present study. Firstly, due to the retrospective nature, certain data were incomplete largely, visual parameter and patients with follow-up time of less than 1 year. Consequently, they were excluded from the cohort, contributing to a reduction in statistical power. Moreover, the unavailability of OCT data in majority of patients presents a notable limitation in our study. As a result, we decided not to evaluate OCT-related. This omission compromise aspects associated with the thinning of the RNFL and macular ganglion cell layer (GCL) in PA with chiasmal compression.Citation39–41 Secondly, the study did not account for the influence of multiple surgeons. This absence likely impacted the true postoperative prognosis, given the potential variability in surgical skills among different surgeons. Existing literature has observed only marginal improvements in vision beyond the 2-years postoperative period.Citation42 Thus, the nearly 50 months follow-up time in our cohort is considered sufficient to serve as a representative timeframe for assessing the long-term visual outcome. This study represents the first investigation within the Thai population examining the visual prognosis over a prolonged follow-up period. Our finding revealed that a prolonged duration is identified as the significant risk of poor visual outcome in Thai PA patients. This emphasized the importance of timely diagnosis and prompt treatment for improving vision outcomes in this population.
Conclusion
Both TSS and Transcranial are effective operations for patients with PA. Patients with a prolonged onset duration should be considered for a prompt operation, accompanied by thorough suggestions regarding the likelihood of a poor postoperative visual outcome.
Disclosure
The authors report no conflicts of interest in this work.
References
- Jho DH, Biller BM, Agarwalla PK, Swearingen B. Pituitary apoplexy: large surgical series with grading system. World Neurosurg. 2014;82(5):781–790. doi:10.1016/j.wneu.2014.06.005
- Giritharan S, Gnanalingham K, Kearney T. Pituitary apoplexy - bespoke patient management allows good clinical outcome. Clin Endo. 2016;85(3):415–422. doi:10.1111/cen.13075
- Singh TD, Valizadeh N, Meyer FB, Atkinson JL, Erickson D, Rabinstein AA. Management and outcomes of pituitary apoplexy. J Neurosurg. 2015;122(6):1450–1457. doi:10.3171/2014.10.JNS141204
- Chanson P, Wolf P. Clinically non-functioning pituitary adenomas. Presse Med. 2021;50(4):104086. doi:10.1016/j.lpm.2021.104086
- Uy B, Wilson B, Kim WJ, Prashant G, Bergsneider M. Visual Outcomes After Pituitary Surgery. Neurosurg Clin N Am. 2019;30(4):483–489. doi:10.1016/j.nec.2019.06.002
- Abouaf L, Vighetto A, Lebas M. Neuro-ophthalmologic exploration in non-functioning pituitary adenoma. Ann Endocrinol. 2015;76(3):210–219. doi:10.1016/j.ando.2015.04.006
- Buchfelder M, Schlaffer SM, Zhao Y. The optimal surgical techniques for pituitary tumors. Best Pract Res Clin Endocri Metab. 2019;33(2):101299. doi:10.1016/j.beem.2019.101299
- Park SH, Kang MS, Kim SY, et al. Analysis of factors affecting visual field recovery following surgery for pituitary adenoma. Int Ophthalmol. 2021;41(6):2019–2026. doi:10.1007/s10792-021-01757-6
- Sun M, Zhang ZQ, Ma CY, Chen SH, Chen XJ. Predictive factors of visual function recovery after pituitary adenoma resection: a literature review and Meta-analysis. Int J Ophthalmol. 2017;10(11):1742–1750. doi:10.18240/ijo.2017.11.17
- Moon CH, Hwang SC, Kim BT, Ohn YH, Park TK. Visual prognostic value of optical coherence tomography and photopic negative response in chiasmal compression. Invest Ophthalmol Vis Sci. 2011;52(11):8527–8533. doi:10.1167/iovs.11-8034
- Grković D, Bedov T. Outcome of visual acuity after surgical removal of pituitary adenomas. Srp Arh Celok Lek. 2013;141(5–6):296–303. doi:10.2298/SARH1306296G
- Thotakura AK, Patibandla MR, Panigrahi MK, Addagada GC. Predictors of visual outcome with transsphenoidal excision of pituitary adenomas having suprasellar extension: a prospective series of 100 cases and brief review of the literature. Asian J Neurosurg. 2017;12(1):1–5. doi:10.4103/1793-5482.149995
- Butenschoen VM, Schwendinger N, von Werder A, et al. Visual acuity and its postoperative outcome after transsphenoidal adenoma resection. Neurosurg Rev. 2021;44(4):2245–2251. doi:10.1007/s10143-020-01408-x
- Sriram PR, Sellamuthu P, Ghani ARI. Factors affecting visual field outcome post-surgery in sellar region tumors: retrospective study. Malays J Med Sci. 2017;24(6):58–67.
- Johnson LN, Guy ME, Krohel GB, Madsen RW. Levodopa may improve vision loss in recent-onset, nonarteritic anterior ischemic optic neuropathy. Ophthalmology. 2000;107(3):521–526. doi:10.1016/s0161-6420(99)00133-5
- Lee DK, Sung MS, Park SW. Factors influencing visual field recovery after transsphenoidal resection of a pituitary adenoma. Korean J Ophthalmol. 2018;32(6):488–496. doi:10.3341/kjo.2017.0094
- Mohr G, Hardy J, Comtois R, Beauregard H. Surgical management of giant pituitary adenomas. Can J Neurol Sci. 1990;17(1):62–66. doi:10.1017/S0317167100030055
- Knosp E, Kitz K, Steiner E, Matula C. Pituitary adenomas with parasellar invasion. Acta Neurochir Suppl. 1991;53:65–71.
- Ho RW, Huang HM, Ho JT. The influence of pituitary adenoma size on vision and visual outcomes after trans-sphenoidal adenectomy: a report of 78 cases. J Korean Neurosurg Soc. 2015;57(1):23–31. doi:10.3340/jkns.2015.57.1.23
- Tagoe NN, Essuman VA, Bankah P, et al. Visual outcome of patients with pituitary adenomas following surgery and its contributory factors at a tertiary hospital in Ghana. Ethiop J Health Sci. 2019;29(1):895–902. doi:10.4314/ejhs.v29i1.11
- Taghvaei M, Sadrehosseini SM, Ostadrahimi N, Sarraf P, Zeinalizadeh M. Preoperative visual evoked potential in the prediction of visual outcome after pituitary macroadenomas surgery. Pituitary. 2019;22(4):397–404. doi:10.1007/s11102-019-00969-5
- Watanabe T, Uehara H, Takeishi G, et al. Characteristics of preoperative visual disturbance and visual outcome after endoscopic endonasal transsphenoidal surgery for nonfunctioning pituitary adenoma in elderly patients. World Neurosurg. 2019;126:e706–e12. doi:10.1016/j.wneu.2019.02.132
- Lu Y, Brommer B, Tian X, et al. Reprogramming to recover youthful epigenetic information and restore vision. Nature. 2020;588:(7836):124–9. doi:10.1038/s41586-020-2975-4
- Gnanalingham KK, Bhattacharjee S, Pennington R, Ng J, Mendoza N. The time course of visual field recovery following transphenoidal surgery for pituitary adenomas: predictive factors for a good outcome. J Neurol Neurosurg Psych. 2005;76(3):415–419. doi:10.1136/jnnp.2004.035576
- Luomaranta T, Raappana A, Saarela V, Liinamaa MJ. Factors affecting the visual outcome of pituitary adenoma patients treated with endoscopic transsphenoidal surgery. World Neurosurg. 2017;105:422–431. doi:10.1016/j.wneu.2017.05.144
- Ben Chat Fong N, Mak CH, Steffi CSY, Wing SK, Shing TT, Ching CF. A factorial analysis on visual outcomes of transsphenoidal surgery for pituitary macroadenoma. Asian J Neurosurg. 2022;17(2):280–285. doi:10.1055/s-0042-1751011
- Cennamo G, Solari D, Montorio D, et al. Early vascular modifications after endoscopic endonasal pituitary surgery: the role of OCT-angiography. PLoS One. 2020;15(10):e0241295. doi:10.1371/journal.pone.0241295
- Hamblin R, Fountas A, Lithgow K, et al. Natural history of non-functioning pituitary microadenomas: results from the UK non-functioning pituitary adenoma consortium. Eur J Endocrinol. 2023;189(1):87–95. doi:10.1093/ejendo/lvad070
- Frangeul L, Pouchelon G, Telley L, Lefort S, Luscher C, Jabaudon D. A cross-modal genetic framework for the development and plasticity of sensory pathways. Nature. 2016;538(7623):96–98. doi:10.1038/nature19770
- Cohen AR, Cooper PR, Kupersmith MJ, Flamm ES, Ransohoff J. Visual recovery after transsphenoidal removal of pituitary adenomas. Neurosurgery. 1985;17(3):446–452. doi:10.1227/00006123-198509000-00008
- Jahangiri A, Lamborn KR, Blevins L, Kunwar S, Aghi MK. Factors associated with delay to pituitary adenoma diagnosis in patients with visual loss. J Neurosurg. 2012;116(2):283–289. doi:10.3171/2011.6.JNS101663
- Powell M. Recovery of vision following transsphenoidal surgery for pituitary adenomas. Br J Neurosurg. 1995;9(3):367–374. doi:10.1080/02688699550041377
- Mishra S, Mishra RC, Gurjar HK, Garg K. Transcranial surgery for pituitary tumors: A “community neurosurgery experience”. Neurol India. 2022;70(5):2039–2046. doi:10.4103/0028-3886.359173
- Chen J, Liu H, Man S, et al. Endoscopic vs. microscopic transsphenoidal surgery for the treatment of pituitary adenoma: A meta-analysis. Front Surg. 2021;8:806855. doi:10.3389/fsurg.2021.806855
- Guo S, Wang Z, Kang X, Xin W, Li X. A meta-analysis of endoscopic vs. microscopic transsphenoidal surgery for non-functioning and functioning pituitary adenomas: Comparisons of efficacy and safety. Front Neurol. 2021;12:614382. doi:10.3389/fneur.2021.614382
- Yu SY, Du Q, Yao SY, et al. Outcomes of endoscopic and microscopic transsphenoidal surgery on non-functioning pituitary adenomas: a systematic review and meta-analysis. J Cell Mol Med. 2018;22(3):2023–2027. doi:10.1111/jcmm.13445
- Sinha S, Sharma BS. Giant pituitary adenomas--an enigma revisited. Microsurgical treatment strategies and outcome in a series of 250 patients. Br J Neurosurg. 2010;24(1):31–39. doi:10.3109/02688690903370305
- Toader C, Bratu BG, Mohan AG, Bentia D, Ciurea AV. comparison of transcranial and transsphenoidal approaches in intra and suprasellar pituitary adenomas - systematic review. Acta Endocrinol. 2023;19(2):228–233. doi:10.4183/aeb.2023.228
- Cennamo G, Solari D, Montorio D, et al. The role of OCT- angiography in predicting anatomical and functional recovery after endoscopic endonasal pituitary surgery: a 1-year longitudinal study. PLoS One. 2021;16(12):e0260029. doi:10.1371/journal.pone.0260029
- Sun M, Zhang Z, Ma C, Chen S, Chen X. Quantitative analysis of retinal layers on three-dimensional spectral-domain optical coherence tomography for pituitary adenoma. PLoS One. 2017;12(6):12.
- Glebauskiene B, Liutkeviciene R, Zlatkute E, Kriauciuniene L, Zaliuniene D. Association of retinal nerve fibre layer thickness with quantitative magnetic resonance imaging data of the optic chiasm in pituitary adenoma patients. J Clin Neurosci. 2018;50:1–6. doi:10.1016/j.jocn.2018.01.005
- Uvelius E, Valdemarsson S, Bengzon J, Hammar B, Siesjö P. Visual acuity in patients with non-functioning pituitary adenoma: Prognostic factors and long-term outcome after surgery. Brain Spine. 2023;3:102667. doi:10.1016/j.bas.2023.102667