
Abstract
Purpose
The purpose of this study was to assess preliminary real-world outcomes in neovascular age-related macular degeneration (nAMD) and diabetic macular edema (DME) treated with intravitreal faricimab.
Patients and Methods
This was a retrospective, observational consecutive-case real-world study of patients with nAMD or DME initiated on intravitreal faricimab between November 2022 and April 2023. Treatment-naïve patients and patients previously treated with alternate anti-vascular endothelial growth factor (anti-VEGF) agents were initiated on an intended treatment plan of four monthly faricimab injections as a loading regime. Efficacy was assessed across four treatment groups. Primary outcomes assessed for both cohorts were changes in best corrected visual acuity (BCVA) and central subfield thickness (CST) on optical coherence tomography (OCT). Secondary outcomes were alterations in OCT-defined structural features.
Results
From 127 patients, 146 eyes received at least one dose of faricimab. Mean BCVA, measured in Early Treatment of Diabetic Retinopathy Study (ETDRS) letters, from baseline to fifth visit increased from: 59.0±12.8 to 62.2±14.3 in treatment-naïve nAMD; 61.1±17.6 to 63.5±14.8 in previously-treated nAMD; 61.1±13.0 to 72.8±11.5 in treatment-naïve DME; and 60.8±14.6 to 63.3±15.6 in previously-treated DME. Mean CST reduced in all four treatment groups between initiation to final loading dose, from: 442.8±172.0µm to 305.2±117.0µm (p<0.0001) in treatment-naïve nAMD; 355.2±115.1µm to 297.9±92.54µm (p<0.0001) in previously-treated nAMD; 465.8±109.1µm to 343.1±100.3µm (p<0.0001) in treatment-naïve DME; and 492.5±133.1µm to 388.5±131.4µm (p<0.0001) in previously-treated DME.
Conclusion
Real-world outcomes showed some improvement in BCVA and CST for nAMD and DME following faricimab administration, including in patients previously treated with other anti-VEGF agents. Further work involving larger cohorts over longer periods is required to determine whether improvement is maintained, and if intervals can be extended to match those observed in clinical trials.
Introduction
Neovascular age-related macular degeneration (nAMD) is one of the leading causes of blindness worldwide, with global prevalence projected to increase from 196 million in 2020 to 288 million in 2040.Citation1 Anti-vascular endothelial growth factor (anti-VEGF) intravitreal injections are the mainstay of treatment for nAMD; anti-VEGF treatment reduces vascular permeability preventing accumulation of sub-retinal and intraretinal fluidCitation2 and demonstrates an acceptable safety profile.Citation3 Due to the short duration of action of anti-VEGF agents and persistent disease activity of nAMD, treatment usually remains frequent and spans several years in order for therapeutic effects to be maintained.Citation4 Diabetic macular edema (DME) affects around 7% of patients with diabetes and is one of the leading causes of preventable vision loss in this patient population.Citation5,Citation6 In the United Kingdom (UK), intravitreal treatment with anti-VEGF is the first-line therapy for individuals exhibiting center-involving DME with a central subfield thickness (CST) of >400µm.Citation7 Results from clinical trials have demonstrated that the use of anti-VEGF leads to improvements in visual acuity and anatomical optical coherence tomography (OCT) findings, whilst retaining a relatively small side effect profile.Citation8–10 The need for frequent intravitreal treatment places a significant treatment burden upon both patients and their caregivers in addition to hospital services. This is indeed one factor that may limit real-world efficacy compared with clinical trial outcomes for both nAMD and DME.Citation11,Citation12
Faricimab (Roche/Genentech, Switzerland) is a new anti-VEGF agent that inhibits both angiopoietin-2 (Ang-2) and VEGF-A. Ang-2 production results in inflammation and vascular leakage and contributes to neovascularization.Citation13 Its blockade stabilizes the endothelium and reduces pericyte loss,Citation14 thereby conferring alternate mechanisms to anti-VEGF-A in the treatment of both nAMD and DME. In the TENAYA and LUCERNE Phase III clinical trials for nAMD, faricimab demonstrated non-inferiority to aflibercept and ranibizumab.Citation15 Robust vision gains and anatomical improvements were achieved and sustained with faricimab injection intervals of up to 16 weeks. In the YOSEMITE and RHINE clinical trials for DME, faricimab showed non-inferiority compared to aflibercept at 8-weekly intervals and demonstrated promising vision gains at dosing intervals of up to 16 weeks, compared to aflibercept every 8 weeks. It was also found to have a comparable safety profile compared to aflibercept in this cohort.Citation16
Results from clinical trials may not always translate to real-world clinical practice,Citation17,Citation18 and there is a paucity of UK data regarding real-world outcomes of faricimab. Existing real-world studies exploring the safety and efficacy of faricimab for nAMDCitation19–24 and DMECitation25–27 mostly examine outcomes in patients with a prior treatment history, and are not based in the UK. One UK study comprising 11 eyes with previously-treated DME observed significant improvements in visual acuity and CST after a month of faricimab,Citation28 and another comprising 81 treatment-switched nAMD eyes from aflibercept found improvements in CST without significant improvement in vision.Citation29 The response in those previously treated requires further evaluation to confirm the utility of switching patients to faricimab treatment. In our unit, patients were considered for switched treatment to faricimab if they demonstrated suboptimal structural outcomes and/or requirement for frequent intravitreal treatment. Therefore, we designed a retrospective study to evaluate the initial efficacy of intravitreal faricimab in patients being treated for nAMD or DME (inclusive of both those treatment-naïve and previously-treated) in a real-world setting.
Materials and Methods
Study Design
A retrospective review of consecutive patients who had received their first dose of intravitreal faricimab, in accordance with NICE criteria, for treatment of their nAMD or DME at the Royal Free London NHS Foundation Trust, was performed. No exclusion criteria were implemented. Patients were included in visual outcome analysis if they had a minimum of 4-week follow-up after faricimab initiation and in analysis of structural outcomes if they had two OCT scans performed at least 4 weeks apart. This study was registered with the audit department at the Royal Free Hospital and was performed in accordance with the tenets of the Declaration of Helsinki.
Treatment Regimen
All patients were treated with at least one dose of intravitreal 6mg faricimab (Genentech, Roche), with the first dose delivered between 1 November 2022 and 1 April 2023. Prior to this, all patients underwent complete ophthalmological assessment, including best corrected visual acuity (BCVA), slit lamp examination and macular OCT imaging (Heidelberg Engineering, Heidelberg, Germany; Topcon DRI OCT Triton plus; Tokyo, Japan). Patients were treated with a loading protocol of faricimab with four injections, spaced approximately one month apart.
Study Outcomes
Data collected included the following: demographics (gender, age, ethnicity); treatment history, if applicable (number of previous treatments, type of previous treatments); BCVA; OCT findings (central subfield thickness, CST; presence/absence of retinal fluid [intraretinal, IRF; subretinal, SRF; sub-retinal pigment epithelium, sub-RPE; presence of pigment epithelial detachment, PED]; subretinal hyper-reflective material, SRHM; hyper-reflective foci; diffuse retinal thickening; or hemorrhage). BCVA was collected at each visit and OCTs were examined at initiation visit and final loading dose visit (number four). Where OCTs were not available for final loading dose visit, OCT from timepoint nearest to that visit was assessed instead. Retinal segmentation was manually checked to ensure the inner and outer retina boundaries had not been inaccurately marked due to anatomical change.
Continuous variables were expressed as mean±standard deviation, and binary categorical variables were expressed as frequency (percentage of total population). Two-way ANOVA tests were used to compare BCVAs, Wilcoxon signed rank test was used to compare CSTs, and Fisher’s test was used for comparison of OCT structural findings. All statistical analyses were performed using GraphPad Prism (Version 5). Statistical significance was defined as p<0.05.
Results
Demographics
One-hundred-and-twenty-seven individuals, accounting for a total of 146 eyes, received an initiation dose of faricimab between 1 November 2022 and 1 April 2023 for treatment of their nAMD or DME and returned for at least one follow-up visit. This included 74 eyes of 69 patients with nAMD and 72 eyes of 58 patients with DME. The average age was 82.6±7.9, with a range of 59–97 years for nAMD, and 62.6±12.3, with a range of 29–96 for DME. Fifty per cent of patients were female. Further demographic details of patients who had received follow-up after one injection of faricimab are provided in .
Table 1 Demographics and Baseline Characteristics of Our Cohort of 127 Individuals
Efficacy of Faricimab in nAMD
Of those AMD eyes receiving faricimab, 35 (49.3%) were treatment-naïve, with a mean BCVA of 59.0±12.8 letters at first visit (). At subsequent loading visits spaced a minimum of 4 weeks apart, BCVA was 60.5±14.5 at second visit, 57.9±16.2 at third visit, 57.9±17.2 at fourth visit (final loading dose), and 62.2±14.3 at fifth visit, with no significant difference found between visits (). This was accompanied by a significant mean CST reduction from 442.8±172.0µm at first visit to 305.2±117.0µm at fourth visit (p<0.0001, ). The mean number of injections given to treatment-naïve individuals with nAMD over the study period was 4.5±0.9.
Table 2 Mean BCVA and Visit Intervals for Treatment-Naïve and Previously-Treated nAMD Patients
Figure 1 Best-corrected visual acuity (BCVA) and central subfield thickness (CST) in patients with neovascular age-related macular degeneration (nAMD) treated with faricimab. (A) Mean BCVA in treatment-naïve patients at visits 1 (baseline), 2, 3, 4 and 5, with each visit spaced at least 4 weeks apart. (B) Mean BCVA in previously-treated patients at visits 1 (baseline), 2, 3, 4 and 5, with each visit spaced at least 4 weeks apart. (C) Mean CST in treatment-naïve patients at initial and final loading dose visits. (D) Mean CST in previously-treated patients at initial and final loading dose visits.
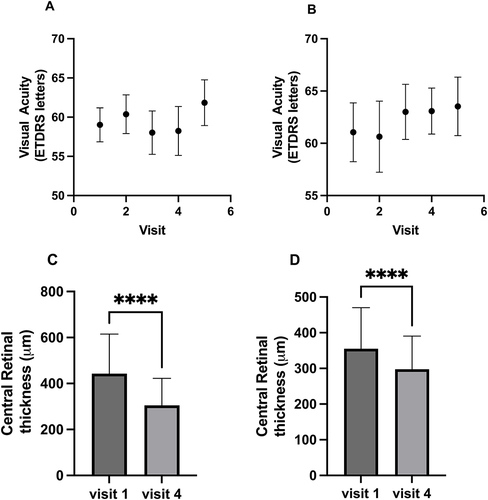
In the cohort of 39 (52.7%) individuals who had switched from any anti-VEGF, mean interval from previous anti-VEGF agent was 7.1±3.3 weeks, with a median interval of 6 (range: 5–8) weeks. Mean BCVA at first visit was 61.1±17.6 letters. At second visit, BCVA was 60.6±21.0 letters, and increased on subsequent visits three, four, and five to 63.0±15.4, 63.1±13.1 and 63.5±14.8, respectively (). Mean CST reduced from 355.2±115.1µm at first visit to 297.9±92.5µm at fourth visit (p<0.0001, ). The mean number of injections given was 4.4±1.0.
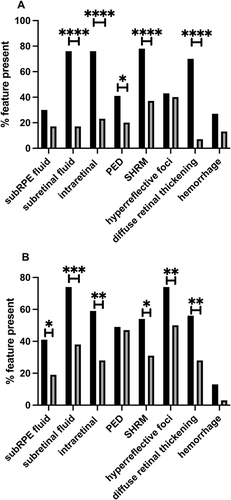
After faricimab treatment, OCTs demonstrated improvements in and resolution of all anatomical parameters assessed (). In treatment-naïve patients (), reductions were demonstrated in a proportion of patients exhibiting the presence of sub-RPE fluid (31.4% to 17.2%), SRF (74.3% to 17.2%), IRF (74.3% to 24.1%), PED (40.0% to 20.7%), SRHM (77.1% to 37.9%), hyper-reflective foci (42.9% to 41.4%), diffuse retinal thickening (68.6% to 6.9%) and hemorrhage (28.6% to 13.8%). These reductions were significant for SRF, IRF, presence of PED, SRHM and diffuse retinal thickening (p<0.05). In patients who had previously received other anti-VEGF (), the proportion of individuals exhibiting anatomical features of nAMD activity also reduced in all parameters assessed: sub-RPE fluid (41.0% to 18.8%), SRF (74.4% to 37.5%), IRF (59.0% to 28.1%), PED (48.7% to 46.9%), SRHM (53.8% to 31.3%), hyper-reflective foci (74.4% to 50.0%), diffuse retinal thickening (56.4% to 28.1%) and hemorrhage (12.8% to 3.1%). These reductions were significant for all forms of retinal fluid, presence of SHRM, hyper-reflective foci and diffuse retinal thickening (p<0.05).
Figure 2 Qualitative changes in optical coherence tomography (OCT)-defined structural features of disease activity in patients with neovascular age-related macular degeneration (nAMD) after at least one injection of faricimab. (A) Proportions of treatment-naïve patients with OCT-derived structural markers of disease activity at visit 1 and visit 4. (B) Proportions of patients treated previously with anti-vascular endothelial growth factor agents exhibiting various markers of disease activity on OCT at visit 1 and visit 4.
Efficacy of Faricimab in DME
Of those DME eyes receiving faricimab, 33 (45.8%) were treatment-naïve, with a mean BCVA of 61.1±13.0 letters at first visit (). Improvements in mean BCVA were observed at subsequent second, third, fourth and fifth visits, with mean BCVA increasing to 66.5±13.4, 68.4±14.9, 67.4±14.4 and 72.8±11.5 letters, respectively (). This was accompanied by a significant decrease in mean CST from 465.8±109.1µm at visit one to 343.1±100.3µm at visit four (p<0.0001, ). The mean number of faricimab injections given to treatment-naïve eyes with DME was 4.4±0.8.
Table 3 Mean BCVA and Visit Intervals for Treatment-Naïve and Previously-Treated DME Patients
Figure 3 Best-corrected visual acuity (BCVA) and central subfield thickness (CST) within patients with diabetic macular edema (DME) treated with faricimab. (A) Mean BCVA in treatment-naïve patients at visits 1 (baseline), 2, 3, 4 and 5, with each visit spaced at least 4 weeks apart. (B) Mean BCVA in previously-treated patients at visits 1 (baseline), 2, 3, 4 and 5, with each visit spaced at least 4 weeks apart. (C) Mean CST in treatment-naïve patients at initial and final loading dose visits. (D) Mean CST in previously-treated patients at initial and final loading dose visits.
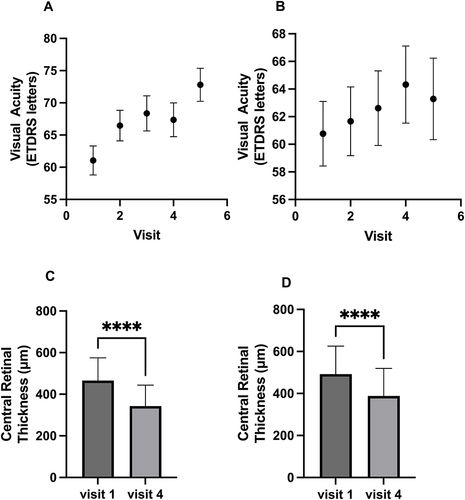
In DME patients who had received previous anti-VEGF agents, mean interval from previous anti-VEGF agent was 30.5±52.1 weeks, with a median interval of 9.0 weeks (range: 5.5–24.5). Improvements in mean BCVA compared to the baseline of 60.8±14.6 letters were also seen: at second, third, fourth and fifth visit, mean BCVA had improved to 61.7±15.5, 62.6±16.2, 64.3±17.0 and 63.3±15.6, respectively (). Mean CST reduced significantly from 492.5±133.1µm at initiation visit to 388.5±131.4µm at fourth visit (p<0.0001, ). The mean number of injections given was 4.7±0.7.
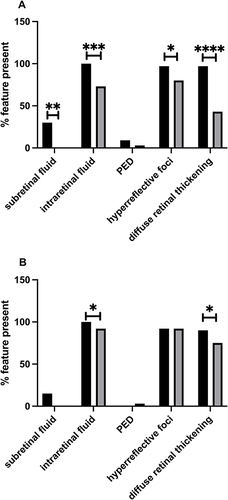
For anatomical outcomes, DME patients also showed improvements in OCT-derived qualitative features assessed. In treatment-naïve patients, improvements were observed in all parameters assessed (), with reductions in proportions of patients exhibiting features of disease activity: SRF (30.3% to 0.0%), IRF (100% to 73.3%), PED (9.1% to 3.3%), hyper-reflective foci (97.0% to 80.0%) and diffuse retinal thickness (97.0% to 43.3%). These reductions were significant (p<0.05) for all qualitative parameters except for PED. In pre-treated patients, improvements in a proportion of patients were also observed but to a lesser degree (): SRF (15.4% to 0.0%), IRF (100% to 91.7%), hyper-reflective foci (92.3% to 91.7%) and diffuse retinal thickening (89.7% to 75.0%). One individual developed a new PED (0.0% to 2.8%). The reductions were significant for IRF and diffuse retinal thickening (p<0.05).
Figure 4 Qualitative changes in optical coherence tomography (OCT)-defined structural features of disease activity in patients with diabetic macular edema (DME) treated with faricimab. (A) Proportions of treatment-naïve patients exhibiting various markers of disease activity at visits 1 and 4. (B) Proportions of patients treated with previous anti-VEGF agents exhibiting various markers of disease activity on OCT at visits 1 and 4.
Discussion
The aims of this study were to determine the outcomes of faricimab treatment for treatment-naïve and previously-treated patients with nAMD and DME in a real-world clinical setting within the UK National Health Service. Patients were treated with four initial loading injections of faricimab.
In nAMD, for both untreated and treatment-switched patients, BCVA improved following the loading regime. OCT showed significant improvements in CST and other anatomical markers of disease activity for both groups. In DME, similar findings were observed. Mean BCVA increased following a loading regime of faricimab in both treatment-naïve and treatment-switched patients, although this was only significant for the treatment-naive group. These improvements in vision were also accompanied by a significant reduction of CST across the DME cohort and notable reductions in the presence of DME markers of disease activity, especially in the treatment-naïve group.
In this study looking at 146 eyes in 127 individuals, nAMD and DME eyes each comprised around half of the cohort; that is, similar numbers of treatment-naïve and pre-treated eyes were assessed. This differed from the YOSEMITE and RHINE trials, which limited their previously-treated study eyes to 25% of the total enrolment.Citation16 Interestingly, of the total cohort, there were more females (69.6%) in the nAMD subgroup and more males (70.7%) in the DME subgroup. This is in keeping with a previous meta-analysis showing that women have a slightly higher risk of nAMD compared to men.Citation30 Although studies have not reported on gender associations with DME, males exhibit a higher prevalence of severe diabetic retinopathy,Citation31 which relates to poor metabolic control in diabetes and subsequent diabetic maculopathy.
Our cohort demonstrated vision gains across both treatment groups, though these were to a lesser extent than those of clinical trials for faricimab. Vision gains were most comparable for the treatment-naïve DME cohort and clinical trials, with a mean increase in BCVA of over 10 letters by the fifth clinical visit. The differences for the other treatment groups may have been partly due to the intervals between loading doses being larger than four weeks. The fourth loading dose across all patient groups for nAMD and DME was delivered at a mean interval of five or more weeks, and notably in the DME pre-treated cohort, all loading doses had a mean interval of five weeks or more. This is a reflection of the high variability of patient adherence in a real-world setting, which itself tends to decline with increasing time from first injection.Citation32 This may have allowed for retinal fluid to reaccumulate and a lack of optimal increments in BCVA to be observed. Delayed follow-up visits have been shown to negatively impact BCVA in nAMD, even despite later re-treatment and normalization of CST.Citation33 Furthermore, there were differences in the spread of ethnicities between our population compared to that of the faricimab clinical trials,Citation16 with a lower proportion of ethnically White individuals within our cohort (75.3% in our nAMD cohort versus >80% in TENAYA/LUCERNE; 56.9% in our DME cohort versus >75% in YOSEMITE/RHINE). The varied responses of different ethnicities to anti-VEGF treatments have not been well-explored, but it has been shown that DME treatment outcomes can differ based upon racial and socioeconomic status, with White patients likely to undergo more frequent anti-VEGF injections than those in certain other ethnic groups.Citation34
Owing to our use of real-world data, this study’s strength is its ability to report on the routine care received by patients outside of a controlled, clinical trial setting. Our results are more likely to be generalizable to the ethnically diverse patient population in London, and reflective of real-world clinical outcomes. However, the limitations of this study include its retrospective design. Visits did not always occur at the stipulated loading dose intervals of four weeks, meaning equivalent visits for different patients may have been accompanied by greater differences in BCVA if treatment intervals were larger than intended. This situation is common in real-world settings where strict treatment intervals are not always maintained. Furthermore, OCT scans were not always performed at the fourth loading dose visit, and instead were taken from the third loading dose visit, or a later visit. This may have affected the visualization of anti-VEGF effects on anatomical outcomes. There are also different OCT platforms used in our clinics which can contribute to different CRT measurements.
Nevertheless, this study produced promising functional and anatomical results from real-world use of faricimab at several clinical sites under the same London hospital trust. Further studies are needed to comment on longer-term efficacy and safety outcomes of faricimab to establish whether improvements can be maintained. Additionally, as the aim of introducing faricimab is to provide an alternative anti-VEGF agent with the possibility of longer treatment intervals than current mainstay therapies, it would also be worthwhile to compare outcomes in treatment-switched individuals treated at intervals matched and unmatched to their prior anti-VEGF agent.
Conclusion
Intravitreal faricimab, when used in both treatment-naïve or previously-treated nAMD and DME patients in our real-world setting, demonstrated improvements in BCVA and structural OCT findings. Larger studies spanning longer observation periods will be useful for determining the long-term efficacy and safety of faricimab, including its potential for longer treatment intervals.
Ethics Approval and Consent to Participate
This was a retrospective audit registered with the Royal Free Hospital Audit Department following study conception and prior to initiation of data collection. Informed consent was obtained from all participants as part of standard treatment of care.
Author Contributions
DH and NQXQ were responsible for initial study conception and design. NQXQ, KMAAJ and LA were responsible for data collection. DH, NQ, KMAAJ and LA were responsible for data analysis and interpretation. The first draft of the manuscript was written by NQ and all authors took part in revising or critically reviewing the article. All authors read and approved the final manuscript, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
Dr Hanumunthadu has financial competing interests in the form of consultancy fees from Bayer and Roche. The authors declare no other conflicts of interest in this work.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Wong WL, Su X, Li X, et al. Global prevalence of age-related macular degeneration and disease burden projection for 2020 and 2040: a systematic review and meta-analysis. Lancet Glob Health. 2014;2(2):e106–16. doi:10.1016/s2214-109x(13)70145-1
- Stahl A. The diagnosis and treatment of age-related macular degeneration. Dtsch Arztebl Int. 2020;117(29–30):513–520. doi:10.3238/arztebl.2020.0513
- Khanna S, Komati R, Eichenbaum DA, Hariprasad I, Ciulla TA, Hariprasad SM. Current and upcoming anti-VEGF Therapies and dosing strategies for the treatment of Neovascular AMD: a comparative review. BMJ Open Ophthalmol. 2019;4(1):e000398. doi:10.1136/bmjophth-2019-000398
- Chandra S, Arpa C, Menon D, et al. Ten-year outcomes of antivascular endothelial growth factor therapy in neovascular age-related macular degeneration. Eye. 2020;34(10):1888–1896. doi:10.1038/s41433-020-0764-9
- Lee R, Wong TY, Sabanayagam C. Epidemiology of diabetic retinopathy, diabetic macular edema and related vision loss. Eye and Vision. 2015;2(1):17. doi:10.1186/s40662-015-0026-2
- Yau JWY, Rogers SL, Kawasaki R, et al. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care. 2012;35(3):556–564. doi:10.2337/dc11-1909
- Amoaku WM, Ghanchi F, Bailey C, et al. Diabetic retinopathy and Diabetic Macular Oedema Pathways and Management: UK Consensus Working Group. Eye. 2020;34(S1):1–51. doi:10.1038/s41433-020-0961-6
- Nguyen QD, Brown DM, Marcus DM, et al. Ranibizumab for diabetic macular edema. Ophthalmology. 2012;119(4):789–801. doi:10.1016/j.ophtha.2011.12.039
- Brown DM, Schmidt-Erfurth U, Do DV, et al. Intravitreal aflibercept for diabetic macular edema. Ophthalmology. 2015;122(10):2044–2052. doi:10.1016/j.ophtha.2015.06.017
- Virgili G, Parravano M, Evans JR, Gordon I, Lucenteforte E. Anti-vascular endothelial growth factor for Diabetic Macular Oedema: a Network Meta-analysis. Cochrane Database Syst Rev. 2018;2018(10):CD007419. doi:10.1002/14651858.cd007419.pub6
- Spooner KL, Guinan G, Koller S, Hong T, Chang AA. Burden Of Treatment Among Patients Undergoing Intravitreal Injections For Diabetic Macular Oedema In Australia. Diabetes Metab Syndrome Obesity. 2019;12:1913–1921. doi:10.2147/dmso.s214098
- Okada M, Mitchell P, Finger RP, et al. Nonadherence or nonpersistence to intravitreal injection therapy for neovascular age-related macular degeneration. Ophthalmology. 2021;128(2):234–247. doi:10.1016/j.ophtha.2020.07.060
- Adamis AP, Brittain CJ, Dandekar A, Hopkins JJ. Building on the success of anti-vascular endothelial growth factor therapy: a vision for the next decade. Eye. 2020;34(11):1966–1972. doi:10.1038/s41433-020-0895-z
- Sharma A, Kumar N, Kuppermann BD, Bandello F, Loewenstein A. Faricimab: expanding horizon beyond VEGF. Eye. 2019;34(5):802–804. doi:10.1038/s41433-019-0670-1
- Heier JS, Khanani AM, Quezada Ruiz C, et al. Efficacy, durability, and safety of Intravitreal Faricimab up to every 16 weeks for neovascular age-related macular degeneration (Tenaya and Lucerne): two randomised, double-masked, phase 3, non-inferiority trials. Lancet. 2022;399(10326):729–740. doi:10.1016/s0140-6736(22)00010-1
- Wykoff CC, Abreu F, Adamis AP, et al. Efficacy, durability, and safety of Intravitreal Faricimab with extended dosing up to every 16 weeks in patients with diabetic macular oedema (YOSEMITE and RHINE): two randomised, double-masked, phase 3 trials. Lancet. 2022;399(10326):741–755. doi:10.1016/s0140-6736(22)00018-6
- Ciulla TA, Pollack JS, Williams DF. Visual acuity outcomes and anti-VEGF therapy intensity in diabetic MACULAR OEDEMA: a real-world analysis of 28 658 Patient Eyes. Br J Ophthalmol. 2020;105(2):216–221. doi:10.1136/bjophthalmol-2020-315933
- Holz FG, Tadayoni R, Beatty S, et al. Multi-country real-life experience of anti-vascular endothelial growth factor therapy for wet age-related macular degeneration. Br J Ophthalmol. 2014;99(2):220–226. doi:10.1136/bjophthalmol-2014-305327
- Rush RB. One-year outcomes of Faricimab treatment for AFLIBERCEPT-resistant neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:2201–2208. doi:10.2147/opth.s424315
- Leung EH, Oh DJ, Alderson SE, et al. Initial real-world experience with Faricimab in treatment-resistant neovascular age-related macular degeneration. Clin Ophthalmol. 2023;17:1287–1293. doi:10.2147/opth.s409822
- Khanani AM, Aziz AA, Khan H, et al. The real-world efficacy and safety of faricimab in neovascular age-related macular degeneration: the Truckee Study – 6 month results. Eye. 2023. doi:10.1038/s41433-023-02553-5
- Pandit SA, Momenaei B, Wakabayashi T, et al. Clinical outcomes of Faricimab in patients with previously treated neovascular age-related macular degeneration. Ophthalmol Retina. 2023. doi:10.1016/j.oret.2023.10.018
- Kataoka K, Itagaki K, Hashiya N, et al. Six-month outcomes of switching from AFLIBERCEPT to faricimab in refractory cases of neovascular age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2023;262(1):43–51. doi:10.1007/s00417-023-06222-x
- Szigiato A, Mohan N, Talcott KE, et al. Short-term outcomes of Faricimab in patients with neovascular age-related macular degeneration on prior Anti-VEGF Therapy. Ophthalmol Retina. 2024;8(1):10–17. doi:10.1016/j.oret.2023.08.018
- Rush RB. One year results of Faricimab for aflibercept-resistant diabetic macular edema. Clin Ophthalmol. 2023;17:2397–2403. doi:10.2147/opth.s424314
- Kusuhara S, Kishimoto-Kishi M, Matsumiya W, Miki A, Imai H, Nakamura M. Short-term outcomes of Intravitreal faricimab injection for diabetic macular edema. Medicina. 2023;59(4):665. doi:10.3390/medicina59040665
- Ohara H, Harada Y, Hiyama T, Sadahide A, Minamoto A, Kiuchi Y. Faricimab for diabetic macular edema in patients refractory to ranibizumab or aflibercept. Medicina. 2023;59(6):1125. doi:10.3390/medicina59061125
- Stanga PE, Valentín-Bravo FJ, Stanga SE, Reinstein UI, Pastor-Idoate S, Downes SM. Faricimab in neovascular AMD: first report of real-world outcomes in an independent Retina Clinic. Eye. 2023;37(15):3282–3289. doi:10.1038/s41433-023-02505-z
- Raimondi R, Falfeli T, Bogdanova-Bennet A, et al. Outcomes of treatment-resistant neovascular age-related macular degeneration switched from aflibercept to Faricimab. Ophthalmol Retina. 2023. doi:10.1016/j.oret.2023.11.015
- Rudnicka AR, Jarrar Z, Wormald R, Cook DG, Fletcher A, Owen CG. Age and gender variations in age-related macular degeneration prevalence in populations of European ancestry: a meta-analysis. Ophthalmology. 2012;119(3):571–580. doi:10.1016/j.ophtha.2011.09.027
- Mathur R, Bhaskaran K, Edwards E, et al. Population trends in the 10-year incidence and prevalence of diabetic retinopathy in the UK: a cohort study in the clinical practice research datalink 2004–2014. BMJ Open. 2017;7(2):e014444. doi:10.1136/bmjopen-2016-014444
- Jones R, Stratton IM, Scanlon PH, Theodoropoulou S. Disengagement and loss to follow-up in Intravitreal injection clinics for neovascular age-related macular degeneration. Eye. 2023;37(15):3186–3190. doi:10.1038/s41433-023-02474-3
- Rozon J-P, Hébert M, Laverdière C, et al. Delayed follow-up in patients with neovascular age-related macular degeneration treated under Universal Health Coverage. Retina. 2022;42(9):1693–1701. doi:10.1097/iae.0000000000003512
- Malhotra NA, Muste J, Hom GL, Conti TF, Greenlee TE, Singh RP. Race and socioeconomic status in anti-VEGF treatment of diabetic macular edema. Ophthalmic Surg Lasers Imaging Retina. 2021;52(11):578–585. doi:10.3928/23258160-20211018-01