Abstract
Purpose
To evaluate the relevance of community eye outreach programs in the early detection of glaucoma patients in southwest Nigeria.
Methods
This was a retrospective, cross-sectional study that was conducted among glaucoma patients referred to the eye clinic of the University College Hospital (UCH), Ibadan, Nigeria, between January 2009 and December 2010 from different sources, including community eye outreach programs. The source of referral, stage of glaucoma, and visual field were recorded.
Results
Six hundred and fifty-three patients were studied during this period. The mean age was 56.3 years ± 16.6 years, with a median age of 60 years. Patients referred from eye outreach programs were more likely to have mild to moderate disease than patients referred from other sources, who were more likely to have severe disease according to both the optic nerve head assessment (P < 0.01, Pearson’s Chi-square = 10.67, odds ratio = 1.7 [confidence interval = 1.23–2.31]) and visual field assessment (24–2) (P < 0.01, Pearson’s Chi-square = 6.07, odds ratio = 1.5 [confidence interval = 1.08–2.03]).
Conclusion
Community eye outreach programs appear highly useful in the earlier detection of glaucoma in sub-Saharan Africa.
Introduction
Glaucoma describes a group of eye diseases in which there is progressive damage to the optic nerve, leading to impaired vision and possibly blindness if untreated.Citation1 Glaucoma is the most common cause of irreversible blindness worldwideCitation2,Citation3 and in Nigeria.Citation4 The prevalence of glaucoma is highest in West Africa and in people of African descent.Citation5 Nearly half of those with glaucomatous optic nerve damage are undiagnosed in the developed world, while in developing countries the rate of undiagnosed glaucoma can be as high as 90%.Citation6,Citation7
Screening programs for the detection of glaucoma are not standard practice in Nigeria because of high costs and unknown effectiveness. However, in the last two decades, new technologies have been introduced that permit earlier detection of structural and functional damage due to glaucoma. Newer treatments also allow for safer and more effective intraocular pressure (IOP) reduction. Several well-conducted clinical trials show the effectiveness of treatment.Citation8–Citation10 These new developments, and the high prevalence of primary open angle glaucoma (POAG) in West Africa,Citation5 make it necessary to re-evaluate screening for the purpose of earlier diagnosis of glaucoma in developing countries.
The tremendous scarcity of resources for eye care in developing countries greatly limits the feasible interventions to prevent blindness from glaucoma through early detection. Integrating glaucoma detection into other blindness prevention programs, such as community cataract outreach programs, may be a simple and useful option. These community cataract outreach programs have proven efficacy in increasing the cataract surgical rate (CSR) in Africa.Citation11
There is a paucity of information about the value of community eye outreach programs in early glaucoma detection in West Africa. This study evaluates community eye outreach programs and provides useful information on this model for early glaucoma detection in West Africa.
Methodology
This retrospective, descriptive, cross-sectional study was conducted among glaucoma patients who presented to the eye clinic of the University College Hospital (UCH), Ibadan, Nigeria, with a diagnosis of glaucoma between January 2009 and December 2010. All patients with complete key outcome variables were included. The study was approved by the institutional review board of the University of Ibadan Ethical Committee.
The UCH Department of Ophthalmology community eye outreach program was initiated fully in January 2007 in response to the need to increase cataract surgical rates. Prior to this period, patients were seen in the UCH eye clinic only if they were referred by medically trained personnel from the general outpatient department or from other clinics within and outside UCH. The community outreach team comprises a community eye outreach specialist (ophthalmologist), an ophthalmology resident doctor, an optometrist, a public health nurse, one medical records staff, and an outreach team manager. The team reaches out to neighboring communities within and outside the state at least twice a week. These communities include the Ibadan metropolis and other towns and villages in Oyo, Osun, Ogun, and Lagos states. There are six permanent outreach centers that are all located within Oyo state. Other outreach programs are conducted at temporary sites ().
Figure 1 Map of Nigeria (right), map of southwest Nigeria (left).
Although the goal of the community eye outreach is to identify patients with cataracts and operate on them at the base hospital, all persons who attended the outreach programs had basic eye examinations, comprising anterior and posterior segment examination, refraction, fundoscopy, and intraocular pressure measurement. Patients with operable cataracts were transported immediately to the base hospital (UCH), while patients with suspected glaucoma and other major eye diseases, such as corneal diseases, traumatic eye disease, and retinal diseases, had comprehensive health education regarding their disease and were given appointments for further evaluation and management at the base hospital. However, patients with simple refractive errors or allergic and infective conjunctivitis were treated at the outreach site. Consultation services at the outreach sites were free, while patients who presented to the hospital had to pay a consultation fee of an equivalent of US$10.
At the outreach sites, patients with either a large cup to disc ratio (CDR) (≥0.5) with or without high intraocular pressure (IOP) (high IOP was defined as ≥21 mmHg,) or a CDR disparity of ≥0.2 between the two eyes were considered as glaucoma suspects and were referred to the base hospital for further evaluation and management. At the base hospital, each patient had complete history and ophthalmic evaluation, consisting of uncorrected and best corrected visual acuity, slit-lamp examination, IOP by Goldmann applanation tonometry, and gonioscopy using a four-mirror Posner lens. Automated full-threshold visual field tests for subjects with best-corrected visual acuity better than 6/60 using the 24–2 SITA standard program on the Humphrey 740 Visual Field Analyzer (Carl Zeiss Meditec AG, Jena, Germany) were performed. All eyes with open angles were dilated and stereoscopic examination of the vitreous, retina, and optic nerve head was done with the 78-diopter lens and the slit lamp. Eyes with narrow angles (occludable angles) were only dilated after a laser peripheral iridotomy was performed. A diagnosis of glaucoma was made based on the evidence of glaucomatous optic neuropathy (typical cupping of the optic nerve head, rim thinning or rim loss, focal notching, saucerization of the optic nerve head, retinal nerve fiber loss, and disc hemorrhage) with corresponding visual field defects with or without a raised IOP.
All patients with a diagnosis of glaucoma in any eye during the study period were identified from the eye clinic registers and their case records were retrieved from the medical records unit of the eye clinic. With the use of a data sheet, demographic and clinical data was retrieved from the case notes of each glaucoma patient. The sources of referral, type of glaucoma, and stage of disease at presentation were also recorded. All patients were seen by the consultant ophthalmologist.
The stage of the disease was defined based on the severity of the cupping of the optic disc and the mean deviation (MD) on visual fields. The stage of disease using the visual field was based on the Hodapp–Parrish–Anderson criteria.Citation12 Mild disease based on visual field defect was defined as MD <6 dB. Moderate disease was defined as MD of 6–12 dB while severe disease based on visual field was defined as MD of >12 dB. The visual fields used for this study were reliable and had reproducible defects. Using the optic disc cupping, mild disease was defined as CDR of 0.5–0.6, moderate disease was defined as CDR of 0.7–0.8, and severe disease was defined as CDR of 0.9–1.0.
Patients with complete data, who had proper documentation of all the key variables, including sources of referral, stereoscopic vertical CDR, reliable visual fields, gonioscopic findings, and type of glaucoma, were included and studied.
Data collected was collated and analyzed using SPSS version 16 (IBM Corporation, Armonk, NY, USA). Frequencies and means were generated to observe patterns of variable distribution among the patients. Bivariate analysis was conducted using cross tabulations and Pearson’s Chi-square tests to evaluate associations between categorical variables. A P–value of <0.05 was considered significant.
Results
Between January 2009 and December 2010, a total of 738 patients presented to the eye clinic with a diagnosis of glaucoma. Of these, 653 (88.5%) had complete data and were included in the study. Within the same period there were a total of 182 community outreach programs, and a total of 15,562 subjects were seen.
Patient ages ranged from 11 years to 95 years, with a mean of 56.3 years ± 16.6 years and a median age of 60 years. The male:female ratio was 1.3:1. There were 366 males with a mean age of 57.1 years ± 17.7 years and 287 females with a mean age of 56.3 years ± 16.6 years. Patients that were excluded from the study as a result of incomplete data had similar baseline characteristics as patients included in the study. There was no statistically significant difference between the two groups in age (P = 0.3) and sex (P = 0.6). shows the socio-demographic profile of glaucoma patients referred from the outreach and from other sources.
Table 1 Sociodemographic characteristics of glaucoma patients referred from the outreach and other sources
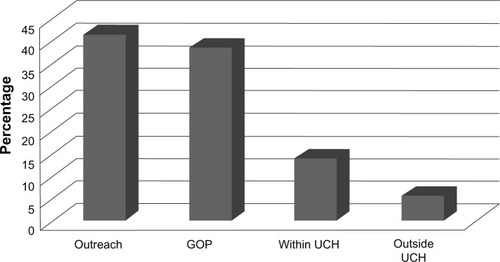
Of the glaucoma patients seen in the eye clinic during this period, 41.7% were referred from the community eye outreach and 38.7% were from the general outpatient clinic; 14.1% were from other clinics within UCH and 5.5% were referred from other clinics outside UCH ().
Figure 2 Sources of referral.
POAG was the most common type of glaucoma seen in patients referred from the outreach (68.8%) and from other sources (69.3%). There was no statistically significant difference in the types of glaucoma seen in patients referred from the outreach and those referred from other sources (P = 0.557, Pearson’s Chi-square = 2.07, df = 3) ().
Table 2 Types of glaucoma seen during the pre and post outreach periods
There were more patients with moderate disc damage referred from the outreach compared with patients referred from other sources using both the CDR in the worst eye (P < 0.01, Chi-square = 16.28, df = 2) and the visual field in the worst eye (P < 0.01, Pearson’s Chi-square = 9.8, df = 2) ().
Table 3 Stage of disease using the optic disc head evaluation and central visual field test
Using bivariate analysis, patients referred from the outreach were more likely to have mild to moderate disease than patients referred from other sources using both the optic nerve head assessment in the worst eye (P < 0.01, Pearson’s Chi-square = 10.67, OR = 1.7 [CI = 1.23–2.31]) and the central visual field assessment(P < 0.01, Pearson Chi-square = 6.07, OR = 1.5 [CI = 1.08–2.03]). shows bivariate analysis between source of referral and stage of glaucoma.
Table 4 Bivariate analysis between source of referral and stage of glaucoma
Discussion
This study evaluated the use of community eye outreach programs in early glaucoma detection in Nigeria. This ‘opportunistic screening’ method has been used to describe the strategy of examining all patients who show up in an eye care setting for glaucoma.Citation13
Most glaucoma in sub-Saharan Africa is POAGCitation14 and it often presents at an earlier age compared to Caucasians. It is associated with a higher IOP, is more rapidly progressive, and patients usually present late, with up to 50% of cases already blind in one eye at presentation.Citation5 The rate of undiagnosed glaucoma in developing countries can be as high as 90%Citation6,Citation7, likely because of the poor availability of adequate eye care facilities and the natural history of glaucoma.
The sociodemographic characteristics of the patients referred from the outreach programs and those referred from other sources were similar. There were more males than females, irrespective of the referral source. In many developing countries, access to eye care services is more limited for women than it is for men.Citation15,Citation16 Although some population studies of Africans and people of African descent, suggest a higher POAG in men compared with womenCitation14,Citation17 while others did not,Citation18,Citation19 Doshi et alCitation20 reported that more men access glaucoma services than women. This may be the result of the generally lower socioeconomic status of women, the associated lack of funds to procure health care, and lower educational status amongst women.
More patients were referred to the eye clinic from the outreach programs than from each of the other referral sources. This illustrates the importance of these types of programs in underdeveloped countries. Community outreach programs provide easier access to health care, create awareness, and also provide health education to the community; therefore, they help to generate awareness and demand for health care services in the community by those that need health intervention but that are not seeking it. Services are made available to the patients at the grassroots and the community level rather than waiting for the patients to access services at the hospital. Outreach programs are useful for social marketing of eye care services and they help to identify major eye problems in a community.Citation21
POAG was the most common type of glaucoma seen. The Baltimore Eye SurveyCitation18 found the prevalence of POAG in people of African descent to be four times greater than that in Caucasians. Ntim-Amposah et alCitation5 reported a POAG prevalence of 8.5% among adults aged 40 years and older in Ghana. Observations among West African ancestrally related populations in the Caribbean also show a very high prevalence of POAG. Studies from St LuciaCitation19 and BarbadosCitation22 reported a prevalence of 8.8% and 7.0%, respectively. Compared to the prevalence of POAG in the Temba eye study in South Africa (2.9%)Citation14 and the Kongwa study in Tanzania (3.1%),Citation23 the prevalence of POAG is higher in West Africa and in West African derived populations. POAG is asymptomatic before blindness occurs; therefore, patients are usually unaware of their disease. Rotchford et alCitation14 reported blindness in at least one eye in 58% of black patients with glaucoma.
More patients referred from outreach programs had moderate disease compared with patients referred from other sources, who often had symptoms and tended to present with more severe disease. This is likely because patients referred from other sources usually seek care when their glaucoma symptoms become more pronounced and affect their everyday lifestyle. Their symptoms may make them seek health care in hospitals often as a last resort. In Nigeria, many patients do not seek appropriate eye care due to various reasons that range from poverty to poor accessibility to eye care facilities.Citation24,Citation25 This may be further worsened by inappropriate health beliefs, whereby patients first seek alternative traditional health care services and only present to the hospital as a last resort.
The community eye outreach programs address some of these problems by making health care delivery more accessible and available. Many patients who attend the outreach programs often come for routine eye check-ups or have a refractive error. These patients feel no social stigma associated with attending outreach programs and there is no economic burden to them as the programs are free. It is during routine ocular examination by the ophthalmologists at the outreach programs that diseases, which are often symptomless, are detected. However, there are still some patients with advanced symptoms of glaucoma that seek health care at these outreach programs because of easier accessibility and availability. This suggests that other forms of screening, such as family screening, may further improve the earlier detection of glaucoma.
Our study indicates that patients who attend outreach programs have glaucoma symptoms that are less severe that those who directly present to the hospital clinics. The presence of an ophthalmologist on the outreach team may have further enhanced the diagnosis of glaucoma at an earlier stage. Low-level eyecare workers are typically trained to identify advanced glaucoma patients or those with blindness in one eye. Lewallen et alCitation11 reported that the ‘traditional screening model’, in which low-level eyecare workers were used to identify patients with visual impairment, was not very effective in referring appropriate patients that could benefit from surgery and other forms of management.
A population based study in the Kilimanjaro region of East Africa,Citation26 where community outreach programs have been carried out with well qualified examiners for many years, showed that all patients that were blind from glaucoma were, at the least, well aware of their diagnosis; thus providing further evidence of the importance of properly trained outreach teams.
Blindness due to glaucoma is a problem of global public-health importance, particularly in Africa, and is preventable through timely diagnosis, effective treatment, and clinic follow-up. Several population based surveys demonstrate the severity of glaucoma blindness in Africa.Citation4,Citation27,Citation28 OgwurikeCitation29 recommended that an integrated eye care program that would target cataract backlog, glaucoma screening, and other conditions would be beneficial in Nigeria.
In developing countries, where eye care services are often limited and many glaucoma patients present with end stage disease or blindness in at least one eye, community eye outreach programs may help in earlier diagnosis and prompt management to prevent blindness from the disease. These programs have proven effects and will help in achieving the objective of Vision 2020 to eliminate the main causes of avoidable blindness in the world.Citation30,Citation31 While it would not be cost effective to screen for glaucoma only, comprehensive eye evaluation inclusive of glaucoma diagnosis is recommended during community eye outreach in developing countries. Although early diagnosis is not the only hurdle to decreasing glaucoma blindness in Africa it may be a first step in achieving this goal. This study had some limitations. It was a retrospective study and not all of the patients had the key variables documented in their case notes. Also, we did not have the records and documentation of all the glaucoma suspects that presented at the base hospital upon referral. Further studies are needed to evaluate the long term benefits of community eye outreach programs in early glaucoma case detection. A prospective study evaluating this program is also recommended.
Author contributions
OO and OIF made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data, drafting of the article, revising it critically for important intellectual content, and final approval of the version to be published.
CCT and RR made substantial contributions to the conception and design, interpretation of data, drafting the article, revising it critically for important intellectual content, and final approval of the version to be published.
Acknowledgments
This paper was presented at the Association for Research in Vision and Ophthalmology annual meeting, May 9, 2012, Fort Lauderdale, Florida, USA.
Disclosure
The authors report no conflicts of interest in this work.
References
- MowattGBurrJMCookJAScreening tests for detecting open-angle glaucoma: systematic review and meta-analysisInvest Ophthalmol Vis Sci2008495373538518614810
- QuigleyHABromanATThe number of people with glaucoma worldwide in 2010 and 2020Br J Ophthalmol20069026226716488940
- ResnikoffSPascoliniDEtya’aleDGlobal data on visual impairment in the year 2002Bull World Health Organ20048284485115640920
- KyariFGudlavalletiMVSivsubramaniamSPrevalence of blindness and visual impairment in Nigeria: the National Blindness and Visual Impairment StudyInvest Ophthalmol Vis Sci2009502033203919117917
- Ntim-AmponsahCTAmoakuWMOfosu-AmaahSPrevalence of glaucoma in an African populationEye (Lond)20041849149715131680
- DandonaLDandonaRSrinivasMOpen-angle glaucoma in an urban population in southern India: the Andhra Pradesh eye disease studyOphthalmology20001071702170910964833
- RamakrishnanRNirmalanPKKrishnadasRGlaucoma in a rural population of southern India: the Aravind comprehensive eye surveyOphthalmology20031101484149012917161
- KassMAHeuerDKHigginbothamEJThe Ocular Hypertension Treatment Study: a randomized trial determines that topical ocular hypotensive medication delays or prevents the onset of primary open-angle glaucomaArch Ophthalmol200212070171312049574
- HeijlALeskeMCBengtssonBHymanLHusseinMReduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma TrialArch Ophthalmol20021201268127912365904
- No authors listedThe effectiveness of intraocular pressure reduction in the treatment of normal-tension glaucoma. Collaborative Normal-Tension Glaucoma Study GroupAm J Ophthalmol19981264985059780094
- LewallenSRobertsHHallAIncreasing cataract surgery to meet Vision 2020 targets; experience from two rural programmes in east AfricaBr J Ophthalmol2005891237124016170107
- HodappEParrishRK2ndAndersonDRClinical Decisions in GlaucomaSt LouisMosby1993
- CookCGlaucoma in Africa: size of the problem and possible solutionsJ Glaucoma20091812412819225348
- RotchfordAPKirwanJFMullerMAJohnsonGJRouxPTemba glaucoma study: a population-based cross-sectional survey in urban South AfricaOphthalmology200311037638212578784
- CourtrightPWestSKContribution of sex-linked biology and gender roles to disparities with trachomaEmerg Infect Dis2004102012201615550216
- LewallenSCourtrightPGender and use of cataract surgical services in developing countriesBull World Health Organ20028030030312075366
- RudnickaARMt-IsaSOwenCGCookDGAshbyDVariations in primary open-angle glaucoma prevalence by age, gender, and race: a Bayesian meta-analysisInvest Ophthalmol Vis Sci2006474254426117003413
- TielschJMSommerAKatzJRoyallRMQuigleyHAJavittJRacial variations in the prevalence of primary open angle glaucoma. The Baltimore Eye SurveyJAMA19912663693742056646
- MasonRPKosokoOWilsonMRNational survey of the prevalence and risk factors of glaucoma in St Lucia, West Indies. Part I. Prevalence findingsOphthalmology198996136313682789357
- DoshiVYing-LaiMAzenSPVarmaRLos Angeles Latino Eye Study GroupSocio-demographic, family history, and lifestyle risk factors for open-angle glaucoma and ocular hypertension. The Los Angeles Latino Eye StudyOphthalmology200811563964717900693
- BabalolaOEBabalolaIBEsugaMKato YohanaPIbeagbulamAAn Eye Care Outreach Programme in the Federal Capital TerritoryNig J Ophthalmology2003111215
- LeskeMCConnellAMSchachatAPHymanLThe Barbados Eye Study: prevalence of open angle glaucomaArch Ophthalmol19941128218298002842
- BuhrmannRRQuigleyHABarronYWestSKOlivaMSMmbagaBBPrevalence of glaucoma in a rural East African populationInvest Ophthalmol Vis Sci200041404810634599
- RabiuMMCataract blindness and barriers to uptake of cataract surgery in a rural community of northern NigeriaBr J Ophthalmol20018577678011423446
- OluleyeTSCataract blindness and barriers to cataract surgical intervention in three rural communities of Oyo State, NigeriaNiger J Med20041315616015293836
- LewallenSHassanHGAl AttasAHCourtrightPA population-based study of care-seeking behavior in rural Tanzanians with glaucoma blindnessJ Glaucoma20112036136520717055
- GuzekJPAnyomiFKFiadoyorSNyonatorFPrevalence of blindness in people over 40 years in the Volta region of GhanaGhana Med J200539556217299544
- AlemayehuWTekle-HaimanotRForsgrenLErkstedtJCauses of visual impairment in central EthiopiaEthiop Med J1995331631747588655
- OgwurikePamVPattern of Eye Diseases in Kaduna State – A rural community outreach experienceNigerian Journal of Ophthalmology: Official Organ of the Ophthalmological Society of Nigeria20041215
- ResnikoffSPararajasegaramRBlindness prevention programs: past, present, and futureBull World Health Organ20017922222611285666
- AcklandPThe accomplishments of the global initiative VISION 2020: The Right to Sight and the focus for the next 8 years of the campaignIndian J Ophthalmol20126038038622944746