
Abstract
Purpose
To analyze the refractive and visual outcomes following cataract surgery and implantation of a new hydrophobic trifocal toric intraocular lens (IOL) in Japanese eyes with different degrees of corneal astigmatism.
Methods
A total of 66 eyes from 39 patients implanted with a FineVision HP Toric IOL (Beaver-Visitec International Inc) were analyzed retrospectively. The main outcome measures considered were refraction, monocular uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), uncorrected intermediate visual acuity (UIVA), and distance-corrected intermediate visual acuity (DCIVA) at 80 and 66 cm, uncorrected near visual acuity (UNVA) and distance-corrected near visual acuity (DCNVA) at 40 cm. Eyes were evaluated at three months post-surgery.
Results
Sixty-five eyes (98.48%) were within ±0.50D of spherical equivalent, and all were within ±1.00D (mean: 0.00±0.21D). Moreover, 63 eyes (95.45%) had ≤0.50D of residual astigmatism, and all had ≤1.00D (mean: –0.08±0.23D). Similarly, 58 (87.88%) and 60 eyes (90.91%) had ≥20/20 UDVA and CDVA, respectively, with 65 (98.48%) and 66 eyes (100%) achieving ≥20/25 UDVA and CDVA, respectively. In addition, 28 (42.42%) and 23 eyes (34.85%) had ≥20/25 DCIVA at 80 and 66 cm, respectively, with 49 (74.24%) and 52 eyes (78.79%) achieving ≥20/32 DCIVA at 80 and 66 cm, respectively. Finally, 39 (59.09%) and 40 eyes (60.61%) had ≥20/20 UNVA and DCNVA, respectively, with 58 (87.88%) and 59 eyes (89.39%) achieving ≥20/25 UNVA and DCNVA, respectively.
Conclusion
Our study shows that implantation of the new hydrophobic FineVision HP Toric IOL results in accurate refractive outcomes, with good visual acuity at different distances, in Japanese eyes.
Introduction
Trifocal intraocular lenses (IOLs) have been developed in order to overcome the need of patients submitted to cataract surgery for spectacles to see objects at intermediate and near vision. The use of three foci is intended to preserve good vision at distance, intermediate, and near distances in such patients. A recent systematic review and meta-analysis comparing trifocal and extended depth-of-focus IOLs concluded that trifocal IOLs yielded improved near visual acuity compared to extended depth-of-focus IOLs, with no difference being found at distance and intermediate visual acuity.Citation1 That study also indicates that trifocal IOLs are associated with improved spectacle independence. In order to provide spectacle independence, both spherical and astigmatic errors should be corrected after cataract surgery. Specifically, it has been reported that useful visual acuity is achieved when astigmatism is ≤0.75D in trifocal IOLs, thus suggesting the need for correction when larger than this value.Citation2 A recent review paper has published the clinical outcomes of trifocal toric IOLs, in which 20 clinical studies encompassing 1404 eyes implanted with different commercially available trifocal toric IOLs were analyzed. This review concluded that the use of these lenses allows complete visual restoration over a wide range of distances.Citation3
One new hydrophobic trifocal toric IOL currently available is the FineVision POD FT 49P IOL (FineVision HP toric, Beaver-Visitec International, Inc., USA). The hydrophilic counterpart of this lens (FineVision toric POD FT), which presents the same optical design, has been analysed in different clinical studies on CaucasianCitation4–14 and AsianCitation15,Citation16 eyes with different degrees of corneal astigmatism. These studies showed the good outcomes of this model in terms of refraction accuracy (sphere and cylinder) and visual acuity at different distances. However, to the best of our knowledge, there are no studies focusing on the outcomes with the new hydrophobic trifocal toric FineVision HP and neither are there any specifically in Asian eyes. As such, the purpose of the present clinical study was to evaluate the accuracy refraction and visual outcomes at distance, intermediate, and near vision in a cohort of Japanese eyes with different amounts of corneal astigmatism diagnosed with cataracts after trifocal toric FineVision HP toric IOL implantation.
Patients and Methods
Patients, Intraocular Lens, and Surgical Technique
In this clinical study, we retrospectively examined 66 eyes from 39 patients at the Akihabara Cataract Clinic and the Nihonbashi Cataract Clinic (Tokyo, Japan), between December 2023 and January 2024. The study was carried out in accordance with the tenets of the Declaration of Helsinki and was approved by the Review Boards of both centers. Due to the retrospective nature of the study, the data was anonymized. All patients signed an informed consent to undergo the surgical procedure and agreed to use their de-identified data for statistical analysis and research purposes. The inclusion criteria were cataracts, aged 40 and over, implanted with the trifocal toric FineVision HP IOL, and patient’s interest in no longer wearing any form of spectacle correction for far, intermediate, and near vision. The exclusion criteria included previous ocular surgery and history of prior ocular disease that may affect the postoperative visual outcome.
As indicated, all patients were implanted with the FineVision HP toric IOL (POD FT 49P). This lens is made of acrylic hydrophobic glistening-free material (GFY, n=1.53 and Abbe number=42). The optical surface (aspheric, biconvex, and diffractive) produces two additions, one for intermediate (+1.75D) and one for near (+3.50D). The lens is available with spherical powers ranging from +10.0 to +35.0D (0.50D steps), and with a cylindrical power at the IOL plane of 1.00, 1.50, 2.25, 3.00, 3.75, 4.50, 5.25, and 6.00D. It also has an ultraviolet and blue light filter, an overall diameter of 11.40 mm, and an optical diameter of 6.00 mm. The haptic design is a double C-loop platform with Ridgetech and posterior angulated haptic. The lens is implanted using the Medicel Accuject 2.1/2.2 injection system.
The surgical procedure involved a phacoemulsification technique using the Centurion Phacoemulsification device (Alcon Labs, Fort Worth, TX, USA) through a 2.2 mm clear corneal incision with topical anaesthesia by an experienced surgeon (TA) using Phaco Prechop technique.Citation17 The toric axis was marked by the Akahoshi Intra-operative Axis Marker with CCC Guide (ASICO AE-2933).
Examinations and Analysis
A complete ophthalmological preoperative assessment, including slit lamp and fundoscopic examinations, refraction, and optical biometry using the IOLMaster 700 device (Carl Zeiss Meditec AG, Germany), was performed in all patients. The Barrett Universal II formula was used to calculate the required IOL power, and the targeted refraction was emmetropia. At three months post-surgery, the following metrics were assessed: manifest refraction (sphere, cylinder, and axis), monocular uncorrected distance visual acuity (UDVA), monocular corrected distance visual acuity (CDVA), monocular uncorrected intermediate visual acuity (UIVA) and monocular distance-corrected intermediate visual acuity (DCIVA) at 80 and 66 cm, monocular uncorrected near visual acuity (UNVA) and monocular distance-corrected near visual acuity (DCNVA) at 40 cm, all of them using the Sloan ETDRS tests (Precision Vision, Woodstock, Ill, USA). A double-angle plot toolCitation18 was used for the astigmatism vector analysis considering the preoperative corneal astigmatism obtained from the optical biometer and the postoperative refraction. Any complications or adverse events during surgery and follow-up were also recorded.
The metrics recorded were analyzed using Excel (2019, version 16.43, Microsoft Corporation, Redmond, WA, USA), and measurements given as the mean ± the standard deviation and ranges. Standard graphs for reporting refractive and visual acuity outcomes for IOL-based refractive surgery were plotted.Citation19
Results
This clinical trial enrolled 66 eyes from 39 patients with a mean age of 67.74±10.74 years (ranging from 44 to 86 years). All eyes were implanted with the FineVision HP Toric IOL, with a mean spherical IOL power of 16.37±3.77D (ranging from 10 to 24D) and mean cylindrical IOL power of 1.80±0.99D (ranging from 1 to 5.50D). shows the preoperative characteristics of the cohort. There were no surgical complications or adverse events during follow-up.
Table 1 Demographics and Characteristics of Eyes Shown as Means, Standard Deviations (SD), and Ranges
Refraction
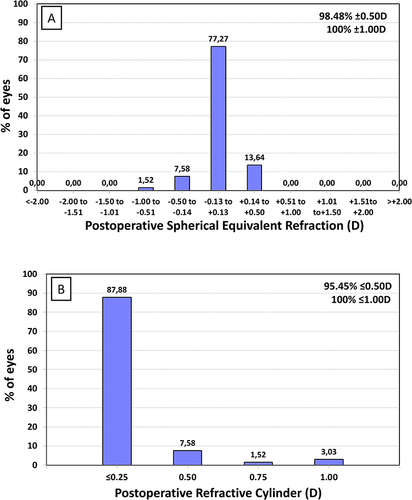
At three months post-surgery, the mean sphere was 0.04±0.18D (ranging from −0.50D to 0.75D), the mean cylinder was –0.08±0.23D (ranging from 0 to –1.00D), and the spherical equivalent (SE) was 0.00±0.21D (ranging from –1.00 to 0.50D). shows the postoperative distribution of SE Refraction, with almost all eyes (65, 98.48%) being within ±0.50D, and all (66, 100%) within ±1.00D. The largest group of eyes (77.27%) were in the range ±0.13D, followed by 13.64% of eyes in the range +0.14 to +0.50D. shows the distribution of the postoperative refractive cylinder, with 95.45% of eyes (63) having 0.50D or less, and all (66) eyes having 1.00D or less, residual astigmatism. Note the high percentage of eyes (87.88%) with a postoperative refractive cylinder of 0.25D or less.
Figure 1 Distribution of postoperative spherical equivalent refraction (A) and refractive cylinder (B) at three months post-surgery.
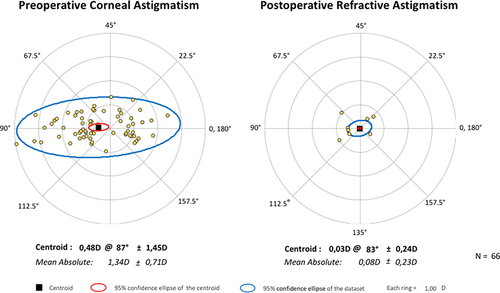
shows the double-angle plots of the preoperative corneal astigmatism and postoperative refractive astigmatism at three months post-surgery. The centroid of the corneal astigmatism before surgery was 0.48±1.45D at 87° and that of the refractive astigmatism was 0.03±0.25D at 83° after the intervention. The mean absolute value was reduced from 1.34±0.71D preoperatively to 0.08±0.23D at three months after the intervention.
Figure 2 Double-angle plots for preoperative corneal astigmatism and postoperative refractive astigmatism at three months post-surgery. Centroids and mean absolute values with standard deviations are also shown.
Visual Acuity
shows the mean monocular visual acuity outcomes at distance, intermediate and near vision recorded at three months postoperatively.
Table 2 Monocular Visual Acuity Outcomes (logMAR) for Eyes Implanted with the FineVision HP Toric Intraocular Lens (IOL) Shown as Means, Standard Deviations (SD), and Ranges at 3 Months of Follow-Up
Distance Visual Acuity
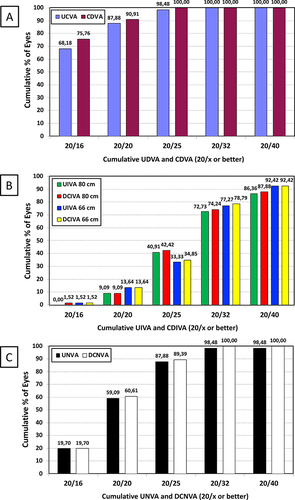
shows the difference in monocular UDVA and CDVA at three months post-surgery. The majority of eyes (89.39%) showed the same or better UDVA than CDVA, and 98.48% of eyes presented a UDVA within 1 line of CDVA. The mean UDVA and CDVA were good, with values better than 20/20 (–0.06±0.07 and –0.07±0.06 logMAR, respectively; ). shows the cumulative proportion of eyes with a given postoperative UDVA and CDVA. At three months post-surgery, 58 (87.88%) and 60 eyes (90.91%) had 20/20 or better UDVA and CDVA, respectively, with 65 (98.48%) and 66 eyes (100%) achieving 20/25 or better UDVA and CDVA, respectively.
Figure 3 Difference in monocular uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) at three months post-surgery.
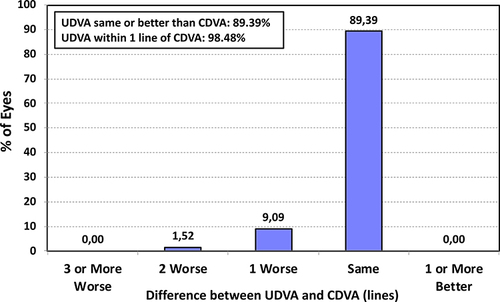
Figure 4 Cumulative proportion of eyes at three months post-surgery with a given postoperative uncorrected distance visual acuity (UDVA) and corrected distance visual acuity (CDVA) (A), uncorrected intermediate visual acuity (UIVA) and distance-corrected intermediate visual acuity (DCIVA) at 80 and 66 cm (B), and uncorrected near visual acuity (UNVA) and distance-corrected visual acuity (DCNVA) at 40 cm (C).
Intermediate Visual Acuity
The mean UIVA and DCIVA values at 80 cm were the same (0.19±0.12 logMAR), as were those at 66 cm (0.18±0.12 logMAR; see ). shows the cumulative proportion of eyes with a given postoperative UIVA and DCIVA at 80 and 66 cm. At three months post-surgery, 28 (42.42%) and 23 eyes (34.85%) had 20/25 or better DCIVA at 80 and 66 cm, respectively, with 49 (74.24%) and 52 eyes (78.79%) achieving 20/32 or better DCIVA at 80 and 66 cm, respectively.
Near Visual Acuity
The mean UNVA and DCNVA were good, with values close to 20/20 (0.03±0.10 and 0.02±0.08 logMAR, respectively; ). shows the cumulative proportion of eyes with a given a postoperative UNVA and DCNVA. At three months post-surgery, 39 (59.09%) and 40 eyes (60.61%) had 20/20 or better UNVA and DCNVA, respectively, with 58 (87.88%) and 59 eyes (89.39%) achieving 20/25 or better UNVA and DCNVA, respectively.
Discussion
In the current study, we have analyzed the outcomes of Japanese eyes implanted with the FineVision HP toric IOL. Although this is the first study to assess this particular model, previous studies have evaluated the hydrophilic counterpart of this lens on Caucasian and Asian eyes, showing good outcomes. As such, these outcomes should be compared with the present ones in order to provide clinical evidence for the refractive and visual acuity of the new model. provides a summary of these studies.
Table 3 Peer-Reviewed Publications Using the Hydrophilic Trifocal Toric FineVision PODFT IOL in Asian and Caucasian Eyes. Data for the Current Study are Also Included for Comparative Purposes (Note That in This Study the Hydrophobic FineVision HP Toric IOL Was Implanted)
In general, the visual outcomes at different distances obtained in our patients after FineVision HP toric IOL implantation were good. First of all, it should be noted that the successfully restored visual function observed with this lens is consistent with the high accuracy obtained in our cohort of eyes. This could be correlated with the spectacle independence of our patients. and shows the efficacy of the refractive correction, with 98.48% of eyes ±0.50D for the SE and 95.45% of eyes with a refractive cylinder of ≤0.50D. The mean SE and cylinder values were less than a quarter of a diopter. These outcomes are consistent with those reported by Yoo et alCitation15 and AngCitation16 in Asian eyes. Thus, at three months post-surgery, Yoo et alCitation15 obtained 86.84% of eyes with a residual refractive cylinder of ≤0.50D, while 87.50% of eyes showed the same at one year. The mean residual refractive cylinder values at three months and one year were –0.32±0.42D and –0.41±0.44D, respectively. In a large and longer follow-up cohort, AngCitation16 found mean SE and cylinder values of –0.07±0.31D and –0.45±0.37D at four- and six-months post-surgery, respectively. These values were maintained during the follow-up of this study (up to 24–26 months). Indeed, at the last follow-up, 87% and 99.4% of eyes were within ±0.50D and ±1.00D of SE, respectively, and 72.2% and 98.1% of eyes were within ±0.50D and ±1.00D of the postoperative refractive cylinder, respectively. The predictability of this lens in these studies broadly agrees with our findings, showing an effective correction of astigmatism. This is exemplified by the concentration of the dots at the 0,0 coordinate in , which represents an eye free from astigmatism.
In relation to the possible differences between Asian and Caucasian eyes, it should be considered that the former have been reported to have different ocular biometric parameters, and that changes in capsular bag diameter are different between them after cataract surgery.Citation20–22 As such, these differences might affect the efficacy and stability of the lens when implanted. Studies on Caucasian eyes with the same follow-up timeframe as ours (3 months) also showed good refractive accuracy. Thus, Gundersen and Potvin,Citation4 Nistad et alCitation5 Poyales and Garzón,Citation8 Ribeiro et al,Citation9 and Ribeiro and FerreiraCitation10 found mean SE values of ≤0.25D with astigmatism values of ≤0.50D. The percentage of eyes showing a refractive astigmatism of ≤0.50D was 82%Citation4 and 86%.Citation8 Another study in eyes with high corneal astigmatism (IOL cylinder power ≥3.75D) with a large follow-up (up to 5 years) reported similar outcomes:Citation14 mean SE was always within the range of ±0.25D and mean astigmatism values were about 0.50D. In general, these outcomes were slightly worse than ours. Differences between the IOL power calculation method employed, the range of IOL spherical and cylindrical powers in the studies and, finally, the different material of the lenses, may play a role. Specifically, the difference in materials, which show different refractive indices and Abbe numbers, may modify the thickness and curvature of the lens and, therefore, be the source of this slight difference. The impact of the lens material on objective refraction in eyes implanted with either the hydrophobic or hydrophilic non-toric version of the FineVision IOL has been studied recently in 100 eyes (50/50 randomly assigned to either one or the other lens material).Citation23 This study concluded that, after using different methods for refraction measurement (subjective, objective with two autorefractors and one aberrometer), better outcomes were obtained with the hydrophobic material for all methods assessed, with the difference between subjective refraction and objective refraction being very close to 0, at one-month post-surgery. These authors indicated that although the objective methods used were different, the myopic shift was always higher in the case of the hydrophilic IOL. This indicates a common pattern to that lens that results in a clear difference with the outcomes found with the hydrophobic model, which reaches clinical relevance in the case of the SE differences.
With regard to visual acuity, we found good outcomes in terms of distance visual acuity post-surgery correlated with high efficacy of the refractive correction since 89.39% of eyes presented the same or better UDVA than CDVA and 98.48% of eyes an UDVA within 1 line of CDVA (). The mean CDVA was good and >20/20 (–0.07±0.06 logMAR), with 90.91% and 100% of eyes with ≥20/20 and ≥20/25 CDVA, respectively (see ). Our outcomes were similar to those reported by Yoo et alCitation15 who found a mean monocular CDVA of –0.05 logMAR at three months and 0.01 logMAR at one year of follow-up. Similarly, AngCitation16 reported a mean monocular CDVA of 0.03±0.10 logMAR, with 75.5% and 88.1% of eyes with ≥20/20 and ≥20/25 CDVA, respectively, at 4–6 months. These values were similar at 21–26 months of follow-up: 0.04±0.09 logMAR, with 69.4% and 90.7% of eyes with ≥20/20 and ≥20/25 CDVA, respectively. The studies performed on Caucasian eyes at three months post-surgery found similar mean monocular CDVA values: –0.01±0.06 logMAR,Citation4 0.02±0.03 logMAR,Citation8 and 0.03±0.11 logMAR.Citation10 In cumulative visual acuities, our results were much better than those published by Poyales and Garzón,Citation8 who found that the CDVA was ≥20/20 in 81% and ≥20/32 in 98% of eyes, and similar to those reported by Orts-Vila et alCitation12 who found a CDVA of 20/20 for 96% of eyes and 20/25 or better for 100% of eyes. Specifically, the latter study analyzed only eyes implanted with the lowest IOL cylindrical power of the lens (1.00D). Longer follow-ups, such as those reported by Ruiz-Mesa et al,Citation14 evidenced lower percentages at five years, with 55.56% and 88.89% of eyes having a CDVA of ≥20/20 and ≥20/25, respectively, with these values being similar to those found by AngCitation16 at 21–26 months.
DCIVA was also excellent with this IOL, with mean values of 0.19±0.12 logMAR and 0.18±0.12 logMAR at 80 and 66 cm, respectively, and with 74.24% and 78.79% of eyes achieving ≥20/32 at these distances, respectively. Previous studies with the hydrophilic lens had already demonstrated improved intermediate vision without compromising distance vision. Specifically, Yoo et alCitation15 found a mean value of 0.19 logMAR for 80 and 60 cm, and AngCitation16 found a mean value of 0.09 logMAR and >90% of eyes ≥20/32 at 70 cm. These outcomes are similar to those published by Poyales and GarzónCitation8 and Ribeiro and Ferreira,Citation10 with monocular mean DCIVA values of 0.12±0.09 logMAR and 0.08±0.10 logMAR, respectively, at 80 cm, 0.08±0.14 logMAR at 63 cm8 and 0.09±0.11 logMAR at 60 cm10. Gundersen and PotvinCitation4 found 82% of eyes with a DCIVA of ≥20/25 at 63 cm, and Poyales and GarzónCitation8 found 24%, 67%, 93%, and 100% of eyes with a DCIVA of ≥20/20, ≥20/25, ≥20/30, and ≥20/40 at 80 cm, respectively. These values increased to 47%, 86%, 100%, and 100% at 63 cm, respectively. Note that these values were better than ours (see ). This may be correlated with the worse outcomes found by these authors at near vision (40 cm), with a mean DCNVA value of 0.17±0.09 logMAR.Citation8 Indeed, Gundersen and PotvinCitation4 found a mean DCNVA value of about 0.03 logMAR and Ribeiro and FerreiraCitation10 a mean value of 0.06±0.11 logMAR, both at 40 cm, which are much better and comparable to those found in our series (0.02±0.08 logMAR), respectively. In Asian eyes, Yoo et alCitation15 found mean values of 0.22 logMAR and 0.17 logMAR at three- and 12-months post-surgery, respectively, and AngCitation16 reported values of 0.10±0.12 logMAR and 0.13±0.13 logMAR at 4–6 and 21–26 months, respectively. Our cumulative DCNVA values were 60.61% for ≥20/20, 89.39% for ≥20/25, and 100% for ≥20/32 () and are much better than those reported by Poyales and Garzón,Citation8 who found values of 5%, 45%, and 90% of eyes for these cumulative visual acuities, respectively. The values reported by AngCitation16 were similar to those found by us (44.4%, 69.4%, and 90%, respectively, at 4–6 months).
Although we have not recorded rotational stability values for the lens in our cohort, it is well known that a reduction of about 15% of cylindrical correction is found for each 5° of error in the alignment of a toric IOL.Citation24 As such, if a significant rotation were to occur in our series, a considerable degree of residual astigmatism would be found. This was not the case since we obtained 95.45% of eyes with a refractive cylinder ≤0.50D, with the cylinder being less than a quarter of a diopter. also supports this given the concentration of dots at the 0.0 coordinate, with a mean centroid of 0.03D. As such, the excellent accuracy of the procedure correlates with the good stability of the lens. Although no rotational stability data have been published with the hydrophobic lens, the hydrophilic counterpart with the same haptic platform shows good mean rotational stability outcomes in the short- (1 month, 3.52±3.38°Citation13), medium- (3 months, 1.18±1.18°,Citation7 1.33±0.90°,Citation9 and 1.89±0.31°Citation10) and long-term (12 months, 2.55±2.62°Citation6) follow-up in Caucasian eyes, and long-term follow-up in Asian eyes (12 months, 2.14±1.72°,Citation15 and 24–26 months, 2.00±2.41°Citation16). Possible differences in the capsular bag between Caucasian and Asian eyes after cataract surgeryCitation20–22 seem not to affect the stability of the lens since the mean rotation values reported for Caucasian and Asian eyes are all around 2°. Consequently, a similar rotational stability performance would be expected with the new hydrophobic lens in both Caucasian and Asian eyes, thus maintaining good refractive outcomes.
The main limitations of our study are the lack of measurement of some metrics such as rotational stability, contrast sensitivity, or patient-reported quality-of-vision questionnaires. Specifically, for the former, we should consider that, although no rotational stability measurement was performed in our cohort, as discussed previously, we have not found any residual significant refractive value that may be produced by a significant rotation of the lens. This is also supported by the vector analysis carried out, thus confirming the good stability of the lens when implanted. Future clinical studies should include measurements of IOL rotation, contrast sensitivity under different lighting conditions and questionnaires to measure the patients’ visual functions and their spectacle independence. In addition, a long-term assessment of the lens would also be desirable.
Conclusions
In conclusion, our clinical study of the hydrophobic trifocal FineVision HP toric IOL three months after cataract surgery demonstrated good vision at a range of different distances, with excellent refractive accuracy in Japanese eyes with pre-existing corneal astigmatism. This lens appears to be a good option for correcting both presbyopia and astigmatism by providing distance, intermediate, and near visual restoration.
Disclosure
The author reports no conflicts of interest in this work.
References
- Karam M, Alkhowaiter N, Alkhabbaz A, et al. Extended depth of focus versus trifocal for intraocular lens implantation: an updated systematic review and meta-analysis. Am J Ophthalmol. 2023;251:52–70. doi:10.1016/j.ajo.2023.01.024
- Hayashi K, Yoshida M, Igarashi C, et al. Effect of refractive astigmatism on all-distance visual acuity in eyes with a trifocal intraocular Lens. Am J Ophthalmol. 2021;221:279–286. doi:10.1016/j.ajo.2020.07.051
- Tañá-Rivero P, Rodríguez-Carrillo MD, Tañá-Sanz P, Ruiz-Santos M, Tañá-Sanz S. Clinical outcomes of trifocal toric intraocular lenses. Eur J Ophthalmol. 2023;33(5):1773–1785. doi:10.1177/11206721231155047
- Gundersen KG, Potvin R. Comparison of visual outcomes after implantation of diffractive trifocal toric intraocular lens and an diffractive apodized bifocal toric intraocular lens. Clin Ophthalmol. 2016;10:455–461. doi:10.2147/OPTH.S103375
- Nistad K, Göransson F, Støle E, Shams H, Gjerdrum B. The use of capsular tension rings to reduce refractive shift in patients with implantation of trifocal intraocular lenses. J Refract Surg. 2017;33(12):802–806. doi:10.3928/1081597X-20170829-02
- Vandekerckhove K. Rotational stability of monofocal and trifocal intraocular toric lenses with identical design and material but different surface treatment. J Refract Surg. 2018;34(2):84–91. doi:10.3928/1081597X-20171211-01
- Poyales F, Garzon N, Pizarro D, Cobreces S, Hernandez A. Stability and visual outcomes yielded by three intraocular trifocal lenses with same optical zone design but differing material or toricity. Eur J Ophthalmol. 2019;29(4):417–425. doi:10.1177/1120672118795065
- Poyales F, Garzon N. Comparison of 3-month visual outcomes of a spherical and a toric trifocal intraocular lens. J Cataract Refract Surg. 2019;45(2):135–145. doi:10.1016/j.jcrs.2018.09.025
- Ribeiro FJ, Ferreira TB, Relha C, Esteves C, Gaspar S. Predictability of different calculators in the minimization of postoperative astigmatism after implantation of a toric intraocular lens. Clin Ophthalmol. 2019;13:1649–1656. doi:10.2147/OPTH.S213132
- Ribeiro FJ, Ferreira TB. Comparison of visual and refractive outcomes of 2 trifocal intraocular lenses. J Cataract Refract Surg. 2020;46(5):694–699. doi:10.1097/j.jcrs.0000000000000118
- Orts P, Piñero DP, Aguilar S, Tañá P. Efficacy of astigmatic correction after femtosecond laser-guided cataract surgery using intraoperative aberrometry in eyes with low-to-moderate levels of corneal astigmatism. Int Ophthalmol. 2020;40(5):1181–1189. doi:10.1007/s10792-020-01283-x
- Orts-Vila P, Aguilar-Córcoles S, Tello-Elordi C, Ramos-Alzamora M, Montés-Micó R, Tañá-Rivero P. Trifocal toric intraocular lenses in eyes with low amount of corneal astigmatism. Int J Ophthalmol. 2020;13(10):1567–1573. doi:10.18240/ijo.2020.10.09
- Sheen-Ophir S, Reitblat O, Levy A, Assia EI, Kleinmann G. Deviation from the planned axis of three toric intraocular lenses. Sci Rep. 2022;12(1):13760. doi:10.1038/s41598-022-17811-x
- Ruiz-Mesa R, Tañá-Sanz P, Tañá-Sanz S, Orts-Vila P, Tañá-Rivero P. Visual and refractive outcomes of a trifocal toric intraocular lens implanted in eyes with high corneal astigmatism. J Refract Surg. 2023;39(4):229–234. doi:10.3928/1081597X-20230127-01
- Yoo YS, Paik DW, Lim DH, Chung TY. One-year long-term clinical outcomes following diffractive trifocal toric intraocular lens implantation: retrospective observational case series study. Ann Transl Med. 2022;10(21):1159. doi:10.21037/atm-22-1007
- Ang RET. Long-term trifocal toric intraocular lens outcomes in Asian eyes after cataract surgery. J Cataract Refract Surg. 2023;49(8):832–839. doi:10.1097/j.jcrs.0000000000001195
- Akahoshi T. Phaco prechop: manual nucleofracture prior to phacoemulsification. In: Elander R, editor. Operative Techniques in Cataract and Refractive Surgery. Philadelphia, PA: W.B. Saunders Company; 1998:69–91.
- Abulafia A, Koch DD, Holladay JT, Wang L, Hill W. Pursuing perfection in intraocular lens calculations: IV. Rethinking astigmatism analysis for intraocular lens-based surgery: suggested terminology, analysis, and standards for outcome reports. J Cataract Refract Surg. 2018;44(10):1169–1174. doi:10.1016/j.jcrs.2018.07.027
- Reinstein DZ, Archer TJ, Srinivasan S, et al. Standard for reporting refractive outcomes of intraocular lens-based refractive surgery. J Refract Surg. 2017;33(4):218–222. doi:10.3928/1081597X-20170302-01
- Yoon JJ, Misra SL, McGhee CN, Patel DV. Demographics and ocular biometric characteristics of patients undergoing cataract surgery in Auckland, New Zealand. Clin Exp Ophthalmol. 2016;44(2):106–113. doi:10.1111/ceo.12634
- Tehrani M, Dick BH, Krummenauer F, Pfirrmann G, Boyle T, Stoffelns BM. Capsule measuring ring to predict capsular bag diameter and follow its course after foldable intraocular lens implantation. J Cataract Refract Surg. 2003;29(11):2127–2134. doi:10.1016/S0886-3350(03)00352-3
- Kim JH, Lee D, Cha YD, Oh SH, Mah KC, Lee MS. The analysis of predicted capsular bag diameter using modified model of capsule measuring ring in Asians. Clin Exp Ophthalmol. 2008;36(3):238–244. doi:10.1111/j.1442-9071.2008.01726.x
- Garzón N, Poyales F, García-Montero M, Vega F, Millán MS, Albarrán-Diego C. Impact of lens material on objective refraction in eyes with trifocal diffractive intraocular lenses. Curr Eye Res. 2022;47(1):51–61. doi:10.1080/02713683.2021.1946563
- Felipe A, Artigas JM, Díez-Ajenjo A, et al. Residual astigmatism produced by toric intraocular lens rotation. J Cataract Refract Surg. 2011;37(10):1895–1901. doi:10.1016/j.jcrs.2011.04.036