Abstract
A premature female infant underwent her first ophthalmologic examination at the age of 4 weeks. The initial examination of the baby was requested for evaluation of a ‘white spot’ on the surface of her right eye. She had been hospitalized in the neonatal intensive care unit because of systemic abnormalities, such as a right clavicle fracture and microcephaly. Slit-lamp examination of the right eye showed a central corneal opacity, corneal thinning, and an iridocorneal adhesion. The lens and fundus of the right eye could not be observed. We observed no pathologic findings in the left eye. The baby’s parents were informed of the high risk for spontaneous corneal perforation without external pressure. At 42 days of age, an ophthalmologic examination of the infant was again requested for evaluation of ‘tears’ from her right eye 3 hours previously. Examination revealed corneal perforation, iris protrusion, and a fat anterior chamber. We performed emergent conjunctival flap surgery. Three months following surgery, the patient’s right eye was successfully preserved with no sign of inflammation or leakage.
Introduction
Corneal perforation in the perinatal period is rare, and only a few cases are described in the literature. In most of the reported cases, low birth weight and systemic infection were associated with corneal perforation in the perinatal period,Citation1–Citation4 but there is one report of corneal perforation in relatively healthy newborns without evidence of trauma.Citation5 Anterior segment dysgenesis, such as Peters anomaly, is also associated with corneal perforation.Citation6–Citation8 Peters’ anomaly is characterized by a central corneal opacity from the time of birth and is accompanied by corresponding defects in the posterior stroma, Descemet’s membrane, and endothelium.Citation9,Citation10 We report a case of spontaneous corneal perforation in a neonate with Peters’ anomaly treated with a conjunctival flap.
Case report
A premature female infant, born after a gestational period of 33 weeks with a birth weight of 1.41 kg, underwent her first ophthalmologic examination at 4 weeks of age. The initial examination of the baby was requested for evaluation of a ‘white spot’ on the surface of her right eye. She was hospitalized in the neonatal intensive care unit due to systemic abnormalities, such as a right clavicle fracture and microcephaly.
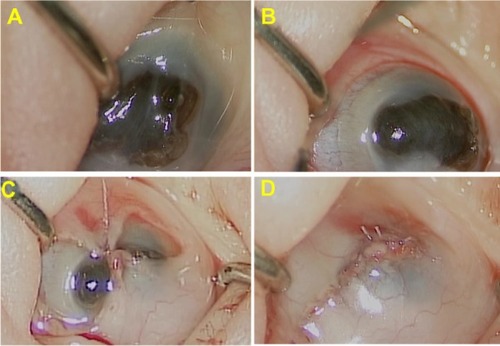
Slit-lamp examination of the right eye revealed a central corneal opacity, corneal thinning, and an iridocorneal adhesion (). The iris was fused with the posterior surface of the peripheral cornea, with poor formation of the anterior chamber. The lens and fundus in the right eye could not be observed. A B-scan, however, showed a normal posterior segment. Intraocular pressure could not be measured due to severe corneal thinning. The left eye showed no pathologic findings. The parents were informed of the high risk of spontaneous corneal perforation without external pressure.
Figure 1 Initial anterior segment findings of the right eye. Central corneal opacity, corneal thinning, and iridocorneal adhesion were observed.

At 42 days of age, an ophthalmologic examination of the infant was again requested for evaluation of ‘tears’ from her right eye observed 3 hours previously. Examination revealed corneal perforation, iris protrusion, and a flat anterior chamber (). We performed a 360° conjunctival peritomy () under general anesthesia to create a conjunctival flap, and the flap was brought down to cover the cornea. Simple interrupted sutures with 8–0 Vicryl (Ethicon Endo-Surgery, Inc, OH, USA) were then used to close the incision ( and ). Three months after the surgery, the right eye of patient was successfully preserved, with no sign of inflammation or leakage.
Figure 2 Intraoperative findings. Iris protrusion and a fat anterior chamber were observed.
Discussion
Since Peters’ original description in 1906,Citation11 many others have reported the ocular abnormalities now known as Peters’ anomaly. In 2007, Zaidman et al subdivided Peters’ anomaly into 3 types: (Type I) central corneal opacity with iridocorneal adhesions; (Type II) central corneal opacity with cataracts or corneolenticular adhesions; and (Type III) Peters’ anomaly in association with cleft lip/palate, short stature, abnormal ears, and mental retardation.Citation12
Peters’ anomaly may be isolated or accompanied by other ocular malformations such as chorioretinal coloboma, a congenital defect caused by faulty closure of the embryonic fissure, and is associated with other ocular and systemic abnormalities.Citation13
To our knowledge, however, only three reports of spontaneous corneal perforation occurring in association with Peters’ anomaly have been reported in the literature.Citation6–Citation8 Krause et al reported the first case of Peters’ syndrome with spontaneous corneal perforation in 1969.Citation6 Traboulsi and Maumenee reported clinical findings in 29 patients with Peters’ anomaly, and one of 29 patients developed spontaneous corneal perforation.Citation7 Banning et al described two patients with corneal perforation and secondary congenital aphakia in Peters’ anomaly. They performed penetrating keratoplasty to preserve the eyes.Citation8 In our case, however, we had to create a conjunctival flap rather than perform penetrating keratoplasty because of the lack of a donor cornea.
The conjunctival flap is a well proven, time honored treatment for numerous disparate corneal diseases that have a persistently compromised ocular surface in common.Citation14–Citation16 The purpose of the conjunctival flap is to restore the integrity of a compromised corneal surface, typically damaged as a result of trauma, neurotrophic disease, severe dry eye, or bullous keratopathy. The flaps prevent progressive corneal ulceration and secondary infection; they also control pain, eliminate frequent medications, and improve cosmesis. Complications encountered after conjunctival flap surgery are relatively uncommon, but the most frequently reported complications include flap retraction, conjunctival buttonholes and erosions, epithelial inclusion cysts, and corneal perforations.Citation17 In the present case, there were no complications. Although the conjunctival flap does not permit good visual acuity or good visualization of the anterior chamber details, it is sufficient to preserve the eye.
In our case, we did not perform genetic analyses. The PAX6 gene, which is expressed in the developing central nervous system, including the eye, is vital to eye development and is influential at early stages of ocular morphogenesis, acting as a master control gene.Citation18 It is therefore believed to play an important role in ocular embryogenesis. Mutations of the PAX6 gene are associated with various ocular anomalies, including Peters’ anomaly, aniridia, and chorioretinal coloboma.Citation19 Genetic studies of the patient may help to elucidate the causes of this anomaly.
Conclusion
Although rare, corneal perforation can occur in Peters’ anomaly. To our knowledge, this is the first documented case of a spontaneous corneal perforation in Peters’ anomaly treated with a conjunctival flap.
Disclosure
The authors report no conflicts of interest in this work.
References
- BachynskiBNAndreuRFlynnJRSpontaneous corneal perforation and extrusion of intraocular contents in premature infantsJ Pediatr Ophthalmol Strabismus19862325283950839
- JensenOANecrotizing keratitis (keratomalacia) with corneal perforation and expulsive uveal hemorrhage in a new-bornActa Ophthalmol (Copenhagen)196846215217
- BackesCRMakleyTAJrRogersGLCorderoLCForsytheRSpontaneous corneal perforation with expulsion of the lens and retina in a premature infantJ Pediatr Ophthalmol Strabismus1980172422446967968
- MichelsonPERuppREfthimiadisBEndogenous Candida endophthalmitis leading to bilateral corneal perforationAm J Ophthalmol1975808008031081343
- ZagelbaumBMStrohEMPerryHDDonnenfeldEDCossariAJCorneal perforation in a premature infantJ Refract Surg19951196987634149
- KrauseUKoivistoMRantakallioPA case of Peters syndrome with spontaneous corneal perforationJ Pediatr Ophthalmol Strabismus19696145149
- TraboulsiEIMaumeneeIHPeters’ anomaly and associated congenital malformationsArch Ophthalmol1992110173917421463415
- BanningCSBlackmonDMSongCDGrossniklausHECorneal perforation with secondary congenital aphakia in Peters’ anomalyCornea20052411812015604880
- NakanishiIBrownSIThe histopathology and ultrastructure of congenital, central corneal opacity (Peters’ anomaly)Am J Ophthalmol1971728018124938989
- WaringGO3rdRodriguesMMLaibsonPRAnterior chamber cleavage syndrome. A stepladder classificationSurv Ophthalmol197520327808872
- PetersAInnate defect formation of Descemet’s membrane. [Ueber angeborene Defektbildung der descemetschen Membran.]Klin Monatsbl Augenheilkd1906442740 German
- ZaidmanGWFlaniganJKFureyCCLong-term visual prognosis in children after corneal transplant surgery for Peters anomaly type IAm J Ophthalmol200714410410817601429
- BerkATYamanASaatçiAOOcular and systemic findings associated with optic disc colobomasJ Pediatr Ophthalmol Strabismus20034027227814560834
- DonzisPBMondinoBJManagement of noninfectious corneal ulcersSurv Ophthalmol198732941103317957
- PortnoySLInslerMSKaufmanHESurgical management of corneal ulceration and perforationSurv Ophthalmol19893447582678553
- BrownDDMcCulleyJPBowmanRWHalstedMHThe use of conjunctival flaps in the treatment of herpes keratouveitisCornea19921144461559346
- AlinoAMPerryHDKanellopoulosAJDonnenfeldEDRahnEKConjunctival flapsOphthalmology1998105112011239627666
- HansonIMFletcherJMJordanTMutations at the PAX6 locus are found in heterogeneous anterior segment malformations including Peters’ anomalyNat Genet199461681738162071
- Gregory-EvansCYWilliamsMJHalfordSGregory-EvansKOcular coloboma: a reassessment in the age of molecular neuroscienceJ Med Genet20044188189115591273