Abstract
Background
The purpose of this study was to evaluate the visual outcome of photorefractive keratectomy (PRK) in patients with mild to moderate stable keratoconus and to assess the risk of progression of the disease after the excimer laser procedure.
Methods
In this prospective study, carried out at the Clemenceau Medical Center, an affiliate of Johns Hopkins International, in Beirut, Lebanon, 119 eyes from 72 patients with grade 1–2 keratoconus (Amsler–Krumeich classification) underwent PRK. Forty-seven patients had both eyes treated and 25 patients had one eye treated. The procedure was done using the Wavelight Eye Q Excimer laser. Uncorrected and best-corrected visual acuity, corneal topography, and pachymetry were assessed before the procedure and 3, 6, 12, 36, and 60 months after the procedure.
Results
Mean uncorrected visual acuity showed a statistically significant improvement (P < 0.05) at one, 3, and 5 years follow-up. One hundred and seventeen eyes (98.3%) showed no progression while two eyes (1.7%) showed progression of the disease at 5 years follow-up, as documented by corneal topography and pachymetry. These two eyes were treated with corneal collagen crosslinking.
Conclusion
PRK in mild to moderate keratoconus is a safe and effective procedure for improving uncorrected vision in patients with mild refractive errors. However, close follow-up of patients is needed to detect any progression of the disease. Longer follow-up is needed to assess the overall effect of this procedure on progression of the disease.
Introduction
Keratoconus is a noninflammatory, progressive, and degenerative disease of the cornea characterized by central thinning and increased corneal curvature. The decrease in visual acuity is moderate to severe. It is due to myopia and irregular astigmatism and, at advanced stages, corneal scarring. Many clinical and surgical options for visual rehabilitation of keratoconus are available, ie, glasses, contact lenses (soft, rigid gas permeable, rigid, sclera, and semiscleral), intracorneal ring segments, phakic intraocular lenses, and keratoplasty (penetrating or lamellar) in advanced stages.Citation1
The unique conservative treatment option for keratoconus is still the fitting of rigid contact lenses to improve quality of vision, which is usually precarious with eyeglasses. Being a disease of the young, contact lens intolerance is a major issue through the years, with the risk of infectious keratitis. The consequences of the latter can be dramatic in already diseased corneas.
Other treatment options are corneal rings. Rings could reduce steepening and improve vision in carefully selected topography cases, especially in those patients experiencing contact lens discomfort.Citation2,Citation3 On the other hand, collagen crosslinking of the anterior stroma by the photosensitizer riboflavin and ultraviolet A light laser is being used for managing progressive keratoconus.Citation4–Citation6 In advanced keratoconus with scarring or hydrops, classic penetrating and lamellar keratoplasty are the mainstay of treatment.Citation7 The newer less invasive lamellar keratoplasty is an appealing option offering better graft tolerance compared with penetrating keratoplasty.Citation8–Citation10
Refractive surgery in patients with such irregular corneas has long been contraindicated because of the risk of postoperative progression of the disease process. This is especially true with laser in situ keratomileusis. The flap created in laser in situ keratomileusis weakens the corneal tissue and renders the cornea more prone to keratectasia.Citation11 However, numerous studies claim the safety of surface ablation in suspected keratoconus or in “forme fruste keratoconus” as in photorefractive keratectomy (PRK) and in PRK followed by corneal collagen crosslinking.Citation12–Citation14
The purpose of this study was to assess the visual outcome of PRK done in patients with mild to moderate stable keratoconus and to evaluate the safety of the procedure in terms of progression of the disease process.
Patients and methods
This was a prospective study that enrolled stable keratoconic patients during the period from January 2006 to December 2008. Participation rate in the study was 0.82 (82%) and the loss to follow-up rate was 0.22 (22%).
Diagnosis of keratoconus was based on a combination of the Pentacam® (Oculus Optikgerate GmbH, Wetzlar, Germany) of the anterior and posterior corneal surfaces, keratometric readings, and corneal pachymetry.Citation15–Citation18 All the patients had mild refractive errors (defined by a manifest refraction requiring a maximum ablation depth of 50 μm and leading to a minimal residual corneal thickness of 450 μm), a best-corrected visual acuity (BCVA) superior or equal to 20/30, and grade 1 or 2 keratoconus according to the Amsler-Krumeich keratoconus classification system (grade 1, eccentric corneal bulging, myopia, and/or astigmatism <5 D and corneal radius ≤48 D, no corneal opacities; grade 2, myopia and/or astigmatism >5 D and <8 D and/or corneal radius ≤53 D, no central opacities, pachymetry ≥400 μm).Citation19 All patients were uncomfortable using either eyeglasses or rigid contact lenses and their refraction was stable for at least one year prior to surgery. A complete ophthalmic examination including dilated fundus examination was done. Other ocular pathologies were ruled out. Exclusion criteria were: central corneal thickness less than 450 μm (measured by optical pachymetry, Oculus Pentacam), corneal opacification/scars, history of keratitis (any form), peripheral marginal degeneration, previous corneal and/or intraocular surgeries, and autoimmune and/or connective tissue disease.
The risks and benefits of the surgery were discussed with the patients, who gave their written informed consent. This study was approved by the review board committee at Clemenceau Medical Center, an affiliate of Johns Hopkins International in Beirut, Lebanon. One hundred and nineteen eyes were treated: 47 patients had both eyes treated and 25 patients had one eye treated. PRK was done at Clemenceau Medical Center. All surgical procedures were done by the same surgeon (EW). The laser treatment was carried out under local anesthesia (oxybuprocaine hydrochloride 0.4%). The central 9 mm of corneal epithelium was removed by application of 20% ethyl alcohol on the cornea for 25–30 seconds, followed by copious irrigation with a balanced salt solution. A dry Merocel sponge was used to peel off the epithelium. A standard non-topoguided PRK with a 5.5–6 mm optical zone and a transition zone of less than 2 mm was performed in all eyes with maximum ablation depth set at 50 μm. Residual corneal thickness was ≥450 μm. Laser treatment was carried out using the wavefront-optimized Wavelight® Eye Q Excimer laser (Allegretto®, [Alcon Laboratories Inc, Fort Worth, TX, USA] with an ablation rate of 400 Hz, 0.95 mm [0.68 mm full width at half maximum] Gaussian laser beam, and 400 Hz active eye-tracker). Mitomycin C 0.2% was applied for 20 seconds after laser treatment to minimize postoperative haze. Soft contact lens wearing was kept and patients maintained on tobramycin and dexamethasone sodium phosphate 0.1% (Tobradex®, Alcon Laboratories Inc) eyedrops four times daily for 10 days. Fluorometholone eyedrops were then prescribed for 3 months with progressive tapering.
Measured parameters were uncorrected visual acuity (UCVA), BCVA, spherical equivalent refraction, and cylindrical component. All were assessed before the procedure and at 3, 6, 12, 36, and 60 months afterwards. Haze was graded using the system described by Fantes et al (0, no haze; +0.5, trace haze on oblique illumination; +1, corneal cloudiness not interfering with the visibility of fine iris details; +2, mild effacement of fine iris details; +3 and +4, details of the lens and iris not discernible).Citation20
Corneal topography and pachymetry were also performed using the Oculus Pentacam before the procedure and at 6, 12, 36, and 60 months afterwards. Progressive keratoconus was defined by an increase in the cone apex keratometry of 0.75 D or an alteration of 0.75 D in the spherical equivalent refraction in the last 6 months.
Statistical analysis
Statistical analysis was performed using the Statistical Program for Social Sciences version 13.0 software (SPSS Inc, Chicago, IL, USA). A paired t-test was used to compare the preoperative and postoperative characteristics of patients. A P-value < 0.05 was considered statistically significant.
Results
Seventy-two patients (40 males and 32 females) with keratoconus and of mean age 31.5 ± 8.4 (19–54) years were included in the study. The logarithm of the minimum angle of resolution (logMAR) for UCVA and BCVA was 0.76 ± 0.34 and 0.018 ± 0.007, respectively. Spherical error and cylinder varied between +2.00 D and −5.75 D and between 0.50 D and 3.00 D, respectively. K flat (keratometry in the flat meridian) and K steep (keratometry in the steep meridian) varied between 39.5 D and 52.2 D and between 40.1 D and 54.2 D, respectively. Remaining preoperative patient characteristics are presented in .
Table 1 Refractive, keratometric, and topographic results
Refractive results
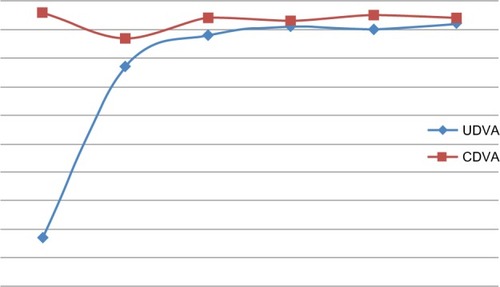
Mean UCVA showed a statistically significant improvement at one, 3, and 5 years follow-up. Seventy-nine eyes (66.3%) had a UCVA of 20/20 at 5 years follow-up and 119 eyes (100%) had a UCVA >20/40 at 5 years follow-up. Mean BCVA remained stable postoperatively (). Two eyes (1.7%) lost two or more lines at 5 years follow-up. The mean spherical error and mean cylindrical component obtained from manifest refraction also showed a statistically significant improvement throughout the follow-up period. A total of 101 eyes (84.9%) had a manifest spherical equivalence within 0.50 D and 1.00 D at 5 years and two of the eyes (1.7%) had a manifest refraction change of more than 1.00 D at 5 years.
Figure 1 Change in UDVA and CDVA (in decimals) over the follow-up period.
Topographic results
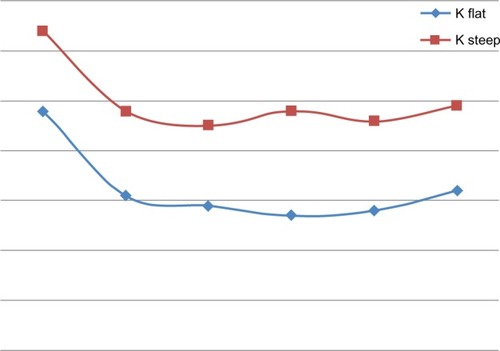
K flat and K steep decreased significantly postoperatively and remained stable during the follow-up period (). One hundred and seventeen eyes (98.3%) showed no progression of the disease, and two eyes (1.7%) showed progression at 5 years follow-up as documented by corneal topography. Progression was evident in two eyes from two different patients. The first patient, aged 33 years, had a BCVA of 20/25, with −2.25 + 1.25 D manifest refraction, a central corneal thickness of 492 μm, and a Kmax of 47.8 D. Keratoconus progression was evident at one-year follow-up, with an increase in maximum keratometry of 1.12 D. The second patient, aged 29 years, had a BCVA of 20/20, with −1.75 + 1.50 D manifest refraction, a central corneal thickness of 502 μm, and a Kmax of 48.1 D. Keratoconus progression was evident at 2-year follow-up, with an increase in maximum keratometry of 1.22 D. The two eyes were treated subsequently by collagen crosslinking, with a final UCVA at 5 years of 20/30 and 20/40, respectively, and a final BCVA at 5 years of 20/25 and 20/30, respectively.
Figure 2 Change in keratometry over the follow-up period.
Postoperative subepithelial opacity
The majority of eyes showed a subepithelial opacity below grade 2 at different time intervals. Eight eyes had grade 2 haze at one-month follow-up, one eye had grade 2 haze at 6 months follow-up, and no eye had grade 2 haze (or higher) at 5 years follow-up.
Discussion
In patients with mild to moderate keratoconus, combined PRK and collagen crosslinking has been proven to be a safe and effective alternative to correct minor refractive error, stabilizing the remaining stromal bed and avoiding progression of ectatic disease.Citation13,Citation14,Citation20
Guedj et al reported 62 eyes of 42 patients with suspected keratoconus who were treated with PRK alone. Postoperatively, visual acuity improved significantly and remained stable during a follow-up period of 5 years. Treatment with PRK alone did not lead to progression or acceleration of the suspected keratoconus or any other complication.Citation12
According to our results and the literature, PRK seems to be a promising option for the rehabilitation of eyes with mild refractive errors and a BCVA ≥20/30, especially when coupled with contact lens intolerance.Citation21–Citation24 To avoid the complications associated with collagen crosslinking (mainly haze), we choose not to perform collagen crosslinking at baseline and to postpone it as much as possible. During the follow-up period, patients had a corneal topography every 6 months in the first year then annually. Of the 119 eyes included in the study, only two eyes had progression and were subsequently treated with collagen crosslinking.
Accurate thresholds for a safe ablation regarding parameters such as K readings and pachymetry are not yet established. Kasparova and Kasparov recommend >500 μm central and peripheral corneal thickness.Citation25 Koller et al also recommend a minimal corneal thickness >500 μm and predicted residual corneal thickness >450 μm with maximal K reading <49.Citation22 In the study by Cennamo et al, maximal K readings were 52.09 ± 3.47.Citation24 Overall keratoconus severity ranged from forme fruste to a maximum grade 2 keratoconus according to the Amsler-Krumeich classification, with stable refraction of at least one year in most studies.Citation11,Citation22,Citation23,Citation26–Citation28
Haze was the most frequently reported complication in the literature. In most studies, mitomycin C was not used during surgery. Kasparova and Kasparov reported haze in 5/70 eyes in the early postoperative period.Citation25 This disappeared in 1–3 months with the use of corticosteroids. In the study by Cennamo et al, haze was 0 in 22 eyes and 0.5 in four eyes at 24 months follow-up.Citation24 Haze was grade 1 in 3/4 eyes treated by Doyle et al and grade 2 in 1/4 eyes.Citation28 The latter patient was given fluorometholone. In the study by Bahar et al, 20% of eyes had grade I haze that disappeared following 3 months of steroids and 7.5% had grade II haze that partially regressed following steroids.Citation27 In our study, we used mitomycin C in all patients and haze was not a major concern (eight patients had grade II haze at one month follow-up). At the end of our follow-up, no patients had any vision-impairing haze.
In the studies reviewed, refractive results were comparable with those in our study, with significant improvement of UCVA, BCVA, and manifest refraction postoperatively.Citation11,Citation22,Citation26 In the study by Kasparova and Kasparov, keratoconus progression appeared in 6/70 eyes (8.57%) in the first to sixth month after surgery.Citation25 This was identified as increased myopia and myopic astigmatism and reduction of corneal thickness. In our study, only 2/119 eyes (1.7%) showed progression at 5 years follow-up. The mean age in our study was 31.5 years, which renders progression less likely and could explain this difference. In the other studies reviewed, no progression of keratoconus was observed during the follow-up period. Topographies done at regular intervals showed notable reduction of steepening and irregularity.Citation11,Citation22,Citation24,Citation25,Citation27,Citation28 However, a longer follow-up period is needed. For instance, Koller et al suggest corneal topography monitoring for up to 5 years to be sure that the photorefractive keratectomy has not induced keratoconus progression in corneas documented to be preoperatively stable for years.Citation22 In fact, corneal ectasia can occur even a decade after PRK.Citation29
In some studies, PRK even seems to halt the progression of keratoconus. Cennamo et al reported a significant decrease in all keratoconus indices during 24 months of follow-up of treated eyes (n = 25) versus an increase in indices in control untreated eyes (n = 8), suggesting a possible therapeutic effect of excimer laser, halting the progression of keratoconus.Citation24 A larger population and longer follow-up is warranted. It is speculated that excimer laser ablation leads to formation of a new fibrocellular membrane instead of the ablated corneal layers. The rigidity of this membrane is much higher than the anterior corneal layers in keratoconus so that better biomechanical qualities of the new membrane could act like a shield that helps to prevent further progression of keratoconus. At the same time, the fibrocellular membrane can serve as the matrix for synthesis and reconstruction of the lamellar structure, characteristic of a normal cornea. Both processes would theoretically prevent keratoconus progression in the postoperative period.Citation25
PRK seems to be a good therapeutic option for patients with mild to moderate stable keratoconus and bad uncorrected visual acuity, low refractive errors, and contact lens intolerance. Significant visual improvement was reached in our study and is reported in the literature. It is reasonably safe, with little risk of disease progression in carefully selected patients. Our results are restricted to a 5-year study period, and safety over a longer follow-up must be assessed to ensure the safety of such an approach in treating patients with stable keratoconus.
Conclusion
Combined PRK and collagen crosslinking have been proven to be a safe and effective procedure for correcting minor refractive error and stabilizing the cornea in keratoconus. PRK alone with regular follow-up could be a safe and effective procedure for improving uncorrected vision in selected patients with mild to moderate stable keratoconus.
Disclosure
The authors report no conflicts of interest in this work.
References
- FadlallahADiraniARamiHECherfaneGJaradeESafety and visual outcome of Visian Toric ICL implantation after corneal collagen cross-linking in keratoconusJ Refract Surg201329848923380407
- PiñeroDPAlióJLTeusMABarraquerRIMichaelRJiménezRModification and refinement of astigmatism in keratoconic eyes with intrastromal corneal ring segmentsJ Cataract Refract Surg2010361562157220692571
- PesandoPMGhiringhelloMPDi MeglioGRomeoSTreatment of keratoconus with Ferrara ICRS and consideration of the efficacy of the Ferrara nomogram in a 5-year follow-upEur J Ophthalmol20102086557320491049
- GoldichYMarcovichALBarkanaYAvniIZadokDSafety of corneal collagen cross-linking with UV-A and riboflavin in progressive keratoconusCornea20102940941120164744
- VinciguerraPAlbèETrazzaSSeilerTEpsteinDIntraoperative and postoperative effects of corneal collagen cross-linking on progressive keratoconusArch Ophthalmol20091271258126519822840
- CaporossiAMazzottaCBaiocchiSCaporossiTLong-term results of riboflavin ultraviolet A corneal collagen cross-linking for keratoconus in Italy: the Siena Eye Cross StudyAm J Ophthalmol201014958559320138607
- FukuokaSHondaNOnoKMimuraTUsuiTAmanoSExtended long-term results of penetrating keratoplasty for keratoconusCornea20102952853020299971
- TanDTHAnshuAParthasarathyAHtoonHMVisual acuity outcomes after deep anterior lamellar keratoplasty: a case-control studyBr J Ophthalmol2010941295129920829318
- JavadiMAFeiziSYazdaniSMirbabaeeFDeep anterior lamellar keratoplasty versus penetrating keratoplasty for keratoconus: a clinical trialCornea20102936537120168217
- FeiziSJavadiMAJamaliHMirbabaeeFDeep anterior lamellar keratoplasty in patients with keratoconus: big-bubble techniqueCornea20102917718220023579
- BührenJSchäffelerTKohnenTPreoperative topographic characteristics of eyes that developed posoperative LASIK keratectasiaJ Refract Surg20132954054923909781
- GuedjMSaadAAudureauEGatinelDPhotorefractive keratectomy in patients with suspected keratoconus: five-year follow-upJ Cataract Refract Surg201339667323102727
- KymionisGDPortaliouDMKounisGALimnopoulouANKontadakisGAGrentzelosMASimultaneous topography-guided photorefractive keratectomy followed by corneal collagen cross-linking for keratoconusAm J Ophthalmol201115274875521794846
- KruegerRRKanellopoulosAJStability of simultaneous topography-guided photorefractive keratectomy and riboflavin/UVA cross-linking for progressive keratoconus: case reportsJ Refract Surg201026S827S83220954679
- FamH-BLimK-LCorneal elevation indices in normal and keratoconic eyesJ Cataract Refract Surg2006321281128716863962
- MaedaNKlyceSDSmolekMKComparison of methods for detecting keratoconus using videokeratographyArch Ophthalmol19951138708747605277
- QuislingSSjobergSZimmermanBGoinsKSutphinJComparison of Pentacam and Orbscan IIz on posterior curvature topography measurements in keratoconus eyesOphthalmology20061131629163216949447
- RabinowitzYSRasheedKYangHElashoffJAccuracy of ultrasonic pachymetry and videokeratography in detecting keratoconusJ Cataract Refract Surg1998241962019530594
- AlióJLShabayekMHCorneal higher order aberrations: a method to grade keratoconusJ Refract Surg20062253954516805116
- FantesFEHannaKDWaringGO3rdPouliquenYThompsonKPSavoldelliMWound healing after excimer laser keratomileusis (photorefractive keratectomy) in monkeysArch Ophthalmol19901086656752334323
- StojanovicAZhangJChenXNitterTAChenSWangQTopography-guided transepithelial surface ablation followed by corneal collagen cross-linking performed in a single combined procedure for the treatment of keratoconus and pellucid marginal degenerationJ Refract Surg20102614515220163079
- KollerTIseliHPDonitzkyCIngDPapadopoulosNSeilerTTopography-guided surface ablation for forme fruste keratoconusOphthalmolog y200611321982202
- AlpinsNStamatelatosGCustomized photoastigmatic refractive keratectomy using combined topographic and refractive data for myopia and astigmatism in eyes with forme fruste and mild keratoconusJ Cataract Refract Surg20073359160217397730
- CennamoGIntravajaABoccuzziDMarottaGCennamoGTreatment of keratoconus by topography-guided customized photorefractive keratectomy: two-year follow-up studyJ Refract Surg20082414514918297938
- KasparovaEAKasparovAASix-year experience with excimer laser surgery for primary keratoconus in RussiaJ Refract Surg200319Suppl 2S250S25412699184
- Wygledowska-PromieńskaDGierek-CiaciuraSEight year results of excimer laser correction for irregular astigmatism by linear excimer laser photoablations of the cornea in cases of keratoconusKlin Oczna2000102439442 Polish11392806
- BaharILevingerSKremerIWavefront-supported photorefractive keratectomy with the Bausch and Lomb Zyoptix in patients with myopic astigmatism and suspected keratoconusJ Refract Surg20062253353816805115
- DoyleSJHynesENarooSShahSPRK in patients with a keratoconic topography picture. The concept of a physiological “displaced apex syndrome”Br J Ophthalmol19968025288664226
- KimHChoiJSJooCKCorneal ectasia after PRK: clinicopathologic case reportCornea20062584584817068463