Abstract
Background
Very few reports have addressed methods of treatment for idiopathic serous (IS) pigment epithelial detachment (PED).
Objective
The purpose of this report was to describe clinical courses of two patients with ISPED in whom reduced-fluence photodynamic therapy (RFPDT) was performed.
Case reports
Two patients (a 38-year-old woman and a 42-year-old man) were diagnosed with ISPED. In both patients, indocyanine green angiography revealed an area of choroidal vascular hyperpermeability including hyperfluorescent PED, which was evident at the subfoveal area. Both patients underwent RFPDT at an energy of 25 J/cm2. The PED was seen to have resolved 1 month after the treatment and visual acuity was maintained or improved. There was no posttreatment recurrence of PED after 6 months to 1 year, and no treatment-related adverse events were observed.
Conclusion
RFPDT may be an effective and safe method of treatment for ISPED with choroidal vascular hyperpermeability.
Introduction
Pigment epithelial detachment (PED) is a condition in which the retinal pigment epithelium is detached from the Bruch membrane due to the accumulation of fluid or blood between them, which occurs in exudative age-related macular degeneration and other chorioretinal disorders. Idiopathic serous PED (ISPED) is not associated with choroidal neovascularization, meaning that, in most cases, the visual prognosis is good, but patients are aware of distorted vision, and it is known to increase the risk of exudative age-related macular degeneration.Citation1 ISPED is categorized into two types, one that exhibits hyperfluorescence under indocyanine green angiography (ICGA), suggesting hyperpermeability of choroidal vessels, and the other that exhibits hypofluorescence. The hyperfluorescent type is extremely similar to the pathology of central serous chorioretinopathy (CSC), and these are regarded as similar disease concepts caused by choroidal hyperpermeability.Citation2,Citation3
Very few reports have addressed methods of treatment for ISPED. Standard-fluence photodynamic therapy (PDT) with verteporfin (50 J/cm2) has been shown to be effective in CSC by improving visual acuity and reducing subretinal fluid.Citation4–Citation6 Reduced-fluence PDT (RFPDT) has also been reported as useful in the treatment of CSC. Reibaldi et al evaluated the efficacy of RFPDT compared with standard-fluence PDT for treating chronic CSC, concluding that both PDTs reduce subretinal fluid and improve visual acuity in CSC, but RFPDT induces less choriocapillaris damage.Citation7 RFPDT (40 J/cm2 with a shorter exposure time than that of the standard-fluence PDT protocol) has recently been administered to patients with ISPED, and the short-term (3-month) outcomes of this treatment have been reported.Citation8
In this study, we report a 6-month to 1-year follow-up of two patients with ISPED in whom ICGA revealed hyperpermeability of the choroidal vessels and ISPED was evident at the subfoveal area, who were treated with RFPDT (25 J/cm2 with the standard exposure time).
Patients and methods
This study was approved by the institutional review board of The Jikei University School of Medicine, Tokyo, Japan after fully informed consent had been obtained from both patients. After intravenous administration of the same dose of verteporfin as used in standard-fluence PDT (6 mg/m2 of body surface intravenously for 10 minutes), RFPDT was carried out using the VISULAS 690S PDT system (Carl Zeiss Meditec AG, Jena, Germany) with 83-second exposure, as for standard-fluence PDT, and energy per surface area of 25 J/cm2. The RFPDT laser spot size was determined by the same method previously reported for CSC;Citation9 namely, the spot size was set to cover hyperfluorescent areas (including the whole PED area) identified from mid-phase or late-phase ICGA images. A Cirrus HD-OCT system (Carl Zeiss Meditec) was used for optical coherence tomography (OCT) using protocols of macular cube scan and HD 5-line raster scan. The Heidelberg Retina Angiograph 2 (Heidelberg Engineering GmbH, Heidelberg, Germany) was used for fluorescein angiography (FA) and ICGA.
Results
Case 1
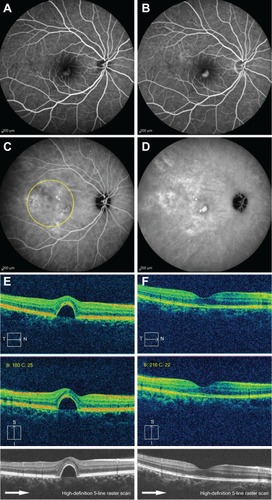
The patient was a 38-year-old woman. She had been attending hospital for 15 months, with principal complaints of reduced visual acuity and distorted vision in the right eye. On initial examination, log of the minimum angle of resolution (log-MAR) best-corrected visual acuity (BCVA) of the right eye was 0.1. The images of FA, ICGA, and OCT are described in . No serous retinal detachment was evident on OCT images, which showed PED of half the disc diameter in the subfovea, including the fovea, and continuity of the inner and outer segments (IS/OS) line was unclear. FA showed hyperfluorescence in the early phase of contrast enhancement in the same location as the PED, and ICGA revealed hyperfluorescence in the mid-phase and late-phase of contrast enhancement in the same location as the PED, as well as hyperpermeability of the choroidal vessels in the surrounding area, resulting in a diagnosis of ISPED. In ICGA, no polypoidal lesion or branching vascular network, which is diagnostically seen in polypoidal choroidal vasculopathy, were observed. Because the PED had not improved, RFPDT (spot size: 5,400 μm) was performed 16 months after onset. The PED was seen to have completely disappeared 1 month after RFPDT. Continuity of the IS/OS line was restored on the OCT images, and logMAR BCVA improved to −0.1 with symptomatic improvement of the distorted vision. Visual acuity was maintained at 12 months posttreatment, with no recurrence of PED. No adverse events were seen in this case during follow-up after RFPDT.
Figure 1 Fundus and optical coherence tomography findings in the right eye (Case 1).
Case 2
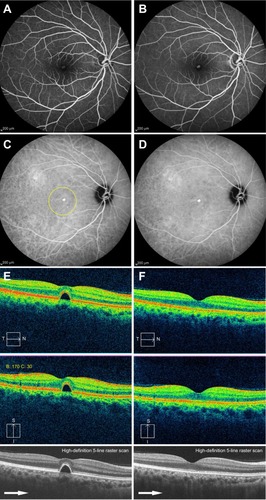
The patient was a 42-year-old man. He had been attending hospital for 4 months, with the principal complaint of distorted vision in the right eye. On initial examination, logMAR BCVA of the right eye was −0.2. The images of FA, ICGA, and OCT were described in . No serous retinal detachment was evident on OCT images, which showed serous PED of one-fifth of the disc diameter at the subfovea, and continuity of the IS/OS line was unclear. FA showed hyperfluorescence in the same location as the PED, and ICGA revealed hyperfluorescence of the PED from the mid-phase to the late-phase and weak hyperfluorescence around the PED due to hyperpermeability of the choroidal vessels, resulting in a diagnosis of ISPED. Because the PED had not improved, RFPDT (spot size: 3,300 μm) was performed 6 months after onset. The PED was seen to have completely disappeared 1 month after RFPDT. Continuity of the IS/OS line was restored on OCT images, and logMAR BCVA was maintained, with symptomatic improvement of distorted vision. Visual acuity was maintained at 6 months posttreatment, with no recurrence of PED. No adverse events were seen in this case during follow-up after RFPDT.
Figure 2 Fundus findings in the right eye (Case 2).
Discussion
This report presents the good therapeutic course of two patients with ISPED with choroidal hyperpermeability, who were treated with RFPDT. Although Case 1 had suffered from this disorder for over 1 year, the PED was seen to have completely disappeared 1 month after treatment, and this good condition was maintained at 1 year following the procedure without the need for additional treatment. In Case 2, the PED was also seen to have completely disappeared 1 month after treatment.
Both patients exhibited hyperfluorescence on ICGA that was suggestive of choroidal hyperpermeability, and although serous retinal detachment was not present, their pathology closely resembled that of CSC. With respect to the natural course of PED associated with CSC, Mudvari et al report that, during a mean follow-up period of 49 months, it disappeared spontaneously in 65% of cases, and mean visual acuity improved.Citation10 However, they also report that visual acuity declined in 50% of their patients in whom PED was present at the subfovea,Citation10 and this may correspond to our patients, whose visual acuity could be expected to decline in future.
Very few reports have addressed methods of treatment for ISPED. Goto et al performed RFPDT to treat PED (at the subfoveal area) with hyperpermeability of the choroidal vessels, and they report the short-term (3-month) outcomes of this treatment.Citation8 They mention that the PED had completely disappeared 1 month after RFPDT in 93% of cases, visual acuity improved significantly during 3 months’ posttreatment follow-up, and no recurrence was observed.Citation8 For their RFPDT procedure, they chose to reduce the fluence to 40 J/cm2 by using a shorter exposure time than that of the standard-fluence PDT protocol.Citation8 We chose to perform RFPDT at an even lower fluence of 25 J/cm2, and we obtained similarly good results. The follow-up period after RFPDT treatment reported by Goto et alCitation8 is short (only 3 months), but the two patients in our study were followed for 6 months to 1 year, and no recurrence of PED was observed. Reducing PDT energy is believed to decrease the incidence of persistent choriocapillaris hypoperfusion, pigmentary changes of retinal pigment epithelium, choroidal atrophy, and secondary choroidal neovascularization as PDT-induced adverse events,Citation7,Citation9 and, if an equivalent therapeutic effect can be obtained, the lower-fluence PDT used in our method of treatment may make it superior to that reported by Goto et al.Citation8
The main limitation of this study was that it was short-term and retrospective with a small number of cases. To establish the most effective and safest PDT protocol for treating ISPED, further studies are required that investigate long-term courses of treatment in larger numbers of patients compared with controls (untreated cases).
Conclusion
Excellent therapeutic results were obtained in two patients with ISPED in whom ICGA revealed choroidal hyperpermeability, who were treated with RFPDT at a reduced fluence of 25 J/cm2.
Acknowledgments
This study was supported by a grant from the Vehicle Racing Commemorative Foundation (TH and HT).
Disclosure
The authors report no conflicts of interest in this work.
References
- MeredithTABraleyREAabergTMNatural history of serous detachments of the retinal pigment epitheliumAm J Ophthalmol197988464365192197
- LewisMLIdiopathic serous detachment of the retinal pigment epitheliumArch Ophthalmol1978964620624646687
- GiovanniniAScassellati-SforzoliniBD’AltobrandoEMariottiCRutiliTTittarelliRChoroidal findings in the course of idiopathic serous pigment epithelium detachment detected by indocyanine green videoangiographyRetina19971742862939279943
- ChanWMLamDSLaiTYTamBSLiuDTChanCKChoroidal vascular remodelling in central serous chorioretinopathy after indocyanine green guided photodynamic therapy with verteporfin: a novel treatment at the primary disease levelBr J Ophthalmol200387121453145814660450
- YannuzziLASlakterJSGrossNEIndocyanine green angiography-guided photodynamic therapy for treatment of chronic central serous chorioretinopathy: a pilot studyRetina200323328829812824827
- Cardillo PiccolinoFEandiCMVentreLRigault de la LongraisRCGrignoloFMPhotodynamic therapy for chronic central serous chorioretinopathyRetina200323675276314707823
- ReibaldiMCardasciaNLongoAStandard-fluence versus low-fluence photodynamic therapy in chronic central serous chorioretinopathy: a nonrandomized clinical trialAm J Ophthalmol20101492307315. e219896635
- GotoSGomiFUenoCNishidaKReduced-fluence photodynamic therapy for subfoveal serous pigment epithelial detachment with choroidal vascular hyperpermeabilityAm J Ophthalmol20121545865871. e122840480
- OhkumaYHayashiTSakaiTWatanabeATsuneokaHOne-year results of reduced fluence photodynamic therapy for central serous chorioretinopathy: the outer nuclear layer thickness is associated with visual prognosisGraefes Arch Clin Exp Ophthalmol201325181909191723456099
- MudvariSSGoffMJFuADThe natural history of pigment epithelial detachment associated with central serous chorioretinopathyRetina20072791168117318046220