
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Purpose
To investigate cycloplegic refraction and ocular alignment in a population of preterm children at 1 and 6 years old.
Patients and methods
We included 261 preterm infants with a birth weight ≤1,500 g and a gestational age ≤32 weeks; there were 217 preterm infants (group 1), 28 preterm infants with mild retinopathy of prematurity (ROP) (group 2), and 16 preterm infants affected by severe ROP (group 3). Each patient underwent retinoscopy, ocular alignment assessment, and fundus examination at 1 and 6 years old.
Results
The prevalence of refractive errors and ocular alignment abnormalities at 1 year old in groups 2 and 3 compared to group 1 were, respectively (P<0.05): myopia 18% and 40.6% versus 6.9%; hyperopia 28.6% and 22% versus 39.2%; astigmatism 53.4% and 37.4% versus 53.9%; and strabismus 12.5% and 38% versus 5.3%. At 6 years old, they were, respectively (P<0.05): myopia 10.8% and 28.4% versus 7.4%; hyperopia 48.3% and 40.5% versus 62%; astigmatism 40.9% and 31.1% versus 30.6%; and strabismus 25% and 56.25% versus 11.5%.
Conclusion
At 6 years old, we observed increased rates of both hyperopia and strabismus in all groups compared to 1-year-old children. In preterm children with mild and severe ROP, we recorded increased rates of myopia and strabismus versus preterm children without ROP, and the risk of developing these disorders increased significantly with ROP severity. Astigmatism at 1 year old is not predictive of further development during growth. Patients born prematurely should be informed of the possible risks of ocular alterations due to refractive and ocular component changes.
Introduction
Neonatal care has increased the survival rates of extremely preterm infants with birth weights (BW) ≤1,000 g, or a gestational age (GA) ≤28 weeks; at the same time retinopathy of prematurity (ROP) has become a major threat to visual function.Citation1–Citation3
ROP is the most widely recognized cause of visual impairment following preterm birth, and it is defined as a vision-threatening disease.Citation4 ROP is responsible for up to 15% of all causes of blindness in Western countries, and up to 60% in developing countries.Citation4 A number of risk factors are implicated in the development of ROP, the most widely recognized of which is the degree of immaturity measured by BW and GA, together with prolonged exposure to supplementary oxygen.Citation1–Citation3 ROP is a biphasic disease that has an initial phase of retinal vessel growth retardation (from birth to 30–32 weeks), and a second phase of vessel proliferation (around 32–34 weeks postmenstrual age).Citation5,Citation6 Serious retinopathy until tractional retinal detachment occurs in 10%–15% of infants with a BW of <1,200 g. Children with ROP are known to develop refractive errorsCitation7 such as myopia, hyperopia, astigmatism, anisometropia, and other alterations in ocular alignment.Citation8,Citation9
Few studies in the literature have reported the prevalence of refractive errors and strabismus in preterm infants at different stages of growth.Citation10,Citation11 In particular, several authors described the impact of myopia and its association with prematurity.Citation12,Citation13 Myopia of prematurity (MOP) is one of these features, and it is represented by the arrested development of the anterior segment, irrespective of ROP, which is different from physiological myopia and myopia secondary to severe ROP.Citation14,Citation15
The aim of the present study was to define a long-term evaluation of cycloplegic refraction errors and ocular alignment abnormalities in a population of preterm children with and without ROP at 1 year and 6 years of age, resulting from the close collaboration of our Department of Surgical and Morphological Sciences (University of Insubria, Varese, Italy) and Neonatology Unit (Ospedale Filippo Del Ponte, Varese, Italy).
Patients and methods
In this observational retrospective study, we examined all preterm infants born between January 1, 1997 and December 31, 2005 at our Neonatology Unit. We considered all infants with a BW of ≤1,500 g and a GA of ≤32 weeks as preterm.
A total of 261 consecutive preterm patients were enrolled. Exclusion criteria were the presence of congenital cataract or corneal opacities, severe ocular or systemic malformations precluding refractive examination or ocular alignment evaluation, patients having undergone ocular surgery for severe ROP, and patients without complete medical records. Infants with mild or severe ROP, and those treated with laser therapy or cryotherapy according to standard clinical protocols, were included in the study. Informed consent was obtained from the parents of the study participants. The study conformed to the tenets of the Declaration of Helsinki.
Patients were subdivided into one of three groups. In presence of ROP, we defined stages 1 and 2 as “mild” ROP, and stages 3, 3 plus, 4, and 5 as “severe” ROP. Visual refraction, ocular alignment, and fundus examination were documented on clinical files for all included patients at 12 months and 72 months from birth, and these were inserted into our informatics database. With respect to visit scheduling, we considered acceptable an interval of ±45 days for the visit at month 12 and of ±3 months for the visit at the year 6.
Visual refraction was assessed by retinoscopy. Cycloplegic refraction was measured after three instillations of 1% cyclopentolate eye drops at 10-minute intervals before the examination. Spherical refraction, cylindrical power, and astigmatic axis were assessed for each eye. Refractive errors were defined as the mean spherical equivalent (MSE):
[1]
Myopia was divided into three categories according to diopter (absolute value): ≤3 D; >3 and ≤6 D; >6 D. Hyperopia was divided into two groups: ≤3 D and >3 D. Astigmatism was divided into two groups (absolute value): ≤1.5 D and >1.5 D. We defined refractive anisometropia as a difference between both eyes that was >1.5 D.
The ocular alignment of preterm children was studied using the cover test. We defined heterophoria as deviations that were kept latent by a fusion mechanism, and heterotropia was regarded as deviations not kept in check by fusion; these were measured using the prism and/or cover test, as well as the Krimsky prism reflex test.Citation16 Hence, we only considered heterotropia as a clinically significant ocular deviation (strabismus); we evaluated and reported the presence of heterophorias only as functional defect; it was not significant with respect to the data collected.
The presence of nystagmus was recorded and ocular movements were assessed to detect abnormalities. Binocular function was evaluated with the Lang Stereotest 1.Citation17
The fundus examination was performed using indirect ophthalmoscopy with a Schepens ophthalmoscope (HEINE OMEGA 200®; HEINE Optotechnik, Herrsching, Germany). Fundus characteristics and any ROP-related structural sequelae in children were described as normal findings (in the absence of pathological features) or as pathological findings in presence of vessel tortuosity, disc pallor, macular distortion or dragging, macular folds, tractional retinal detachment, and as a result of laser therapy or cryotherapy.
Cycloplegic refraction and ocular alignment were compared in patients without ROP to those with mild and severe ROP at 1 and 6 years of age to evaluate significant changes. A computerized database was established to facilitate data management and statistical analysis using commercial software (Excel 2007; Microsoft Corporation, Redmond, WA, USA) and GraphPad version 4 (GraphPad Software, Inc., La Jolla, CA, USA). Two-sample paired t-tests were used to compare the mean values of the continuous variables between study groups. In all data analyses, a P-value <0.05 was considered statistically significant.
Results
According to the presence and stage of ROP, group 1 (434 eyes) included 217 preterm infants without signs of ROP. Group 2 (56 eyes) included 28 preterm infants with mild ROP. Group 3 (32 eyes) included 16 preterm infants with severe ROP. The summary statistics of the included patients are reported in , which shows the mean GA and weight at birth in the three different groups. The refractive status and ocular alignment rates are shown in and .
Figure 1 Refractive error prevalence at 1 year old and 6 years old in all groups.
Abbreviation: ROP, retinopathy of prematurity.
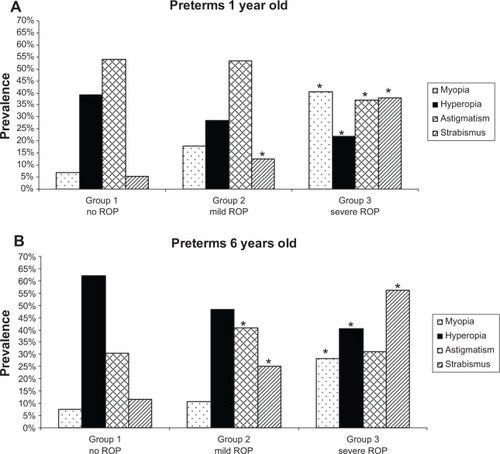
Figure 2 Refractive error prevalence at 1 year old and 6 years old in all groups.
Abbreviation: ROP, retinopathy of prematurity.
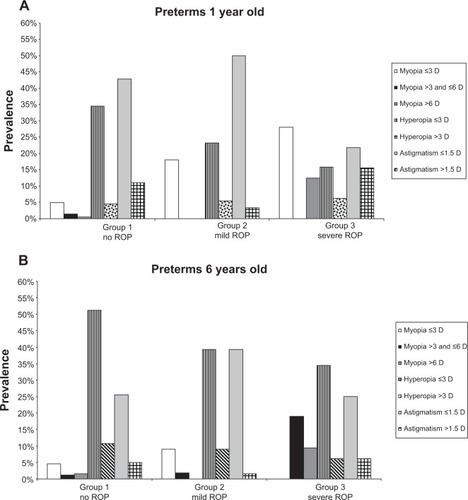
Table 1 Summary statistics of the enrolled patients
In groups 1 and 2, the most represented refractive error at 1 year old was astigmatism (54% and 53%, respectively), while at 6 years old it was hyperopia (62% and 48%, respectively). In group 3, myopia was the most represented refractive error at 1 year old (41%), and hyperopia was the most represented at 6 years old (41%). showed the same rates, which were classified according to the refractive values. Significant anisometropia (≥1.5 D) was reported in three patients in group 1, two patients in group 2, and four patients in group 3.
With regard to ocular alignment, the most frequent deviation in each group was esotropia, both at 1 year old (Group 1, 3.4%; Group 2, 7.1%; Group 3, 21%) and at 6 years old (Group 1, 8.2%; Group 2, 15%; Group 3, 31.25%).
Only two cases of nystagmus were observed in group 1; three cases of nystagmus were identified in group 3.
Discussion
The most active stage of ocular development is known to be from 6 months in utero to term.Citation5 While previous studies focus particularly on the development of myopia, in the present study, we have considered all refractive errors – myopia, hyperopia, and astigmatism – together with the presence of strabismus at two different stages of infant growth.
Myopia is present in preterm infants, and its prevalence increases with the degree of prematurity and with ROP severity.Citation18–Citation20 Some authors have already described three types of myopia associated with prematurity.Citation12,Citation13 The first is physiological myopia, which is associated with premature birth and stage of gestation. It is secondary to a flat anterior chamber, increased corneal curvature, and a spherical lens. The second type is called MOP, which is the arrested development of the anterior segment, occurs irrespective of ROP. MOP is characterized by a short axial length, a shallow anterior chamber, and a thick lens.Citation14,Citation15 The third type of myopia is secondary to severe ROP. It can vary from mild to severe, and it is stable throughout childhood. In our study ( and ), the prevalence of myopia was significantly higher in preterm children with severe ROP, compared with those without ROP at 1 year old (40.6% versus 7%, respectively; P<0.05) and 6 years old (28% versus 7%, respectively; P<0.05). Moreover, at 6 years old, in accordance with Garcia-Valenzuela and Kaufman in 2005,Citation20 our study underlined incremental rates of myopia that were higher than 3 D in patients with severe ROP compared with patients with mild or no ROP, probably due to a mechanism of altered anterior segment development ().
It is known that infants at term are commonly hypermetropic, and this kind of refractive error is primarily axial.Citation21 clearly shows the increased prevalence of hyperopia in each study group at 6 years old compared to the situation observed at 1 year old. O’Connor et alCitation22 reported that 20.5% of preterm eyes become more hyperopic at age 10 years. In accordance with Haugen et alCitation23 our study showed that hypermetropic refractive error was prevalent between 0 D and 3 D rather than >3 D at both visits (). High hyperopia was found in only one child, who was affected by microphthalmia and severe ROP, which was treated with cryotherapy.
The prevalence of astigmatism, in accordance with Larsson and Holmström,Citation24 decreased in all groups at 6 years old compared to the situation at 1 year old (). Corneal curvature might be influenced by prematurity, and some studies have suggested that abnormally steep curvature disappears gradually during infancy.Citation25 The presence of astigmatism might be caused by an arrest in the normal process of emmetropization.Citation26 It is well known that preterm birth influences the process of emmetropization by arresting the development of the anterior segment (induced by temperature decreases during corneal growth), or by causing biological stress (retinopathy).Citation7,Citation27,Citation28 In contrast with the evidence we observed with patients who were 6 years old, Theng et alCitation29 found increasing degrees of astigmatism in premature infants during the first 3 years. Our study concluded that the presence of astigmatism at 1 year old is not predictive of further development of this defect during a child’s development ( and ).
The high incidence of strabismus in preterm children has an unclear pattern of development and etiology, which has implications for its management. Strabismus may be attributed to ROP, increased refractive errors, anisometropia, BW, and neurological impairment.Citation30,Citation31 Shah et alCitation32 described occipital brain volume reduction in preterm children affected by strabismus. Schalij-Delfos et alCitation33 found that the rate of strabismus increases with decreasing GA. The incidence of strabismus in our study () was significantly higher in preterm children with mild and severe ROP (P<0.05) when compared to children without ROP at 1 year and 6 years of age. Moreover, manifest strabismus was associated with hyperopia (esotropia), and in many cases with myopia (exotropia), but further investigation in this area is needed. Many authors have found that the onset of strabismus in preterm infants is variable, which influences the planning of long-term follow-up and care.Citation34,Citation35
We found that nine out of 217 preterm children (1.6%) were affected by anisometropia. In accordance with other authors, we noted a low prevalence of anisometropia in ROP patients (six ROP cases): ROP is always symmetric in both eyes and it doesn’t represent a risk factor for a different ocular development might be influenced in the same way.Citation36,Citation37
This study presented some limits. 1) The number of patients included in groups 2 and 3 presenting with different stages of ROP is limited, as the treatment of preterm children nowadays has changed and severe stages of ROP are rare. 2) Astigmatism was evaluated using retinoscopy rather than keratometry. This modality was necessary in order to make this evaluation possible in infants, as keratometry requires good patient/physician collaboration; moreover, a cycloplegic autorefraction/autokeratometry was not available. 3) Many authors have previously studied the relationship between refractive errors and premature birth: some differences in the prevalence rates of myopia, hyperopia, astigmatism, and anisometropia can be largely attributed to the different BW and GA criteria used to define a preterm infant.Citation8,Citation11,Citation16,Citation38
Conclusion
Refractive errors and strabismus are common in preterm children. We observed increasing rates of both hyperopia and strabismus in all preterm children at 1 year and 6 years old, and these findings might be considered as refractive sequelae of preterm birth. Our study shows that the rate of astigmatism measured via retinoscopy might be a marker of eye immaturity in all preterm children. As per the findings in the literature, decreased prevalence of astigmatism at 6 years old might explain the progressive development and modification of anterior segment structures (mostly corneal curvature). The prevalence of myopia and strabismus in preterm children with ROP is significantly higher (P<0.05) than in those without ROP, and the risk of these disorders increases significantly (P<0.05) with the severity of ROP.
These disorders must all be recognized early in preterm children. Particularly in patients with ROP, early and long-term follow up is important for correct lens prescription to avoid severe amblyopia in adulthood. Moreover, in our study, we found that the presence of astigmatism at 1 year old is not predictive of the further development of this defect during child growth. The importance of ophthalmological visits in childhood should be emphasized. Further studies are needed to examine refractive error changes in preterm patients during adolescence up to adulthood.
Acknowledgments
The authors thank Michael John (BA) of the San Raffaele Medical School for the English language editing of this manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChenCZhangQSAdvances in medical care for extremely low birth weight infants worldwideZhongguo Dang Dai Er Ke Za Zhi2013158703707 Chinese23965891
- MccolmJRFleckBWRetinopathy of prematurity: causationSemin Neonatol20016645346012014886
- GogatePGilbertCZinASevere visual impairment and blindness in infants: causes and opportunities for controlMiddle East Afr J Ophthalmol201118210911421731320
- GilbertCFielderAGordilloLInternational NO-ROP GroupCharacteristics of infants with severe retinopathy of prematurity in countries with low, moderate, and high levels of development: implications for screening programsPediatrics20051155e518e52515805336
- HellströmASmithLEDammannORetinopathy of prematurityLancet201338299021445145723782686
- ChenJStahlAHellstromASmithLECurrent update on retinopathy of prematurity: screening and treatmentCurr Opin Pediatr201123217317821150442
- IbarraMSCaponeARetinopathy of prematurity and anterior segment complicationsOphthalmol Clin North Am2004174577582vii15533751
- GoktasASenerECSanacASAn assessment of ocular morbidities of children born prematurely in early childhoodJ Pediatr Ophthalmol Strabismus201249423624122329549
- O’ConnorARWilsonCMFielderAROphthalmological problems associated with preterm birthEye (Lond)200721101254126017914427
- WangJRenXShenLYanniSELefflerJNBirchEEDevelopment of refractive error in individual children with regressed retinopathy of prematurityInvest Ophthalmol Vis Sci20135496018602423920368
- ChenTCTsaiTHShihYFLong-term evaluation of refractive status and optical components in eyes of children born prematurelyInvest Ophthalmol Vis Sci201051126140614820688740
- QuinnGEDobsonVDavittBVEarly Treatment for Retinopathy of Prematurity Cooperative GroupProgression of myopia and high myopia in the Early Treatment for Retinopathy of Prematurity study: findings at 4 to 6 years of ageJ AAPOS201317212412823622444
- NissenkornIYassurYMashkowskiDSherfIBen-SiraIMyopia in premature babies with and without retinopathy of prematurityBr J Ophthalmol19836731701736687430
- FielderARQuinnGEMyopia of prematurity: nature, nurture, or disease?Br J Ophthalmol1997811239135397
- FledeliusHCPreterm delivery and subsequent ocular development. A 7–10 year follow-up of children screened 1982–84 for ROP. 3) Refraction. Myopia of prematurityActa Ophthalmol Scand19967432973008828731
- ChoiRYKushnerBJThe accuracy of experienced strabismologists using the Hirschberg and Krimsky testsOphthalmology19981057130113069663237
- SchmidMLargoRHVisual acuity and stereopsis between the ages of 5 and 10 years. A cross-sectional studyEur J Pediatr198614564754793493140
- QuinnGEDobsonVKivlinJPrevalence of myopia between 3 months and 5 1/2 years in preterm infants with and without retinopathy of prematurity. Cryotherapy for Retinopathy of Prematurity Cooperative GroupOphthalmology19981057129213009663236
- GalloJEFagerholmPLow-grade myopia in children with regressed retinopathy of prematurityActa Ophthalmol (Copenh)19937145195238249585
- Garcia-ValenzuelaEKaufmanLMHigh myopia associated with retinopathy of prematurity is primarily lenticularJ AAPOS20059212112815838438
- DenisDBensoCWaryPFogliariniCChildhood refraction: epidemiology, progression, evaluation and a method for correcting ametropiaJ Fr Ophtalmol20042794395215547479
- O’ConnorARStephensonTJJohnsonATobinMJRatibSFielderARStrabismus in children of birth weight less than 1701 gArch Ophthalmol2002120676777312049582
- HaugenOHNepstadLStandalOAElgenIMarkestadTVisual function in 6 to 7 year-old children born extremely preterm: a population-based studyActa Ophthalmol201290542242721044277
- LarssonEKHolmströmGEDevelopment of astigmatism and anisometropia in preterm children during the first 10 years of life: a population-based studyArch Ophthalmol2006124111608161417102009
- FrilingRWeinbergerDKremerIAvisarRSirotaLSnirMKeratometry measurements in preterm and full term newborn infantsBr J Ophthalmol200488181014693760
- ChoiMYParkIKYuYSLong-term refractive outcome in eyes of preterm infants with and without retinopathy of prematurity: comparison of keratometric value, axial length, anterior chamber depth, and lens thicknessBr J Ophthalmol200084213814310655187
- KentDPennieFLawsDWhiteSClarkDThe influence of retinopathy of prematurity on ocular growthEye (Lond)200014Pt 1232910755095
- FledeliusHCJensenHLate subsequent ocular morbidity in retinopathy of prematurity patients, with emphasis on visual loss caused by insidious ‘involutive’ pathology: an observational seriesActa Ophthalmol201189431632320055773
- ThengJTWongTYLingYRefractive errors and strabismus in premature Asian infants with and without retinopathy of prematuritySingapore Med J200041839339711256347
- LarssonEKRydbergACHolmströmGEA population-based study of the refractive outcome in 10-year-old preterm and full-term childrenArch Ophthalmol2003121101430143614557179
- BremerDLPalmerEAFellowsRRStrabismus in premature infants in the first year of life. Cryotherapy for Retinopathy of Prematurity Cooperative GroupArch Ophthalmol199811633293339514486
- ShahDKGuinaneCAugustPReduced occipital regional volumes at term predict impaired visual function in early childhood in very low birth weight infantsInvest Ophthalmol Vis Sci20064783366337316877404
- Schalij-DelfosNEde GraafMETreffersWFEngelJCatsBPLong-term follow up of premature infants: detection of strabismus, amblyopia, and refractive errorsBr J Ophthalmol200084996396710966945
- KushnerBJStrabismus and amblyopia associated with regressed retinopathy of prematurityArch Ophthalmol198210022562616895993
- HolmströmGel AzaziMKugelbergUOphthalmological follow up of preterm infants: a population based, prospective study of visual acuity and strabismusBr J Ophthalmol199983214315010396188
- CookeRWFoulder-HughesLNewshamDClarkeDOphthalmic impairment at 7 years of age in children born very pretermArch Dis Child Fetal Neonatal Ed2004893F249F25315102730
- DarlowBAClemettRSHorwoodLJMogridgeNProspective study of New Zealand infants with birth weight less than 1500 g and screened for retinopathy of prematurity: visual outcome at age 7–8 yearsBr J Ophthalmol199781119359409505814
- YangCSWangAGSungCSHsuWMLeeFLLeeSMLong-term visual outcomes of laser-treated threshold retinopathy of prematurity: a study of refractive status at 7 yearsEye (Lond)2010241142019343053