
Abstract
Background
The purpose of this study was to investigate treatment outcomes in 360° suture trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation (360P-LOT + DS)
Methods
Thirty-two eyes in 32 consecutive patients treated by 360P-LOT + DS for primary open angle glaucoma with coexisting cataracts at Sato Eye Clinic from March 2011 to April 2013 were retrospectively compared with 23 eyes in 23 consecutive patients treated by cataract surgery and 120° trabeculotomy with deep sclerectomy (120P-LOT + DS) at the same clinic from January 2010 to February 2011. The parameters investigated during the 15 months after surgery were the course of intraocular pressure, number of antiglaucoma medications, best-corrected visual acuity, and complications.
Results
Both groups showed a significant decrease in intraocular pressure starting at one month after surgery when compared with values before surgery. At 3, 6, 9, and 15 months after surgery, the intraocular pressure was significantly lower and the survival rate was significantly higher in the 360P-LOT + DS group compared with the 120P-LOT + DS group. The number of antiglaucoma medications, best-corrected visual acuity value, and complications did not differ significantly between the groups.
Conclusion
Although the complications are similar to those seen in 120P-LOT + DS, treatment of primary open angle glaucoma and coexisting cataracts using 360P-LOT + DS may yield better outcomes.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Introduction
The combination of phacoemulsification and intraocular lens implantation (PEA + IOL) with glaucoma surgery is widely performed to treat open angle glaucoma with coexisting cataract.Citation1–Citation11 Although trabeculectomy has provided excellent outcomes as a routine surgical procedure for glaucoma with poor intraocular pressure (IOP) control,Citation1–Citation3,Citation12 it has the disadvantage of having a higher incidence of complications, such as hypotony, choroidal effusion, cataract, and flat or shallow anterior chamber, compared with nonpenetrating surgery.Citation3,Citation12 Trabeculotomy (LOT) is a type of nonpenetrating surgery that involves opening Schlemm’s canal over 120°. It is effective not only for exfoliation glaucoma and congenital glaucoma,Citation4,Citation13 but also for primary open angle glaucoma (POAG).Citation5,Citation6,Citation10,Citation13 In addition, it has been found to further reduce the IOP when performed in combination with cataract surgery.Citation4,Citation5 Moreover, LOT combined with cataract surgery and deep sclerectomy (DS) has been found to achieve the same surgical outcomes as trabeculectomy with cataract surgery.Citation6
In 1995, Beck and Lynch reported on a technique in which there was a 360° incision of the trabecular meshwork (360° LOT) using a 6-0 polypropylene (Prolene, Ethicon Endo-Surgery, Blue Ash, OH, USA) suture to treat congenital glaucoma.Citation14 Although the IOP was reduced below 22 mmHg without eye drops in 85% of the cases, the effectiveness of this technique for other types of glaucoma was not determined. Using a modified procedure, Chin et al treated adults open angle glaucoma in 2012 and achieved a better effect than when using standard LOT, with the IOP decreasing to 13.1 mmHg at 12 months after surgery.Citation15 However, there have been no studies published in the literature on the IOP-lowering effect of this technique when combined with cataract surgery and DS.
We conducted a retrospective, comparative study of the postoperative clinical course and the incidence of complications in patients treated for POAG by 360° LOT combined with cataract surgery and DS (360P-LOT + DS) and in earlier patients treated by 120° LOT combined with cataract surgery and DS (120P-LOT + DS).
Subjects and methods
Subjects
Thirty-two eyes in 32 consecutive patients treated by 360P-LOT + DS for POAG with coexisting cataracts at Sato Eye Clinic from March 2011 to April 2013 were retrospectively compared with 23 eyes in 23 consecutive patients treated by 120P-LOT + DS at the same clinic from January 2010 to February 2011. The study targeted POAG with a coexisting visually significant cataract, and excluded exfoliation glaucoma, uveitic or neovascular secondary glaucoma, angle closure glaucoma, and history of intraocular surgery. The eyes (one eye per subject) had to be available for at least 15 months of follow-up, and in cases of bilateral surgery, the first eye operated on was studied.
A diagnosis of POAG was made if all of the following criteria were satisfied: presence of glaucomatous optic disc neuropathy (a cup/disc ratio of >0.7 or the presence of notching) accompanied by corresponding visual field defects; a threshold examination of SITA 24-2 showing a glaucoma hemifield test “outside normal limits”, and a cluster of three contiguous points on the pattern deviation plot depressed at a P-value of <5% (occurring in age-matched normal subjects) not crossing the horizontal meridian, which were compatible with glaucoma; and assessed as an open angle on gonioscopy.
After providing a written explanation to the patient and his/her family detailing the effects and potential complications of the surgery, each subject gave their written consent before the surgery. The study followed the tenets of the Declaration of Helsinki. All subjects were operated on by the same surgeon. The characteristics of each group are summarized in . While the duration of the postoperative follow-up was significantly different between the groups, there were no significant differences noted for sex, age, left or right eye, history of selective laser trabeculoplasty, mean preoperative IOP, number of antiglaucoma medications, or best-corrected visual acuity (BCVA).
Table 1 Preoperative characteristics for 360P-LOT + DS and 120P-LOT + DS
Surgical procedure PEA + IOL + 360° suture LOT with DS
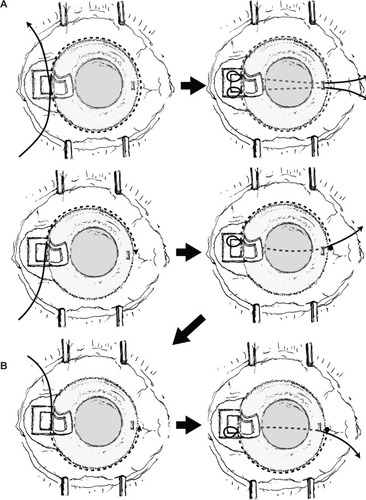
The temporal approach was adopted in all cases in order to preserve the upper conjunctiva. After making a conjunctival incision at the fornix base, we first created a 1/2 scleral thickness scleral flap measuring 4×4 mm in the exposed sclera, followed by creation of a second scleral flap inside the first flap that measured 3×3 mm. Subsequently, the inner wall of Schlemm’s canal was exposed and viscoelastic material was injected into the canal. A 5-0 nylon suture rounded at the tip by cautery was then inserted into Schlemm’s canal, passed through the perimeter, and pulled out from the opposite side. Next, the anterior chamber was filled with viscoelastic material and a small incision was made at the angle of the trabecular meshwork and inner wall of Schlemm’s canal (window) with a 30G needle. The suture was then passed through the anterior chamber from the same site and pulled from a corneal side port created on the side opposite the window, with both ends of the suture gently pulled, thereby completing the 360° LOT (). If the suture could not be passed around the entire perimeter of Schlemm’s canal and became stuck at, for example, 180°, an incision was made in the trabecular meshwork in that region only and the suture was retrieved. It was then reinserted in order to pass it through the remaining side of Schlemm’s canal before pulling it out from the corneal side port on the opposite side to incise the remaining half of the perimeter (). After this, PEA + IOL were performed at the same incision. The second scleral flap dissection was prolonged anteriorly for 1–1.5 mm in order to remove the sclerocorneal tissue behind the anterior trabeculum and Descemet’s membrane. When the anterior dissection between the corneal stroma and Descemet’s membrane was completed, the second scleral flap was removed by cutting anteriorly and the first flap was sutured using one to four sutures in order to allow slight leakage of the aqueous humor and create a filtration bleb that would suppress any transient postoperative elevation of the IOP. The procedure was completed using a continuous suture of the conjunctiva (10-0 nylon suture) in such a way to prevent leakage of the aqueous humor. Mitomycin C was not used during surgery.
Figure 1 Surgical procedure 360° suture trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation.
PEA + IOL + 120° LOT with DS
As with the previous procedure, after making a conjunctival incision at the fornix base, we first created a 1/2 scleral thickness scleral flap measuring 4×4 mm in the exposed sclera, followed by creation of a second scleral flap inside the first flap that measured 3×3 mm. After exposing Schlemm’s canal, a trabeculotome was inserted in both sides of the canal in order to make an incision over a total of 120°, and PEA + IOL was performed at the same incision. The second scleral flap was excised and the first scleral flap was sutured using one to four sutures in order to allow slight leakage of the aqueous humor and create a filtration bleb that would suppress any transient postoperative elevation of IOP. The procedure was completed using a continuous suture of the conjunctiva (10-0 nylon suture) in such a way as to prevent leakage of the aqueous humor. Mitomycin C was not used during surgery.
Study parameters and statistical evaluation
The four parameters studied included: IOP over time, number of antiglaucoma medications over time, BCVA over time, and complications. IOP, number of antiglaucoma medications, and BCVA are expressed as the mean and standard deviation.
IOP over time, preoperative and postoperative IOP, and IOP in the two groups were compared using the mean value of the three most recent measurements for the preoperative IOP and individual postoperative IOP values after one day, one week, and one, 3, 6, 9, 12, and 15 months. Survival analysis using the Kaplan–Meier method was also performed in order to evaluate the postoperative IOP and compared the results across the two groups. We defined three criteria for an IOP decrease at one or more months with or without antiglaucoma medications: ≥20% IOP reduction from baseline and an IOP ≤21 mmHg (category A), ≥30% IOP reduction from baseline and an IOP ≤18 mmHg (category B), and ≥40% IOP reduction from baseline and an IOP ≤15 mmHg (category C).
Failure was defined by three events that included: the first time the IOP exceeded the defined levels on two consecutive occasions, concomitant use of an oral carbonate dehydratase inhibitor, and performance of glaucoma surgery. Elevation of the IOP within the first postoperative month was excluded from the final determination of success or failure.
For the number of antiglaucoma medications, glaucoma eye drops were scored as one, combination drugs as two, and oral carbonate dehydratase inhibitors as two. However, none of the patients in the current analysis used any oral carbonate dehydratase inhibitors.
We investigated incidence and days until normalization of transient elevation of IOP as early postoperative complications, as is common in LOT. In addition, because we deliberately formed a filtration bleb by loosely suturing the first flap with the aim of suppressing any transient elevation of the IOP in both groups, we also evaluated the incidence of postoperative filtration bleb formation and the filtration bleb-related complications of hypotony, shallow anterior chamber, choroidal detachment, and hypotony maculopathy. In order to investigate the degree of anterior chamber hemorrhage, its severity was classified using the following scoring system. Disappearance of the anterior chamber hemorrhage within the first postoperative week was scored as one point, while protracted, visually significant anterior chamber hemorrhage lasting beyond the first postoperative week was scored as two points, and anterior chamber hemorrhage requiring surgery was scored as three points. In line with the study by Inatani et al we defined an IOP spike as when the IOP level was over 30 mmHg after surgery or had increased by over 5 mmHg compared with the IOP level on the previous day.Citation16 A filtration bleb was defined by the appearance of a conjunctival protuberance, while the presence or absence of anterior chamber hemorrhage and filtration bleb was determined from the medical chart and photographs of the anterior eye segment. Hypotony was defined as IOP ≤5 mmHg, and presence or absence of choroidal detachment and hypotony maculopathy were confirmed by ophthalmoscope.
GraphPad Prism version 6.01 (GraphPad Software, San Diego, CA, USA) was used for the statistical analysis. Fisher’s exact test was used for comparisons of sex, left and right eye, history of selective laser trabeculoplasty, and incidence of postoperative complications between the two procedures. Age, IOP, time to disappearance of postoperative filtration bleb, and time until normalization of hypotony and elevated IOP for the two procedures were compared using the Student’s t-test. BCVA, number of antiglaucoma medications, and postoperative anterior chamber hemorrhage score for the two procedures were compared using the Mann–Whitney U-test. Changes in the postoperative IOP over time were tested using a one-way analysis of variance while preoperative and postoperative comparisons were compared using Dunnett’s multiple comparison test. Changes in the number of antiglaucoma medications and BCVA over time were tested using the Kruskal–Wallis test, with preoperative and postoperative comparisons done using Dunn’s multiple comparison test. The Kaplan–Meier method was used for survival analysis of the postoperative IOP, and a log-rank test was used for comparison of the two procedures. The significance level was set at P<0.05.
Results
Preoperative characteristics for each group are shown in . No significant differences were found between the two groups for sex, age at surgery, left or right eye, previous history, preoperative IOP, number of antiglaucoma medications, and preoperative BCVA. The mean follow-up period was 14.5±1.0 months in the 360P-LOT + DS group and 15.0±0.2 months in the 120P-LOT + DS group, which was a significant difference (P<0.017, Mann–Whitney U-test).
Change in IOP over time
Changes in IOP over time in the 360P-LOT + DS group and 120P-LOT + DS group are shown in . In the 360P-LOT + DS group, the IOP (mean ± standard deviation) was 18.4±2.8 mmHg before surgery. Over the postoperative follow-up period, significant changes were seen, with values of 18.4±10.6 mmHg at one day after surgery, 16.5±8.3 mmHg after one week, 13.6±2.9 mmHg after one month, 12.1±2.0 mmHg after 3 months, 12.3±2.2 mmHg after 6 months, 12.3±2.0 mmHg after 9 months, 12.8±2.3 mmHg after 12 months, and 12.6±2.0 mmHg after 15 months (P<0.001, one-way analysis of variance). IOP at all follow-up points beginning from one month onwards were significantly lower than the preoperative value (each P<0.005, Dunnett’s multiple comparison test).
Figure 2 Changes in the mean IOP (mean ± standard error of the mean) from before to 15 months after surgery.
Abbreviations: 360P-LOT + DS, 360°suture trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation; 120P-LOT + DS, 120° trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation; IOP, intraocular pressure; preop, preoperative; d, day; w, week; m, month.
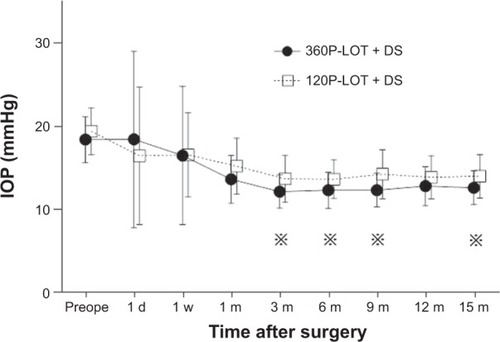
In the 120P-LOT + DS group, the IOP (mean ± standard deviation) was 19.4±2.8 mmHg before surgery. Over the postoperative follow-up period, significant changes were seen, with values of 16.4±8.3 mmHg at one day after surgery, 16.6±5.1 mmHg after one week, 15.2±3.4 mmHg after one month, 13.7±2.8 mmHg after 3 months, 13.6±2.3 mmHg after 6 months, 14.2±3.0 mmHg after 9 months, 13.8±2.6 mmHg after 12 months, and 14.0±2.6 mmHg after 15 months (P<0.001, one-way analysis of variance). IOP at all follow-up points beginning from one month onwards were significantly lower than the preoperative value (each P<0.005, Dunnett’s multiple comparison test).
Comparisons of the postoperative IOP between the two groups were significantly lower in the 360P-LOT + DS group than in the 120P-LOT + DS group at 3, 6, 9, and 15 months after surgery (P=0.021, P=0.036, P=0.007, and P=0.038, respectively, Student’s t-test).
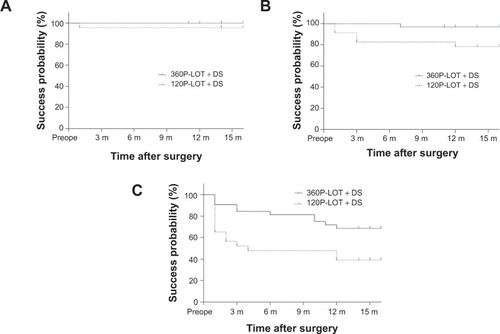
The results of the Kaplan–Meier survival analysis are shown in . Category A survival rate at 15 months was 100% in the 360P-LOT + DS group and 95.7% in the 120P-LOT + DS group, which were not significantly different (P=0.238, log-rank test). Category B and C survival rates in the 360P-LOT + DS group were 96.9% and 68.6%, and were significantly higher than the rates of 78.3% and 39.1% observed in the 120P-LOT + DS group (P=0.028 and P=0.017, respectively).
Figure 3 Kaplan–Meier survival curve with category A, B, and C.
Abbreviations: 360P-LOT + DS, 360° suture trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation; 120P-LOT + DS, 120° trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation; preop, preoperative; m, month.
Change in number of antiglaucoma medications over time
The number of antiglaucoma medications (mean ± standard deviation) in the 360P-LOT + DS and 120P-LOT + DS groups is shown in . The number of antiglaucoma medications in the 360P-LOT + DS group changed significantly over the follow-up period (P<0.001, Kruskal–Wallis test), with significantly lower than baseline values found at each of the follow-up points (each P<0.001, Dunn’s multiple comparison test). In the 120P-LOT + DS group, the number of antiglaucoma medications also changed significantly over the follow-up period (P<0.001, Kruskal–Wallis test), with significantly lower than baseline values found at one, 3, 6, 9, and 15 months after surgery (each P<0.05, Dunn’s multiple comparison test). There were no significant differences between the two groups at any of the follow-up points (Mann–Whitney U-test).
Table 2 Medications for 360P-LOT + DS and 120P-LOT + DS
BCVA over time
BCVA (mean ± standard deviation) in the 360P-LOT + DS and 120P-LOT + DS groups are shown in . BCVA in both groups changed significantly over the follow-up period (P<0.005, Kruskal–Wallis test). Significant improvement was observed for all of the follow-up points, beginning from one month onwards (each P<0.05, Dunn’s multiple comparison test). There were no significant differences between the two groups at any of the follow-up points (Mann–Whitney U-test). shows a scattergram of visual acuity before surgery and at 15 months after surgery. At 15 months after surgery, none of the patients had poorer visual acuity than before surgery.
Figure 4 Preoperative BCVA and BCVA 15 months after surgery (•, 360°P-LOT + DS group; ○, 120P-LOT + DS group).
Abbreviations: 360P-LOT + DS, 360° suture trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation; 120P-LOT + DS, 120° trabeculotomy with deep sclerectomy combined with phacoemulsification and aspiration and intraocular lens implantation; BCVA, best-corrected visual acuity.
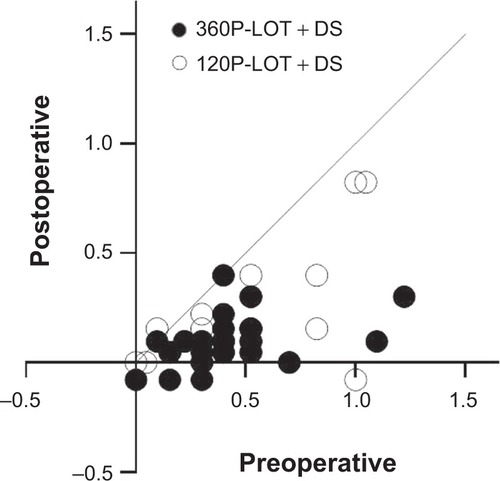
Table 3 Best corrected visual acuity for 360P-LOT + DS and 120P-LOT + DS
Complications
Complications are shown in . With regard to intraoperative complications, while all patients in each group experienced anterior chamber hemorrhage, none of the patients had anterior chamber flattening or Descemet’s detachment.
Table 4 Intraoperative and postoperative complications in 360P-LOT + DS and 120P-LOT + DS groups
Postoperative filtration blebs were observed in 20 eyes (62.5%) of the 360P-LOT + DS group and in ten eyes (43.5%) of the 120P-LOT + DS group; however, the difference between the groups was not significant (P=0.182). The mean time until disappearance of the filtration bleb was 4.6 days in the 360P-LOT + DS group and 5.0 days in the 120P-LOT +DS group (P=0.377).
Among the postoperative complications, IOP spiking occurred in eight eyes (25.0%) of the 360P-LOT + DS group and in three eyes (13.0%) of the 120P-LOT + DS group, although the difference between the groups was not significant (P=0.326). IOP decreased below 30 mmHg after a mean period of 6.8 days in the 360P-LOT + DS group and 2.3 days in the 120P-LOT + DS group. Hypotony of ≤5 mmHg due to hyperfiltration occurred in one eye (3.1%) of the 360P-LOT + DS group and in two eyes (8.7%) of the 120P-LOT + DS group, although the difference between the groups was not significant (P=0.565).
There was no hypotony-related choroidal detachment, shallow anterior chamber, or hypotony maculopathy, and the mean period required for the IOP to increase to ≥5 mmHg was 4.0 days in the 360P-LOT + DS group and 2.5 days in the 120P-LOT + DS group.
The anterior chamber hemorrhage score was 1.28±0.58 in the 360P-LOT + DS group, and did not differ significantly from the value of 1.13±0.34 in the 120P-LOT + DS group (P=0.864). In two patients in the 360P-LOT + DS group, anterior chamber lavage was performed on day 8 after surgery because of prolonged massive anterior chamber hemorrhage [defined by Inatani et al as when the meniscus of the hyphema (anterior chamber hemorrhage) is present around the pupil and lasts for at least 7 daysCitation16].
Discussion
Nonpenetrating glaucoma surgery combined with cataract surgery has been reported as an effective means of treating open angle glaucoma and visually significant cataract.Citation3–Citation5,Citation7–Citation9 In 2008, a new surgical technique combining phacotrabeculotomy and DS (120P-LOT + DS) showed significant IOP reduction and a success rate which might be comparable with that of the current standard phacotrabeculectomy.Citation6 With the goal of further reducing the IOP and comparing outcomes of these two procedures, our current study performed 360P-LOT + DS, which modifies 120P-LOT + DS by extending the angle of incision of the inner wall of Schlemm’s canal from 120° to 360°.
Because the IOP was relatively well controlled by eye drops in many of the patients in this study who underwent surgery for POAG and coexisting visually significant cataract, the number of antiglaucoma medications and preoperative IOP levels were not high. However, the number of antiglaucoma medications and IOP levels did decrease further after the surgery in these patients.
At 15 months after surgery, the IOP was 12.6 mmHg in the 360P-LOT + DS group and 14.0 mmHg in the 120P-LOT + DS. Further, the average IOP value at 3, 6, 9, and 15 months after surgery in the 360P-LOT + DS group was approximately 13 mmHg, which was significantly lower than the IOP value in the 120P-LOT + DS group. In the Kaplan–Meier survival analysis, both groups had good outcomes in category A, with no significant difference between the groups. However, the survival rates for categories B and C in the 360P-LOT + DS group were 96.9% and 68.6%, and were 78.3% and 39.1% in the 120P-LOT + DS group. These rates were significantly higher for the 360P-LOT + DS group.
Trabeculotomy ab externo is thought to relieve resistance to aqueous outflow by mechanical cleavage of the trabecular meshwork and the inner wall of Schlemm’s canal.Citation5,Citation10,Citation16 According to a histological study of the mechanism of repair of the internal wall of Schlemm’s canal after LOT in monkey eyes, repair of the incised part began about 3 months after surgery, and by 12 months had almost achieved the baseline condition present before surgery. However, 72-month results post-LOT combined with cataract surgeries for POAG and coexisting cataract have demonstrated that this is a suitable method for lowering IOP and reducing antiglaucoma medications.Citation5 Even if tissue repair occurs, resistance to aqueous outflow would be expected to be alleviated over the long term.
In this study, in both groups, the IOP reduction was attributed to the effect of the cataract surgery itself,Citation17 an increase in conventional outflow due to incision of Schlemm’s canal by LOT,Citation10,Citation16 and increased filtration into the subconjunctival space and uveoscleral outflow due to DS.Citation6,Citation11,Citation18 The difference in procedure between the two groups was the width of the Schlemm’s canal incisions. Therefore, 360P-LOT + DS probably results in lower postoperative IOP and higher survival rates than 120P-LOT + DS by a wider range incision of the inner wall of Schlemm’s canal, as Chin et al have reported.Citation15
In our current study, the number of antiglaucoma medications was reduced significantly in both groups during the first postoperative month compared with numbers before surgery, with no significant difference found between the groups. Given that the number of antiglaucoma medications before and after surgery did not differ between the two groups, it is unlikely that differences in medication had an effect on the IOP changes before and after surgery. Thus, the lower IOP level and the significantly higher survival rate in the 360P-LOT + DS group compared with the 120P-LOT + DS group were thought to be due to the effect of the surgery itself rather than the medication.
In both groups, BCVA improved from one month after surgery compared with before surgery. In addition, none of the patients had a poorer BCVA after 15 months as compared with before surgery. Both groups followed a similar course, with no significant differences observed between the groups.
With regard to the intraoperative complications, although all patients in each group had anterior chamber hemorrhage, there were no other complications observed. There were also no significant intergroup postoperative differences for the incidence of IOP spike, incidence of hypotony to ≤5 mmHg, or anterior chamber hemorrhage score. Two eyes in the 360P-LOT + DS group underwent anterior chamber lavage on postoperative day 8. Inatani et al have previously defined prolonged massive anterior chamber hemorrhage as when the meniscus of the anterior chamber hemorrhage is present around the pupil and lasts for at least 7 days. They reported finding that it was possible to lower an elevated IOP of ≥30 mmHg by performing anterior chamber lavage.Citation16 In our study, there was normalization of the IOP on the day after we performed anterior chamber lavage in one patient who complained strongly of a loss of visual acuity, and in one other patient who had IOP elevated above 30 mmHg. Thus, as described by Inatani et alCitation16 anterior chamber lavage should probably be performed in 360P-LOT + DS cases having prolonged massive anterior chamber hemorrhage that lasts more than one week and who have an elevated IOP of ≥30 mmHg.
There are some limitations in our current study. These include the small number of subjects, the short observation period, the fact that all patients were operated on by the same surgeon, the lack of randomization, and the retrospective study design. The last two in particular were major limitations, and there is a need for further long-term, prospective, randomized studies.
In conclusion, despite similar complications to those seen in 120P-LOT + DS, our study suggests that treatment of POAG and coexisting cataracts by 360P-LOT + DS may yield better outcomes.
Disclosure
The authors report no conflicts of interest in this work.
References
- Ogata-IwaoMInataniMTakiharaYInoueTIwaoKTaniharaHA prospective comparison between trabeculectomy with mitomycin C and phacotrabeculectomy with mitomycin CActa Ophthalmol2013916e500e50123617934
- CassonRJSalmonJFCombined surgery in the treatment of patients with cataract and primary open-angle glaucomaJ Cataract Refract Surg200127111854186311709261
- MatlachJFreibergFJLeippiSGrehnFKlinkTComparison of phacotrabeculectomy versus phacocanaloplasty in the treatment of patients with concomitant cataract and glaucomaBMC Ophthalmol201313123360243
- FukuchiTUedaJNakatsueTSudaKHaraHAbeHTrabeculotomy combined with phacoemulsification, intraocular lens implantation and sinusotomy for exfoliation glaucomaJpn J Ophthalmol201155320521221559910
- HoffmannESchwennOKarallusMKrummenauerFGrehnFPfeifferNLong-term results of cataract surgery combined with trabeculotomyGraefes Arch Clin Exp Ophthalmol200224012611954776
- LukeCDietleinTSLukeMKonenWKrieglsteinGKA prospective trial of phaco-trabeculotomy combined with deep sclerectomy versus phaco-trabeculectomyGraefes Arch Clin Exp Ophthalmol200824681163116818414886
- Arriola-VillalobosPMartinez-de-la-CasaJMDiaz-ValleDMidterm evaluation of the new Glaukos iStent with phacoemulsification in coexistent open-angle glaucoma or ocular hypertension and cataractBr J Ophthalmol201397101250125523603758
- CravenERKatzLJWellsJMGiamporcaroJEiStent Study GroupCataract surgery with trabecular micro-bypass stent implantation in patients with mild-to-moderate open-angle glaucoma and cataract: two-year follow-upJ Cataract Refract Surg20123881339134522814041
- Arriola-VillalobosPMartinez-de-la-CasaJMDiaz-ValleDFernandez-PerezCGarcia-SanchezJGarcia-FeijooJCombined iStent trabecular micro-bypass stent implantation and phacoemulsification for coexistent open-angle glaucoma and cataract: a long-term studyBr J Ophthalmol201296564564922275344
- HonjoMTaniharaHNegiATrabeculotomy ab externo, cataract extraction, and intraocular lens implantation: preliminary reportJ Cataract Refract Surg19962256016068784634
- LeszczynskiRForminska-KapuscikMBubala-StachowiczBMrukwa-KominekEFilipekEPawlickiKNonpenetrating very deep sclerectomy with hyaluronic acid implant vs trabeculectomy – a 2-year follow-upGraefes Arch Clin Exp Ophthalmol2012250121835184122569857
- RulliEBiagioliERivaIEfficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: a systematic review and meta-analysisJAMA Ophthalmol2013131121573158224158640
- NambuHJoNKuroMLong-term surgical results of initial trabeculotomy combined with sinusotomy performed inferiorlyNihon Ganka Gakkai Zasshi20121168740750 Japanese22973738
- BeckADLynchMG360 degrees trabeculotomy for primary congenital glaucomaArch Ophthalmol19951139120012027661757
- ChinSNittaTShinmeiYReduction of intraocular pressure using a modified 360-degree suture trabeculotomy technique in primary and secondary open-angle glaucoma: a pilot studyJ Glaucoma201221640140721543994
- InataniMTaniharaHMutoTTransient intraocular pressure elevation after trabeculotomy and its occurrence with phacoemulsification and intraocular lens implantationJpn J Ophthalmol200145328829211369380
- DamjiKFKonstasAGLiebmannJMIntraocular pressure following phacoemulsification in patients with and without exfoliation syndrome: a 2 year prospective studyBr J Ophthalmol20069081014101816672324
- DrolsumLLongterm follow-up after deep sclerectomy in patients with pseudoexfoliative glaucomaActa Ophthalmol Scand200684450250616879571