
Abstract
Purpose
To investigate repeatability of steep and flat keratometry measurements, as well as astigmatism axis in cohorts with normal range and regular astigmatic such as: eyes following laser-assisted in situ keratomileusis (LASIK) and normal population, as well as cohorts of high and irregular astigmatism such as keratoconic eyes, and keratoconic eyes following corneal collagen cross-linking, employing a novel corneal reflection topography device.
Methods
Steep and flat keratometry and astigmatism axis measurement repeatability was investigated employing a novel multicolored-spot reflection topographer (Cassini) in four study groups, namely a post myopic LASIK-treated Group A, a keratoconus Group B, a post-CXL keratoconus Group C, and a control Group D of routine healthy patients. Three separate, maps were obtained employing the Cassini, enabling investigation of the intra-individual repeatability by standard deviation. Additionally we investigated in all groups,the Klyce surface irregularity indices for keratoconus, the SAI (surface asymmetry index) and the SRI (surface regularity index).
Results
Flat keratometry repeatability was 0.74±0.89 (0.03 to 5.26) diopters (D) in the LASIK Group A, 0.88±1.45 (range minimum to maximum, 0.00 to 7.84) D in the keratoconic Group B, and 0.71±0.94 (0.02 to 6.23) D in the cross-linked Group C. The control Group D had flat keratometry repeatability 0.36±0.46 (0.00 to 2.71) D. Steep keratometry repeatability was 0.64±0.82 (0.01 to 4.81) D in the LASIK Group A, 0.89±1.22 (0.02 to 7.85) D in the keratoconic Group B, and 0.93±1.12 (0.04 to 5.93) D in the cross-linked Group C. The control Group D had steep keratometry repeatability 0.41±0.50 (0.00 to 3.51) D. Axis repeatability was 3.45±1.62° (0.38 to 7.78°) for the LASIK Group A, 4.12±3.17° (0.02 to 12.13°) for the keratoconic Group B, and 3.20±1.99° (0.17 to 8.61°) for the cross-linked Group C. The control Group D had axis repeatability 2.16±1.39° (0.05 to 5.86°). The SAI index measurement repeatability was 0.33±0.40 (0.01 to 2.31) in the post-LASIK Group A, 0.39±0.75 (0.00 to 7.15) in the keratoconic Group B, and 0.43±0.56 (0.05 to 3.50) in the keratoconus post-CXL Group C. The control group had SAI measurement repeatability of 0.26±0.30 (0.00 to 2.39). The SRI index repeatability was 0.22±0.17 (0.01 to 0.96) for post-LASIK Group A, 0.20±0.18 (0.00 to 1.07) in keratoconic Group B, and 0.13±0.09 (0.00 to 0.45) in the keratoconus post-CXL Group C. The control Group D had SRI measurement repeatability of 0.23±0.16 (0.00 to 0.75).
Conclusion
This novel corneal topography device appears to offer very high specificity in estimating corneal keratometry and specific corneal irregularity indices, even in topographically challenging corneas such as LASIK treated, keratoconic, and cross-linked.
Introduction
Corneal topographers provide qualitative characteristics and quantitative metrics of the anterior corneal surface,Citation1 transforming raw data into color-coded dioptric power-scale refractive and curvature maps. In addition, elevation maps can be derived by slope measurement data. Specific topography indices associated with corneal pathology have also been introduced by topography – analysis algorithms.Citation2
While Placido-disc systems have been the mainstream of videokeratoscopy,Citation3–Citation6 certain restrictions exist with this technology,Citation7 such as the limited ability to identify contour topographic changes.Citation8 To override these limitations, topography systems with color-coded specular reflection forward ray-tracing have been proposedCitation9 as alternatives to Placido-ring imaging,Citation10 enabling, among other things, the proper imaging of radial, in addition to only contour topographic, changes.
The “Cassini” (i-Optics, The Hague, the Netherlands) system is a novel topographer utilizing a multicolor (red, yellow, and green) spot pattern consisting of hundreds of light-emitting diode (LED) spots (up to 700) projected on the cornea. Image-processing software locates feature points in the reflected images and accounts for smearing and deformation in irregular corneas. The system has been recently introducedCitation11 and has received US Food and Drug Administration approval for clinical topography.
Due to their novelty, the clinical validation of such systems and their clinical implications have yet to be investigated and compared with those of established topographers. We have recently reported cases of forme fruste keratoconusCitation12 and central corneal scarCitation13 in which the Cassini device appeared to be more sensitive than established cornea imaging devices.
The aim of the work reported here was to evaluate the repeatability measurement of this newly introduced device in a large number of LASIK-treated eyes, keratoconic eyes, and eyes treated with anterior-surface normalization and cross-linking. Specifically, we investigated the repeatability of measurement of the following parameters: flat and steep meridian keratometry, axis of astigmatism, form factor, surface regularity index (SRI), and surface asymmetry index (SAI).
Materials and methods
This observational, prospective study received approval by the ethics committee of our institution, adherent to the tenets of the Declaration of Helsinki. Informed written consent was obtained from each subject at the time of the first clinical visit.
Inclusion criteria
The study group consisted of 373 different patients. One eye was selected randomly from each patient to be included in the study. The following study groups were formed: Group A (nA=51 different eyes) consisted of eyes that had received myopic laser-assisted in situ keratomileusis (LASIK) treatment. Group B (nB=95) consisted of untreated keratoconic eyes; the keratoconus condition had been previously determined as being grade 1 or more on the Amsler–Kruemeich keratoconus severity scale, as determined by Scheimpflug imaging. Group C (nC=47) consisted of eyes treated with partial anterior-surface topography-guided excimer ablation and same-session high-fluence collagen cross-linking, in a procedure known as the “Athens Protocol”.Citation14 In addition, a control Group D (nD=180) was formed consisting of subjects having no current or past ocular pathology other than refractive error, no other previous surgery, no epithelial defects, and no present irritation or dry-eye disorder, all confirmed by a complete ophthalmologic evaluation.
Instrumentation
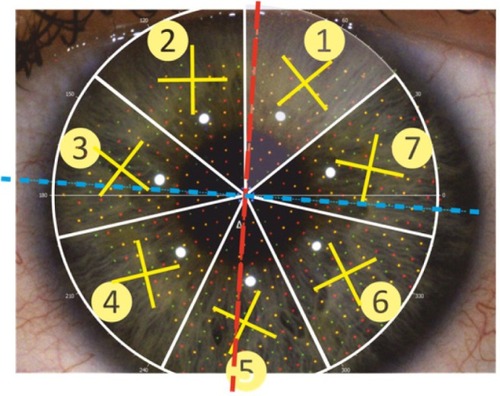
The system employed in this study was the Cassini, a multicolored-spot reflection corneal topographer. The system projects approximately 700 LED point-sources onto the cornea and evaluates their reflection pattern, extending to up to 8.5 mm of the corneal diameter area as raw data. These spots are grouped in seven “septima” segments with a specific Cartesian array arrangement within each segment, as illustrated in .
Figure 1 Raw data image as obtained by the Cassini multicolored-spot reflection topographer.
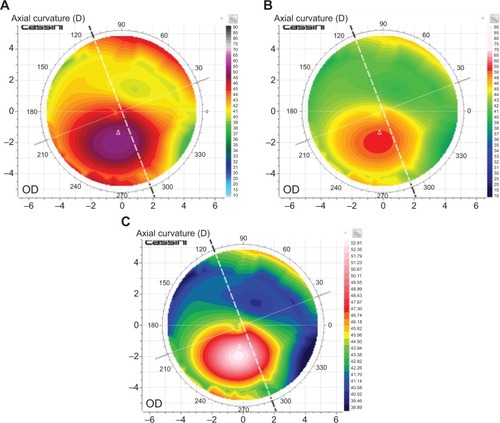
The system consequently provides anterior-surface topography results, including axial and tangential curvature, refractive power, and elevation maps. The user may select from among various color-coded scales (), including the American Style, the ISO (International Organization for Standardization [French]) 19980, the Oculus, and the topographic modeling system scale.Citation15 The system calculates flat and steep keratometry (diopters [D]), axis orientation (°), and related astigmatism (D), and identifies the location of the corneal apex. Four topographic indicesCitation16 relating to surface asphericity, and three keratoconus indices – form factor, the SRI, and SAI (created by Dr Stephen Klyce)Citation17 – are also provided. Acquisition quality was evaluated by four image quality indices. The system employed in the study ran on software version 1.2.0 (updated September 2013).
Figure 2 Axial curvature maps.
Abbreviations: D, diopters; OD, optical density.
Data collection and analysis
Three successive acquisitions, centered on the pupil, were performed in each case (eye), assuring that each acquisition had at least 75% coverage, as reported by the quality factor. In each acquisition, the data collected were: flat and steep keratometry (in diopters, D), axis of steep keratometry (in degrees, °), form factor, and the indices SRI and SAI (both unit-less). The repeatability of measurement was assessed by the standard deviation of the three values of each parameter investigated as obtained by the three consecutive acquisitions performed in each eye. Statistical analysis was performed using Minitab software (v 16.2.3; MiniTab Ltd, Coventry, UK).
Results
Post-myopic LASIK Group A, of the 51 eyes included, there were 24 male (47%) and 27 female (53%). Mean subject age at the time of examination was 35.05±8.11 (24 to 49) years of age. Mean value of flat keratometry was 38.20±4.50 (23.93 to 45.57) D, of steep keratometry was 39.50±4.23 (29.28 to 47.04) D, of steep axis was 87.78±42.09° (4.42 to 179.75°), of form factor was 2.62±2.18 (0.07 to 10.61), of SRI was 1.60±0.78 (−0.11 to 3.52), and of SAI was 1.01±0.98 (0.12 to 6.31). Descriptive statistics of these values as well as of those from Groups B, C, and control Group D are reported in .
Table 1 Descriptive statistics of flat and steep keratometry (diopters [D]), axis (°), form factor, surface regularity index (SRI), and surface asymmetry index (SAI) measurements for the control group and the three study groups
The keratoconic Group B consisted of 95 eyes (55.7% male; eye laterality 47.3% right). Mean patient age was 30.72±7.98 (17 to 45) years of age. Mean value of flat keratometry was 42.45±3.90 (31.00 to 53.98) D, of steep keratometry was 45.71±3.65 (39.49 to 58.07) D, of steep axis was 93.85±46.78° (1.15 to 179.79°), of form factor was 2.96±1.96 (−0.05 to 10.47), of SRI was 1.88±0.71 (−0.26 to 3.60), and of SAI was 2.96±2.89 (0.10 to 20.47).
The cross-linked Group C consisted of 47 eyes, belonging to 29 male and 11 female patients; 25 eyes were right and 22 left. Mean patient age was 27.45±7.46 (17 to 49) years of age. Mean value of flat keratometry was 43.29±4.22 (34.79 to 53.75) D, of steep keratometry was 46.39±4.72 (35.43 to 57.52) D, of steep axis was 92.51±39.43° (13.00 to 179.23°), of form factor was 2.42±1.91 (−0.84 to 7.27), of SRI was 2.09±0.63 (0.13 to3.25), and of SAI was 3.02±2.33 (0.18 to 10.31).
The control Group D consisted of 180 eyes, belonging to 55 male and 52 female patients; 92 eyes were right and 88 left. Mean patient age was 40.04±16.86 (16 to 61) years of age. Mean value of flat keratometry was 42.83±2.02 (32.36 to 50.94) D, of steep keratometry was 44.35±2.17 (33.48 to 54.01) D, of steep axis was 91.85±27.15° (0.15 to 179.86°), of form factor was 0.96±0.63 (−0.20 to 6.30), of SRI was 0.91±0.62 (−0.46 to 3.01), and of SAI was 0.61±0.65 (−0.11 to 5.38).
Specifically, flat keratometry repeatability was 0.74±0.89 (0.03 to 5.26) D in the LASIK Group A, 0.88±1.45 (0.00 to 7.84) D in the keratoconic Group B, and 0.71±0.94 (0.02 to 6.23) D in the cross-linked Group C. The control Group D had flat keratometry repeatability of 0.36±0.46 (0.00 to 2.71) D. Steep keratometry repeatability was 0.64±0.82 (0.01 to 4.81) D in the LASIK Group A, 0.89±1.22 (0.02 to 7.85) D in the keratoconic Group B, and 0.93±1.12 (0.04 to 5.93) D in Group C. The control Group D had steep keratometry repeatability of 0.41±0.50 (0.00 to 3.51) D. Axis repeatability was 3.45±1.62° (0.38 to 7.78°) for the LASIK Group A, 4.12±3.17° (0.02 to 12.13°) for the keratoconic Group B, and 3.20±1.99° (0.17 to 8.61°) for the Athens Protocol Group C. The control Group D had axis repeatability of 2.16±1.39° (0.05 to 5.86°). presents box plots illustrating steep and flat keratometry and axis measurement repeatability. The repeatability results are also reported in .
Figure 3 Box plots illustrating steep and flat keratometry and axis measurement repeatability.
Abbreviation: D, diopters.
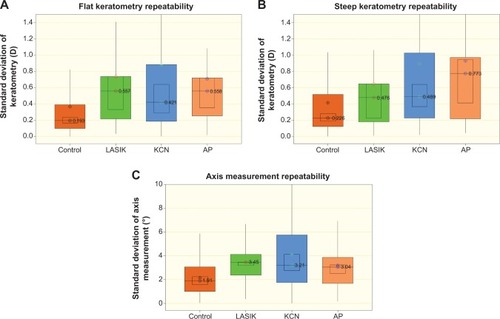
Table 2 Repeatability of flat and steep keratometry (diopters [D]), axis (°), form factor, surface regularity index (SRI), and surface asymmetry index (SAI) measurements for the control group and the three study groups
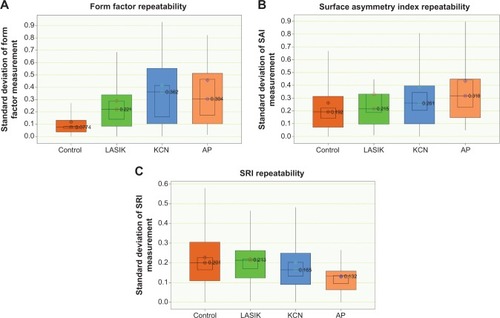
The form factor measurement repeatability was 0.29±0.32 (0.00 to 1.69) in the LASIK Group A, 0.42±0.42 (0.00 to 2.03) in the keratoconic Group B, and 0.46±0.50 (0.02 to 1.85) in the cross-linked Group C. The control Group D had form factor repeatability of 0.12±0.15 (0.00 to 1.06) (). The SAI index measurement repeatability was 0.33±0.40 (0.01 to 2.31) in the LASIK Group A, 0.39±0.75 (0.00 to 7.15) in the keratoconic Group B, and 0.43±0.56 (0.05 to 3.50) in the cross-linked Group C. The control group had SAI measurement repeatability of 0.26±0.30 (0.00 to 2.39). The SRI index repeatability was 0.22±0.17 (0.01 to 0.96) for LASIK Group A, 0.20±0.18 (0.00 to 1.07) in keratoconic Group B, and 0.13±0.09 (0.00 to 0.45) in the cross-linked Group C. The control Group D had SRI measurement repeatability of 0.23±0.16 (0.00 to 0.75).
Figure 4 Box plots illustrating form factor, surface asymmetry index (SAI), and surface regularity index (SRI) measurement repeatability.
Discussion
There are many advantages justifying the widespread use of Placido-ring based topography systems, such as the noncontact measurement of the single-shot capture, which reduces motion artifacts. However, there is a number of limitations associated with Placido topography, including the skew-ray error,Citation18,Citation19 lower data reliability at the corneal center, and susceptibility to error in areas of abrupt corneal elevation changes.Citation20,Citation21 Specifically, when reconstructing the anterior corneal surface, the numerical algorithms employed in commercially available Placido-disc topographers neglect skew-ray reflections,Citation22 leading to inaccuracy in reconstructing non-rotationally symmetric corneas.Citation23 The new modality introduced by the Cassini topographer aims to avoid these two critical limitations.
The work presented here is an investigation of this novel device which is currently under evaluation by our team. We chose to focus on a very specific metric, that of the repeatability of measurement in various groups of several clinical settings. We have already reportedCitation12,Citation13 early clinical case reports of this device in specific challenging cases in which other established devices have failed to properly image the cornea.
In the present study, we observed the distributions and repeatability of keratometric, axis, and three qualitative indices associated with anterior corneal surface. The distributions measured in the control group were of the same range reported in the literature,Citation24 the keratometries encountered in the keratoconic- and Athens Protocol-treated eyes were also within the same range reported in previous work by our team employing Placido topographyCitation21 and Scheimpflug imaging technologies.Citation25 The anterior-surface indices were also within the range of SAI and SRI measurements reported in keratoconic eyes.Citation26 The keratometric repeatability was under 0.5 D in the control group, 0.7–0.9 D in the keratoconic and cross-linked eyes, and 0.65–0.75 D in the LASIK-treated eyes. Axis measurement repeatability was under 2.5° in the control group, in the range of under 4° in the keratoconic and cross-linked eyes, and approximately 3.5° in the LASIK-treated eyes. Obviously, the sensitivity to centration in the keratoconic and LASIK-treated eyes could be a reason for the larger fluctuation among values, in comparison to the control group. In the LASIK-treated group, the surface analysis was also complex compared with the spherical corneas encountered in the control group, due to the central flattening as a result of the excimer ablation performed.
Comparison with the values reported in the literature suggests that the findings herein are quite comparable to established corneal-screening devices such as standard manual keratometry,Citation27,Citation28 Placido topography,Citation29 the Orbscan II (Bausch & Lomb, Rochester, NY, USA), the Pentacam (Oculus, Weltzlar, Germany), the Galilei (Ziemer Ophthalmic Systems AG, Port, Switzerland),Citation30 and the Sirius (CSO Costruzione Strumenti Oftalmici, Scandicci, Italy).Citation31 For example, the standard deviation of the test–retest reliability in the size of corneal astigmatism was 0.293 D as reported in automated keratometry measurements.Citation32
Conclusion
The Cassini demonstrated extreme measurement precision in terms of sensitivity and specificity. It appears to precisely measure irregular corneas, both in keratometry and axis. Perhaps more importantly it appears to precisely measure normal and even post-myopic LASIK corneas, expected to have minimal astigmatism which poses a challenging diagnostic measurement.
Disclosure
AJK has held consultant/advisory positions with Alcon/Wave-Light, Avedro, i-Optics, Allergan, Inc., and KeraMed Inc. The authors declare no other conflicts of interest in this work.
References
- CourvilleCBSmolekMKKlyceSDContribution of the ocular surface to visual opticsExp Eye Res200478341742515106921
- HolladayJTKeratoconus detection using corneal topographyJ Refract Surg20092510 SupplS958S96219848378
- Alonso-CaneiroDIskanderDRCollinsMJEstimating corneal surface topography in videokeratoscopy in the presence of strong signal interferenceIEEE Trans Biomed Eng200855102381238718838363
- ReadSACollinsMJIskanderDRDavisBACorneal topography with Scheimpflug imaging and videokeratography: comparative study of normal eyesJ Cataract Refract Surg20093561072108119465294
- ShirayamaMWangLWeikertMPKochDDComparison of corneal powers obtained from 4 different devicesAm J Ophthalmol2009148528535.e119541287
- Mejía-BarbosaYMalacara-HernándezDA review of methods for measuring corneal topographyOptom Vis Sci200178424025311349932
- SeitzBBehrensALangenbucherACorneal topographyCurr Opin Ophthalmol19978482410170448
- RandRHHowlandHCApplegateRAMathematical model of a Placido disk keratometer and its implications for recovery of corneal topographyOptom Vis Sci199774119269309403889
- VosFMvan der HeijdeRGSpoelderHJvan StokkumIHGroenFCA new instrument to measure the shape of the cornea based on pseudorandom color codingIEEE Trans Instrum Meas1997464794797
- SnellenburgJJBraafBHermansEAvan der HeijdeRGSicamVAForward ray tracing for image projection prediction and surface reconstruction in the evaluation of corneal topography systemsOpt Express20101818193241933820940828
- WeikertMPKochDDWangDEvaluation of corneal topography based on color LED technologyPaper presented at the American Society of Cataract and Refractive Surgery Symposium and CongressApril 19–23, 2013San Francisco, California, USA
- KanellopoulosAJAsimellisGForme Fruste Keratoconus Imaging and Validation via Novel Multi-Spot Reflection TopographyCase Rep Ophthalmol20134319920924348403
- KanellopoulosAJAsimellisGClinical Correlation between Placido, Scheimpflug and LED Color Reflection Topographies in Imaging of a Scarred CorneaCase Rep Ophthalmol2014531131725408671
- KanellopoulosAJAsimellisGKeratoconus management: long-term stability of topography-guided normalization combined with high-fluence CXL stabilization (the Athens Protocol)J Refract Surg2014302889324763473
- SmolekMKKlyceSDHovisJKThe Universal Standard Scale: proposed improvements to the American National Standards Institute (ANSI) scale for corneal topographyOphthalmology2002109236136911825824
- MaedaNEvaluation of optical quality of corneas using corneal topographersCornea2002217 SupplS75S7812484703
- SmolekMKKlyceSDCurrent keratoconus detection methods compared with a neural network approachInvest Ophthalmol Vis Sci19973811229022999344352
- KleinSAAxial curvature and the skew ray error in corneal topographyOptom Vis Sci199774119319449403890
- IskanderDRDavisBACollinsMJThe skew ray ambiguity in the analysis of videokeratoscopic dataOptom Vis Sci200784543544217502828
- KleinSACorneal topography reconstruction algorithm that avoids the skew ray ambiguity and the skew ray errorOptom Vis Sci199774119459629403891
- KanellopoulosAJAsimellisGComparison of Placido disc and Scheimpflug image-derived topography-guided excimer laser surface normalization combined with higher fluence CXL: the Athens Protocol, in progressive keratoconusClin Ophthalmol201371385139623901251
- van SaarloosPPConstableIJImproved method for calculation of corneal topography for any photokeratoscope geometryOptom Vis Sci199168129609651787956
- GreivenkampJEMellingerMDSnyderRWSchwiegerlingJTLowmanAEMillerJMComparison of three videokeratoscopes in measurement of toric test surfacesJ Refract Surg19961222292398653525
- SwartzTMartenLWangMMeasuring the cornea: the latest developments in corneal topographyCurr Opin Ophthalmol200718432533317568210
- KanellopoulosAJAsimellisGRevisiting keratoconus diagnosis and progression classification based on evaluation of corneal asymmetry indices, derived from Scheimpflug imaging in keratoconic and suspect casesClin Ophthalmol201371539154823935360
- HassanZSzalaiEMódisLJrBertaANémethGAssessment of corneal topography indices after collagen crosslinking for keratoconusEur J Ophthalmol201323563564023483510
- KarabatsasCHCookSDPapaefthymiouJTurnerPSparrowJMClinical evaluation of keratometry and computerised videokeratography: intraobserver and interobserver variability on normal and astigmatic corneasBr J Ophthalmol19988266376429797664
- VisserNBerendschotTTVerbakelFde BrabanderJNuijtsRMComparability and repeatability of corneal astigmatism measurements using different measurement technologiesJ Cataract Refract Surg201238101764177022999600
- KarabatsasCHPapaefthymiouIAslanidesIMChatzoulisDZComparison of keratometric and topographic cylinder and axis measurements on normal corneas with low astigmatismEur J Ophthalmol200515181615751233
- CrawfordAZPatelDVMcGheeCNComparison and repeatability of keratometric and corneal power measurements obtained by Orbscan II, Pentacam, and Galilei corneal tomography systemsAm J Ophthalmol20131561536023540708
- De la Parra-ColínPGarza-LeónMBarrientos-GutierrezTRepeatability and comparability of anterior segment biometry obtained by the Sirius and the Pentacam analyzersInt Ophthalmol2014341273323616225
- NinomiyYKanazawaYKojimaYMaedaNSimulation of toric intraocular lens results: the effect of repeatability and increments of automated keratometryNihon Ganka Gakkai Zasshi20131178621628 Japanese24063159