
Abstract
Endophthalmitis is an uncommon diagnosis but can have devastating visual outcomes. Endophthalmitis may be endogenous or exogenous. Exogenous endophthalmitis is caused by introduction of pathogens through mechanisms such as ocular surgery, open-globe trauma, and intravitreal injections. Endogenous endophthalmitis occurs as a result of hematogenous spread of bacteria or fungi into the eye. These categories of endophthalmitis have different risk factors and causative pathogens, and thus require different diagnostic, prevention, and treatment strategies. Novel diagnostic techniques such as real-time polymerase chain reaction (RT-PCR) have been reported to provide improved diagnostic results over traditional culture techniques and may have a more expanded role in the future. While the role of povidone-iodine in prophylaxis of postoperative endophthalmitis is established, there remains controversy with regard to the effectiveness of other measures, including prophylactic antibiotics. The Endophthalmitis Vitrectomy Study (EVS) has provided us with valuable treatment guidelines. However, these guidelines cannot be directly applied to all categories of endophthalmitis, highlighting the need for continued research into attaining improved treatment outcomes.
Introduction
Endophthalmitis is a rare but potentially sight-threatening disease characterized by marked inflammation of intraocular tissues and fluids.Citation1 This ocular pathology can be divided into broad categories of exogenous and endogenous endophthalmitis. Exogenous endophthalmitis is caused by inoculation of the eye by microorganisms from the external environment and most commonly occurs as a complication of ocular surgery, trauma, or intravitreal injections.Citation1 Endogenous endophthalmitis is caused by hematogenous spread of infectious organisms from distant sites of the body. Both categories of endophthalmitis lead to subsequent intraocular inflammation and potentially severe visual loss.Citation2
Classification of endophthalmitis
Acute-onset postoperative endophthalmitis
Background and incidence
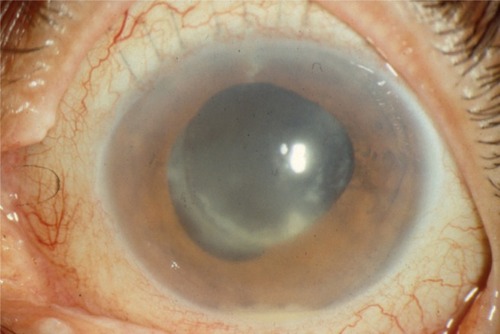
Acute-onset postoperative endophthalmitis () is generally defined as occurring within 6 weeks of an ocular procedure. Cataract surgeries are responsible for the majority of these cases.Citation3,Citation4 The reported incidence of acute-onset postoperative endophthalmitis following cataract surgery ranges from 0.03% to 0.2%.Citation5–Citation12 Less commonly, acute-onset postoperative endophthalmitis has been reported following other ocular procedures including penetrating keratoplasty,Citation5,Citation13,Citation14 scleral buckling,Citation15 glaucoma drainage device implantation,Citation16 and others.
Figure 1 Acute-onset postoperative endophthalmitis (note the sutured corneal wound and hypopyon).

Due to increasing utilization of pars plana vitrectomy (PPV),Citation17 there is increasing interest in endophthalmitis following this type of surgery. Reported incidence rates range from 0% to 2.4% for 20 G surgeries (with most rates falling between 0.02% and 0.05%) and 0%–1.3% following 23 G and 25 G PPV.Citation18–Citation23
Presentation
In the Endophthalmitis Vitrectomy Study (EVS),Citation24 94% of patients with acute-onset postoperative endophthalmitis following cataract surgery or secondary intraocular lens (IOL) implantation presented with decreased visual acuity, 82% with conjuctival injection, 74% with eye pain, and approximately 35% with eyelid edema. Acute-onset postoperative endophthalmitis following other types of surgery present with same general signs, to varying degrees.Citation22,Citation25
Risk factors
Among patients undergoing cataract surgery, preoperative risk factors associated with acute-onset postoperative endophthalmitis include blepharitis, diabetes mellitus, and older age.Citation12,Citation26–Citation30 Perioperative risk factors include preoperative steroids, intraoperative complications, posterior capsular rupture, vitreous loss, and surgeons with less experience.Citation11,Citation26,Citation27,Citation29–Citation36 Some series have reported clear corneal incisions and lack of intracameral antimicrobials as risk factors but these are controversial. Postoperative risk factors include inpatient status and wound leak on postoperative day 1.Citation37,Citation38
Causative organisms
The EVS recruited only patients with suspected bacterial endophthalmitis. The investigators reported that among culture-positive cases, 94.2% of isolates were Gram-positive bacteria.Citation24 Among these, coagulase-negative staphylococci were the most commonly identified pathogens (70%) followed by Staphylococcus aureus (9.9%) and Streptococcus species (9%).Citation24 Coagulase-negative Staphylococcus species have also been the predominant isolates reported in endophthalmitis following PPV.Citation21,Citation22
There were no reported cases of acute-onset postoperative fungal endophthalmitis in the EVS and other US-based studies.Citation5,Citation39 However, two publications from India reported a high incidence of postoperative fungal endophthalmitis ranging from 17% to 22%.Citation40,Citation41
Delayed-onset postoperative endophthalmitis
Background and incidence
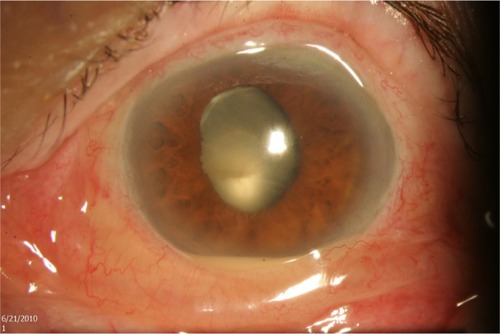
Delayed-onset (chronic) postoperative endophthalmitis () is generally defined as occurring more than 6 weeks after surgery.Citation42 A recent study reported a mean of 343 days from the date of surgery to the date of diagnosis.Citation43 Delayed-onset postoperative endophthalmitis is less common than the acute-onset category with a reported ratio of approximately 1:3.5.Citation43 Similarly, delayed-onset post-cataract endophthalmitis was reported to account for only 7.2% of all postoperative endophthalmitis cases.Citation3 The incidence of delayed-onset postoperative endophthalmitis has been reported at 0.02%.Citation44
Figure 2 Delayed-onset (chronic) postoperative endophthalmitis (note the small hypopyon and peripheral intracapsular infiltrates).
Presentation
Delayed-onset postoperative endophthalmitis typically progresses slowly and may involve only mild inflammation.Citation43 When compared with acute-onset type, delayed-onset postoperative endophthalmitis is less commonly associated with hypopyon. Pain may or may not be present. Characteristic white plaques within the capsular bag are frequently seen.Citation43
Causative organisms
Propionibacterium acnes is the most common microorganism isolated in culture-positive cases of chronic postoperative endophthalmitis, accounting for 41%–63% of cases.Citation43–Citation45 Fungal infections are also important causative pathogens and are responsible for 16%–27% of cases.Citation43–Citation45
Bleb-associated endophthalmitis
Background and incidence
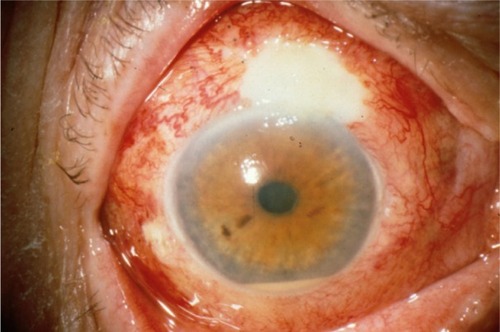
Bleb-associated endophthalmitis () may occur following trabeculectomy in either an acute (<4 weeks) or more commonly delayed (>4 weeks) onset.Citation46 The reported mean time from surgery to diagnosis varies but has generally been in the range of approximately 1.5 yearsCitation47 to 7 yearsCitation48,Citation49 and even up to 44 years.Citation50,Citation51 The reported incidence rates of bleb-associated endophthalmitis range from 0.17% to 13.2%.Citation52–Citation62
Figure 3 Bleb-related endophthalmitis (note the purulent filtering bleb and hypopyon).
Presentation
Bleb-associated endophthalmitis must be differentiated from blebitis, which presents with a purulent filtering bleb, conjuctival injection and discharge along with photophobia, but no hypopyon or vitreous involvement. Bleb-associated endophthalmitis may be associated with pain, decreased visual acuity, relative afferent pupillary defect, and hypopyon.Citation50,Citation63 Prodromal symptoms such as headache, browache, and conjunctivitis have been reported in 35% of cases of bleb-associated endophthalmitis.Citation64
Risk factors
Reported risk factors include a history of previous blebitis, late-onset bleb leak, younger age, use of antimetabolites, inferior trabeculectomy, thin avascular bleb, axial myopia, blepharitis, and chronic antibiotic use.Citation62,Citation64–Citation67 While intraoperative use of antimetabolites (specifically mitomycin C) has significantly increased the success rate of trabeculectomies,Citation68 their use has been associated with a 3-fold increased risk of developing endophthalmitis.Citation66,Citation69 This increased risk may have been reduced in recent years due to increased surgeons’ confidence levels in using intraoperative mitomycin C and a shift from limbus-based to fornix-based conjuctival flaps.Citation70
Causative organisms
Similar to acute-onset postoperative endophthalmitis, coagulase-negative staphylococci (specifically Staphylococcus epidermidis) and S. aureus are the most common isolates in early bleb-associated endophthalmitis.Citation50,Citation60 In contrast, Streptococcus species and gram-negative organisms (specifically Moraxella catarrhalis) are the predominant causes of delayed-onset bleb-associated endophthalmitis.Citation50,Citation71
Postintravitreal injection endophthalmitis
Background and incidence
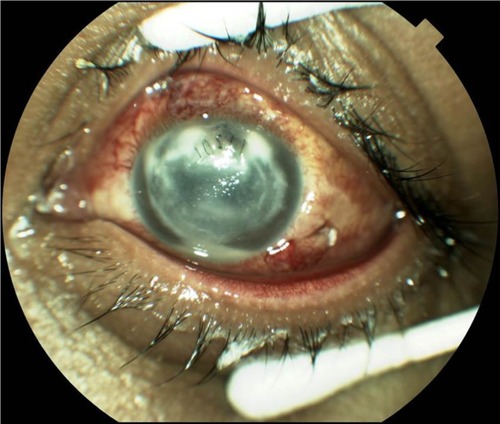
The incidence of endophthalmitis following anti-vascular endothelial growth factor (anti-VEGF) injections () has been reported in the range of 0.02%–0.32% per injection.Citation72 Because most patients are treated with a series of injections, the incidence rate per patient is higher. A large meta-analysis including 350,535 injections among 45 published studies between 2005 and 2012 reported an overall incidence rate of 0.056% or 1 per 1,779 intravitreal injections.Citation72 The incidence of endophthalmitis following intravitreal injection of triamcinolone acetonide has been reported to be in the range of 0.001%–0.87% per injection, but is generally thought to be higher than that following anti-VEGF injections.Citation73–Citation75
Figure 4 Endophthalmitis following intravitreal injection (note the chemosis and hypopyon).
Noninfectious endophthalmitis may occur following intravitreal injections. The etiology is poorly understood but may represent an inflammatory reaction to a component in the medication vehicle or migration of triamcinolone acteonide crystals.Citation76 Reported incidence rates of noninfectious endophthalmitis are 0.37% after aflibercept injections,Citation77 0.27%–1.49% after bevacizumab injections,Citation78–Citation80 and 1.6%–2.7% after triamcinolone acetonide injections.Citation81,Citation82
Presentation
Post-intravitreal injection endophthalmitis typically occurs acutely within the first few days.Citation83,Citation84 Just like other types of endophthalmitis, the most common presenting signs and symptoms of endophthalmitis following intravitreal injections are decreased vision, eye pain, and redness, with presence of anterior chamber cells, hypopyon, and vitritis.Citation83–Citation86
Generally, eye pain, anterior chamber fibrin, and profound visual loss are less common in noninfectious postinjection endophthalmitis than in infectious cases and this could potentially help in distinguishing between the two.Citation76,Citation86 However, in a retrospective review of cases with presumed endophthalmitis, substantial overlap was observed in the presenting signs and symptoms of noninfectious versus infectious types.Citation83
Risk factors
Reported risk factors include older age, diabetes mellitus, blepharitis, subconjuctival anesthesia, patient moving/squeezing during the injection, and the use of compounded medications.Citation87,Citation88 Batch-related noninfectious endophthalmitis has also been reported in 27% and 39% of patients injected from two specific bevacizumab lots.Citation89
Causative organisms
Two meta-analyses of isolates from endophthalmitis following intravitreal injection of anti-VEGF agents have reported that overall, coagulase-negative Staphylococcus (aggregated mean of 38%–65%) and Streptococcus species (29%–31%) are the most cultured organisms.Citation72,Citation90 Other less common pathogens found are Bacillus cereus, Enterococcus faecalis, S. epidermidis, and S. aureus. While coagulase-negative Staphylococcus species are the most commonly isolated pathogens in both postoperative and postinjection endophthalmitis cases, Streptococcus species are 3 times more prevalent in postinjection endophthalmitis than in postoperative cases.Citation90 Of note, Streptococcus species make up 41% of normal oral flora.Citation91 Therefore, the mechanism of infection in postinjection endophthalmitis may involve contamination of the ocular surface by oropharyngeal bacteria.Citation90
In multiple series, a large proportion of clinically suspected endophthalmitis cases were culture-negative (aggregated means of 46.5%–48%).Citation72,Citation90
Posttraumatic endophthalmitis
Background and epidemiology
Posttraumatic endophthalmitis is an uncommon but important complication of open-globe injury ().Citation92–Citation94 In recent years, the incidence of endophthalmitis following open-globe trauma has been reported to be between 0% and 12%Citation95–Citation103 with rates as high as 35% when an intraocular foreign body (IOFB) is present.Citation94
Figure 5 Posttraumatic endophthalmitis (note the sutured corneal wound and hypopyon).
Presentation
The presentation and onset of posttraumatic endophthalmitis vary depending on the mechanism of injury and the virulence of organisms involved. Endophthalmitis can present within hours or can be diagnosed years after the initial injury.Citation104 Signs and symptoms include hypopyon, decreased vision, pain out of proportion to the degree of trauma, retinitis, vitritis, retinal necrosis, and periphlebitis.Citation96,Citation104 Other findings which could potentially aid the clinician in suspecting endophthalmitis in a case of globe injury include corneal and/or lid edema and loss of red reflex.Citation105
Risk factors
Many predisposing factors have been associated with the development of endophthalmitis following open-globe injuries. These include IOFB, traumatic lens rupture, corneal wound, retinal break/detachment, traumatic cataract/posterior lens rupture, dirty wound, long hospital stay, and rural location.Citation94,Citation95,Citation98,Citation100,Citation101 Delayed wound closure and primary repair (beyond 12–24 hours) have also been reported as important risk factors.Citation95,Citation96,Citation106,Citation107 Tissue prolapse (iris, vitreous) and presence of hyphema may reduce the risk of endophthalmitis since they may act as a barrier against entrance of microbes.Citation96,Citation100
Causative organisms
Approximately 80%–90% of culture-positive cases are caused by bacteria.Citation108,Citation109 Gram-positive cocci are the more common isolates among bacteria, followed by Gram-positive bacilli and other Gram-negative organisms.Citation108,Citation109 Among Gram-positive cocci, coagulase-negative Staphylococcal organisms (ie, S. epidermidis and Staphyloccoccus saprophyticus) along with Streptococcus species are the predominant groups. Gram-positive Bacillus species have been commonly reported in culture isolates of posttraumatic endophthalmitis.Citation95,Citation101,Citation108–Citation110 Enterobacter and Pseudonomas species are the most common Gram-negative pathogens and Aspergillus species are the most prevalent fungal cause of posttraumatic endophthalmitis.Citation108,Citation109
Endogenous endophthalmitis
Background and incidence
In contrast to exogenous endophthalmitis, endogenous endophthalmitis is caused by inoculation of the eye by infectious pathogens spread systemically through the bloodstream and across the blood-ocular barrier.Citation111 Endogenous endophthalmitis is uncommon and generally accounts for 2%–16% of all reported endophthalmitis cases Citation92,Citation93,Citation112–Citation114 but the prevalence has been reported to be as high as 41% in one series.Citation115
Presentation
Symptoms of endogenous endophthalmitis include decreased vision, eye pain, eye redness, photophobia, floaters, and eyelid swelling.Citation116–Citation120 Reported ocular signs include hypopyon, subconjuctival hemorrhage, conjuctival injection, iritis/retinitis, corneal edema, anterior chamber cells, and reduced or absent red reflex.Citation117,Citation119,Citation121
Since the pathogenesis of endogenous endophthalmitis typically involves hematogenous spread of infection to the eye, systemic findings and bilateral involvement are relatively common. Systemic finding would be signs and symptoms associated with sepsis or bacteremia such as fever, chills, and nausea and vomiting. Bilateral involvement of endogenous endophthalmitis has been reported in 19%–33% of cases.Citation116–Citation118,Citation120,Citation122
Risk factors
Several studies have reported a high prevalence of comorbidities, which can potentially predispose patients to development of endogenous endophthalmitis. These include immunocompromisation, diabetes mellitus, malignancies, intravenous drug use, organ abscess, immunosuppressive therapy, indwelling catheter, urinary tract infection, organ transplant, end-stage renal or liver disease, and endocarditis.Citation116,Citation118,Citation123–Citation125 While most studies evaluating patients with endogenous endophthalmitis have reported predisposing comorbidities, one series reported seven cases of culture proven endogenous endophthalmitis in healthy, immunocompetent individuals without any apparent extraocular loci of infection.Citation126
Causative organisms
The pathogens involved in endogenous endophthalmitis vary from study to study and appear to be potentially affected by geographic location and by the origin of the extraocular loci of infection. In contrast to other types of endophthalmitis where bacteria are the most prevalent pathogens, fungal causes were the most commonly isolated microorganisms in several series of endogenous endophthalmitis.Citation120,Citation122,Citation124,Citation127,Citation128 The leading cause of fungal endogenous endophthalmitis is Candida albicans, followed by Aspergillus species.Citation117,Citation118,Citation120,Citation127,Citation128
Bacterial endogenous endophthalmitis is typically due to Gram-positive species in western nations.Citation119,Citation120,Citation123,Citation128 Meanwhile, Gram-negative species (specifically Klebsiella species) are the main cause of bacterial endogenous endophthalmitis in East Asian countries.Citation111,Citation116,Citation121,Citation129
Diagnosis of endophthalmitis
Background
Endophthalmitis is initially suspected based upon clinical presentation, subsequently confirmed with laboratory testing of vitreous or aqueous. It is important to consider potential mimickers of endophthalmitis, including noninfectious inflammation (including toxic anterior segment syndrome), retained lens material, vitreous hemorrhage, and others. While suspected cases of endophthalmitis are typically treated with empiric broad-spectrum antibiotics, identifying the causative microorganisms becomes important in assessing antibiotic susceptibility and also in guiding treatment in cases that do not respond to initial therapy.
Vitreous specimens provide more accurate and reliable culture results than do aqueous cultures.Citation130–Citation133 For example, in one series, 48% of the cases that had a negative aqueous culture showed microbial growth in vitreous cultures.Citation134 Vitreous specimens have been traditionally obtained by vitreous tap using a needle and syringe. Other options include using vitrectomy cutters (when PPV is indicated) and office-based automated vitrectors.Citation135,Citation136 No difference has been shown in the positivity of cultures obtained from vitreous tap versus PPV.Citation133
Challenges in diagnosing specific classes of endophthalmitis
Approximately 70% of cases of postoperative endophthalmitis yield a positive culture,Citation5,Citation11,Citation134 although noninfectious endophthalmitis is relatively more common after intravitreal injection. In a meta-analysis, over 50% of endophthalmitis cases following anti-VEGF injections were culture-negative.Citation72
The diagnosis of posttraumatic endopthalmitis may be challenging as the signs and symptoms of endophthalmitis may overlap with those of the initial injury. As such, the presence of hypopyon, vitritis, and/or worsening pain should be considered possible signs of infection.Citation110,Citation137 Another important diagnostic step in posttraumatic endophthalmitis is the use of imaging techniques to identify the presence of occult IOFBs. In one series, IOFB was identified by clinical examination in 46% of cases, by B-scan echography in 52%, and by computed tomography (CT) in 95%.Citation138 Magnetic resonance imaging (MRI) may be considered after CT scan (so that metallic IOFBs are ruled out) to better identify nonmetallic IOFBs.Citation139
In endogenous endophthalmitis, the diagnosis can sometimes be aided by the presence of systemic signs and symptoms of infection and also by blood cultures. However, endogenous endophthalmitis may occur in patients with no overt signs of systemic infection.Citation126 In addition, negative blood cultures do not necessarily rule out a diagnosis of endogenous endophthalmitis. In one series, blood cultures were positive in only 33% of cases while vitreous samples were positive in 87% of the same patients.Citation128
Recent advances in identifying pathogens
Beyond the use of traditional culture media, there have been recent advances in the rapid and accurate detection of causative bacteria and fungi in endophthalmitis.Citation140 Real-time-polymerase chain reaction (RT-PCR) has been utilized to identify both bacteriaCitation141,Citation142 and fungi.Citation143,Citation144 As an example, in one series the rate of detection of bacteria in aqueous and vitreous samples increased from approximately 48% to over 95% using PCR.Citation142 Other novel microbial detection techniques which could potentially be used in rapid diagnosis of endophthalmitis causes are Matrix-Assisted Laser Desorption Ionization–Time of Flight (MALDI-TOF) Mass SpectrometryCitation145,Citation146 and the use of magneto-DNA nanoparticle system. The latter technique was reported to simultaneously identify 13 species of bacteria in under 2 hours.Citation147
Treatment of endophthalmitis
Acute-onset postoperative endophthalmitis
The EVS enrolled patients with endophthalmitis following cataract surgery or secondary IOL implantation within 6 weeks of surgery. The EVS reported that in patients with visual acuity of light perception (LP), when compared to tap and inject, prompt PPV was associated with a 3-fold increase in the proportion of patients achieving visual acuity of 20/40 or better, a 2-fold increase in the proportion of patients achieving visual acuity of 20/100 or better, and a decrease in the proportion of patients achieving visual acuity of worse than 5/200. In patients with better than LP initial visual acuity, however, tap and inject had comparable outcomes as PPV.Citation24 Based on these results, PPV is generally recommended in patients presenting with LP, and tap and inject is generally recommended for eyes presenting with visual acuity of better than LP.
The role of systemic antibiotics in the treatment of exogenous endophthalmitis remains controversial. The EVS reported that systemic amikacin and ceftazidime had no effect on the final visual outcome.Citation24 Fourth-generation fluoroquionolones, which were not tested by the EVS, achieve therapeutic levels from the systemic circulation in the noninflamed eye.Citation148 One study compared the use of oral ciprofloxacin versus moxifloxacin in patients with acute-onset postoperative endophthalmitis and reported that the group treated with oral moxifloxacin had a faster resolution of hypopyon and a decreased need for repeat intravitreal antibiotics.Citation149
Delayed-onset postoperative endophthalmitis
The treatment of delayed-onset (chronic) postoperative endophthalmitis is controversial because of the variable clinical presentations and different virulences of the causative organisms. Treatment with PPV combined with partial capsulectomy and injection of intraocular antibiotics led to complete resolution in only 50% of the cases in one series.Citation150 In another series, recurrent disease occurred in more than 70% of the cases of treated delayed-onset endophthalmitis but when PPV with total capsulectomy and IOL exchange or removal were performed, 90% had complete resolution of endophthalmitis.Citation43 As a result, total capsulectomy and removal of IOL may be considered for recurrent cases.Citation43,Citation151
Postintravitreal injection endophthalmitis
To date, there are no randomized clinical trials regarding the treatment of postinjection endophthalmitis. Since the most common isolates in both acute postoperative and postinjection endophthalmitis are Staphylococcus species, many clinicians use the EVS as a guideline for endophthalmitis following intravitreal injections. The role of initial PPV, however, remains unclear in postinjection endophthalmitis. In one series, 90% of the patients treated with tap and inject regained their preinjection visual acuity, while only 46% for patients treated with initial PPV did so.Citation152
Bleb-associated endophthalmitis
Streptococcus species and other virulent organisms are relatively more common in bleb-associated endophthalmitis, potentially leading to worse visual outcomes.Citation46,Citation71 As a result, more aggressive management, including prompt PPV, has been suggested for the treatment of bleb-associated endophthalmitis.Citation153,Citation154,Citation47,Citation63 Alternatively, another study reported that the eyes that underwent initial PPV had worse outcomes, so this question remains unsettled.Citation71
Endogenous endophthalmitis
Management of endogenous endophthalmitis includes a variable combination of systemic and intravitreal antibiotics (or antifungals) and PPV.Citation155 In a meta-analysis of endogenous endophthalmitis cases published from 2001 to 2012, 56% of the cases received systemic antibiotics, 76% received intravitreal antibiotics (vancomycin most commonly), 12% received intravitreal corticosteroids, and 32% of the eyes underwent PPV.Citation119 Systemic antibiotics and antifungals (depending on the causative organism) are generally recommended as endogenous endophthalmitis generally has extraocular loci of infection. In a meta-analysis of cases from 1986 to 2012, eyes which underwent PPV were more likely to have a final visual acuity of at least 20/200 and were less likely to progress to enucleation.Citation119
Posttraumatic endophthalmitis
While it is generally agreed that primary closure of an open-globe injury is important, there is no consensus with regards to managing established or suspected post-traumatic endophthalmitis. Similar to bleb-associated endophthalmitis, causative organisms in posttraumatic endophthalmitis are generally more virulent. The high prevalence of Streptococcus and Bacillus species has led to the suggestion of aggressive treatment, including initial PPV when feasible.Citation105,Citation110,Citation154 In addition to PPV, a combination of intravitreal, subconjuctival, topical, and systemic antibiotics are also recommended.Citation105,Citation110,Citation156
Changing trends in microbial profiles and antibiotic susceptibilities
Causative organisms evolve over time. For example, cases of fungal endophthalmitis following intravitreal injections were initially very rare but recently there have been reports of these cases in association with compounded triamcinolone acetonideCitation157 and compounded bevacizumab.Citation158
Two studies have reported that overall, S. epidermidis is the predominant pathogen in cases of endophthalmitis followed by Streptococcus viridans and other coagulase negative Staphylococcus species.Citation3,Citation159 Vancomycin for Gram-positive bacteria, ceftazidime for Gram-negative bacteria, and voriconazole for fungal endophthalmitis continue to be effective choices for initial treatment of endophthalmitis.Citation3,Citation159,Citation160
Visual outcomes of endophthalmitis treatment
Acute-onset postoperative endophthalmitis
In the EVS, only 53% of patients had a final visual acuity of 20/40 or better and 15% had a final visual acuity of 20/200 or worse.Citation24 In a more recent single-center series, 50% of eyes with acute-onset postoperative endophthalmitis had a final visual acuity of 20/40 or better and overall more than 36% had a final visual acuity of worse than 20/200.Citation5 A large retrospective study reported that eyes with final visual acuity of 20/40 or better were more likely to be culture-negative or culture-positive for coagulase-negative Staphylococci.Citation11 In another series, coagulase-negative Staphylococcus was associated with good final visual outcomes (20/40 or better) while Streptococcus species were more prevalent in eyes with worse than 20/200 outcomes.Citation161
Delayed-onset postoperative endophthalmitis
Delayed-onset endophthalmitis has been reported to have generally more favorable final visual outcomes when compared to acute-onset cases: 50% achieved final vision of better than 20/40 versus 27% respectively.Citation43 A review of 4 case series of delayed-onset endophthalmitis reported that eyes infected with P. acnes generally had a better final visual outcome while fungal cases were associated with significantly worse outcomes where more than one-fifth of these cases resulted in final visual acuity of worse than 20/200.Citation162
Bleb-associated endophthalmitis
Bleb-associated endophthalmits is also associated with unfavorable final visual outcomes due to high prevalence of virulent pathogens such as Streptococcus species and Gram-negative bacteria.Citation46,Citation71 In one series, 35% of cases had a final visual outcome of no light perception (NLP) and in another study this number was 23%.Citation47,Citation163 Initial visual acuity was reported to have a significant correlation with final visual acuity.Citation163 In one study, 83% of patients with initial visual acuity of better than LP had a final visual acuity of better than 20/40 while this degree of improvement was achieved by only 31% of patients who presented with LP on initial presentation.Citation46 Culture positivity with more virulent organisms (such as Streptococcus species) was also correlated with worse visual outcomes.Citation46,Citation163
Posttraumatic endophthalmitis
Posttraumatic endophthalmitis is associated with generally poor outcomes. One series reported a final visual outcome of NLP in 23% of cases with 45% of cases with hand motions (HM) or worse.Citation102 Recent studies have reported that a final visual acuity of 20/40 or better was achieved in only 15%–40% of cases with posttraumatic endophthalmitis.Citation95,Citation98,Citation164,Citation165 One series reported that a good final visual outcome (defined as 20/45 or better) was significantly associated with initial visual acuity of at least LP and an absence of a pupillary fibrin membrane.Citation165
Endogenous endophthalmitis
A meta-analysis reported that among endogenous endophthalmitis case series between 2001 and 2012 (a total of 89 eyes), 41% had a final visual acuity of at least 20/200 and 19% underwent enucleation or evisceration. These visual outcomes were improved compared to cases treated prior to 2001, in which final visual acuity of at least 20/200 was seen in only 31%.Citation119 Among the three broad categories of pathogens found in endogenous endophthalmitis (bacterial, yeast, and molds), cases caused by molds (Aspergillus species) are associated with the worst final visual outcomes and cases caused by yeasts (Candidia species) with the best. In one study, despite appropriate therapy, 25% of cases of endogenous endophthalmitis caused by Aspergillus species required enucleation while there were no enucleated cases with Candida isolates.Citation155 In other studies cases caused by Aspergillus were associated with poorer final visual outcomes.Citation120 In another series, while 80% of cases caused by Candidia had a final visual acuity of at least 20/200, only 18% of cases with Gram-positive bacteria achieved that visual acuity.Citation128
Postintravitreal injection endophthalmitis
Endophthalmitis cases following intravitreal injections have a high prevalence of more virulent Streptococcus species – approximately 3 times more prevalent than in postoperative cases – resulting in relatively poorer visual outcomes.Citation166 In one series, 80% of the postinjection endophthalmitis cases caused by Streptococcus species had final visual outcome of HM or worse.Citation84 Visual outcomes have varied among studies with the proportion of eyes returning to preinjection visual acuity in three recent studies ranging from 33% to 78%.Citation84,Citation167,Citation168 Another study concluded that compared to postoperative endophthalmitis, postinjection endophthalmitis was 6 times more likely to have final visual acuity of count fingers (CF) or worse and was much less likely to have improvement in visual acuity following treatment.Citation166
Prophylaxis of endophthalmitis
Postoperative endophthalmitis
Endophthalmitis probably cannot be completely prevented, but its incidence may be reduced. The use of preoperative povidone-iodine antisepsis significantly reduces the rate of bacterial endophthalmitis.Citation169 The European Society of Cataract and Refractive Surgeons (ESCRS) performed a large prospective randomized clinical trial, and reported that intracameral cefuroxime during phacoemulsification reduced the incidence of postoperative endophthalmitis by approximately 5-fold.Citation29 These results were replicated in later studies originating from different countries,Citation170–Citation174 although these results remain controversial and intracameral antibiotics are not universally employed even in Europe.
Multiple concerns have been raised about the use of prophylactic intracameral antibiotics. In the US, cefuroxime is not available in prepackaged form and must be reconstituted from powder in the operating room, creating risks of dilution errors and contamination. In addition, prophylactic use of antibiotics increases costs and contributes to increasing bacterial drug resistance.Citation175
Similarly, the prophylactic role of topical antibiotics in postoperative endophthalmitis is unclear. While a 2007 survey from American Society of Cataract and Refractive Surgery (ASCRS) members reported that 88% of respondents used preoperative, 91% used perioperative, and 98% used postoperative topical antibiotics,Citation176 no large-scale prospective studies have been performed to assess their efficacy. Preoperative topical antibiotics significantly reduce conjuctival floraCitation177 but it is unclear whether this actually decreases the rate of postoperative endophthalmitis. One series reported that substituting a combination of postoperative topical antibiotics and corticosteroids with topical corticosteroids alone did not change the incidence of endophthalmitis.Citation178
Postintravitreal injection endophthalmitis
An expert panel has recently reported updated guidelines for reducing the rate of endophthalmitis after intravitreal injections.Citation179 As with postoperative endophthalmitis, povidone-iodine is effective in reducing endophthalmitis rates following intravitreal injections.Citation180 Oral flora, including Streptococcus species, are more commonly isolated from postinjection cases than from postoperative cases.Citation90 The routine use of surgical masks during intravitreal injections is logicalCitation181 but has not been reported to reduce endophthalmitis rates.Citation182 The use of lid speculums has been traditionally recommended as part of a sterile protocol for administrating intravitreal injections.Citation74,Citation183 However, one series reported omitting lid speculums did not increase the rate of postinjection endophthalmitis.Citation167
Numerous studies have reported that prophylactic antibiotics do not reduce the incidence of postintravitreal injection endophthalmitis.Citation184,Citation185 Furthermore, a meta-analysis of seven studies and 72,823 intravitreal injections found no statistically significant benefit in using postinjection antibiotics.Citation186 Some series have reported that the use of topical antibiotics immediately after or for 5 days after injections were actually associated with higher rates of postinjection endophthalmitis, perhaps by altering conjunctival flora.Citation187 In addition, several studies have reported that the use of prophylactic antibiotics for intravitreal injections contributes to emergence of antibiotic-resistant bacteria.Citation188,Citation189 It has been suggested that prophylactic antibiotics are not a necessary part of intravitreal injection preparation and management.Citation129
Posttraumatic endophthalmitis
Antibiotic prophylaxis in posttraumatic endophthalmitis is controversial because there have been very few randomized clinical trials evaluating their effects. Systemic antibiotics have been widely utilized in open-globe injuriesCitation190 and non-use of systemic antibiotics appears to be a risk factor for post-traumatic endophthalmitis.Citation191,Citation192 In a prospective, randomized study assessing the prophylactic effects of intracameral and intravitreal antibiotics in posttraumatic endophthalmitis, there was a statistically significant reduction in rates of endophthalmitis in antibiotic-treated eyes with IOFB.Citation193
Bleb-associated endophthalmitis
There is little or no evidence that prophylactic topical antibiotics prevent bleb-associated endophthalmitis. On the contrary, it was reported that intermittent use or chronic use of antibiotics was associated with an increased risk of bleb-associated endophthalmitis.Citation66 Risk reduction of bleb-associated endophthalmitis should include addressing its risk factors such as early treatment of blebitisCitation194 and repair of leaking blebs.Citation195
Conclusion
Endophthalmitis remains an important complication of surgery, injections, and trauma. The EVS provided important guidelines which remain relevant to this date.Citation196 However, those guidelines were derived from cases of acute-onset postoperative endophthalmitis following cataract surgery and secondary IOL implantation and cannot be directly applied to other categories of endophthalmitis. Although it appears unlikely that large-scale randomized clinical trials will be performed on these other categories of endophthalmitis, management strategies continue to evolve by consensus and based on published clinical series.
Accurate identification of causative organisms of endophthalmitis is important, especially in patients who fail to respond to initial broad-spectrum therapy. Newer diagnostic techniques such as RT-PCR may provide more accurate and more sensitive results than traditional culture methods, although at the present time these techniques are not widely available outside of major medical centers.
The types of pathogens involved in infectious endophthalmitis and their antibiotic susceptibilities evolve over time, requiring periodic reassessment. At the present time, almost all isolates are susceptible to the combination of vancomycin and ceftazidime.Citation159,Citation160 As we continue to collect clinical trial data, treatment of endophthalmitis should continue to improve.
Disclosure
This study was partially supported by NIH Center Core Grant P30EY014801 and an unrestricted grant from Research to Prevent Blindness, New York, NY. Dr Schwartz has served on advisory boards for Alimera and Bausch + Lomb, and has received speakers’ fees from ThromboGenics. The remaining authors have no financial disclosures.
References
- MamalisNEndophthalmitisJ Cataract Refract Surg200228572973011978440
- SmithSRKrollAJLouPLRyanEAEndogenous bacterial and fungal endophthalmitisInt Ophthalmol Clin200747217318317450017
- MoloneyTPParkJMicrobiological isolates and antibiotic sensitivities in culture-proven endophthalmitis: a 15-year reviewBr J Ophthalmol201498111492149724939423
- VerbraekenHTreatment of postoperative endophthalmitisOphthalmologica199520931651717630625
- WykoffCCParrottMBFlynnHWJrShiWMillerDAlfonsoECNosocomial acute-onset postoperative endophthalmitis at a University Teaching Hospital (2002–2009)Am J Ophthalmol20101503392.e2398.e220619391
- MillerJJScottIUFlynnHWJrSmiddyWENewtonJMillerDAcute-onset endophthalmitis after cataract surgery (2000–2004): incidence, clinical settings, and visual acuity outcomes after treatmentAm J Ophthalmol2005139698398715953426
- RavindranRDVenkateshRChangDFSenguptaSGyatshoJTalwarBIncidence of post-cataract endophthalmitis at Aravind Eye Hospital: outcomes of more than 42,000 consecutive cases using standardized sterilization and prophylaxis protocolsJ Cataract Refract Surg200935462963619304082
- FreemanEERoy-GagnonM-HFortinEGauthierDPopescuMBoisjolyHRate of endophthalmitis after cataract surgery in quebec, Canada, 1996–2005Arch Ophthalmol2010128223023420142547
- MoshirfarMFeizVVitaleATWegelinJABasavanthappaSWolseyDHEndophthalmitis after uncomplicated cataract surgery with the use of fourth-generation fluoroquinolones: a retrospective observational case seriesOphthalmology2007114468669117184840
- JensenMKFiscellaRGMoshirfarMMooneyBThird- and fourth-generation fluoroquinolones: retrospective comparison of endophthalmitis after cataract surgery performed over 10 yearsJ Cataract Refract Surg20083491460146718721704
- FrilingELundströmMSteneviUMontanPSix-year incidence of endophthalmitis after cataract surgery: Swedish national studyJ Cataract Refract Surg2013391152123245359
- KeayLGowerEWCassardSDTielschJMScheinODPostcataract surgery endophthalmitis in the United States: analysis of the complete 2003 to 2004 Medicare database of cataract surgeriesOphthalmology2012119591492222297029
- AlharbiSSAlrajhiAAlkahtaniEEndophthalmitis following keratoplasty: incidence, microbial profile, visual and structural outcomesOcul Immunol Inflamm201322321822324131044
- TabanMBehrensANewcombRLNobeMYMcDonnellPJIncidence of acute endophthalmitis following penetrating keratoplasty: a systematic reviewArch Ophthalmol2005123560560915883278
- TayEBainbridgeJda CruzLSubretinal abscess after scleral buckling surgery: a rare risk of retinal surgeryCan J Ophthalmol200742114114217361261
- Al-TorbakAAAl-ShahwanSAl-JadaanIAl-HommadiAEdwardDPEndophthalmitis associated with the Ahmed glaucoma valve implantBr J Ophthalmol200589445445815774923
- RamuluPYDoDVCorcoranKJCorcoranSLRobinALUse of retinal procedures in medicare beneficiaries from 1997 to 2007Arch Ophthalmol2010128101335134020938004
- GovettoAVirgiliGMenchiniFLanzettaPMenchiniUA systematic review of endophthalmitis after microincisional versus 20-gauge vitrectomyOphthalmology2013120112286229123769332
- KunimotoDYKaiserRSIncidence of endophthalmitis after 20- and 25-gauge vitrectomyOphthalmology2007114122133213717916378
- EifrigCWGScottIUFlynnHWJrSmiddyWENewtonJEndophthalmitis after pars plana vitrectomy: incidence, causative organisms, and visual acuity outcomesAm J Ophthalmol2004138579980215531315
- ShiX-YZhaoH-SWeiW-BAnalysis of post-operative endophthalmitis after pars plana vitrectomy: a 10-year experience at a single centerChin Med J (Engl)2013126152890289323924462
- ScottIUFlynnHWJrDevSEndophthalmitis after 25-gauge and 20-gauge pars plana vitrectomy: incidence and outcomesRetina200828113814218185150
- ParkJCRamasamyBShawSA prospective and nationwide study investigating endophthalmitis following pars plana vitrectomy: incidence and risk factorsBr J Ophthalmol201498452953310.1136/bjophthalmol-2013-30448524420916
- Endophthalmitis Vitrectomy Study GroupResults of the endophthalmitis vitrectomy study: a randomized trial of immediate vitrectomy and of intravenous antibiotics for the treatment of postoperative bacterial endophthalmitisArch Ophthalmol199511312147914967487614
- ParkJCRamasamyBShawSA prospective and nationwide study investigating endophthalmitis following pars plana vitrectomy: clinical presentation, microbiology, management and outcomeBr J Ophthalmol20149881080108610.1136/bjophthalmol-2013-30448624686917
- HatchWVCernatGWongDDevenyiRBellCMRisk factors for acute endophthalmitis after cataract surgery: a population-based studyOphthalmology2009116342543019091417
- LalithaPRajagopalanJPrakashKRamasamyKPrajnaNVSrinivasanMPostcataract endophthalmitis in South India: incidence and outcomeOphthalmology2005112111884188916157381
- WestESBehrensAMcDonnellPJTielschJMScheinODThe incidence of endophthalmitis after cataract surgery among the U.S. Medicare population increased between 1994 and 2001Ophthalmology200511281388139415953637
- ESCRS Endophthalmitis Study GroupProphylaxis of postoperative endophthalmitis following cataract surgery: results of the ESCRS multicenter study and identification of risk factorsJ Cataract Refract Surg200733697898817531690
- CaoHZhangLLiLLoSRisk factors for acute endophthalmitis following cataract surgery: a systematic review and meta-analysisPLoS One201388e7173123990980
- MenikoffJASpeakerMGMarmorMRaskinEMA case-control study of risk factors for postoperative endophthalmitisOphthalmology19919812176117681775307
- Romero-ArocaPMéndez-MarinISalvat-SerraMFernández-BallartJAlmena-GarciaMReyes-TorresJResults at seven years after the use of intracamerular cefazolin as an endophthalmitis prophylaxis in cataract surgeryBMC Ophthalmol2012121222272570
- García-SáenzMCArias-PuenteARodríguez-CaravacaGBañuelosJBEffectiveness of intracameral cefuroxime in preventing endophthalmitis after cataract surgery: ten-year comparative studyJ Cataract Refract Surg201036220320720152598
- PleyerUGeldsetzerKProphylaxe der postoperativen infektiösen Endophthalmitis durch intrakamerale Cefuroximgabe – auf dem Weg zum Therapiestandard [Will intracameral cefuroxime become the new standard in endophtaalmitis prevention]?Klin Monbl Augenheilkd200822511934940 German19016201
- LundströmMWejdeGSteneviUThorburnWMontanPEndophthalmitis after cataract surgery: a nationwide prospective study evaluating incidence in relation to incision type and locationOphthalmology2007114586687017324467
- Al-MezaineHSKangaveDAl-AssiriAAl-RajhiAAAcute-onset nosocomial endophthalmitis after cataract surgery: incidence, clinical features, causative organisms, and visual outcomesJ Cataract Refract Surg200935464364919304084
- LiJMorletNNgJQSemmensJBKnuimanMWSignificant nonsurgical risk factors for endophthalmitis after cataract surgery: EPSWA fourth reportInvest Ophthalmol Vis Sci20044551321132815111584
- WallinTParkerJJinYKefalopoulosGOlsonRJCohort study of 27 cases of endophthalmitis at a single institutionJ Cataract Refract Surg200531473574115899450
- AabergTMJrFlynnHWJrSchiffmanJNewtonJNosocomial acute-onset postoperative endophthalmitis survey: a 10-year review of incidence and outcomesOphthalmology19981056100410109627649
- KunimotoDYDasTSharmaSMicrobiologic spectrum and susceptibility of isolates: Part I. Postoperative endophthalmitisAm J Ophthalmol1999128224024210458187
- AnandARThereseKLMadhavanHNSpectrum of aetiological agents of postoperative endophthalmitis and antibiotic susceptibility of bacterial isolatesIndian J Ophthalmol200048212311116508
- JohnsonMWDoftBHKelseySFThe endophthalmitis vitrectomy study: relationship between clinical presentation and microbiologic spectrumOphthalmology199710422612729052630
- ShirodkarARPathengayAFlynnHWJrDelayed- versus acute-onset endophthalmitis after cataract surgeryAm J Ophthalmol20121533391.e2398.e222030353
- Al-MezaineHAl-AssiriAAl-RajhiAIncidence, clinical features, causative organisms, and visual outcomes of delayed-onset pseudophakic endophthalmitisEur J Ophthalmol200819580481119787601
- FoxGMJoondephBCFlynnHWJrPflugfelderSCRousselTJDelayed-onset pseudophakic endophthalmitisAm J Ophthalmol199111121631731992736
- Brillat-ZaratzianEBronAAptelFFRIENDS Group: clinical and microbiological characteristics of post-filtering surgery endophthalmitisGraefes Arch Clin Exp Ophthalmol2014252110110724248809
- BusbeeBGRecchiaFMKaiserRNagraPRosenblattBPearlmanRBBleb-associated endophthalmitis: clinical characteristics and visual outcomesOphthalmology200411181495150315288977
- SongAScottIUFlynnHWJrBudenzDLDelayed-onset bleb-associated endophthalmitis: clinical features and visual acuity outcomesOphthalmology2002109598599111986108
- YamamotoTSawadaAMayamaCThe 5-year incidence of bleb-related infection and its risk factors after filtering surgeries with adjunctive mitomycin C: collaborative bleb-related infection incidence and treatment study 2Ophthalmology201412151001100624424248
- CiullaTABeckADToppingTMBakerASBlebitis, early endophthalmitis, and late endophthalmitis after glaucoma-filtering surgeryOphthalmology199710469869959186440
- YamamotoTKuwayamaYKanoKSawadaAShojiNStudy Group for the Japan Glaucoma Society Survey of Bleb-related InfectionClinical features of bleb-related infection: a 5-year survey in JapanActa Ophthalmol201391761962422883301
- AlwitryAKingAJSurveillance of late-onset bleb leak, blebitis and bleb-related endophthalmitis – a UK incidence studyGraefes Arch Clin Exp Ophthalmol201225081231123622249317
- DeBryPWPerkinsTWHeatleyGKaufmanPBrumbackLCIncidence of late-onset bleb-related complications following trabeculectomy with mitomycinArch Ophthalmol2002120329730011879132
- GreenfieldDSSuñerIJMillerMPKangasTAPalmbergPFFlynnHWJrEndophthalmitis after filtering surgery with mitomycinArch Ophthalmol199611489439498694729
- KatzLJCantorLBSpaethGLComplications of surgery in glaucoma. Early and late bacterial endophthalmitis following glaucoma filtering surgeryOphthalmology19859279599633895103
- SolomonATichoUFrucht-PeryJLate-onset, bleb-associated endophthalmitis following glaucoma filtering surgery with or without antifibrotic agentsJ Ocul Pharmacol Ther199915428329310463867
- MochizukiKJikiharaSAndoYHoriNYamamotoTKitazawaYIncidence of delayed onset infection after trabeculectomy with adjunctive mitomycin C or 5-fluorouracil treatmentBr J Ophthalmol199781108778839486030
- MuckleyEDLehrerRALate-onset blebitis/endophthalmitis: incidence and outcomes with mitomycin COptom Vis Sci200481749950415252348
- KuangT-MLinY-CLiuCJ-LHsuW-MChouC-KEarly and late endophthalmitis following trabeculectomy in a Chinese populationEur J Ophthalmol2008181667018203087
- WallinÖAl-ahramy AbdullahMLundströmMMontanPEndophthalmitis and severe blebitis following trabeculectomy. Epidemiology and risk factors; a single-centre retrospective studyActa Ophthalmol201492542643124020653
- Ba’arahBTSmiddyWEBleb-related endophthalmitis: clinical presentation, isolates, treatment and visual outcome of culture-proven casesMiddle East Afr J Ophthalmol2009161202420142955
- SharanSTropeGEChipmanMBuysYMLate-onset bleb infections: prevalence and risk factorsCan J Ophthalmol200944327928319491982
- YeHSunXGanDBleb-associated endophthalmitis in a Chinese population (2003–2010): clinical characteristics and visual outcomeEur J Ophthalmol201222571972522287170
- PoulsenEJAllinghamRRCharacteristics and risk factors of infections after glaucoma filtering surgeryJ Glaucoma20009643844311131749
- HoriNMochizukiKIshidaKYamamotoTMikamoHClinical characteristics and risk factors of glaucoma filtering bleb infectionsNihon Ganka Gakkai Zasshi200911310951963 Japanese19882931
- JampelHDQuigleyHAKerrigan-BaumrindLAMeliaBMFriedmanDBarronYRisk factors for late-onset infection following glaucoma filtration surgeryArch Ophthalmol200111971001100811448322
- AshkenaziIMelamedSAvniIBartovEBlumenthalMRisk factors associated with late infection of filtering blebs and endophthalmitisOphthalmic Surg199122105705741961613
- KupinTHJuzychMSShinDHKhatanaAKOlivierMMAdjunctive mitomycin C in primary trabeculectomy in phakic eyesAm J Ophthalmol1995119130397825687
- LehmannOJBunceCMathesonMMRisk factors for development of post-trabeculectomy endophthalmitisBr J Ophthalmol200084121349135311090471
- RaiPKotechaAKaltsosKChanging trends in the incidence of bleb-related infection in trabeculectomyBr J Ophthalmol201296797197522334138
- LengTMillerDFlynnHWJrJacobsDJGeddeSJDelayed-onset bleb-associated endophthalmitis (1996–2008): causative organisms and visual acuity outcomesRetina201131234435220838358
- FiletaJBScottIUFlynnHWJrMeta-analysis of infectious endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agentsOphthalmic Surg Lasers Imaging Retina201445214314924635156
- WestfallACOsbornAKuhlDBenzMSMielerWFHolzERAcute endophthalmitis incidence: intravitreal triamcinoloneArch Ophthalmol200512381075107716087840
- MoshfeghiDMKaiserPKScottIUAcute endophthalmitis following intravitreal triamcinolone acetonide injectionAm J Ophthalmol2003136579179614597028
- BhavsarARIpMSGlassmanARDRCRnet and the SCORE Study GroupsThe risk of endophthalmitis following intravitreal triamcinolone injection in the DRCRnet and SCORE clinical trialsAm J Ophthalmol2007144345445617765429
- RothDBFlynnHWJrDistinguishing between infectious and noninfectious endophthalmitis after intravitreal triamcinolone injectionAm J Ophthalmol2008146334634718724979
- GoldbergRAShahCPWiegandTWHeierJSNoninfectious inflammation after intravitreal injection of aflibercept: clinical characteristics and visual outcomesAm J Ophthalmol20141584733.e1737.e124983791
- ChongDYAnandRWilliamsPDQureshiJACallananDGCharacterization of sterile intraocular inflammatory responses after intravitreal bevacizumab injectionRetina20103091432144020559156
- WickremasingheSSMichalovaKGilhotraJAcute intraocular inflammation after intravitreous injections of bevacizumab for treatment of neovascular age-related macular degenerationOphthalmology2008115111911191518672291
- GeorgopoulosMPolakKPragerFPrünteCSchmidt-ErfurthUCharacteristics of severe intraocular inflammation following intravitreal injection of bevacizumab (Avastin)Br J Ophthalmol200993445746219033289
- SakamotoTIshibashiTOguraYSurvey of triamcinolone-related non-infectious endophthalmitisNihon Ganka Gakkai Zasshi2011115652352821735756
- AhnSJKimTWAhnJHuhJWYuHGChungHAssociated factors and treatment outcome of presumed noninfectious endophthalmitis occurring after intravitreal triamcinolone acetonide injectionGraefes Arch Clin Exp Ophthalmol2013251371572322820815
- IrigoyenCZiahosseiniKMorphisGStapplerTHeimannHEndophthalmitis following intravitreal injectionsGraefes Arch Clin Exp Ophthalmol2012250449950522048244
- MoshfeghiAARosenfeldPJFlynnHWJrEndophthalmitis after intravitreal vascular endothelial growth factor antagonists: a six-year experience at a university referral centerRetina201131466266821836400
- DiagoTMcCannelCABakriSJPulidoJSEdwardsAOPachJMInfectious endophthalmitis after intravitreal injection of antiangiogenic agentsRetina200929560160519357558
- Mezad-KourshDGoldsteinMHeilwailGZayit-SoudrySLoewensteinABarakAClinical characteristics of endophthalmitis after an injection of intravitreal antivascular endothelial growth factorRetina20103071051105720616683
- ArtunayOYuzbasiogluERasierRSengülABahceciogluHIncidence and management of acute endophthalmitis after intrav-itreal bevacizumab (Avastin) injectionEye (Lond)200923122187219319218994
- LyallDATeyAFootBPost-intravitreal anti-VEGF endophthalmitis in the United Kingdom: incidence, features, risk factors, and outcomesEye (Lond)201226121517152623060022
- EntezariMRamezaniAAhmadiehHGhasemiHBatch-related sterile endophthalmitis following intravitreal injection of bevacizumabIndian J Ophthalmol201462446847123619494
- McCannelCAMeta-analysis of endophthalmitis after intravitreal injection of anti-vascular endothelial growth factor agents: causative organisms and possible prevention strategiesRetina201131465466121330939
- GordonDFJongBBIndigenous flora from human salivaAppl Microbiol196816242842916349796
- FanJCNiedererRLvon LanyHPolkinghornePJInfectious endophthalmitis: clinical features, management and visual outcomesClin Experiment Ophthalmol200836763163618983548
- BhoomibunchooCRatanapakornTSinawatSSanguansakTMoontaweeKYospaiboonYInfectious endophthalmitis: review of 420 casesClin Ophthalmol2013724725223403798
- NicoarăSDIrimescuICăliniciTCristianCOutcome and prognostic factors for traumatic endophthalmitis over a 5-year periodJ Ophthalmol2014201474701525302113
- EssexRWYiQCharlesPGPAllenPJPost-traumatic endophthal-mitisOphthalmology2004111112015202215522366
- ZhangYZhangMNJiangCHYaoYZhangKEndophthalmitis following open globe injuryBr J Ophthalmol201094111111419692359
- ColyerMHWeberEDWeichelEDDelayed intraocular foreign body removal without endophthalmitis during Operations Iraqi Freedom and Enduring FreedomOphthalmology200711481439144717331579
- AndreoliCMAndreoliMTKloekCEAhueroAEVavvasDDurandMLLow rate of endophthalmitis in a large series of open globe injuriesAm J Ophthalmol20091474601.e2608.e219181306
- YangC-SLuC-KLeeF-LHsuW-MLeeY-FLeeS-MTreatment and outcome of traumatic endophthalmitis in open globe injury with retained intraocular foreign bodyOphthalmologica20102242798519707031
- FaghihiHHajizadehFEsfahaniMRPosttraumatic endophthalmitis: report No 2Retina201232114615121775927
- DehghaniARRezaeiLSalamHMohammadiZMahboubiMPost traumatic endophthalmitis: incidence and risk factorsGlob J Health Sci2014663663410.5539/gjhs.v6n6p68
- ChaudhryIAShamsiFAAl-HarthiEAl-TheebAElzaridiERileyFCIncidence and visual outcome of endophthalmitis associated with intraocular foreign bodiesGraefes Arch Clin Exp Ophthalmol2008246218118617468878
- LiEYMChanTCYLiuATWYuenHKLLow endophthalmitis rate and absence of sympathetic ophthalmia after open globe injuries – a ten-year review of open globe injuryJ Clin Exp Ophthalmol201453282
- AlfaroDVRothDLiggettPEPosttraumatic endophthalmitis. Causative organisms, treatment, and preventionRetina19941432062117973114
- ReynoldsDSFlynnHWJrEndophthalmitis after penetrating ocular traumaCurr Opin Ophthalmol199783323810168892
- ParkeDWPathengayAFlynnHWJrAlbiniTSchwartzSGRisk factors for endophthalmitis and retinal detachment with retained intraocular foreign bodiesJ Ophthalmol2012201275852622619702
- ThompsonJTParverLMEngerCLMielerWFLiggettPEInfectious endophthalmitis after penetrating injuries with retained intraocular foreign bodies. National Eye Trauma SystemOphthalmology199310010146814748414406
- LongCLiuBXuCJingYYuanZLinXCausative organisms of post-traumatic endophthalmitis: a 20-year retrospective studyBMC Ophthalmol2014143424661397
- JindalAPathengayAMithalKEndophthalmitis after open globe injuries: changes in microbiological spectrum and isolate susceptibility patterns over 14 yearsJ Ophthalmic Inflamm Infect201441524548669
- AhmedYSchimelAMPathengayAColyerMHFlynnHWJrEndophthalmitis following open-globe injuriesEye (Lond)201226221221722134598
- WongJSChanTKLeeHMCheeSPEndogenous bacterial endophthalmitis: an east Asian experience and a reappraisal of a severe ocular afflictionOphthalmology200010781483149110919895
- PuliafitoCABakerASHaafJFosterCSInfectious endophthalmitis. Review of 36 casesOphthalmology19828989219296982445
- ShraderSKBandJDLauterCBMurphyPThe clinical spectrum of endophthalmitis: incidence, predisposing factors, and features influencing outcomeJ Infect Dis199016211151202355187
- KresloffMSCastellarinAAZarbinMAEndophthalmitisSurv Ophthalmol19984331932249862309
- KrauseLBechrakisNEHeimannHKildalDFoersterMHIncidence and outcome of endophthalmitis over a 13-year periodCan J Ophthalmol2009441889419169320
- LimHWShinJWChoHYEndogenous endophthalmitis in the Korean population: a six-year retrospective studyRetina201434359260224056527
- BinderMIChuaJKaiserPKProcopGWIsadaCMEndogenous endophthalmitis: an 18-year review of culture-positive cases at a tertiary care centerMedicine (Baltimore)20038229710512640186
- ZhangHLiuZEndogenous endophthalmitis: a 10-year review of culture-positive cases in northern ChinaOcul Immunol Inflamm201018213313820370344
- JacksonTLParaskevopoulosTGeorgalasISystematic review of 342 cases of endogenous bacterial endophthalmitisSurv Ophthalmol Epub6182014
- SchiedlerVScottIUFlynnHWJrDavisJLBenzMSMillerDCulture-proven endogenous endophthalmitis: clinical features and visual acuity outcomesAm J Ophthalmol2004137472573115059712
- ChungKSKimYKSongYGClinical review of endogenous endophthalmitis in Korea: a 14-year review of culture positive cases of two large hospitalsYonsei Med J201152463063421623606
- LeibovitchILaiTRaymondGZadehRNathanFSelvaDEndogenous endophthalmitis: a 13-year review at a tertiary hospital in South AustraliaScand J Infect Dis200537318418915849050
- OkadaAAJohnsonRPLilesWCD’AmicoDJBakerASEndogenous bacterial endophthalmitis. Report of a ten-year retrospective studyOphthalmology199410158328388190467
- ConnellPPO’NeillECFabinyiDEndogenous endophthalmitis: 10-year experience at a tertiary referral centreEye (Lond)2011251667220966972
- EssmanTFFlynnHWJrSmiddyWETreatment outcomes in a 10-year study of endogenous fungal endophthalmitisOphthalmic Surg Lasers19972831851949076791
- ShankarKGyanendraLHariSNarayanSDCulture proven endogenous bacterial endophthalmitis in apparently healthy individualsOcul Immunol Inflamm200917639639920001259
- LingappanAWykoffCCAlbiniTAEndogenous fungal endophthalmitis: causative organisms, management strategies, and visual acuity outcomesAm J Ophthalmol20121531162.e1166.e121917234
- NessTPelzKHansenLLEndogenous endophthalmitis: microorganisms, disposition and prognosisActa Ophthalmol Scand200785885285617725616
- ChenY-JKuoH-KWuP-CA 10-year comparison of endogenous endophthalmitis outcomes: an east Asian experience with Klebsiella pneumoniae infectionRetina200424338339015187660
- ForsterRKAbbottRLGelenderHManagement of infectious endophthalmitisOphthalmology19808743133196967200
- KattanHMFlynnHWJrPflugfelderSCRobertsonCForsterRKNosocomial endophthalmitis survey. Current incidence of infection after intraocular surgeryOphthalmology19919822272382008282
- DonahueSPKowalskiRPJewartBHFribergTRVitreous cultures in suspected endophthalmitis. Biopsy or vitrectomy?Ophthalmology199310044524558479699
- BarzaMPavanPRDoftBHEvaluation of microbiological diagnostic techniques in postoperative endophthalmitis in the Endophthalmitis Vitrectomy StudyArch Ophthalmol19971159114211509298055
- SandvigKUDannevigLPostoperative endophthalmitis: establishment and results of a national registryJ Cataract Refract Surg20032971273128012900232
- RachitskayaAVFlynnHWJrWongJKuriyanAEMillerDA 10-year study of membrane filter system versus blood culture bottles in culturing vitrectomy cassette vitreous in infectious endophthalmitisAm J Ophthalmol20131562349.e2354.e223668678
- JosephbergRGEndophthalmitis: the latest in current managementRetina2006266 SupplS47S5016832300
- GokceGSobaciGOzgonulCPost-traumatic endophthalmitis: a mini-reviewSemin Ophthalmol Epub2272014
- PatelSNLangerPDZarbinMABhagatNDiagnostic value of clinical examination and radiographic imaging in identification of intraocu-lar foreign bodies in open globe injuryEur J Ophthalmol201222225926821607931
- MoisseievELastDGoezDBarakAMardorYMagnetic resonance imaging and computed tomography for the detection and characterization of nonmetallic intraocular foreign bodiesRetina Epub7302014
- CornutP-LBoissetSRomanetJ-PPrinciples and applications of molecular biology techniques for the microbiological diagnosis of acute post-operative endophthalmitisSurv Ophthalmol201459328630324359808
- OgawaMSugitaSShimizuNWatanabeKNakagawaIMochizukiMBroad-range real-time PCR assay for detection of bacterial DNA in ocular samples from infectious endophthalmitisJpn J Ophthalmol201256652953522936171
- BispoPJMde MeloGBHofling-LimaALPignatariACCDetection and gram discrimination of bacterial pathogens from aqueous and vitreous humor using real-time PCR assaysInvest Ophthalmol Vis Sci201152287388120702819
- OgawaMSugitaSWatanabeKShimizuNMochizukiMNovel diagnosis of fungal endophthalmitis by broad-range real-time PCR detection of fungal 28S ribosomal DNAGraefes Arch Clin Exp Ophthalmol2012250121877188322527320
- SugitaSKamoiKOgawaMWatanabeKShimizuNMochizukiMDetection of Candida and Aspergillus species DNA using broad-range real-time PCR for fungal endophthalmitisGraefes Arch Clin Exp Ophthalmol2012250339139821947326
- LacroixCGicquelASendidBEvaluation of two matrix-assisted laser desorption ionization-time of flight mass spectrometry (MALDI-TOF MS) systems for the identification of Candida speciesClin Microbiol Infect201420215315823594150
- SengPAbatCRolainJMIdentification of rare pathogenic bacteria in a clinical microbiology laboratory: impact of MALDI-TOF mass spectrometryJ Clin Microbiol20135172182219410.1128/JCM.00492-1323637301
- ChungHJCastroCMImHLeeHWeisslederRA magneto-DNA nanoparticle system for rapid detection and phenotyping of bacteriaNat Nanotechnol20138536937523644570
- LottMNFullerJJHancockHAVitreal penetration of oral moxifloxacin in humansRetina200828347347618327141
- HooperCYLightmanSLPachecoPTamPMKKhanATaylorSRJAdjunctive antibiotics in the treatment of acute bacterial endophthalmitis following cataract surgeryActa Ophthalmol2012907e572e57322429465
- AldaveAJSteinJDDeramoVAShahGKFischerDHMaguireJITreatment strategies for postoperative Propionibacterium acnes endophthalmitisOphthalmology1999106122395240110599678
- PackerMChangDFDeweySHPrevention, diagnosis, and management of acute postoperative bacterial endophthalmitisJ Cataract Refract Surg20113791699171421782382
- ChaudharyKMRomeroJMEzonIFastenbergDMDeramoVAPars plana vitrectomy in the management of patients diagnosed with endophthalmitis following intravitreal anti-vascular endothelial growth factor injectionRetina20133371407141623492945
- PrasadNLatinaMABlebitis and endophthalmitis after glaucoma filtering surgeryInt Ophthalmol Clin2007472859717450009
- SternbergPMartinDFManagement of endophthalmitis in the post-endophthalmitis vitrectomy study eraArch Ophthalmol2001119575475511346404
- SridharJFlynnHWJrKuriyanAEMillerDAlbiniTEndogenous fungal endophthalmitis: risk factors, clinical features, and treatment outcomes in mold and yeast infectionsJ Ophthalmic Inflamm Infect2013316024053550
- AabergTMSternbergPJrTrauma: principles and techniques of treatmentRyanSSchachatAWilkinsonCHintonDSaddaSWiedemanPRetinaSt Louis, MOMosby200124002426
- MikoszCASmithRMKimMFungal endophthalmitis associated with compounded productsEmerg Infect Dis201420224825624447640
- SheymanATCohenBZFriedmanAHAckertJMAn outbreak of fungal endophthalmitis after intravitreal injection of compounded combined bevacizumab and triamcinoloneJAMA Ophthalmol2013131786486923640384
- GentileRCShuklaSShahMMicrobiological spectrum and antibiotic sensitivity in endophthalmitis: a 25-year reviewOphthalmology201412181634164224702755
- SchimelAMMillerDFlynnHWJrEndophthalmitis isolates and antibiotic susceptibilities: a 10-year review of culture-proven casesAm J Ophthalmol2013156150.e152.e123540710
- LalwaniGAFlynnHWJrScottIUAcute-onset endophthalmitis after clear corneal cataract surgery (1996–2005). Clinical features, causative organisms, and visual acuity outcomesOphthalmology2008115347347618067969
- MaaloufFAbdulaalMHamamRNChronic postoperative endophthalmitis: a review of clinical characteristics, microbiology, treatment strategies, and outcomesInt J Inflamm20122012313248
- Al-TurkiTAAl-ShahwanSAl-MezaineHSKangaveDAbu El-AsrarAMMicrobiology and visual outcome of bleb-associated endophthalmitisOcul Immunol Inflamm201018212112620370342
- LiebDFScottIUFlynnHWJrMillerDFeuerWJOpen globe injuries with positive intraocular cultures: factors influencing final visual acuity outcomesOphthalmology200311081560156612917173
- CornutP-LYoussefEBBronAA multicentre prospective study of post-traumatic endophthalmitisActa Ophthalmol201391547548222313810
- SimunovicMPRushRBHunyorAPChangAAEndophthalmitis following intravitreal injection versus endophthalmitis following cataract surgery: clinical features, causative organisms and post-treatment outcomesBr J Ophthalmol201296686286622446145
- ShahCPGargSJVanderJFOutcomes and risk factors associated with endophthalmitis after intravitreal injection of anti-vascular endothe-lial growth factor agentsOphthalmology2011118102028203421705087
- NentwichMMYactayo-MirandaYSchwarzbachFWolfAKampikAMino de KasparHEndophthalmitis after intravitreal injection: decreasing incidence and clinical outcome-8-year results from a tertiary ophthalmic referral centerRetina201434594395024136408
- CiullaTAStarrMBMasketSBacterial endophthalmitis prophylaxis for cataract surgery: an evidence-based updateOphthalmology20021091132411772573
- RahmanNMurphyCCImpact of intracameral cefuroxime on the incidence of postoperative endophthalmitis following cataract surgery in IrelandIr J Med Sci20141423934377
- MaBWuXLuWFanXLuoMEvaluation of intracameral cefuroxime injection for endophthalmitis prophylaxis following cataract surgery in a China ophthalmology department during 2009–2013J Clin Exp Ophthalmol201453442
- ShorsteinNHWinthropKLHerrintonLJDecreased postoperative endophthalmitis rate after institution of intracameral antibiotics in a Northern California eye departmentJ Cataract Refract Surg201339181423036356
- Rodríguez-CaravacaGGarcía-SáenzMCVillar-Del-CampoMCAndrés-AlbaYArias-PuenteAIncidence of endophthalmitis and impact of prophylaxis with cefuroxime on cataract surgeryJ Cataract Refract Surg20133991399140323820306
- BarreauGMounierMMarinBAdenisJ-PRobertP-YIntracameral cefuroxime injection at the end of cataract surgery to reduce the incidence of endophthalmitis: French studyJ Cataract Refract Surg20123881370137522814043
- SchimelAMAlfonsoECFlynnHWJrEndophthalmitis prophylaxis for cataract surgery: are intracameral antibiotics necessary?JAMA Ophthalmol2014132111269127025125316
- ChangDFBraga-MeleRMamalisNProphylaxis of postoperative endophthalmitis after cataract surgery: results of the 2007 ASCRS member surveyJ Cataract Refract Surg200733101801180517889779
- VasavadaARGajjarDRajSMVasavadaVVasavadaVComparison of 2 moxifloxacin regimens for preoperative prophylaxis: prospective randomized triple-masked trial. Part 2: residual conjunctival floraJ Cataract Refract Surg20083481383138818655992
- RåenMSandvikGFDrolsumLEndophthalmitis following cataract surgery: the role of prophylactic postoperative chloramphenicol eye dropsActa Ophthalmol201391211812222151787
- AveryRLBakriSJBlumenkranzMSIntravitreal injection technique and monitoring: updated guidelines of an expert panelRetinaIn press
- FriedmanDAMasonJOEmondTMcgwinGPovidone–iodine contact time and lid speculum use during intravitreal injectionRetina201333597598123416514
- WenJCMcCannelCAMochonAGarnerOBBacterial dispersal associated with speech in the setting of intravitreous injectionsArch Ophthalmol2011129121551155421825179
- SchimelAMScottIUFlynnHWJrEndophthalmitis after intravitreal injections: Should the use of face masks be the standard of care?Arch Ophthalmol2011129121607160922159682
- ScottIUFlynnHWJrReducing the risk of endophthalmitis following intravitreal injectionsRetina2007271101217218909
- StoreyPDollinMPitcherJThe role of topical antibiotic prophylaxis to prevent endophthalmitis after intravitreal injectionOphthalmology2014121128328924144453
- MossJMSanisloSRTaCNA prospective randomized evaluation of topical gatifloxacin on conjunctival flora in patients undergoing intravitreal injectionsOphthalmology200911681498150119501409
- DhootSBKunjukunjuNSabatesNThe role of prophylactic antibiotic use in prevention of endophthalmitis following intravitreal injection of anti-vascular endothelial growth factor agents: a meta-analysisOpen J Ophthalmol2013324649
- CheungCSYWongAWTLuiAKertesPJDevenyiRGLamWCIncidence of endophthalmitis and use of antibiotic prophylaxis after intravitreal injectionsOphthalmology201211981609161422480743
- YinVTWeisbrodDJEngKTAntibiotic resistance of ocular surface flora with repeated use of a topical antibiotic after intravitreal injectionJAMA Ophthalmol2013131445646123430175
- KimSJTomaHSAntimicrobial resistance and ophthalmic antibiotics: 1-year results of a longitudinal controlled study of patients undergoing intravitreal injectionsArch Ophthalmol201112991180118821911665
- NarangSGuptaVGuptaADograMRPandavSSDasSRole of prophylactic intravitreal antibiotics in open globe injuriesIndian J Ophthalmol2003511394412701861
- SchmidsederEde KasparHMKampikAKlaußVPost-traumatic endophthalmitis after penetrating eye injury. Risk factors, microbiological diagnosis and functional outcomeOphthalmologe1998953153157 German9578692
- WoodcockMGLScottRAHHuntbachJKirkbyGRMass and shape as factors in intraocular foreign body injuriesOphthalmology2006113122262226917157134
- SoheilianMRafatiNMohebbiMProphylaxis of acute post-traumatic bacterial endophthalmitis: a multicenter, randomized clinical trial of intraocular antibiotic injection, report 2Arch Ophthalmol2007125446046517420365
- ReynoldsACSkutaGLMonluxRJohnsonJManagement of blebitis by members of the American Glaucoma Society: a surveyJ Glaucoma200110434034711558820
- SoltauJBRothmanRFBudenzDLRisk factors for glaucoma filtering bleb infectionsArch Ophthalmol2000118333834210721955
- FlynnHWJrScottIULegacy of the Endophthalmitis Vitrectomy StudyArch Ophthalmol2008126455956118413530