
Abstract
Aim
The aim of this report was to present a case of varicella zoster virus (VZV)-associated anterior uveitis, which developed in an adult who was seronegative for anti-VZV antibodies.
Case presentation
A 66-year-old male patient was referred to the National Defense Medical College, Tokorozawa City, Japan with iridocyclitis in his right eye. On examination, intraocular pressure was 30 mmHg in the right eye, and biomicroscopy revealed ciliary injection, corneal epithelial edema, mutton fat keratic precipitates, flare, and infiltrating cells in the anterior chamber. Serological tests were negative for anti-VZV antibodies, but VZV-DNA copies of 1.28×107 copies/mL were detected by quantitative reverse transcriptase polymerase chain reaction using the aqueous humor obtained from the right eye. Iridocyclitis was reduced by administration of oral valaciclovir in addition to corticosteroid eye drops, and serum anti-VZV antibodies were first detected after 4 months’ administration. When ocular inflammation was resolved after 6 months, VZV-DNA could not be detected in the aqueous humor any more.
Conclusion
VZV-associated uveitis may develop in an adult with undetectable serum anti-VZV antibodies. Multiplex polymerase chain reaction of the aqueous humor is the key investigation necessary for the diagnosis in such cases.
Introduction
Reactivation of latent varicella zoster virus (VZV) infection may cause anterior uveitis.Citation1 Ocular manifestations are usually described as unilateral iridocyclitis with mutton-fat keratic precipitates, elevation of intraocular pressure, and late sectorial iris atrophy.Citation2 VZV-associated anterior uveitis with skin lesions along the first branch of the trigeminal nerve is called herpes zoster ophthalmicus (HZO), although HZO can present without any eye problems (anterior uveitis and/or keratitis); HZO without skin lesions is known as zoster sine herpete (ZSH).Citation3 In these cases, serum anti-VZV antibodies are detected, which allow confirmation of prior VZV infection.Citation1 We report a case of ZSH in an adult who was seronegative for anti-VZV antibodies at presentation.
Case presentation
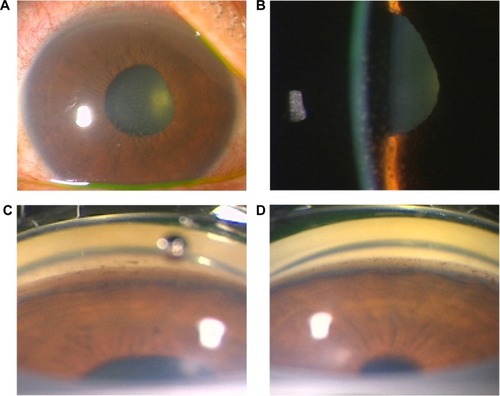
A 66-year-old man was referred to our hospital, the National Defense Medical College, Tokorozawa City, Japan from an ophthalmology clinic with a 1-week history of visual disturbance in his right eye. There was no ocular history of trauma, inflammation, or medication. His family history and medical history for systemic diseases were unremarkable. At presentation, the best corrected visual acuity was 20/30 in the right eye and 20/15 in the left eye. Intraocular pressure (IOP) was 30 mmHg in the right eye and 14 mmHg in the left eye. Biomicroscopy revealed ciliary injection, corneal epithelial edema, mutton-fat keratic precipitates, flare, and infiltrating cells in the anterior chamber of the right eye (). In addition, pigmentation of trabecular pigment band in the angle was increased in the right eye compared with the left eye (). Although mild opacity and cell infiltration in the anterior vitreous of the right eye were present, retinitis or retinal vasculitis was not observed. No abnormalities were found in the left eye.
Figure 1 Ocular findings at presentation.
In addition to the laboratory blood tests, the multiplex polymerase chain reaction (PCR) for human herpes viruses (HHVs) 1 through 8, of the aqueous humor from the right eye was performed, and treatment with topical 0.1% betamethasone, mydriatic (0.1% phenylephrine and 0.1% tropicamide), and 0.005% latanoprost for ocular hypertension was initiated. The serological tests were negative for syphilis and anti-herpes simplex virus, as well as anti-VZV antibodies. However, VZV-DNA was detected by multiplex PCR in the aqueous humor obtained from the right eye, and quantitative real-time PCR revealed VZV-DNA copies of 1.28×107 copies/mL. Although the patient had not been vaccinated for VZV, there was no history of chickenpox in childhood or later, and serum anti-VZV antibodies were not detected. However, ZSH was diagnosed since the clinical findings were compatible with VZV-associated anterior uveitis and skin lesions were absent, thus excluding HZO.
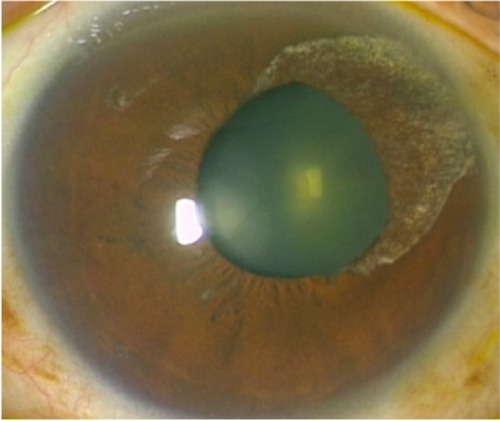
We initiated medical treatment for VZV with oral valaciclovir 1,500 mg three times a day for 1 month, in addition to the topical treatment. Ocular inflammation resolved gradually, and IOP decreased to lower than 21 mmHg. VZV-DNA in the aqueous humor was reduced to 4.08×104 copies/mL at 3 months after the first visit, and serum anti-VZV antibodies were first detected after 4 months. Distorted pupil and fan-shaped iris atrophy, which are characteristics of VZV iridocyclitis, appeared at the upper nasal iris (). Ocular inflammation was not observed at 6 months, and VZV-DNA was not detected from the aqueous humor. Written informed consent was obtained from the patient for publication of this case report and accompanying images.
Figure 2 Ocular findings observed after treatment was started.
Discussion
VZV is transmitted through respiratory droplets. An initial viremia is followed by viral spread to the skin, the eye, and then the sensory ganglia throughout the body, where the virus establishes latency. Primary infection of VZV manifests as a generalized vascular rash (chicken pox) caused by inhaled virus particles, and thereafter the virus may reside dormant in sensory nerve ganglia for many years.Citation4 Ocular diseases such as keratitis, anterior uveitis, and acute retinal necrosis are secondary clinical manifestations of VZV infection as well as herpes zoster, and serum anti-VZV antibodies are in principle positive when ocular disease develops.Citation3 In the present case, although serum anti-VZV antibodies were negative, the clinical findings such as unilateral iridocyclitis with mutton-fat keratic precipitates and elevated IOP were compatible with the characteristics of VZV-associated anterior uveitis. A definitive diagnosis was made isolating the VZV DNA in the aqueous humor with multiplex PCR and quantitative real time PCR. Thus, the multiplex PCR and quantitative real time PCR results were key to arriving at the correct diagnosis in this case.
Thus, multiplex PCR and quantitative real time PCR are definitely useful for the diagnosis in this type of case. VZV-DNA was detected in the aqueous humor in larger number of copies at presentation, which decreased and disappeared along with the improvement of ocular inflammation by valaciclovir treatment. Since serum anti-VZV antibodies, fan-shaped iris atrophy, and distorted pupil emerged thereafter, the diagnosis based on multiplex PCR was confirmed clinically.
Since it has been reported that microdendritic keratitis, nummular keratitis, disciform keratitis, mucous plaque keratitis, sclerokeratitis, and iridocyclitis may occur during primary infection of VZV, although with less frequency,Citation5 this case might be atypical ZSH developed following primary VZV infection that did not clinically manifest systemic varicella symptoms. However, most cases of primary VZV infection are mild, or are not recognized as chickenpox.Citation4 In addition, anti-VZV antibodies in the present case were tested by complement fixation test which is less sensitive than enzyme immunoassay.Citation6 Therefore, in this case, we cannot exclude a possibility of prior infection with VZV before the development of ocular manifestations.
Conclusion
ZSH may develop in an adult without serum anti-VZV antibodies and without a history of chickenpox. In such cases, multiplex PCR using aqueous humor is useful for a definitive diagnosis.
Author contributions
IM participated in treatment of the patient, analysis and interpretation of data, and drafted the manuscript. SI participated in diagnosis and treatment of the patient, designed the structure of the manuscript, and critically revised the manuscript for important intellectual content. MT participated in analysis and interpretation of data, and critically revised the manuscript for important intellectual content. All authors have given final approval of the version to be published. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors read and approved the final manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
- LiesegangTJHerpes zoster virus infectionCurr Opin Ophthalmol200415653153615523199
- KidoSSugitaSHorieSAssociation of varicella zoster virus load in the aqueous humor with clinical manifestations of anterior uveitis in herpes zoster ophthalmicus and zoster sine herpeteBr J Ophthalmol200892450550818245272
- LiesegangTJHerpes zoster ophthalmicus: natural history, risk factors, clinical presentation, and morbidityOphthalmology20081152 SupplS3S1218243930
- ArvinAMVaricella-zoster virusClin Microbiol Rev1996933613818809466
- Pavan-LangstonDViral disease of the ocular anterior segment: basic science and clinical diseaseSmolinGFosterCSAzarDTDohlmanCHSmolin and Thoft’s The Cornea: Scientific Foundations and Clinical Practice4th edPhiladelphiaLippincott Williams and Wilkins2005297393
- ForghaniBSchmidtNJDennisJAntibody assays for varicella-zoster virus: comparison of enzyme immunoassay with neutralization, immune adherence hemagglutination, and complement fixationJ Clin Microbiol197885545552215602