
Abstract
Purpose
To investigate the clinical outcomes of tube shunt coverage using sterile gamma-irradiated cornea allograft.
Patients and methods
The Wills Eye Hospital Glaucoma Research Center retrospectively reviewed the medical records of 165 patients who underwent glaucoma tube shunt procedures using sterile gamma-irradiated cornea allograft (VisionGraft) between December 2012 and November 2013. Demographic characteristics, type of tube shunt, and position were noted. Complications were recorded at 1 day; 1 week; 1, 3, 6, and 12 months; and on the final postoperative visit.
Results
One hundred and sixty-nine eyes of 165 patients were included. The mean follow-up time was 4.8±3.5 (ranging from 1 to 16) months. There was no evidence of immunological reaction, infection, or exposure in 166 eyes (98.2%). Three eyes (1.8%) experienced graft or tube exposure within the first 3 postoperative months. Two of the cases had underlying diseases: bullous pemphigoid and chronic allergic conjunctivitis.
Conclusion
Coverage of tube shunts using gamma-irradiated cornea allograft had a low exposure rate and was well tolerated. The graft can be stored long term at room temperature and has an excellent postoperative cosmetic appearance.
Introduction
Tube shunts have been widely used in the treatment of eyes with complicated glaucoma.Citation1 Although tube shunts were introduced primarily for refractory cases, recently they are increasingly used as a primary surgical procedure.Citation2
Tube shunt surgery is associated with complications including tube or plate exposure, tube migration, and infection.Citation3 Tube-related exposure, which is a significant risk factor for the development of postoperative endophthalmitis, requires prompt surgical intervention.Citation4 Numerous materials including pericardium,Citation5 human sclera,Citation6 dura,Citation7 fascia lata,Citation8 porcine intestinal submucosa,Citation9 and amniotic membraneCitation10 have been used to decrease the exposure rates of tube shunt surgeries. Each material has its own advantages and disadvantages regarding success rates, storage conditions, availability, patient comfort, and cosmetic appearance.
Recently, several types of processed donor cornea tissue have been used in primary coverage of tube shunts, repair of exposed implant, and repair of filtering bleb leaks.Citation11–Citation14 Gamma irradiation is an effective method for the sterilization of donor tissues. By avoiding the risk of bacterial, fungal, and virus transmission it offers more safety when compared to fresh corneas.Citation15 In recent pilot studies, gamma-irradiated sterile cornea allograft has been reported effective and safe as a coverage material for glaucoma tube shunt surgery in a limited number of patients.Citation16,Citation17
In this study, we report our outcomes of using gamma-irradiated cornea allograft as a coverage material for glaucoma tube shunt surgeries. To the best of our knowledge, this current study is the largest study to date reporting the outcomes of tube shunt coverage using this patch graft.
Patients and methods
After the approval by the Institutional Review Board at the Wills Eye Hospital, a retrospective chart review was performed. All research methods were in compliance with the Declaration of Helsinki.
A total of 185 eyes underwent a primary or secondary tube shunt surgery using sterile gamma-irradiated cornea allograft (VisionGraft, Tissue Banks International Inc., Baltimore, MD, USA) between December 2012 and November 2013. Charts were included from 169 eyes of 165 patients who had complete information and follow-up data for at least 1 month. Preoperative data collected included age, sex, race, and type of glaucoma. Intraoperative data collected included type of tube, tube position, and type of surgery. Complications were recorded at 1 day; 1 week; 1, 3, 6, and 12 months; and final postoperative visit. Primary outcome was the ability of the allograft to remain stable and biocompatible post-operatively. Stability and biocompatibility were measured clinically by the integrity of the overlying conjunctiva and the allograft itself, signs of inflammation, and the need for surgical revision.
Sterile gamma-irradiated cornea allograft is obtained from a medically qualified donor. This procedure is committed to tissue safety and maintains compliance with appropriate and required regulatory agencies including the Eye Bank Association of America, the American Association of Tissue Banks, and the US Food and Drug Administration.Citation18 The allografts are sterilized using gamma radiation. The allograft is stored at room temperature for up to 18 months in a box containing a vial of sterile 5 mL 25% human albumin.
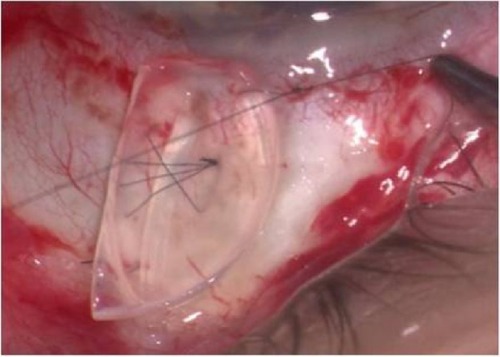
For this study we used 9 mm split-thickness half-moon cornea allograft (Catalog number: CO300AL-90) (). During the surgery, the allograft was transported to the surgical table, removed from the sterile vial and rinsed with balanced salt solution before use. All allografts were implanted over the tube, under the conjunctiva and sutured to the sclera with several 10-0 nylon sutures ().
Figure 1 Gamma-irradiated cornea allograft.
Figure 2 Intraoperative view of the gamma-irradiated cornea allograft.
Results
A total of 169 eyes from 165 patients (71 male, 94 female) were included in this study. Mean age was 69.5±16.5 (ranging from 15 to 99) years. Patients’ demographic data are summarized in . Mean follow-up time was 4.8±3.5 (ranging from 1 to 16) months.
Table 1 Demographic characteristics of the patients reviewed in the study
Cornea allografts were used for primary (87.5%) and secondary (7.7%) surgeries as well as for the repair of exposure (4.7%). The majority of tube shunts were implanted in the superotemporal quadrant (72.7%). Thirty-three eyes (19.5%) had tube shunts in the inferior quadrants. Clinical characteristics are summarized in .
Table 2 Clinical characteristics of the surgeries performed
The vast majority of the allografts, 166/169 (98.2%), were stable during the follow-up period, with no evidence of immunological reaction, infection, or exposure. Three eyes (1.8%) experienced exposure of the graft or tube within the first 3 postoperative months and all these three patients had tubes superotemporally located. Two graft exposures occurred in the first postoperative month, and both cases had underlying diseases: chronic allergic conjunctivitis with history of eye rubbing and bullous pemphigoid. The third patient had tube erosion that was noticed during the third postoperative month. All three cases underwent tube revision surgery and were successfully repaired.
Discussion
Tube shunt surgery for glaucoma is gaining popularity and is being increasingly used as a primary glaucoma surgery.Citation2 Erosion of the conjunctiva overlying the tube shunt and tube exposure is a complication that significantly increases the risk of endophthalmitis.Citation4 Coverage of the tube shunt is necessary both during primary implantation and for the repair of an eroded tube to prevent further conjunctival erosion and erosion-related infection and inflammation. In this study, we reviewed the outcomes of using a sterile gamma-irradiated cornea allograft to cover tube shunts. We found that cornea allografts were safe, effective, biocompatible, and stable for both primary implantations and secondary repair surgeries.
Traditionally, tube shunts were covered with scleral patch grafts and conjunctival erosion or exposure was found in 2%–3% of cases.Citation19 Smith et al compared donor sclera, donor dura, and donor pericardium and none of the patch grafts used to cover tube shunts was superior to the others in preventing conjunctival erosion and exposure.Citation20 More recently, different materials, such as processed cornea, porcine intestinal submucosa, and amniotic membrane have been used to cover tube shunts. These materials are readily prepared and commercially available for this specific purpose. shows the rate of tube exposure for the different materials, ranging between 0%–16%.Citation9,Citation10,Citation12,Citation14,Citation16,Citation20–Citation23
Table 3 Rates of tube exposure for patch graft materials
Using corneal tissue as a patch graft to facilitate postoperative suture lysis was first described in 1996.Citation11 Others have described the use of glycerol preserved or cryoprotected and frozen corneal tissues as a patch graft.Citation12,Citation14 Cryopreserved corneal patch grafts were well tolerated after the repair of exposed implants.Citation12 A recently published study found the exposure rates of glycerol-preserved corneal patch grafts significantly lower than those seen with pericardium patch grafts.Citation14
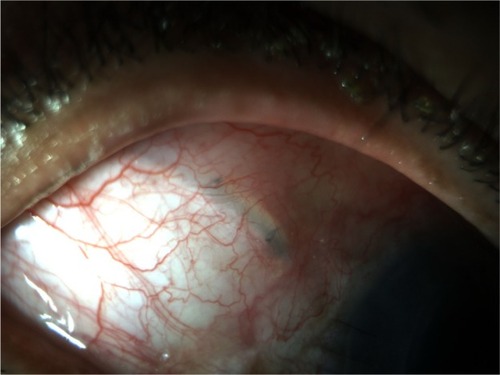
The use of gamma-irradiated cornea allograft has the advantages of decreased risk of disease transmission due to the sterilization process by gamma-irradiation, and shelf life of up to 2 years at room temperature. The graft material comes pre-cut in various shapes and does not require pre-surgical preparation.Citation17 It has been suggested that the dense lamellar structure of the corneal tissue offers high tensile strength, rigidity, and relatively more resistance to melting when compared with the loose structure of other tissues such as sclera or pericardium.Citation12,Citation16 The clarity of the graft () allows postoperative procedures such as suture lysis and provides excellent postoperative cosmetic appearance, especially with inferiorly placed implants.
Figure 3 Postoperative view (month 1) demonstrating excellent cosmetic appearance using the gamma-irradiated cornea allograft.
Two pilot studies found the gamma-irradiated cornea allograft to be effective and safe in tube shunt surgery with no exposures during the follow-up period.Citation16,Citation17 To the best of our knowledge, the current study is the largest study to date reporting the outcomes of tube shunt coverage using this patch graft. We found an exposure rate of 2% (three out of 169 eyes).
There are several studies in the literature identifying the risk factors for tube erosions. Prior or concomitant surgeries were found to induce conjunctival scarring and thinning leading to erosion.Citation23–Citation26 Additionally, diabetes, African–American or Hispanic ethnicity, neovascular glaucoma, previous glaucoma laser procedures, smoking and history of dry eye were also associated with erosions.Citation23,Citation25,Citation26
Patch graft melting and exposure may be related to several mechanisms: high grade immune mediated process with resultant rapid melting, mechanical processes and a low grade immune-mediated long-term atrophy.Citation20 Lankaranian et al postulated that the frequent rubbing combined with mechanical actions of the upper lid may also lead to tube erosions.Citation22 In this current study, two of the three patients who experienced tube erosions had an underlying cause: one had bullous pemphigoid and the other had chronic allergic conjunctivitis with a history of chronic eye rubbing. Bullous pemphigoid is a common autoimmune subepidermal blistering disease characterized by poor wound healing and chronic inflammation.Citation27,Citation28 Chronic allergic conjunctivitis is directly linked with increased tendency for inflammation, and it was suggested that prematurely loosened sutures following keratoplasty was associated with this condition.Citation29 Moreover, eye rubbing secondary to allergic conjunctivitis may cause mechanical insult to the patch graft and contribute to the exposure as well.
The cost of the gamma-irradiated corneal allograft in our surgical center is approximately 10% higher compared with Tutoplast pericardium, Tutoplast dura, and porcine small intestinal patch grafts. When taking into consideration the total costs of the surgery, using gamma-irradiated cornea allograft increases the cost of the surgery by approximately 1% compared with other commercially available materials.
The primary weaknesses of our study is its retrospective, non-comparative nature and our short-term follow-up period. A larger prospective comparative study is needed to fully investigate the rate of exposures with this patch graft compared to other materials.
In conclusion, the gamma-irradiated cornea allograft was well tolerated in nearly all of our patients. There was no clinical evidence of graft-related infection and inflammation in any of the eyes. The gamma-irradiated cornea allograft is readily available, offers sterility advantages, as well as improved cosmesis due to its transparency. Gamma-irradiated cornea allograft may be an alternative coverage graft material for glaucoma tube shunt surgeries.
Disclosure
The authors have no conflicts of interest to disclose.
References
- GeddeSJParrishRK2ndBudenzDLHeuerDKUpdate on aqueous shuntsExp Eye Res201193328429021443872
- MosaedSUpdate on aqueous shunts in glaucomaInt Ophthalmol Clin201151315516421633245
- NguyenQHAvoiding and managing complications of glaucoma drainage implantsCurr Opin Ophthalmol200415214715015021228
- Al-TorbakAAAl-ShahwanSAl-JadaanIAl-HommadiAEdwardDPEndophthalmitis associated with the Ahmed glaucoma valve implantBr J Ophthalmol200589445445815774923
- LamaPJFechtnerRDTube erosion following insertion of a glaucoma drainage device with a pericardial patch graftArch Ophthalmol199911791243124410496400
- ZeppaLRomanoMRCapassoLTortoriAMajoranaMACostagliolaCSutureless human sclera donor patch graft for Ahmed glaucoma valveEur J Ophthalmol201020354655120037905
- BrandtJDPatch grafts of dehydrated cadaveric dura mater for tube-shunt glaucoma surgeryArch Ophthalmol199311110143614398216025
- Gutierrez-DiazEMontero-RodriguezMMencia-GutierrezECabelloAMonescilloJLong-term persistence of fascia lata patch graft in glaucoma drainage device surgeryEur J Ophthalmol200515341241415945014
- NagiKSCumbaRJBellNPShort-Term Outcomes of KeraSys Patch Graft for Glaucoma Drainage Devices: A Case SeriesJ Ophthalmol2013201378470923577238
- AnandAShehaHTengCCLiebmannJMRitchRTelloCUse of amniotic membrane graft in glaucoma shunt surgeryOphthalmic Surg Lasers Imaging201142318418921563743
- RojanapongpunPRitchRClear corneal graft overlying the seton tube to facilitate laser suture lysisAm J Ophthalmol199612234244258794716
- SinghMChewPTTanDCorneal patch graft repair of exposed glaucoma drainage implantsCornea200827101171117319034134
- MistlbergerABiowskiRGrabnerGRepair of a late-onset filtering bleb leak using a corneal graft shaped with an excimer laserOphthalmic Surg Lasers200132542843111563789
- WigtonEC SwannerJJoinerWOutcomes of Shunt Tube Coverage With Glycerol Preserved Cornea Versus PericardiumJ Glaucoma201423425826122955016
- MiekkaSIForngRYRohwerRGInactivation of viral and prion pathogens by gamma-irradiation under conditions that maintain the integrity of human albuminVox Sang2003841364412542732
- LawrenceSDNetlandPAGamma-irradiated cornea allograft for glaucoma surgeryJ Glaucoma201322535535723429612
- DaoudYJSmithRSmithTAkpekEKWardDEStarkWJThe intraoperative impression and postoperative outcomes of gamma-irradiated corneas in corneal and glaucoma patch surgeryCornea201130121387139121993467
- Tissue Banks International [homepage on the Internet]Accreditation and Licensure Available from: http://www.tbionline.org/accreditation-licensure.phpAccessed 3 April, 2014
- StewartWCKristoffersenCJDemosCMFsadniMGStewartJAIncidence of conjunctival exposure following drainage device implantation in patients with glaucomaEur J Ophthalmol201020112413019927268
- SmithMFDoyleJWTicrneyJWJrA comparison of glaucoma drainage implant tube coverageJ Glaucoma200211214314711912362
- RavivTGreenfieldDSLiebmannJMSidotiPAIshikawaHRitchRPericardial patch grafts in glaucoma implant surgeryJ Glaucoma19987127329493112
- LankaranianDReisRHendererJDChoeSMosterMRComparison of single thickness and double thickness processed pericardium patch graft in glaucoma drainage device surgery: a single surgeon comparison of outcomeJ Glaucoma2008171485118303385
- TrubnikVZangalliCMosterMREvaluation of Risk Factors for Glaucoma Drainage Device-related Erosions: A Retrospective Case-Control StudyJ Glaucoma20131210
- ByunYSLeeNYParkCKRisk factors of implant exposure outside the conjunctiva after Ahmed glaucoma valve implantationJpn J Ophthalmol200953211411919333694
- HuddlestonSMFeldmanRMBudenzDLAqueous shunt exposure: a retrospective review of repair outcomeJ Glaucoma201322643343821673598
- KovalMSEl SayyadFFBellNPRisk factors for tube shunt exposure: a matched case-control studyJ Ophthalmol2013201319621523970955
- SadikCDSezinTKimNDLeukotrienes orchestrating allergic skin inflammationExp Dermatol2013221170570924433180
- Lo SchiavoARuoccoEBrancaccioGCaccavaleSRuoccoVWolfRBullous pemphigoid: etiology, pathogenesis, and inducing factors: facts and controversiesClin Dermatol201331439139923806156
- EgrilmezSSahinSYagciAThe effect of vernal keratoconjunctivitis on clinical outcomes of penetrating keratoplasty for keratoconusCan J Ophthalmol200439777277715696768