
Abstract
Purpose
Compare the lymphatic flow in the arm after breast cancer surgery and axillary lymph node dissection (ALND) versus sentinel lymph node biopsy (SLNB) using lymphos-cintigraphy (LS).
Patients and methods
A cross-sectional study with 39 women >18 years who underwent surgical treatment for unilateral breast cancer and manipulation of the axillary lymph node chain through either ALND or SLNB, with subsequent comparison of the lymphatic flow of the arm by LS. The variables analyzed were the area reached by the lymphatic flow in the upper limb and the sites and number of lymph nodes identified in the ALND or SLNB groups visualized in the three phases of LS acquisition (immediate dynamic and static images, delayed scan images). For all analyses, the level of significance was set at 5%.
Results
There was a significant difference between the ALND and SLNB groups, with predominant visualization of lymphatic flow and/or lymph nodes in the arm and axilla (P=0.01) and extra-axillary lymph nodes (P<0.01) in the ALND group. There was no significant difference in the total number of lymph nodes identified between the two groups. However, there was a significant difference in the distribution of lymph nodes in these groups. The cubital lymph node was more often visualized in the immediate dynamic images in the ALND group (P=0.004), while the axillary lymph nodes were more often identified in the delayed scan images of the SLNB group (P<0.01). The deltopectoral lymph node was only identified in the ALND group, but with no significant difference.
Conclusion
The lymphatic flow from the axilla was redirected to alternative extra-axillary routes in the ALND group.
Introduction
Breast cancer treatment has evolved over recent decades due to advances in techniques for early detection of the disease, with consequent decreases in the mortality rateCitation1,Citation2 and morbidity rate that result from less aggressive surgeries. The status of axillary lymph nodes determines whether the treatment should be more or less invasive, indicating either axillary lymph node dissection (ALND) or sentinel lymph node biopsy (SLNB),Citation3–Citation5 respectively. Surgical injuries resulting from ALND cause obstruction of the primary route of lymphatic drainage of the arm,Citation5,Citation6 leading to postoperative complications, such as hemorrhage, infection, seroma, axillary web syndrome, chronic pain, paraesthesia caused by intercostobrachial nerve damage, reduced range of motion and muscle weakness on the shoulder ipsilateral to the surgery, and, especially, lymphedema.Citation7,Citation8 More conservative intraoperative techniques to approach the axillary chain, such as SLNB have been used in an attempt to prevent lymphedema. Krag et alCitation9 and Giuliano et alCitation10 introduced innovative techniques that represent a new standard of axillary treatment for patients in the early stages of breast cancer, allowing a selective, safe, and less mutilating resection with satisfactory results and a significant reduction of surgical morbidities.Citation11,Citation12 However, this treatment is limited to patients with clinically negative axilla.Citation13,Citation14 The main goal of SLNB is to provide information about the stage and prognosis of the axillary chain to avoid unnecessary axillary lymphadenectomy, consequently decreasing morbidities in the upper limb ipsilateral to the axilla manipulated. Although this surgical technique has been improved, its use reduces but does not eliminate the risk of developing lymphedema,Citation15,Citation16 which has an incidence of 0%–13%.Citation6,Citation17,Citation18 Several factors can lead to this condition, such as the transection of lymphatic vessels of the arm during the SLNBCitation19,Citation20 and obesity.Citation20,Citation21 The increased incidence of lymphedema, especially associated with complementary radiotherapy,Citation22,Citation23 impacts the quality of life of these patients.Citation24
Once established, lymphedema is incurable. Studies have demonstrated that both surgical and drug therapies have failed in the cure of the disease.Citation25 However, lymphedema can be avoided, treated, and controlled through daily preventive measures.Citation26 Its diagnosis is difficult, especially in the early stages.Citation23 Without a correct early diagnosis, the treatment begins late and at more advanced stages of the disease. Immediate treatment leads to rapid improvement and prevents disease progression.Citation27 The lymphatic system is anatomically complex and difficult to image. For a long time, lymphatic imaging was limited to the use of conventional lymphography, which is an invasive procedure with a high incidence of discomfort and complications.Citation28
Lymphoscintigraphy (LS) has been used since 1950 to study diseases associated with the lymphatic system. Initially, it was used qualitatively to determine the relationship between edema of the extremities and lymphatic system disorders without any association with etiology. In the past three decades, the use of quantitative analysis was implemented.Citation29,Citation30 Numerous studies have demonstrated the reliability of the lymphatic flow studies, regardless of modes of investigation, radiotracers, and interpretation, as described by Akita et alCitation31 using indocyanine green fluorescence imaging for lower leg lymphedema investigation following lymph node dissection for gynecologic cancer.
In mastology, LS is widely used for SLNB. There are no data in the literature on the use of LS to evaluate the lymphatic drainage pathway of the upper limb after SLNB.
In agreement with the new guidelines for the use of more conservative surgical procedures, this study aimed to analyze changes in the lymphatic flow of the arm by LS after ALND versus SLNB performed for postoperative breast cancer.
Patients and methods
This prospective cross-sectional study selected 39 women >18 years who underwent surgical treatment for unilateral breast cancer and either ALND or SLNB as the axillary lymph node chain approach between 2005 and 2012. The lymphatic flow of the arm in the postoperative period was compared between the two lymphatic manipulation techniques. LS was performed up to 60 days after the surgery. An arm range of motion corresponding to >120° of shoulder flexion was also required for women who underwent ALND. The exclusion criteria were as follows: patients who underwent chemotherapy or radiotherapy before surgery, patients with knowledge of the lymphatic pathology before ALND and SLNB, and presence of inflammatory or infectious processes associated with arms. The Research Ethics Committee of Barretos Cancer Hospital approved this study, and all patients signed an informed consent form.
All lymphoscintigraphies were performed with a standardized acquisition technique according to the protocol developed by Sarri et alCitation29 using a dual-head gamma camera (GE Medical Systems Israel Ltd, Millennium VG Hawkeye, Tirat Hacarmel, Israel) equipped with a low-energy high-resolution collimator with a 20% window centered around the 140 keV photopeak and matrices of 128×128 for dynamic images, 256×256 for static images, and 256×1,024 for the whole-body scan (WBS), with no magnification. With patients in the supine position and arms raised above the head, 37 MBq of 99m Tc-phytate (Nuclear and Energetic Research Institute – IPEN, FITA-TEC fitato de sódio [99m Tc], São Paulo, Brazil) by volume of 0.5 mL was administered subcutaneously (fan technique) into the second interdigital spaceCitation29 of the manipulated limb using an insulin syringe. Dynamic images were obtained immediately after injection at a rate of 1 minute per image for 20 minutes for a field of view including the area from the hands to the axillae (Dynamic). Two static images with time of 500 seconds were acquired immediately after the end of the Dynamic: one was acquired in the same field of view as the Dynamic projection (Static 1), and the other was acquired in the anterior thoracic region and axillae projection (Static 2). With the patient in the same position, a WBS at a bed speed of 7 cm/minute started 90 minutes after injection of the radiotracer and included anterior and posterior projections. The patients attended the LS procedures wearing appropriate clothing that would not restrict the superficial lymphatic flow.
Qualitative analysis
The lymphoscintigraphies from the two groups were analyzed based on the area reached by the radiotracer in the lymphatic ducts of the upper limb and on the sites and number of lymph nodes visualized in the three phases of LS acquisition. A sequential ordinal classification was used for the area reached by the lymphatic fluid, from the injection site to the most distant point reached, using a 0–14 scale, respectively, with the number of lymph nodes visualized, as proposed by Sarri et alCitation29 and is shown in .
Figure 1 Lymphoscintigraphy including the area from the hand to the abdominal region.
Source: Reprinted with permission from Sarri AJ, Moriguchi SM, Dias R, et al. Physiotherapeutic stimulation: Early prevention of lymphedema following axillary lymph node dissection for breast cancer treatment. Exp Ther Med. 2010;1(1): 147–152.Citation29
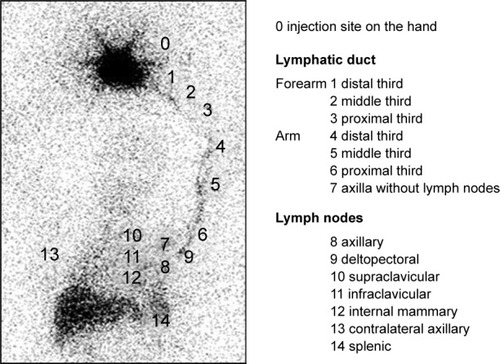
For statistical analysis, the points reached by the lymphatic fluid were grouped into the forearm (points 0–3), arm and axilla (points 4–9), and extra-axillary lymph nodes in the thoracic region (points 10–12). The images acquired in the three phases of the LS of women who underwent ALND and SLNB were paired and compared. Frequencies, percentages, and measures of central tendency and dispersion were used to characterize the sample. The Mann–Whitney U test was used to compare the number of lymph nodes visualized, age, and body mass index (BMI) between the ALND and SLNB groups () and descriptive analysis in . Fisher’s exact test was used to compare the qualitative variables (). For all analyses, the level of significance was set at 5%.
Table 1 Descriptive statistics of the sample ALND and SLNB groups
Table 2 Types of surgery in ALND and SLNB groups
Table 3 Sites reached by the lymphatic flow in the ALND and SLNB groups distributed over the dynamic, static, and WBS image stages and classified into forearm, arm/axilla, and thoracic extra-axillary lymph nodes
Results
The sample analyzed (n=39) consisted of two groups of patients: patients who underwent ALND (n=22) and patients who underwent SLNB (n=17). The mean age and BMI were similar between the groups, but there was a significant difference in the number of lymph nodes removed (P<0.01) and in the number of positive lymph nodes, evident only in the ALND samples, as shown in . The patients with positive sentinel lymph nodes were sequentially submitted to ALND and excluded from the study.
A total of 54.5% (n=12) of patients who underwent ALND and 35.3% (n=6) of patients who underwent SLNB had surgery on the right breast. Regarding the type of surgery, conservative and partial surgeries were predominant in the SLNB group, while in the ALND group, ~50% of the patients underwent radical mastectomies, as shown in . Only 23.5% (n=4) underwent immediate breast reconstruction, and these patients were from the SLNB group.
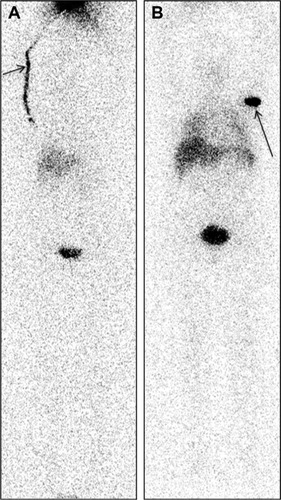
The lymph ducts were more evident in the early LS images, which were acquired within up to 40 minutes (Dynamic and Static 1, 2), with the arm and axilla being the most frequent sites reached by the lymphatic fluid in both groups analyzed (ALND × SLNB), with no significant difference. The delayed LS images at 90 minutes (WBS) identified significant differences between the ALND and SLNB groups, with predominant visualization of lymphatic flow and/or lymph nodes in the arm and axilla in the ALND group (P=0.01) () and of extra-axillary lymph nodes only in the ALND group (P<0.01), as shown in .
Figure 2 Difference in lymphatic progression between the (A) ALND and (B) SLNB groups. WBS of the ALND and SLNB groups.
Abbreviations: ALND, axillary lymph node dissection; SLNB, sentinel lymph node biopsy; WBS, whole-body scan.
There was no significant difference in the total number of lymph nodes identified between the ALND and SLNB groups. However, there was a significant difference in the distribution of lymph nodes in these groups. The cubital lymph node was more frequently visualized in the immediate Dynamic imaging in the ALND group (P=0.004), while the axillary lymph nodes were more frequently visualized in the delayed imaging (WBS) in the SLNB group (P<0.01) (). The deltopectoral lymph node was identified only in the ALND group (), but without a significant difference, as shown in .
Figure 3 WBS of the ALND group.
Abbreviations: ALND, axillary lymph node dissection; WBS, whole-body scan.
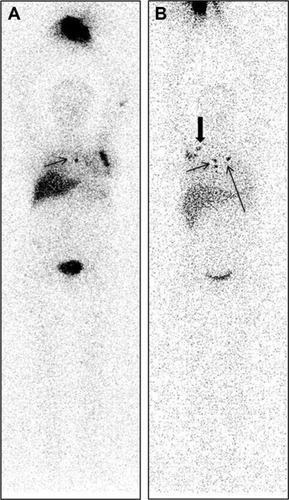
Figure 4 Lymphoscintigraphy. Different distributions of lymph nodes in the ALND and SLNB groups.
Abbreviations: ALND, axillary lymph node dissection; SLNB, sentinel lymph node biopsy; WBS, whole-body scan.
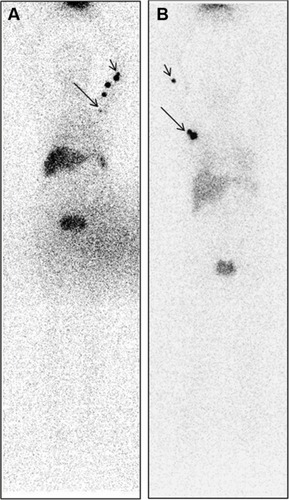
Table 4 Location of lymph nodes in the ALND and SLNB groups observed in the dynamic, static, and WBS imaging
Discussion
Currently, the implementation of modern surgical techniques for patients with breast cancer seeks to minimize the risk of treatment-associated morbidities, particularly lymphedema,Citation8,Citation32,Citation33 with a subsequent decline in ALND practice after positive SLNB for micrometastases or isolated tumor cells, suggesting that ALND is more prognostic than therapeutic.Citation34
Lymphedema develops when the rate of production of lymphatic fluid exceeds the capacity of lymph transport. It is characterized by lymphatic fluid accumulation in the interstitial space (edema), which often occurs in the extremities.Citation35,Citation36 Once established, lymphedema is incurable, and it is difficult to diagnose, especially in the early stages.Citation12 Without a correct diagnosis, treatment begins late and at a more advanced stage of the disease. Immediate treatment leads to rapid improvement and also prevents the progression of the disease to the chronic phase.Citation16,Citation23 The concern of patients regarding lymphedema development was reported by McLaughlin et alCitation34 who found that 50% of patients who underwent SLNB versus 75% of patients who underwent ALND were concerned about the development of this disease. Despite reports showing that the concerns of patients who underwent SLNB are unfounded due to the low risk of developing lymphedema, preventive measures should be taken because, although low, the risk exists. Several factors are attributed to the development of lymphedema after the SLNB and ALND procedures, such as the rupture of lymphatic vessels of the arm;Citation19,Citation20,Citation37 the fact that the sentinel lymph node draining to the breast and upper limb is the same and that its removal disrupts lymphatic drainage;Citation38 obesity;Citation20,Citation21 poor surgical techniques;Citation39 low educational level; advanced stage of disease; infections; number of lymph nodes involved; associated comorbidities; trauma; time after surgery;Citation36 anatomical peculiarities of the lymphatic system, which vary among patients;Citation35 and combination with adjuvant radiotherapy.Citation40,Citation41
Nuclear medicine technology plays an important role in evaluating the pattern of lymphatic drainage.Citation42,Citation43 The lymphatic system is complex, and its imaging remains a challenge. First, the lymphatic system is not an organ but connects different structures of small lymphatic capillaries to main ducts through lymph nodes and valves. Each of these structures can be visualized separately in images. Second, the lymphatic system can comprise a variety of diseases, including neoplasias and infectious diseases.Citation16,Citation18,Citation44 Studies using LS to evaluate the lymphatic circulation of the arm immediately after surgical treatment in patients with breast cancer (ALND and SLNB) were not found in the literature, so comparisons with this study could not be performed. This study was able to evaluate the lymphatic route in the early and delayed phases of scintigraphy in both groups. The delayed LS images (WBS) were more significant in identifying the differences in the lymphatic alterations between the ALND and SLNB groups. It is possible that a larger sample might generate a significant difference.
Using LS, Celebioglu et alCitation35 qualitatively and quantitatively compared the operated and nonoperated upper limbs of patients who underwent ALND and SLNB, where the second examination was 2–3 years after surgery and radiotherapy. The authors found a difference in the ALND group, where patients had dermal backflow and decreased accumulation of radiotracer in the axilla, while there was no difference in the SLNB group. In this study, dermal backflow was not visualized in any patient, most likely due to the short interval between the surgery and the LS. An attempt to maintain the lymphatic flow through alternative routes was identified. Additionally, more axillary lymph nodes were observed in the SLNB group, obviously due to the preservation of the axilla in this group. In contrast, a greater number of extra-axillary lymph nodes, especially in the cubital and deltoid regions, were observed in the ALND group. This finding is most likely due to damage to the normal lymphatic circulation, with flow redirected to alternative routes of deeper lymphatic chains, confirming the study conducted by Sarri et alCitation29 comparing lymphatic drainage before and after ALND. These findings show an attempt to maintain the lymphatic flow of the upper limb after more aggressive surgeries. Lymphoscintigraphies performed at longer intervals after surgery (a minimum of 6 months after) may clarify the impact of these findings. Further studies should be conducted at such intervals to try to better elucidate these points.
Conclusion
In conclusion, the data from this study showed lymphatic damage, with the lymphatic flow from the axilla being redirected to alternative routes in the ALND group in early postoperative breast surgery.
Acknowledgments
The authors thank the Teaching and Research Institute of Barretos Cancer Hospital, Brazil, and all patients who gave their consents to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
- CidonEUPereaCLopez-LaraFLife after breast cancer: dealing with lymphoedemaClin Med Insights Oncol2011591421339859
- HashimDBoffettaPLa VecchiaCThe global decrease in cancer mortality: trends and disparitiesAnn Oncol201627592693326802157
- NoguchiMAxillary reverse mapping for breast cancerBreast Cancer Res Treat2010119352953519842033
- YildizRUrkanMHancerliogullariOComparison of five different popular scoring systems to predict nonsentinel lymph node status in patients with metastatic sentinel lymph nodes: a tertiary care center experienceSpringerplus2015465126543785
- Maaskant-BraatAJde BruijnSZWoensdregtKPijpersHVoogdACNieuwenhuijzenGALymphatic mapping after previous breast surgeryBreast201221444444822104251
- RebegeaLFirescuDDumitruMAnghelRThe incidence and risk factors for occurrence of arm lymphedema after treatment of breast cancerChirurgia (Bucur)20151101333725800313
- AertsPDDe VriesJVan der SteegAFRoukemaJAThe relationship between morbidity after axillary surgery and long-term quality of life in breast cancer patients: the role of anxietyEur J Surg Oncol201137434434921296542
- ChoYDoJJungSKwonOJeonJYEffects of a physical therapy program combined with manual lymphatic drainage on shoulder function, quality of life, lymphedema incidence, and pain in breast cancer patients with axillary web syndrome following axillary dissectionSupport Care Cancer20162452047205726542271
- KragDNWeaverDLAlexJCFairbankJTSurgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probeSurg Oncol199326335339 discussion 3408130940
- GiulianoAEKirganDMGuentherJMMortonDLLymphatic mapping and sentinel lymphadenectomy for breast cancerAnn Surg19942203391398 discussion 398–401.8092905
- MorrowMProgress in the surgical management of breast cancer: Present and futureBreast201524Suppl 2S2S526249120
- PesceCMorrowMThe need for lymph node dissection in nonmetastatic breast cancerAnnu Rev Med20136411912923020881
- RaoRThe evolution of axillary staging in breast cancerMo Med2015112538538826606821
- RubioITSentinel lymph node biopsy after neoadjuvant treatment in breast cancer: Work in progressEur J Surg Oncol201642332633226774943
- AhmedMRubioITKovacsTKlimbergVSDouekMSystematic review of axillary reverse mapping in breast cancerBr J Surg2016103317017826661686
- SzubaAShinWSStraussHWRocksonSThe third circulation: radionuclide lymphoscintigraphy in the evaluation of lymphedemaJ Nucl Med2003441435712515876
- BourgeoisPLeducOLeducAImaging techniques in the management and prevention of posttherapeutic upper limb edemasCancer19988312 Suppl American280528139874402
- EllisSStructure and function of the lymphatic system: an overviewBr J Community Nurs2006114S4S616739286
- De GournayEGuyomardACoutantCImpact of sentinel node biopsy on long-term quality of life in breast cancer patientsBr J Cancer2013109112783279124169352
- HelyerLKVarnicMLeLWLeongWMcCreadyDObesity is a risk factor for developing postoperative lymphedema in breast cancer patientsBreast J2010161485419889169
- MehraraBJGreeneAKLymphedema and obesity: is there a link?Plast Reconstr Surg20141341154e160e
- EzzoJManheimerEMcNeelyMLManual lymphatic drainage for lymphedema following breast cancer treatmentCochrane Database Syst Rev20155CD003475
- LahtinenTSeppalaJVirenTJohanssonKExperimental and analytical comparisons of tissue dielectric constant (TDC) and bioimpedance spectroscopy (BIS) in assessment of early arm lymphedema in breast cancer patients after axillary surgery and radiotherapyLymphat Res Biol201513317618526305554
- KibarSDalyan ArasMUnsal DelialiogluSThe risk factors and prevalence of upper extremity impairments and an analysis of effects of lymphoedema and other impairments on the quality of life of breast cancer patientsEur J Cancer Care (Engl) Epub2016113
- BulleyCGaalSCouttsFComparison of breast cancer-related lymphedema (upper limb swelling) prevalence estimated using objective and subjective criteria and relationship with quality of lifeBiomed Res Int2013201380756923853774
- StuiverMMten TusscherMRAgasi-IdenburgCSConservative interventions for preventing clinically detectable upper-limb lymphoedema in patients who are at risk of developing lymphoedema after breast cancer therapyCochrane Database Syst Rev20152CD009765
- RidnerSHDietrichMSKiddNBreast cancer treatment-related lymphedema self-care: education, practices, symptoms, and quality of lifeSupport Care Cancer201119563163720393753
- MunnLLPaderaTPImaging the lymphatic systemMicrovasc Res201496556324956510
- SarriAJMoriguchiSMDiasRPhysiotherapeutic stimulation: Early prevention of lymphedema following axillary lymph node dissection for breast cancer treatmentExp Ther Med20101114715223136607
- YamamotoTMatsudaNDoiKThe earliest finding of indocyanine green lymphography in asymptomatic limbs of lower extremity lymphedema patients secondary to cancer treatment: the modified dermal backflow stage and concept of subclinical lymphedemaPlast Reconstr Surg20111284314e321e
- AkitaSMitsukawaNRikihisaNEarly diagnosis and risk factors for lymphedema following lymph node dissection for gynecologic cancerPlast Reconstr Surg2013131228329023357989
- KootstraJJHoekstra-WeebersJERietmanJSA longitudinal comparison of arm morbidity in stage I–II breast cancer patients treated with sentinel lymph node biopsy, sentinel lymph node biopsy followed by completion lymph node dissection, or axillary lymph node dissectionAnn Surg Oncol20101792384239420221902
- NoguchiMAxillary reverse mapping for preventing lymphedema in axillary lymph node dissection and/or sentinel lymph node biopsyBreast Cancer201017315515719789947
- McLaughlinSABagariaSGibsonTTrends in risk reduction practices for the prevention of lymphedema in the first 12 months after breast cancer surgeryJ Am Coll Surg20132163380389 quiz 511–51323266421
- CelebiogluFPerbeckLFrisellJGrondalESvenssonLDanielssonRLymph drainage studied by lymphoscintigraphy in the arms after sentinel node biopsy compared with axillary lymph node dissection following conservative breast cancer surgeryActa Radiol200748548849517520423
- ShahparHAtiehAMaryamARisk factors of lymph edema in breast cancer patientsInt J Breast Cancer2013201364181823862068
- NoguchiMYokoiMNakanoYAxillary reverse mapping with indo-cyanine fluorescence imaging in patients with breast cancerJ Surg Oncol2010101321722120063370
- BrittonTBSolankiCKPinderSEMortimerPSPetersAMPurushothamADLymphatic drainage pathways of the breast and the upper limbNucl Med Commun200930642743019319006
- UnsalMGDuralACCelikMFThe adaptation process of a teaching and research hospital to changing trends in modern breast surgeryUlus Cerrahi Derg2015311343825931942
- ChevilleALBrinkmannDHWardSBThe addition of SPECT/CT lymphoscintigraphy to breast cancer radiation planning spares lymph nodes critical for arm drainageInt J Radiat Oncol Biol Phys201385497197723452455
- DonkerMSlaetsLvan TienhovenGRutgersEJOkselklierdissectie versus okselbestraling bij borstkankerpatiënten met een positieve schildwachtklier. [Axillary lymph node dissection versus axillary radiotherapy in patients with a positive sentinel node: the AMAROS trial]Ned Tijdschr Geneeskd2015159A9302 Dutch26488192
- GiammarileFAlazrakiNAarsvoldJNThe EANM and SNMMI practice guideline for lymphoscintigraphy and sentinel node localization in breast cancerEur J Nucl Med Mol Imaging201340121932194724085499
- UrenRFLymphatic drainage of the skinAnn Surg Oncol2004113 Suppl179S185S15023748
- ChoiILeeSHongYKThe new era of the lymphatic system: no longer secondary to the blood vascular systemCold Spring Harb Perspect Med201224a00644522474611