
Abstract
Background
Accurate and useful predictors of gastric carcinoma treated with neoadjuvant chemotherapy are lacking at present. We aim to explore the potential prognostic significance of the neutrophil-to-lymphocyte ratio (NLR) in advanced gastric cancer receiving S-1 plus oxaliplatin (SOX) or oxaliplatin and capecitabine (XELOX) regimen.
Methods
We enrolled 91 patients with advanced gastric cancer treated with neoadjuvant chemotherapy from August 2008 to September 2015. The peripheral venous blood samples were collected before neoadjuvant chemotherapy. The NLR was divided into two groups: low NLR <2.17 group and high NLR ≥2.17 group. Univariate analysis on disease-free survival (DFS) and overall survival (OS) were generated using the Kaplan–Meier method and compared using the log-rank test. Prognostic factors were assessed by univariate analyses, and the independent prognostic factors were evaluated using multivariate analysis (Cox’s proportional-hazards regression model).
Results
The univariate analysis showed that median DFS and median OS were worse for high NLR values than low NLR values before neoadjuvant chemotherapy (median DFS: 19.97 and 26.87 months, respectively, P=0.299; median OS: 25.83 and 29.73 months, respectively, P=0.405). Multivariate analysis showed that the NLR before neoadjuvant chemotherapy was not an independent prognostic factor for DFS and OS. However, median DFS and median OS were worse for high neutrophil values than for low neutrophil values (median DFS: 21.03 and 26.87 months, respectively, P=0.396; median OS: 24.43 and 29.37 months, respectively, P=0.534); for low lymphocyte values than for high lymphocyte values before neoadjuvant chemotherapy (median DFS: 22.33 and 26.87 months, respectively, P=0.624; median OS: 26.37 and 27.93 months, respectively, P=0.584). Nevertheless, patients with low NLR had better 1-year, 3-year, and 5-year DFS and OS rates.
Conclusion
NLR may serve as a cheap and convenient prognostic indicator in gastric carcinoma patients receiving SOX or XELOX neoadjuvant chemotherapy. Low NLR may help the doctors to take efficient treatment measures for gastric cancer.
Introduction
Gastric carcinoma is one of the most malignant tumors, severely influencing the physical and mental health of people, and the second leading major cause of cancer-related mortality worldwide.Citation1,Citation2 The latest publication data from the World Health Organization (WHO) and International Arctic Research Center (IARC) indicate that the incidence of gastric cancer is 952,000 worldwide and 405,000 in China, accounting for 42.6% of the global incidence.Citation3 In China, most of the patients are diagnosed in advanced stages of gastric carcinoma, ~10% patients are at the early stage of gastric cancer, and the 5-year survival rate is 10%–30%.Citation4 Gastric resection with D2 lymph node dissection is the mainstay of treatment in advanced gastric carcinoma. Many randomized trials have indicated that adjuvant chemoradiotherapy has been a part of the combined modality therapy of advanced gastric cancer.Citation5–Citation7 Therefore, it is of significance to explore actively the potential prognostic factor in gastric cancer.
Neoadjuvant chemotherapy has, for several decades, been proven to benefit patients with advanced gastric cancer. It has been reported that neoadjuvant chemotherapy may decrease the tumor staging and volume, increase the R0 resection rate without increasing surgical morbidity and mortality compared with those undergoing surgical treatment alone.Citation8 Nevertheless, there is no internationally generally acknowledged standard neoadjuvant chemotherapy regimen for patients with advanced gastric carcinoma. For the past few years, novel chemotherapeutics have been emerging prominently. Although there are numerous neoadjuvant chemotherapy regimens for gastric cancer treatment, the S-1 plus oxaliplatin (SOX) and oxaliplatin and capecitabine (XELOX) regimens are the commonly used.Citation9,Citation10 In Asia, neoadjuvant chemotherapy regimen with SOX or XELOX delivered at R0 surgical resection with D2 lymph node dissection has shown remarkably improved survival for patients with locally advanced gastric carcinoma compared to those treated with surgery alone.Citation11 For the sake of improving the survival outcome and providing better treatment measures, it is important to find some accurate and sensitive tumor indicators.Citation12
Although there are some immunological and histological biomarkers that may influence the prognosis of patients with gastric carcinoma, these largely depend on the primary tumor specimens and are often time consuming and expensive; this limits their use in clinical practice.Citation13,Citation14 Tumor and inflammation are relationships dependent on each other.Citation15 Inflammation is an essential component of the tumor microenvironment, and the changes in inflammatory cells might influence tumor progression, such as neoplastic cell proliferation, migration, invasion, collapse of antitumor immunity, metastasis, and so forth.Citation16,Citation17 Tumor–inflammation interaction might represent a possible therapeutic target for cancer treatment. At the time of diagnosis and treatment, peripheral blood tests can reflect the tumor inflammatory conditions. The peripheral blood parameters, including white blood cell, neutrophil, lymphocyte, monocyte, and platelet counts, as well as the neutrophil-to-lymphocyte ratio (NLR), derived NLR (d-NLR), platelet-to-lymphocyte ratio (PLR), and monocyte-to-lymphocyte ratio (MLR), are the systemic inflammatory response indicators that have been widely proposed as prognostic factors for many malignancies.Citation18,Citation19
To our knowledge, the NLR has been previously identified as a useful predictive factor in gastric cancer.Citation20,Citation21 Nevertheless, the NLR is reported rarely in patients receiving neoadjuvant chemotherapy for advanced gastric carcinoma, especially the SOX or XELOX regimen.Citation22,Citation23 This study was aimed at evaluating the prognostic significance of NLR in patients with advanced gastric carcinoma receiving neoadjuvant chemotherapy such as SOX or XELOX regimen.
Materials and methods
The study was approved by the ethics committee of Harbin Medical University Cancer Hospital, Harbin Medical University, China, and complied with the standards of the Declaration of Helsinki. Prior to the research, written informed consent was obtained from all patients.
Patient selection
This retrospective analysis included data from 91 patients with stage II/III gastric carcinoma and treated with neoadjuvant chemotherapy in the Department of Gastrointestinal Surgery, Harbin Medical University Cancer Hospital, Harbin Medical University, between August 2008 and September 2015. All advanced gastric cancer cases were confirmed in accordance with pathological evidence, and the clinical stage was determined as II/III according to the tumor–node–metastasis (TNM) staging system.Citation24 The treatment regimens of patients with advanced gastric cancer were obtained from the patients’ history. The inclusion criteria included the following: 1) patients with locally advanced gastric cancer were confirmed in accordance with pathological evidence; 2) Eastern Cooperative Oncology Group (ECOG) performance status ≥2, Karnofsky performance status (KPS) ≥80; 3) patients with life expectancy ≥3 months; 4) no previous chemotherapy, radiotherapy, targeted therapy, and so forth. Exclusion criteria included the following: 1) patients with distant metastases; 2) patients with diabetes mellitus, hypertension, atherosclerotic heart diseases, and other acute or chronic diseases; 3) patients with serious complications, such as intestinal obstruction, active bleeding, enterobrosis, and obvious infections; 4) patients having received a blood product transfusion within 1 month before neoadjuvant chemotherapy.
Treatment protocols
SOX regimen: on the first day, oxaliplatin (130 mg/m2) was administered by intravenous infusion in 500 mL of 5% glucose over a period of 2 h. From the first day to the 14th day, S-1 (60 mg, twice daily [bid]) was administered as oral (per os [po]) XELOX regimen: on the first day, oxaliplatin (130 mg/m2) was administered by intravenous infusion in 500 mL of 5% glucose over a period of 2 h. From the first day to the 14th day, capecitabine (1,500 mg, bid) was administered by the po route. A cycle of the two regimens lasted for 3 weeks.
Response evaluation
Response rates were evaluated according to the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines.Citation25 The clinical response was divided into four groups: complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). The clinical objective response rate was defined as CR and PR, and nonclinical response was defined as SD or PD.
Peripheral venous blood sample
Peripheral venous blood samples were taken at the time of diagnosis before neoadjuvant chemotherapy. These samples were obtained from patients with empty stomach. Hematological parameters were analyzed by XE-2100 hematology analyzer (Sysmex, Kobe, Japan).
Follow-up
After surgery, all cases were followed regularly every 3–6 months for the first and second years, every 6–12 months from the third to the fifth years, then annually and until death. The patients were followed regularly every year thereafter with laboratory tests, multislice computed tomography (CT), and gastroscopy. Disease-free survival (DFS) was defined as the time from surgery to relapse (local recurrence and distant metastases). Overall survival (OS) was defined as the time from surgery to death by any cause or the last follow-up. The last follow-up date was December 3, 2016.
Statistical analysis
The optimal cutoff levels were decided using receiver operating characteristic (ROC) curve analyses. The areas under the curve (AUCs) were used to assess the predictive value. The categorical variables were described by frequencies and percentages (%) and then compared using the chi-square test or Fisher’s exact test. The continuous variables were described by the mean value ± standard error and were compared using the Student’s t-test. Survival curves were generated using the Kaplan–Meier and log-rank tests. Univariate analyses were used to assess the prognostic factors. Multivariate analysis (Cox’s proportional-hazards regression model) was used to evaluate independent prognostic factors. Hazard ratio (HR) and 95% confidence interval (95% CI) were used as common measures to assess relative risk. These analyses were performed using SPSS software (version 17.0, SPSS Inc, Chicago, IL, USA). Alpha was set at 0.05, and P<0.05 was found to be of statistical significance.
Results
Patient demographic and clinicopathological characteristics
The AUC of NLR was 0.570, and the optimal cutoff value by ROC was 2.17. The patients were categorized into two groups: low NLR <2.17 group and high NLR ≥2.17 group. shows the distribution of the demographic and clinicopathological characteristics of the 91 patients in the two groups divided according to the NLR. The males and females numbered 70 and 21, respectively; the median age was 57 years, with the range being 32–73 years; the median body mass index (BMI) was 22.32, and the range was 17.06–34.08. The number of patients with each of the ABO blood type (A, B, O, and AB) was 23, 32, 27, and 9, respectively. Moreover, 35 patients received the SOX regimen and 56 patients received the XELOX regimen. The radical resection cases (R0, R1, and R2) were 51, 21, and 19, respectively. All 91 patients underwent gastrectomy, 52 underwent distal gastrectomy, 6 underwent proximal gastrectomy, and 33 underwent total gastrectomy. The differentiation of tumors in these patients was as follows: 54 patients showed poorly differentiated, 32 patients moderately differentiated, and 5 patients well differentiated tumors. Tumors were located in the upper one-third (n=11), middle one-third (n=31), and the lower one-third (n=49) parts of the stomach, respectively. In terms of pathology, 64 patients had adenocarcinoma, 10 patients showed mucinous carcinoma, 12 patients had signet ring cell carcinoma, and 5 patients had other types. Of these patients, 54 were human epidermal growth factor receptor (HER)2 negative (0−+), and 37 were HER2-positive (++−+++). A median neutrophil count of 3.70 (range: 1.06–11.46), and a median lymphocyte count of 1.68 (range: 0.70–3.91). The overall response, CR, and PR were 76.9%, 5.5%, and 71.4%, respectively. A low baseline NLR (low NLR <2.17) correlated with improved demographic and clinicopathological characteristics, including age (χ2=3.963, P-value =0.046), gender (χ2=5.275, P-value =0.022), neutrophil count (χ2=26.381, P-value <0.001), and lymphocyte count (χ2=6.920, P-value =0.009).
Table 1 Demographic and clinicopathological characteristics of 91 patients with gastric cancer
Prognostic variables for DFS and OS
The median DFS was 23.73 months (range: 1.17–93.87 months), and the median OS was 26.87 months (range: 4.03–96.00 months) ( and ). The factors predicting high DFS were R0 resection, pathological N0 stage, pathological tumor in situ (Tis)/I stage. In multivariate Cox regression analysis, factors predicting improved DFS were R0 resection (P-value <0.001, HR: 3.084, 95% CI: 2.001–4.753), pathological N0 stage (P-value =0.002, HR: 4.289, 95% CI: 1.682–10.937), and pathological Tis/I stage (P-value <0.001, HR: 2.782, 95% CI: 1.829–4.233) (). Factors predicting high OS were R0 resection, pathological N0 stage, and pathological Tis/I stage. In multivariate Cox regression analysis, factors predicting high OS were R0 resection (P-value <0.001, HR: 2.494, 95% CI: 1.730–3.595), pathological N0 stage (P-value =0.002, HR: 4.263, 95% CI: 1.680–10.815), and pathological Tis/I stage (P-value <0.001, HR: 3.401, 95% CI: 1.949–4.746) ().
Figure 1 Disease-free survival of 91 patients with gastric cancer.
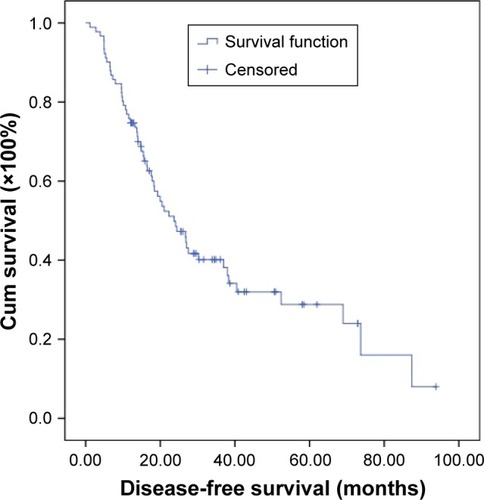
Figure 2 Overall survival of 91 patients with gastric cancer.
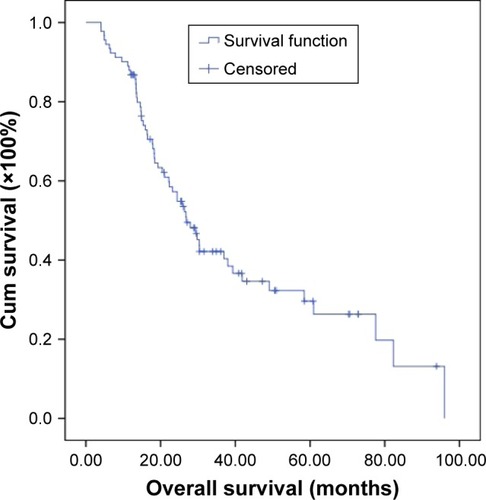
Table 2 Univariate and multivariate Cox regression analyses of disease-free survival in 91 patients with gastric cancer
Table 3 Univariate and multivariate Cox regression analyses of overall survival in 91 patients with gastric cancer
Meanwhile, we found that neutrophil count, lymphocyte count, and NLR before neoadjuvant chemotherapy had no statistical significance using the cutoff values of 3.70×109/L, 1.68×109/L, and 2.17 for DFS (P-value =0.510, 0.644, and 0.550, respectively) and OS (P-value =0.941, 0.621, and 0.625, respectively) in univariate analysis ( and ). However, median DFS and median OS were worse for high NLR values than for low NLR values before neoadjuvant chemotherapy ( and ). Nevertheless, median DFS and median OS were worse for high neutrophil values than for low neutrophil values ( and ) and for low lymphocyte values than for high lymphocyte values before neoadjuvant chemotherapy ( and ) ().
Figure 3 Disease-free survival in relation to NLR.
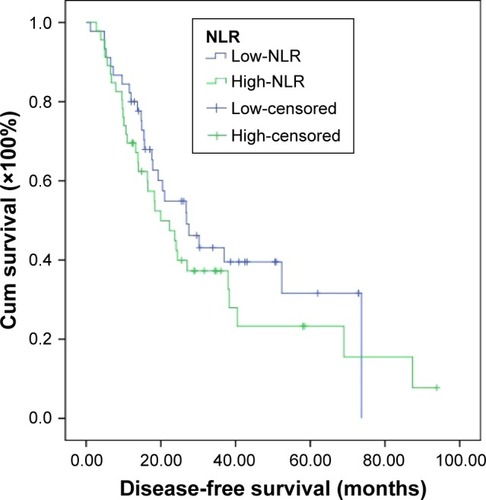
Figure 4 Overall survival in relation to NLR.
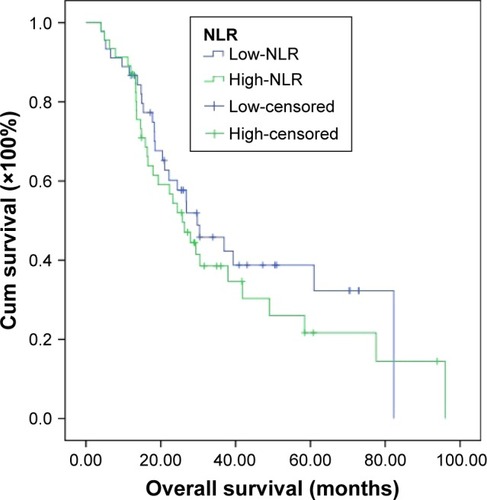
Figure 5 Disease-free survival in relation to neutrophil count.
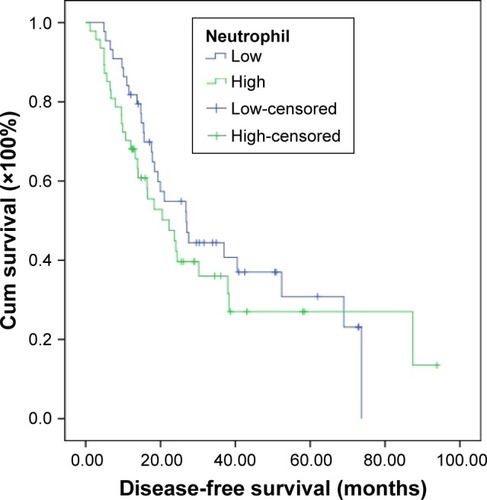
Figure 6 Overall survival in relation to neutrophil count.
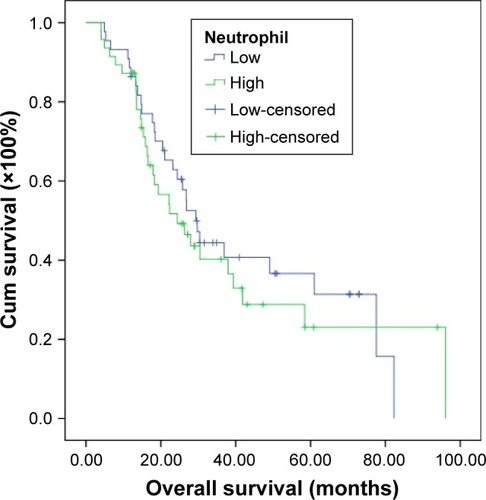
Figure 7 Disease-free survival in relation to lymphocyte count.
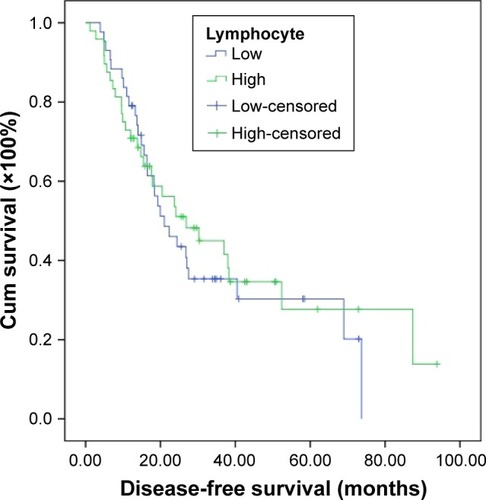
Figure 8 Overall survival in relation to lymphocyte count.
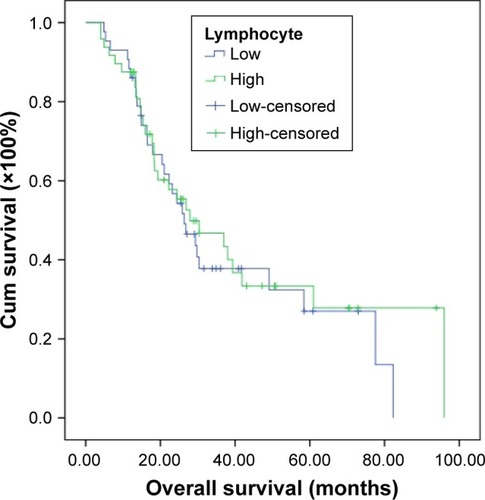
Table 4 Clinical and laboratory characteristics as well as disease-free survival and overall survival of the 91 patients with gastric cancer
and show the characteristics of the 91 patients before neoadjuvant chemotherapy: patients with low NLR and low neutrophil count had better median DFS and OS (median DFS: 26.87 and OS: 29.73 months, respectively) values; patients with low NLR and high lymphocyte count had better median DFS and OS values (median DFS: 36.93 and OS: 39.33 months, respectively).
Table 5 Clinical and laboratory characteristics as well as disease-free survival of the 91 patients with gastric cancer by NLR
Table 6 Clinical and laboratory characteristics as well as overall survival of the 91 patients with gastric cancer by NLR
Among the 91 patients with gastric cancer, the 1-year, 3-year, and 5-year DFS rates were 75.8%, 23.1%, and 7.7%; the 1-year, 3-year, and 5-year OS rates were 87.9%, 26.4%, and 11.0%, respectively. We also found that the patients with low NLR <2.17 had better 1-year, 3-year, and 5-year DFS and OS rates ().
Table 7 One-year, 3-year, and 5-year DFS and OS rates of the 91 patients with gastric cancer
The common hematologic toxicities after neoadjuvant chemotherapy of the 91 patients with gastric cancer were National Cancer Institute Common Toxicity Criteria (NCI-CTC) grades 1 and 2 anemia, leukopenia, neutropenia, and thrombocytopenia in 33/91 (36.3%), 18/91 (19.8%), 21/91 (23.1%), and 4/91 (4.4%), respectively ( and ). We found that NLR before neoadjuvant chemotherapy had no significance on toxicities of the 91 patients with gastric cancer using the cutoff value of 2.17 ( and ).
Table 8 Main toxicities according to NCI-CTC scale of the 91 patients with gastric cancer
Table 9 Main toxicities according to NCI-CTC scale of the 91 patients with gastric cancer
Discussion
Gastric carcinoma is one of the common types of malignant tumors worldwide. Although mortality and morbidity rates of gastric carcinoma have declined over the past several decades, the disease still has a poor prognosis and leads to hundreds of thousands of deaths annually.Citation26 Over the past 2 decades, multiple therapies, including radiotherapy, adjuvant chemotherapy, neoadjuvant chemotherapy, perioperative chemotherapy, and targeted therapy, have improved survival and quality of life for these gastric cancer patients.Citation27
Cancer and inflammation are closely connected and have implications for prevention and treatment. Inflammation contributes to tumor proliferation, migration, invasion, angiogenesis, and so forth.Citation28,Citation29 Various studies have suggested that a systemic inflammatory response is associated with a poor prognosis in many malignancies.Citation30–Citation35 Using the cellular components of a systemic inflammatory response in peripheral venous blood for predicting survival has received increased attention. Nevertheless, the mechanisms are still ambiguous and poorly understood. Clinical and epidemiological studies have shown the connection between gastric carcinoma and inflammation.Citation36 There is growing interest in a clinical interpretation of the relation between inflammation and tumor cells, resulting in the establishment of novel biomarkers of cancer to evaluate the prognostic significance. For selecting the optimal treatment regimen for individuals, accurate and useful predictors are needed. To our knowledge, the association of NLR values with DFS and OS in patients receiving neoadjuvant chemotherapy with SOX or XELOX regimen has been studied rarely.
We analyzed the relationship between NLR and clinicopathological characteristics in patients with advanced gastric carcinoma. We found that low NLR correlated with improved demographic and clinicopathological characteristics, including age, gender, neutrophil count, and lymphocyte count. In univariate and multivariate Cox regression analyses, factors predicting improved DFS and OS were R0 resection, pathological N0 stage, and pathological Tis/I stage. We also found that the neutrophil count, lymphocyte count, and NLR had no significance using the cutoff values of 3.70×109/L, 1.68×109/L, and 2.17 for DFS and OS in univariate analysis. However, median DFS and median OS were worse for high NLR values than for low NLR values before neoadjuvant chemotherapy (median DFS: 19.97 and 26.87 months; median OS: 25.83 and 29.73 months), and this is consistent with the results of other authors.Citation37–Citation39 At the same time, median DFS and median OS were worse for high neutrophil values than for low neutrophil values (median DFS: 21.03 and 26.87 months; median OS: 24.43 and 29.37 months), as well as for low lymphocyte values than for high lymphocyte values before neoadjuvant chemotherapy (median DFS: 22.33 and 26.87 months; median OS: 26.37 and 27.93 months).
Meanwhile, we found that the patients with low NLR and low neutrophil count had better median DFS and OS (median DFS: 26.87 and OS: 29.73 months); the patients with low NLR and high lymphocyte count had better median DFS and OS (median DFS: 36.93 and OS: 39.33 months). A study by Eo et alCitation40 suggested that low monocyte count and high lymphocyte count had better 5-year DFS and OS rates. We also found that the 1-year, 3-year, and 5-year DFS and OS rates in the low NLR group were higher than in the high NLR group. Although the NLR values before neoadjuvant chemotherapy lost their independent prognostic significance for DFS or OS, they still provided fundamental information for clinical practice. Jin et alCitation41 reported that NLR had statistical significance with PFS, but not with OS, in multivariate analysis. Another study by el AzizCitation38 suggested that NLR lost its independent prognostic significance for PFS, but had significance with OS, in multivariate analysis.
Various studies have indicated that elevated NLR is associated with poor survival in many tumors, and the association has not been clear.Citation42–Citation45 The tumor microenvironment inhabited by inflammatory cells is important in carcinogenesis, promoting cancer growth, invasion, tumor cell proliferation, and migration.Citation46 The neutrophils inhibit the immune system via restraining the cytolytic activity of immune cells and influence the tumor environment, thus probably contributing to stimulating tumor angiogenesis and progression.Citation47 The lymphocyte is known to play a significant role in defense of tumor cells by inducing cytotoxic cell death and suppressing tumor cell proliferation and migration.Citation48 Furthermore, patients with lymphocyte infiltration may have a better prognosis than those with no infiltration.Citation49 In the development of gastric cancer, chronic inflammation may be caused by Helicobacter pylori, and it may be a critical risk factor for gastric carcinoma.Citation50 The mechanism of NLR responses to tumors may be explained as decrease in the number of lymphocytes and increase in the number of neutrophils. Hence, the NLR, calculated based on both the neutrophil and the lymphocyte counts, may be a good marker reflecting the degree of tumor progression and predict prognosis.
To the best of our knowledge, the significance of NLR values’ association with DFS and OS in gastric carcinoma receiving neoadjuvant chemotherapy is reported rarely. This research suggests that the NLR may be used in the prediction of prognosis in advanced gastric carcinoma. It is crucial to take into consideration the high gastric cancer morbidity and unbalanced medical condition in China, and thus, these cheap, noninvasive, and convenient biomarkers may be beneficial with regard to the prevention and treatment of gastric cancer. Therefore, better understanding of hematologic parameters can help identify new targets for individual treatment. Thus, this study may provide important information for clinical practice.
In summary, SOX and XELOX regimens were well tolerated by all patients who received it. Our study explains the reason for the NLR enhancing tumor progression, and low NLR may be a more favorable prognostic factor. The differences in the cutoff values of NLR among these studies may be attributable to the differences in the cumulative number of patients and the disease stage among the studies. Whether the cutoff value of 2.17 for NLR used in our study is correct requires further investigation.
Conclusion
It is believed that the NLR may be a cheap and convenient prognostic indicator in gastric carcinoma patients receiving neoadjuvant chemotherapy. Low NLR may help doctors to take efficient treatment measures for gastric cancer. However, more studies are needed to assess changes in inflammatory markers in larger groups of patients with advanced gastric carcinoma.
Disclosure
The authors report no conflicts of interest in this work.
References
- SchuhmacherCReimDNovotnyANeoadjuvant treatment for gastric cancerJ Gastric Cancer2013132737823844320
- SiegelRLMillerKDJemalACancer Statistics, 2015CA Cancer J Clin201565152925559415
- TorreLABrayFSiegelRLFerlayJLortet-TieulentJJemalAGlobal cancer statistics, 2012CA Cancer J Clin20156528710825651787
- MackenzieMSpithoffKJonkerDSystemic therapy for advanced gastric cancer: a clinical practice guidelineCurr Oncol2011184e202e20921874111
- ManoharanVLeeSChongSSerial imaging using [18F] Fluorodeoxyglucose positron emission tomography and histopathologic assessment in predicting survival in a population of surgically resectable distal oesophageal and gastric adenocarcinoma following neoadjuvant therapyAnn Nucl Med201731431532328299585
- LiSLiBWangJIdentification of sensitivity predictors of neoadjuvant chemotherapy for the treatment of adenocarcinoma of gastroesophageal junctionOncol Res2017251939728081737
- Neves FilhoEHde Sant’AnaRONunesLVPiresAPda CunhaMDHistopathological regression of gastric adenocarcinoma after neoadjuvant therapy: a critical reviewAPMIS20171252798428044374
- ParkSCChunHJChemotherapy for advanced gastric cancer: review and update of current practicesGut Liver20137438539323898376
- WangXWangMLZhouLYLuXYYangJFYuHGRandomized phaseII study comparing paclitaxel with S-1 vs. S-1 as first-line treatment in patients with advanced gastric cancerClin Transl Oncol2013151083684223381898
- BangYJKimYWYangHKCLASSIC trial investigators. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): a phase 3 open-label, randomised controlled trialLancet2012379981331532122226517
- QuéroLGuillermSHennequinCNeoadjuvant or adjuvant therapy for gastric cancerWorld J Gastrointest Oncol20157810211026306142
- PangWLouNJinCCombination of preoperative platelet/lymphocyte and neutrophil/lymphocyte rates and tumor-related factors to predict lymph node metastasis in patients with gastric cancerEur J Gastroenterol Hepatol201628549350226854795
- KimKHKwonHCOhSYClinicopathological significance of ERCC1, thymidylate synthase and glutathione S-transferase P1 expression for advanced gastric cancer patients receiving adjuvant 5-Fu and cisplatin chemotherapyBiomarkers2011161748221133646
- ShiraiOOhmiyaNTaguchiAP53, P21 and P73 gene polymorphisms in gastric carcinomaHepatogastroenterology2010571041595160121443127
- ColottaFAllavenaPSicaAGarlandaCMantovaniACancer-related inflammation, the seventh hallmark of cancer: links to genetic instabilityCarcinogenesis20093071073108119468060
- GrivennikovSIGretenFRKarinMImmunity, inflammation, and cancerCell2010140688389920303878
- BalkwillFMantovaniAInflammation and cancer: back to Virchow?Lancet2001357925553954511229684
- BorsigLWolfMJRoblekMLorentzenAHeikenwalderMInflammatory chemokines and metastasis-tracing the accessoryOncogene201433253217322423851506
- FengFSunLZhengGLow lymphocyte-to-white blood cell ratio and high monocyte-to-white blood cell ratio predict poor prognosis in gastric cancerOncotarget2017835281529128029656
- LianLXiaYYZhouCApplication of platelet/lymphocyte and neutrophil/lymphocyte ratios in early diagnosis and prognostic prediction in patients with resectable gastric cancerCancer Biomark201515689990726444485
- WangSCChouJFStrongVEPretreatment neutrophil to lymphocyte ratio independently predicts disease-specific survival in resectable gastroesophageal junction and gastric adenocarcinomaAnn Surg2016263229229725915915
- KunisakiCTakahashiMOnoHAInflammation-based prognostic score predicts survival in patients with advanced gastric cancer receiving biweekly docetaxel and S-1 combination chemotherapyOncology201283418319122890015
- GohBKChokAYAllenJCJrBlood neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios are independent prognostic factors for surgically resected gastrointestinal stromal tumorsSurgery201615941146115626688506
- WashingtonK7th edition of the AJCC cancer staging manual: stomachAnn Surg Oncol201017123077307920882416
- EisenhauerEATherassePBogaertsJNew response evaluation criteria in solid tumours: revised RESIST guideline (version 1.1)Eur J Cancer200945222824719097774
- SiegelRNaishadhamDJemalACancer statistics, 2012CA Cancer J Clin2012621102922237781
- BrenkmanHJHaverkampLRuurdaJPvan HillegersbergRWorldwide practice in gastric cancer surgeryWorld J Gastroenterol201622154041404827099448
- DiakosCICharlesKAMcMillanDCClarkeSJCancer-related inflammation and treatment effectivenessLancet Oncol20141511e493e50325281468
- MantovaniAAllavenaPSicaABalkwillFCancer-related inflammationNature2008454720343644418650914
- KohCHBhoo-PathyNNgKLUtility of pre-treatment neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as prognostic factors in breast cancerBr J Cancer2015113115015826022929
- StotzMPichlerMAbsengerGThe preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancerBr J Cancer2014110243544024357796
- TanogluAKaragozEYiyitNBerberUIs combination of neutrophil to lymphocyte ratio and platelet lymphocyte ratio a useful predictor of postoperative survival in patients with esophageal squamous cell carcinoma?Onco Targets Ther2014743343424665204
- GuLMaXLiHPrognostic value of preoperative inflammatory response biomarkers in patients with sarcomatoid renal cell carcinoma and the establishment of a nomogramSci Rep20166238462385627035802
- XiaW-KLiuZ-LShenDLinQ-FSuJMaoW-DPrognostic performance of pre-treatment NLR and PLR in patients suffering from osteosarcomaWorld J Surg Oncol20161412713527125872
- BaganteFTranTBPostlewaitLMNeutrophil-lymphocyte and platelet-lymphocyte ratio as predictors of disease specific survival after resection of adrenocortical carcinomaJ Surg Oncol2015112216417226234285
- LochheadPEl-OmarEMGastric cancerBr Med Bull2008858710018267927
- KimJHHanDSBangHYKimPSLeeKYPreoperative neutrophil-to-lymphocyte ratio is a prognostic factor for overall survival in patients with gastric cancerAnn Surg Treat Res2015892818626236697
- el AzizLMBlood neutrophil–lymphocyte ratio predicts survival in locally advanced cancer stomach treated with neoadjuvant chemotherapy FOLFOX 4Med Oncol2014311231131625367855
- LeeSOhSYKimSHPrognostic significance of neutrophil lymphocyte ratio and platelet lymphocyte ratio in advanced gastric cancer patients treated with FOLFOX chemotherapyBMC Cancer20131335023876227
- EoWKJeongDWChangHJAbsolute monocyte and lymphocyte count prognostic score for patients with gastric cancerWorld J Gastroenterol20152192668267625759535
- JinHZhangGLiuXBlood neutrophil-lymphocyte ratio predicts survival for stages III-IV gastric cancer treated with neoadjuvant chemotherapyWorld J Surg Oncol20131111212223705622
- LeeSMRussellAHellawellGPredictive value of pretreatment inflammation-based prognostic scores (neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and lymphocyte-to-monocyte ratio) for invasive bladder carcinomaKorean J Urol2015561174975526568792
- JiangCHuWMLiaoFXElevated preoperative neutrophil-to-lymphocyte ratio is associated with poor prognosis in gastrointestinal stromal tumor patientsOnco Targets Ther2016987788326966375
- KimSHLeeHWGoSILeeSILeeGWClinical significance of the preoperative platelet count and platelet-to-lymphocyte ratio (PLT-PLR) in patients with surgically resected non-small cell lung cancerOncotarget2016724361983620627105529
- HoCLLuCSChenJHChenYGHuangTCWuYYNeutrophil/lymphocyte ratio, lymphocyte/monocyte ratio, and absolute lymphocyte count/absolute monocyte count prognostic score in diffuse large B-cell lymphoma: useful prognostic tools in the rituximab eraMedicine (Baltimore)20159424e99326091479
- ElinavENowarskiRThaissCAHuBJinCFlavellRAInflammation-induced cancer: crosstalk between tumours, immune cells and microorganismsNat Rev Cancer2013131175977124154716
- JungMRParkYKJeongOElevated preoperative neutrophil to lymphocyte ratio predicts poor survival following resection in late stage gastric cancerJ Surg Oncol2011104550451021618251
- MilneKAlexanderCWebbJRAbsolute lymphocyte count is associated with survival in ovarian cancer independent of tumor-infiltrating lymphocytesJ Transl Med2012103322369276
- KimJWNamKHAhnSHPrognostic implications of immunosuppressive protein expression in tumors as well as immune cell infiltration within the tumor microenvironment in gastric cancerGastric Cancer2016191425225424150
- MatsumotoYMarusawaHKinoshitaKHelicobacter pylori infection triggers aberrant expression of activation-induced cytidine deaminase in gastric epitheliumNat Med200713447047617401375