

Abstract
Background
Recent studies have showed that nonsteroidal anti-inflammatory drugs (NSAIDs) could reduce the risk of several types of cancer. However, epidemiological evidence of the association between NSAIDs intake and the risk of hepatocellular carcinoma (HCC) remains controversial.
Methods
To assess the preventive benefit of NSAIDs in HCC, we simultaneously searched the databases of PubMed, EmBase, Web of Science, and Scopus and screened eligible publications.
Results
A total of twelve articles (published from 2000 to 2017) from five countries were identified by retrieval. We observed a significantly lower risk of HCC incidence among users of NSAIDs than among those who did not use NSAIDs (pooled hazard ratio [HR] value =0.81, 95% confidence interval [CI]: 0.69–0.94). No evidence of publication bias was observed (Begg’s test, P=0.755; Egger’s test, P=0.564). However, when stratified according to the categories of NSAIDs, users of non-aspirin NSAIDs (HR =0.81, 95% CI: 0.70–0.94), but not aspirin (HR =0.77, 95% CI: 0.58–1.02), showed a statistically significant reduced HCC incidence. We also found that NSAIDs use significantly reduced the recurrent risk of HCC, with a HR value of 0.79 (95% CI: 0.75–0.84), whereas there was no statistically significant association between NSAIDs use and HCC mortality, with a HR value 0.65 (95% CI: 0.40–1.06).
Conclusion
Taken together, our meta-analysis demonstrates that NSAIDs significantly reduce the incident and recurrent risk of HCC.
Supplementary materials
Figure S1 Galbraith’s plot of studies that assessed the preventive effect of NSAIDs use in risk of HCC incidence.
Notes: *Aspirin; #non-aspirin NSAIDs; &all NSAIDs.
Abbreviations: HCC, hepatocellular carcinoma; NSAIDs, nonsteroidal anti-inflammatory drugs.
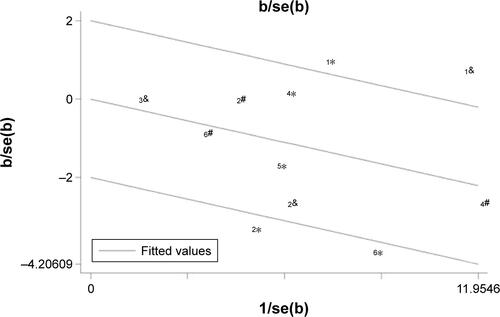
Figure S2 Forest plots of the meta-analysis on the association between NSAIDs and risk of HCC incidence after removal of the outliers of the heterogeneity.
Note: Weights are from random-effects analysis.
Abbreviations: HCC, hepatocellular carcinoma; NSAIDs, nonsteroidal anti-inflammatory drugs; HR, hazard ratio; CI, confidence interval.
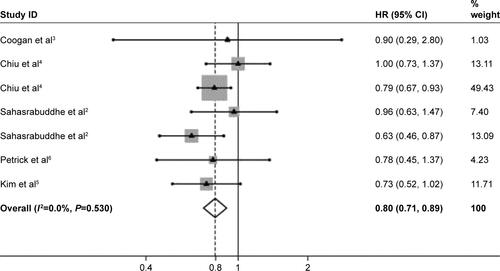
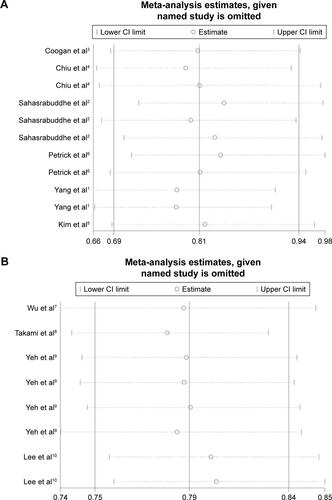
Figure S3 Influence analysis of studies that assessed the effects of NSAIDs use in the risk of HCC incidence (A) and recurrence (B).
Abbreviations: HCC, hepatocellular carcinoma; NSAIDs, nonsteroidal anti-inflammatory drugs; CI, confidence interval.
References
- YangBPetrickJLChenJAssociations of NSAID and paracetamol use with risk of primary liver cancer in the Clinical Practice Research DatalinkCancer Epidemiol20164310511127420633
- SahasrabuddheVVGunjaMZGraubardBINonsteroidal anti-inflammatory drug use, chronic liver disease, and hepatocellular carcinomaJ Natl Cancer Inst2012104231808181423197492
- CooganPFRosenbergLPalmerJRNonsteroidal anti-inflammatory drugs and risk of digestive cancers at sites other than the large bowelCancer Epidemiol Biomarkers Prev20009111912310667472
- ChiuHFHoSCChenCCYangCYStatin use and the risk of liver cancer: a population-based case-control studyAm J Gastroenterol2011106589489821157439
- KimGJangSYHanEEffect of statin on hepatocellular carcinoma in patients with type 2 diabetes: a nationwide nested case-control studyInt J Cancer2017140479880627861855
- PetrickJLSahasrabuddheVVChanATNSAID use and risk of hepatocellular carcinoma and intrahepatic cholangiocarcinoma: the liver cancer pooling projectCancer Prev Res (Phila)20158121156116226391917
- WuCYChenYJHoHJAssociation between nucleoside analogues and risk of hepatitis B virus-related hepatocellular carcinoma recurrence following liver resectionJAMA2012308181906191423162861
- TakamiYEguchiSTateishiMA randomised controlled trial of meloxicam, a Cox-2 inhibitor, to prevent hepatocellular carcinoma recurrence after initial curative treatmentHepatol Int201610579980626846471
- YehCCLinJTJengLBNonsteroidal anti-inflammatory drugs are associated with reduced risk of early hepatocellular carcinoma recur rence after curative liver resection: a nationwide cohort studyAnn Surg2015261352152624950265
- LeePCYehCMHuYWAntiplatelet therapy is associated with a better prognosis for patients with hepatitis B virus-related hepatocellular carcinoma after liver resectionAnn Surg Oncol201623Suppl 587488327541812
Acknowledgments
This work was supported by the National Natural Science Foundation of China (no 81600452).
Disclosure
The authors report no conflicts of interest in this work.