
Abstract
Occult breast cancer is defined by the presence of axillary metastases without an identifiable primary breast tumor. Here, we report a rare case of a male occult breast cancer with dermatomyositis. We performed a modified radical mastectomy consisting of whole breast mastectomy and axillary lymph node dissection. Immunohistochemistry and fluorescent in situ hybridization analyses demonstrated an adenocarcinoma likely of breast origin, which was an occult triple-negative breast cancer. Interestingly, the patient’s previously noted periorbital dermatomyositis resolved promptly following surgical excision.
Introduction
Occult breast cancer (OBC) is defined by the presence of axillary metastases without an identifiable breast tumor. It has been reported that most hormone receptor (HR)-positive rate of male breast cancer (MBC) is higher than that of female breast carcinomas. We encountered a unique case of OBC, the immunohistochemistry (IHC) and fluorescent in situ hybridization (FISH) studies of which was a triple-negative breast carcinoma (TNBC). Interestingly, the patient developed periorbital erythematous papules 3 months before diagnosis of MBC. This was suspected to be dermatomyositis (DM), which has not been reported in male OBC patients previously. The purpose of this study is to describe and discuss the diagnosis, the clinicopathologic characteristics, and treatment of this rare subtype of breast carcinoma.
Case report
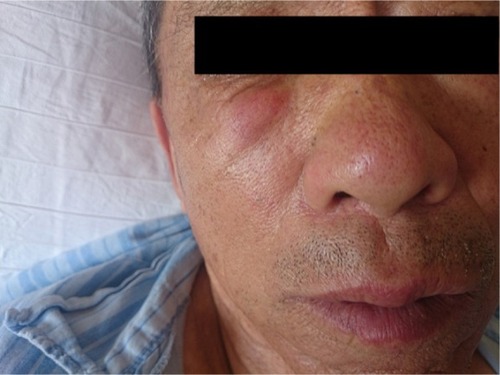
In May 2015, an 84-year-old male patient who denied any history of smoking or alcohol consumption, with no family history of breast cancer, discovered a palpable nodule in his right axilla. An ultrasound examination confirmed an irregular hypoechoic solid mass in the right axillary cavity measuring 3.9 cm in the longest diameter (). Color Doppler signal demonstrated internal vascularity with absent fatty hilum. A core needle biopsy revealed a poorly differentiated adenocarcinoma (), which was likely of breast origin. Three months before presentation to our department, the patient had developed periorbital erythematous papules, distributed over the lower eyelids, measuring 2.0×1.5 cm (), which was diagnosed as DM by the rheumatology department. Over the subsequent 3 months, he had also noted progressive proximal upper muscle weakness in a symmetric distribution. However, he declined any therapeutic intervention.
Figure 1 Ultrasound of the right axillary mass.
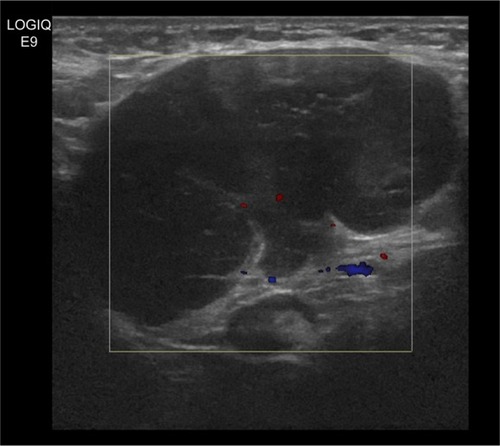
Figure 2 Image of core needle biopsy histologic diagnosis using hematoxylin and eosin staining (original ×100).
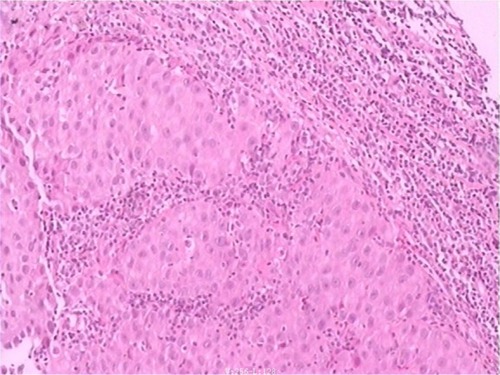
Figure 3 Preoperative facial photo of patient.
Physical examination identified a nonmobile mass in the right axilla, measuring 5.0 cm in diameter; other superficial lymph nodes were not significantly enlarged and the skin covering the mass was normal. No nipple discharge and no masses were identified in either breast or other organs. A computed tomography scan of the brain, abdomen, and pelvis failed to reveal any malignant primary lesions. The bone scan screening for metastasis was negative.
On May 19, 2015, the patient underwent a modified radical mastectomy, which consisted of whole breast mastectomy and axillary lymph node dissection. However, no lesions were found on the right breast during surgery. The IHC of the lymph node tissue was negative for estrogen receptor (), progesterone receptor (), prostate-specific antigen (PSA) (−), positive gross cystic disease fluid protein-15 (GCDFP-15), AE1/AE3, cytokeratin 7 (CK7), CK20, and human epidermal growth factor receptor 2 (HER2), while HER2 was amplified (negative) by FISH analysis (). Dissection of axillary demonstrated 0 of 17 signs of metastatic lymph nodes except for the original malignant axillary lymph node. Based on these findings, he was diagnosed with right axillary metastatic TNBC presumably from an OBC. According to American Joint Committee on Cancer Staging, the stage of cancer classification was II stage (T0N1M0). The patient was submitted to adjuvant chemotherapy with 4 cycles of TC (Paclitaxel: 270 mg, Cyclophosphamide: 0.9 g) and a rest of 21 days.
Figure 4 Expression of ER/PR by IHC staining (original ×100) and HER2 by FISH analysis (original ×400).
Abbreviations: ER, estrogen receptor; PR, progesterone receptor; IHC, immunohistochemistry; HER2, human epidermal growth factor receptor 2; FISH, fluorescent in situ hybridization.

Following mastectomy, he experienced remarkable improvement of the dermal erythematous papules () and gradual recovery of muscle strength with normalization of creatinine kinase blood levels without glucocorticoid therapy.
Figure 5 Postoperative facial photo of patient.

Over >2 years of follow-up, the patient remained in good condition, without cutaneous or muscle DM recurrence or recurrence of breast cancer or other lesions.
Discussion
OBC is defined by the presence of axillary metastases without an identifiable breast tumor. It accounts for 0.3%–1% of all newly diagnosed malignant diseases of the breast.Citation1 A man’s lifetime risk of developing breast cancer is ~0.7%, but it has an increase in incidence in the seventh decade of life.Citation2,Citation3 Because of the rarity of OBC in men, the diagnosis and treatment can be challenging. Most of the studies available in the literature have demonstrated that there were several reasons for palpable axillary masses, most commonly being metastatic lymph nodes associated with breast cancer.Citation4 When an axillary mass does occur, the most widely accepted method is to identify whether physical examination and imaging studies identify benign or malignant features. The next question is to confirm the primary source of disease.
Data can also be obtained for immunocytochemistry through a core needle biopsy of the metastasis. In this case, immunohistochemical and FISH studies revealed ER (−), PR (−), HER2 (−), GCDFP-15 (+), AE1/AE3 (+), CK7 (+), CK20 (+), and PSA (−). Thus, we diagnosed the axillary tumor as primary breast cancer with axillary lymph node involvement. Based on immunohistochemical and FISH analyses of ER, PR, Ki-67, and HER2, a simplified classification was adopted to identify different subtypes of breast cancer. In the previous literature, it has been reported that most primary lesions of OBC exhibit a significantly higher positive rate for hormone receptors than that of female breast carcinomas.Citation5 Our case was even more unusual being TNBC.
TNBC, which is a special subtype of breast cancer, has been demonstrated to have a significantly higher risk of recurrence and death compared with luminal subtypes.Citation6 Numerous studies have addressed the classification of TNBC to assist clinical management. Recently, Zhang et al described subnetwork biomarkers of low oncogenic GTPase activity, low ubiquitin/proteasome degradation, effective protection from oxidative damage, and tightly immune response to be linked with better prognosis through integrative analysis of cancer genomics data and protein interactome data.Citation7 However, clinical data on TNBC in male patients are limited, and it is still unclear if the major prognostic factors in MBC are the same as those in women. An abstract presented at the 45th Annual Meeting of the American Society of Clinical Oncology in 2010 by Forester reported that male TNBC had a significantly worse prognosis than female TNBC or than other subtypes.Citation8
Principles of treatment for male occult TNBC are similar to those of female breast cancer. Widely used adjuvant chemotherapy in breast cancer for TNBC is more chemosensitive than the HR-positive/HER2-negative phenotype.Citation9 Compared with that of stage and subtype-matched patients, similar outcome was observed in OBC patients, while there was a trend for higher risk of recurrence and mortality in OBC patients with the triple negative subtype.Citation10
DM is an idiopathic inflammatory myopathy associated with proximal muscle weakness and cutaneous findings such as heliotrope rashes, Gottron’s papules, and periungual telangiectasis.Citation11 Laboratory studies show creatine kinase elevation, electrophysiologic abnormalities, and inflammatory lesions on muscle biopsy. DM carries an increased risk of malignancy and can present as a paraneoplastic syndrome to multiple types of underlying malignancies, especially lung and prostate cancers, gastrointestinal tumors in men, and gynecological tumors in women, rarely in MBC. Polymyositis (PM)/DM can precede or present at the same time of or after the onset of malignant tumor development. Most commonly, however, the literature reports that malignant tumors appear >2 years after the onset of PM/DM. The risk of malignancy within the first year after the diagnosis of PM/DM is the highest, then decreases by each year, but remains higher than in the normal population. Therefore, the screening of malignant tumor should be carried out extensively within the first year after the appearance of PM/DM. Andras et al found that with 309 cases of PM/DM analysis,Citation12 among the 37 cases with malignant tumors, the proportion of malignancy and myositis in the first year was 64.8%. Another study from 2003 to 2012, 246 cases of DM was retrospectively reviewed for 10 years. Including 60 cases with malignant tumors, 39 cases (65.0%) occurred 1 year after diagnosis of DM. Malignancies were detected in 13 (21.7%, 13/60) patients during the second year and 8 (13.3%, 8/60) during the third year after DM.Citation13
There is little evidence to guide treatment of DM. Wolff et al reported a rare case of DM with triple negative female breast cancer managed with chemotherapy and injectable adrenocorticotropic hormone agonist without surgery.Citation14 However, the role of neoadjuvant chemotherapy is debatable. Ideally, detection and surgical removal of the malignant tumor yields the best results in improvement of DM. In this case, the patient developed periorbital erythematous papules 3 months before diagnosis of MBC. It is noteworthy that, after surgery, he experienced remarkable improvement in the dermal erythematous papules with gradual recovery of muscle strength without glucocorticoid therapy. These findings strongly confirm the importance of diagnosis and surgical treatment of the underlying malignancy.
The prognosis of DM patients with malignant tumors is poor. The main causes of death are extensive metastasis of tumor, secondary infection, and systemic failure. The overall survival rate of PM/DM patients with malignant tumors is worse than that of other forms of myositis, and prognosis and life expectancy are determined by the underlying malignancies.Citation15
Conclusion
We presented a rare case of male occult TNBC with DM. No conclusion has been drawn regarding current drug therapy, and surgery is still the main treatment.
Acknowledgments
Our study received approval from the ethics committee of the Second Affiliated Hospital of Dalian Medical University. The patient and family members also provided written informed consent to publish this case report details.
Disclosure
The authors report no conflicts of interest in this work.
References
- BrillKLBreninDROccult breast cancer and axillary massCurr Treat Options Oncol20012214915512057133
- HeMLiuHJiangYA case report of male occult breast cancer first manifesting as axillary lymph node metastasis with part of metastatic mucinous carcinomaMedicine (Baltimore)20159425e103826107674
- KhanMHAllertonRPettitLHormone therapy for breast cancer in menClin Breast Cancer201515424525026165199
- ParkJESohnYMKimEKSonographic findings of axillary masses: what can be imaged in this space?J Ultrasound Med20133271261127023804349
- GuGLWangSLWeiXMRenLZouFXAxillary metastasis as the first manifestation of occult breast cancer in a male patientBreast Care (Basel)200941434520877684
- Chavez-MacgregorMClarkeCALichtensztajnDHortobagyiGNGiordanoSHMale breast cancer according to tumor subtype and race: a population-based studyCancer201311991611161723341341
- ZhangFRenCZhaoHIdentification of novel prognostic indicators for triple-negative breast cancer patients through integrative analysis of cancer genomics data and protein interactome dataOncotarget2016744716207163427690302
- ArslanUYOksuzogluBOzdemirNOutcome of non-metastatic male breast cancer: 118 patientsMed Oncol201229255456021573973
- YamamotoYIwaseHClinicopathological features and treatment strategy for triple-negative breast cancerInt J Clin Oncol201015434135120632057
- MontagnaEBagnardiVRotmenszNImmunohistochemically defined subtypes and outcome in occult breast carcinoma with axillary presentationBreast Cancer Res Treat2011129386787521822638
- YehCNChenSCHwangTLChenMFLiawCCChanHLBreast carcinoma in patients with dermatomyositis: a retrospective analysis of eight casesChang Gung Med J200225637438012173666
- AndrasCPonyiAConstantinTDermatomyositis and polymyositis associated with malignancy: a 21-year retrospective studyJ Rheumatol200835343844418203322
- ChenDYuanSWuXIncidence and predictive factors for malignancies with dermatomyositis: a cohort from southern ChinaClin Exp Rheumatol201432561562125068842
- WolffMMancusoCLalKDicostanzoDGropperCParaneoplastic dermatomyositis with cutaneous and myopathic disease responsive to adrenocorticotropic hormone therapyJ Clin Aesthet Dermato20171015762
- PonyiAConstantinTGaramiMCancer-associated myositis: clinical features and prognostic signsAnn N Y Acad Sci20051051647116126945