
Abstract
Purpose
There is a great controversy regarding the prognostic significance of epidermal growth factor receptor (EGFR) in glioma patients. The current meta-analysis was conducted to evaluate the effect of abnormal EGFR expression on overall survival in glioma patients.
Materials and methods
A comprehensive literature search of PubMed, EMBASE, Google Scholar, Web of Science, and Cochrane Library was conducted. The combined hazard ratio (HR) and its 95% confidence intervals (CIs) were used to evaluate the association between EGFR expression and survival in glioma.
Results
A total of 476 articles were screened, and 17 articles containing 1,458 patients were selected. The quality assessment of the included studies was performed by the Newcastle–Ottawa Scale. Overexpression of EGFR was found to be an indicator of poor prognosis in overall survival in glioma patients (HR =1.72, 95% CI 1.32–2.25, P=0.000, random effect) and glioblastoma multiforme patients (HR =1.57, 95% CI 1.15–2.14, P=0.004, random effect). Subgroup analysis was conducted to explore the source of high heterogeneity.
Conclusion
This meta-analysis indicated that high expression of EGFR may serve as a biomarker for poor prognosis in glioma patients.
Introduction
Epidermal growth factor receptor (EGFR) is a transmembrane tyrosine kinase on chromosome 7p12, containing an extracellular ligand-binding domain, a transmembrane domain, and an intracellular tyrosine kinase domain, belonging to the HER family. The family includes four members (HER1/EGFR, HER2/neu, HER3, and HER4), with downstream signaling pathways regulating a number of processes, including growth, migration, and survival.Citation1 The pathway is involved in the development and progression of several human malignancies, including non-small-cell lung cancer, gastric cancer, pancreatic cancer, and nasopharyngeal carcinoma.Citation2–Citation6
Glioma is the most common primary malignancy of the central nervous system, accounting for over half of all malignant brain tumors in adults.Citation7 According to the WHO grading (2016), glioma can be divided into four grades. Glioblastoma multiforme (GBM) has the highest grade and the greatest malignancy. The median survival after standard treatment is ∼13 months. Median progression-free survival (PFS) is only 7.2 months.Citation8 The EGFR gene is one of the earliest known carcinogenic genes found in GBM. Its increased transcriptional activity directly causes EGFR expression.Citation9 Due to its pro-oncogenic effects, it is not surprising that increased EGFR expression is associated with the malignancy of glioma.Citation10 A study has found that serum levels of EGFR are substantially increased in patients with malignant glioma, suggesting poor survival.Citation11
It has been hypothesized that EGFR may be a potential prognostic biomarker for glioma. However, there remains some controversy as to the prognostic value of EGFR in glioma. Because of the limitations of sample size and research methods, individual studies have not reached consensus on the question. Therefore, this meta-analysis was conducted to evaluate the effect of abnormal EGFR expression on overall survival (OS) in glioma patients.
Materials and methods
Retrieval strategy
Comprehensive literature retrieval was conducted using electronic databases such as PubMed, EMBASE, Google Scholar, Web of Science, and Cochrane Library (up to June 10, 2017). Medical subject headings (MeSH) (Emtree for EMBASE) and free-text words were adopted to balance comprehensiveness and accuracy. The following search terms were used: “Receptor, Epidermal Growth Factor” [Mesh], “Receptor Tyrosine-protein Kinase erbB-1”, “Transforming Growth Factor alpha Receptor”, “TGF-alpha Receptor”, “Epidermal Growth Factor Receptor Kinase”, “erbB-1 Proto-Oncogene Protein”, “erbB-1 Proto-Oncogene Protein”, “Receptor, Transforming-Growth Factor alpha”, “Receptor, TGF-alpha”, “c-ErbB-1 Protein, Proto-oncogene”; “Glioma” [Mesh], “astrocytoma”, “ependymoblastoma”, “ependymoma”, “glioblastoma”, “medulloblastoma”, “oligodendroglioma”, “optic nerve glioma”, “pontine glioma”, and “subependymoma”, and key words related to survival included prognostic, survival, predictive, outcome, and death. The references of retrieved articles were also screened for eligible studies.
Inclusion and exclusion criteria
Inclusion criteria were as follows: 1) studies on pathological diagnosis of glioma in humans and investigation of EGFR expression in glioma; 2) studies containing hazard ratio (HR) or including survival data such as survival curves to estimate HR and its 95% confidence interval (CI); 3) studies published in English; 4) studies in which detection methods for EGFR were restricted to immunohistochemistry (IHC); and 5) randomized controlled trials, retrospective or prospective studies.
Exclusion criteria were as follows: 1) non-human experiments; 2) letters, case reports, and reviews; 3) duplicated publications; and 4) inability to extract HR or necessary information.
Data extraction and quality assessment
All data were extracted independently by two authors (Junhong Li and Ruofei Liang). Disagreements were resolved by consensus with a third investigator (Yanhui Liu). The following data were extracted from the eligible studies: last name of the first author, publication year, region, study design, tumor type, assay, sample size, cutoff point, maximum follow-up time, HR, and its 95% CI.
HR and its 95% CI were extracted directly from the publications. If HRs and 95% CI were not available directly, they were calculated from the available survival data or extracted from the Kaplan–Meier curves by using the methods of Parmar et alCitation12 and Tierney et al.Citation13 If a study contained both univariate and multivariate analyses, both with HR, the HR provided by multivariate analysis was selected preferentially.
The quality of the eligible articles was evaluated on the Newcastle–Ottawa Scale (NOS), including assessments of patient selection, study comparability, follow-up time, and relevant outcome. NOS scores ranged from 0 to 9, with high-quality study defined as a score of >6.
Statistical analysis
HR and 95% CIs were used to evaluate the association between EGFR expression and OS in glioma. An HR of >1 indicated worse survival with elevated EGFR expression, and a 95% CI not overlapping 1 was taken to be statistically significant. Statistical heterogeneity of the included studies was assessed by I2 statistics and chi-square test, and I2 value >50% or Pheterogeneity <0.05 indicated substantial heterogeneity. The random-effects model was used to estimate the pooled HR if heterogeneity appeared. Otherwise, the fixed-effect model was applied.Citation14 All P-values were two-sided, and P<0.05 was considered to be statistically significant. Sensitivity analysis was also performed to evaluate the stability and reliability of the combinative results. The funnel plot with Begg’s test and Egger’s test was applied to evaluate publication bias. STATA 12.0 (StataCorp LP, College Station, TX, USA) was used to perform statistical analysis.
Results
Characteristics of the included studies
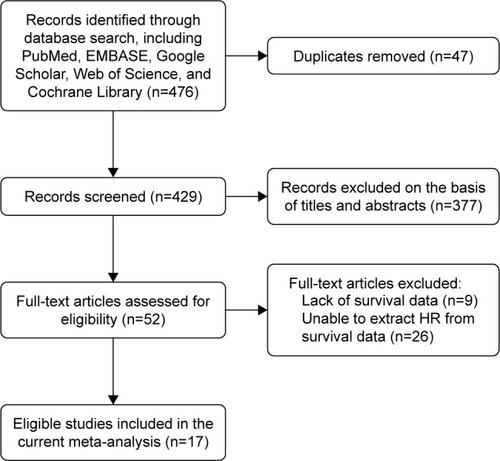
A total of 476 articles were screened from the databases, and 17 eligible articles including 1,458 patients were selected ( and ).Citation15–Citation31 The publication dates ranged from 1998 to 2015, sample size from 18 to 199, and maximum follow-up time from 25 to 180 months. On NOS scoring, five articles were rated 6 points, one article was rated 7 points, and only one article was rated 8 points. Among all the included studies, only two were prospective studies, and the rest were retrospective studies. In most studies, specimens were fixed with formalin and embedded with paraffin. The treatment of tumor tissues was not clearly defined in two studies. IHC was performed in all studies. Of the 17 articles, seven reported the available HR and 10 provided the Kaplan–Meier curves. Considering glioma subgroups, 10 studies focused on GBM, two studies focused on ependymoma, two focused on low-grade glioma (LGG), one focused on astrocytoma, one included anaplastic astrocytoma (AA) and GBM, and one included glioma of various subgroups and grades. No study reported disease-free survival or PFS.
Table 1 The main characteristics of the included 17 studies in the meta-analysis
Figure 1 Flow diagram of the study selection process.
Prognostic significance of EGFR expression in glioma patients
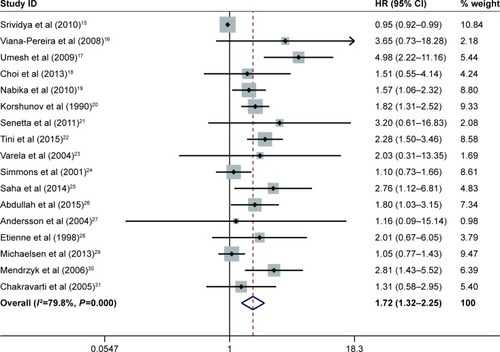
A total of 1,458 glioma patients were included in the survival analysis. The pooled HR was 1.72 (95% CI 1.32–2.25, P=0.000, random effect; ). High expression of EGFR had a significant relationship with poor prognosis for glioma patients.
Figure 2 Meta-analysis of pooled HRs of OS in gliomas.
Abbreviations: CI, confidence interval; HR, hazard ratio; OS, overall survival.
Due to the emergence of high heterogeneity in the study (I2=79.8%, Ph=0.000), a subgroup analysis was conducted to further explore the source of heterogeneity. The subgroups included tumor types, publication years, region, study design, sample size, cutoff value, maximum follow-up time, source of HR, and quality score (). High EGFR expression was significantly associated with reduced OS in GBM (HR 1.57, 95% CI 1.15–2.14, P=0.004) and mixed gliomas (HR 1.95, 95% CI 1.37–2.77, P=0.000), but not in LGG (HR 1.67, 95% CI 0.037–7.62, P=0.508). There was substantial heterogeneity in GBM (I2=83.8%, Ph=0.000), while heterogeneity was not found in LGG (I2=0%, Ph=0.731) and mixed gliomas (I2=0%, Ph=0.522). In subgroups of publication years, study design, sample size, source of HR, and quality score, the following predicted poor survival: publication year <2010 (HR 1.95, 95% CI 1.37–2.77, P=0.000); publication year ≥2010 (HR 1.52, 95% CI 1.10–2.10, P=0.011); retrospective study (HR 1.75, 95% CI 1.39–2.19, P=0.000); sample size <100 (HR 1.99, 95% CI 1.54–2.57, P=0.000); sample size ≥100 (HR 1.43, 95% CI 1.04–2.97, P=0.027); HRs extracted from the Kaplan–Meier curves (HR 2.10, 95% CI 1.71–2.58, P=0.000); quality score <7 (HR 1.37, 95% CI 1.00–1.87, P=0.048); and quality score ≥7 (HR 1.72, 95% CI 1.32–2.25, P=0.000).
Table 2 Meta-analysis results of subgroups for the OS of gliomas
Apparent heterogeneity existed in the subgroup of publication year ≥2010 (I2=80.2%, Ph=0.000), prospective study (I2=81.1%, Ph =0.000), sample size ≥100 (I2=85.5%, Ph=0.000), HRs that were reported (I2=69.5%, Ph=0.003), and quality score ≥7 (I2=84.8%, Ph=0.000). Low heterogeneity existed in the subgroup of publication year <2010 (I2=45.6%, Ph=0.065) and retrospective study (I2=45.8%, Ph=0.024). Sample size <100 (I2=0%, Ph=0.501) and quality score <7 (I2=0%, Ph=0.618) did not show heterogeneity.
The subgroup region included three variables: Europe, America, and Asia, where Europe (HR 1.86, 95% CI 1.32–2.61, P=0.000) and Asia (HR 1.83, 95% CI 1.04–3.23, P=0.037) were significantly related to worse prognosis, but not related to America (HR 1.32, 95% CI 0.98–1.79, P=0.070). The heterogeneity of America (I2=0%, Ph=0.546), Europe (I2=53.3%, Ph=0.036), and Asia (I2=85.7%, Ph=0.000) gradually increased. In the two subgroups of cutoff value and maximum follow-up time, each subitem gave significance for predicting prognosis. The heterogeneity of cutoff value <20% (I2=28.2%, Ph=0.223) and cutoff value ≥20% (I2=43.9%, Ph=0.129) was relatively low, while there was substantial heterogeneity in the subgroup of cutoff value determined by other modes and of unavailable cutoff value (I2=83.3%, Ph=0.000). There was substantial heterogeneity in the subgroup of maximum follow-up time <100 months (I2=81.8%, Ph=0.000), while there was no substantial heterogeneity in the subgroup of maximum follow-up time ≥ 100 months (I2=0%, Ph=0.976) and unavailable maximum follow-up time (I2=0%, Ph=0.944).
Prognostic significance of EGFR expression in GBM patients
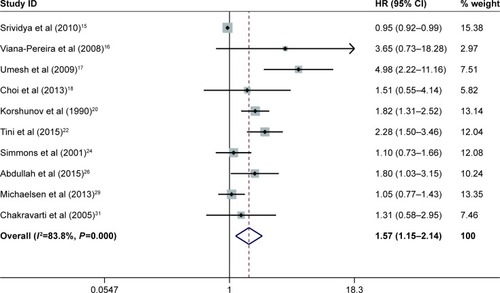
GBM is one of the most common gliomas with the highest degree of malignancy. It accounts for a large proportion of the included studies, and therefore, a meta-analysis was conducted to determine the prognostic significance of EGFR expression in GBM patients. Ten studies including 1,074 patients were considered in the survival analysis. The pooled HR was 1.57 (95% CI 1.15–2.14, P=0.004, random effect; ). This indicated that high expression of EGFR was significantly associated with poor prognosis in GBM patients. Similarly, subgroup analysis was performed because of high heterogeneity (I2=83.8%, Ph=0.000). The grouping and results of subgroup analysis are displayed in .
Table 3 Meta-analysis results of subgroups for the OS of GBMs
Figure 3 Meta-analysis of pooled HRs of OS in GBM.
Abbreviations: CI, confidence interval; GBM, glioblastoma multiforme; HR, hazard ratio; OS, overall survival.
Sensitivity analysis and publication bias
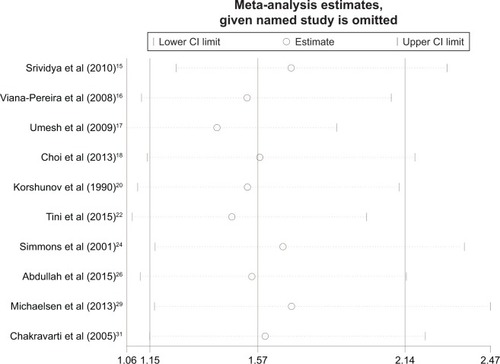
All the studies were sequentially removed to determine whether a single study had significant influence on pooled HR and to verify the stability and reliability of HR estimates. It was found that the pooled HRs were not significantly influenced by any individual study ( and ).
Figure 4 Sensitivity analysis of the relationship between EGFR expression and overall survival in glioma patients.
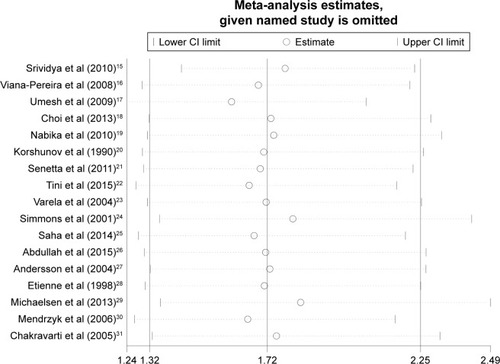
Figure 5 Sensitivity analysis of the relationship between EGFR expression and overall survival in GBM patients.
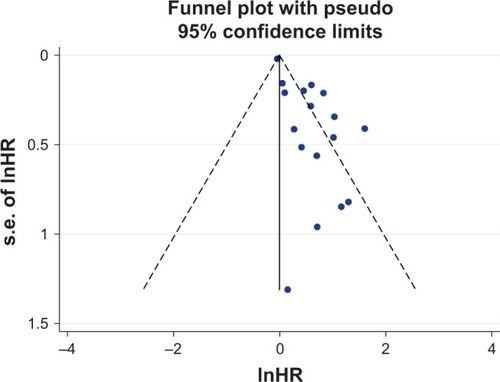
Publication bias was assessed using the funnel plot (), Begg’s and Egger’s tests. The funnel plot was asymmetrical. Begg’s test (z =0.54, P > |z| =0.592) revealed no publication bias among the 17 eligible studies, while Egger’s test (t=5.41, P> |t| =0.000) showed clear bias.
Figure 6 The funnel plot for all the included studies for overall survival.
Discussion
EGFR plays an important role in tumor growth, participating in cell motility, adhesion, invasion, and angiogenesis.Citation32 In recent years, EGFR has been a focus of numerous studies on tumor prognosis. Similar meta-analyses involving gastric cancer, non-small-cell lung cancer, nasopharyngeal carcinoma, pancreatic cancer, and esophageal adenocarcinoma have shown poor prognosis associated with EGFR expression.Citation32–Citation36 Comparatively speaking, biomarker studies in glioma have been relatively recent. There have been a large number of inconsistent and even contradictory results regarding the prognostic significance of EGFR in glioma. Among the included studies, 12 suggested that high expression of EGFR indicates poor prognosis, while five others were negative or uncertain on the question. In addition to the 17 studies included in the current meta-analysis, the studies that were excluded according to the inclusion criteria also showed a substantial degree of polarization. High expression of EGFR was not found to predict the poor prognosis of glioma in the studies of Reis-Filho et al,Citation37 Bouvier-Labit et al,Citation38 Smith et al,Citation39 and Dorward et al,Citation40 while other studies suggested that elevated EGFR predicted reduced OS.Citation41–Citation46
Similarly, as the direct source of EGER expression, EFEG amplification was also used as a prognostic marker of glioma. The literature also returned two levels of differentiation. Some studies showed that EGFR amplification was related to worse survival,Citation47–Citation50 while other studies returned the opposite result.Citation51–Citation53 Hobbs et alCitation54 showed that low-to-moderate EGFR amplification was an independent adverse prognostic variable, while high-level EGFR amplification did not play a role in a similar model. In the study of EGFR gene polymorphisms, Costa et alCitation55 found that EGFR variants “−191C/A” and “intron 1 (CA)n repeat” were prognostic markers in GBM patients. Li et alCitation56 conducted a similar gene polymorphism study. In the molecular studies of the Tunisian population, both EGFR amplification and EGFR overexpression predicted significantly poor OS.Citation57 The study on pediatric glioma indicated that no association was apparent between EGFR expression level and either PFS or OS.Citation58,Citation59 All the abovementioned studies have provided rigorous experimental design and accurate and reliable data analysis but contradictory results. A previous meta-analysis of EGFR amplification done by Chen et alCitation60 concluded that there is not enough evidence to suggest that EGFR amplification has prognostic value in GBM patients.
In addition to being a potential prognostic factor, EGFR is also a potential target for the treatment. Some reports claim that 97% of primary GBM show EGFR amplification.Citation61 Because of the important role of EGFR signaling in the pathogenesis of malignant tumor, a growing number of studies have been devoted to developing therapeutic strategies targeting EGFR aberrant activity. As a transmembrane tyrosine kinase, small molecule tyrosine kinase inhibitors (TKIs) may theoretically inhibit EGFR expression and function in malignant tumor. The mechanism would involve displacement of ATP from the catalytic pocket of the enzyme to inhibit kinase activity. Monoclonal antibodies may play a role by combining with the extracellular domain of EGFR.Citation9 Both the methods have been applied in clinical practice with remarkable results in the treatment of non-small-cell lung cancer and colon cancer. However, the use of TKIs and monoclonal antibodies in glioma is challenged. Preusser et alCitation62 concluded in their clinical trial that only a small number of malignant glioma patients benefited from EGFR inhibitor monotherapy. Bevacizumab has a tendency to increase the risk of adverse effects in people older than 65 years, and there is not enough evidence to recommend the use of bevacizumab in pediatric glioma patients.Citation8 Combined with other treatments, such as temozolomide and radiation therapy, stereotactic surgery may be helpful in controlling glioma. Newer and safer targeted therapies have yet to be developed to improve treatment efficacy.
There is a considerable degree of heterogeneity among various studies. Heterogeneity emerged from differences in experimental items, overall experimental design, and analyzed indicators. There was substantial heterogeneity (I2=79.8%, Ph=0.000) in pooled HR in the current meta-analysis. Similar results in pooled HR were observed in the GBM group (I2=83.8%, Ph=0.000). Although the final results suggested poor prognostic role of EGFR, high heterogeneity substantially reduces the reliability of the results. The operations from setting include criteria, subgroup analysis and sensitivity analysis were used to ensure the reliability of the final results, in other words, to provide a strong reference. All the included studies used HR with 95% CI as the index of survival analysis. With I2 and Ph as indicators of heterogeneity, subgroup analysis suggested high heterogeneity in tumor types, publication year, region, sample size, maximum follow-up time, source of HR, and quality score, as follows: GBM (I2=83.8%, Ph =0.000), publication year ≥2010 (I2=80.2%, Ph=0.000), Asia (I2=85.7%, Ph =0.000), sample size ≥100 (I2=85.5%, Ph=0.000), and other methods to divide cutoff value and cutoff value not available (I2=83.3%, Ph=0.000), maximum follow-up time <100 months (I2=81.8%, Ph=0.000), and quality score ≥7 (I2=84.8%, Ph=0.000). There was low heterogeneity in Europe (I2=53.3%, Ph=0.036) when HR was reported (I2=69.5%, Ph=0.003). The abovementioned items were the actual source of heterogeneity; other items showed low or no heterogeneity. Among 22 items in the nine subgroups, only three had HR with no statistical significance, including LGG (HR 1.67, 95% CI 0.37–7.62, P=0.508), America (HR 1.32, 95% CI 0.98–1.79, P=0.070), and HR that were reported (HR 1.28, 95% CI 0.98–1.66, P=0.072). This suggested a stable and reliable final result.
In the GBM subgroup analysis, there was substantial heterogeneity in items such as publication year ≥2010 (I2=82.2%, Ph =0.000), Europe (I2=73.7%, Ph=0.010), Asia (I2=88.1%, Ph=0.000), sample size ≥100 (I2=84.4%, Ph=0.000), other methods to divide cutoff value (I2=80.4%, Ph=0.000), unavailable cutoff value (I2=80.4%, Ph=0.000), maximum follow-up time <100 months (I2=82.0%, Ph =0.000), and quality score ≥7 (I2=86.2%, Ph=0.000). The condition was basically consistent with HR subgroup analysis of the whole set of glioma. Among 19 items in the eight subgroups, pooled HR of eight items showed no statistical significance, and the reliability and stability of the pooled results were lower than that of the entire group of glioma. The greater heterogeneity of the GBM group (83.8% vs 79.8%) is one of the reasons for these results.
In sensitivity analysis, individual studies were sequentially removed, and the bottom limits of 95% CI of pooled HR of other studies were all larger than 1, suggesting that individual studies had limited impact on the entire study. The pooled HR had statistical significance, and the entire study was stable.
Asymmetry of the funnel plot and Egger’s test demonstrated the existence of publication bias (the most common source of bias) affecting the authenticity and reliability of the data to some extent. First, positive results are easier to publish. Of the 17 studies, five were negative, and the inclusion of negative results would theoretically reduce publication bias. Second, repeatedly published theses will also lead to bias, if a single-center or multiple-center results are both published and included. Repeated calculation would lead to larger weight for some studies, affecting the reliability of the clinical research. The research institutions and localities were carefully checked, and overlapping of institutions or experimental data was not found. Next, the small sample size studies return low test efficiencies. In other words, positive results may be caused by opportunities, which may not provide a reliable basis for clinical practice. In the subgroup analysis, HR was merged with a sample size of 100 as the boundary. Our results suggested larger HR and lower P in the subgroup with a sample size of <100, without heterogeneity, while greater heterogeneity was observed in the subgroup with large sample size (≥100). This confirmed that bias was caused by small sample size from the side. There may be many other unknown confounding factors that play a role in publication bias.
As a meta-analysis of prognostic analysis, there are inevitable limitations in several aspects which should be further discussed. First, the areas and population involved in this study are irregular (Africa, the Middle East, South America, and other regions). In addition, China, with a large population, was not considered. Second, there are differences in diagnostic standard and inspection methods in studies on glioma at different times. The accuracy of IHC results is improved by the optimization of the equipment and test methods with the passage of time. The diverse definitions of cutoff values among the studies may also lead to bias. Among experimental designs, there were no randomized controlled trials, which might have improved the accuracy of the analysis. However, there were two prospective studies, which are superior to retrospective studies. Finally, patients in several studies underwent standard therapy with temozolomide plus radiotherapy after surgeryCitation15,Citation22,Citation29 and some patients did not undergo uniform treatments, while the remaining studies failed to report postoperative treatments. This too may result in heterogeneity of survival data.
Conclusion
Our meta-analysis suggested that EGFR may serve as a useful biomarker for poor prognosis in glioma patients. In the future, targeted therapy aiming at EGFR signaling pathways may help slow the disease progression of glioma and prolong OS. To verify this result, studies with large sample sizes, covering extensive areas, with more reasonable experimental designs, more standardized diagnostic criteria, and standardized postoperative treatment are required.
Acknowledgments
This study was supported by the Key Research and Development Item from the Department of Science and Technology of Sichuan Province, China (No 2017SZ0006). Junhong Li and Ruofei Liang are the co-first authors.
Disclosure
The authors report no conflicts of interest in this work.
References
- HobbsJNikiforovaMNFardoDWParadoxical relationship between the degree of EGFR amplification and outcome in glioblastomasAm J Surg Pathol20123681186119322472960
- PanJKongLLinSChenGChenQLuJJThe clinical significance of coexpression of cyclooxygenases-2, vascular endothelial growth factors, and epidermal growth factor receptor in nasopharyngeal carcinomaLaryngoscope2008118111970197518758376
- MatsumuraTSugimachiKTakahashiYClinical significance of GAB2, a scaffolding/docking protein acting downstream of EGFR in human colorectal cancerAnn Surg Oncol201421Suppl 4S743S74925029990
- DengWGuLLiXCD24 associates with EGFR and supports EGF/EGFR signaling via RhoA in gastric cancer cellsJ Transl Med2016143226830684
- LaurieSAGossGDRole of epidermal growth factor receptor inhibitors in epidermal growth factor receptor wild-type non-small-cell lung cancerJ Clin Oncol20133181061106923401452
- QinCFHaoKTianXDXieXHYangYMCombined effects of EGFR and Hedgehog signaling pathway inhibition on the proliferation and apoptosis of pancreatic cancer cellsOncol Rep201228251952622581058
- BrandesAAFranceschiETosoniAHegiMEStuppREpidermal growth factor receptor inhibitors in neuro-oncology: hopes and disappointmentsClin Cancer Res200814495796018281526
- GhiaseddinAPetersKBUse of bevacizumab in recurrent glioblastomaCNS Oncol20154315716925906439
- KrishnanSRaoRDJamesCDSarkariaJNCombination of epidermal growth factor receptor targeted therapy with radiation therapy for malignant gliomasFront Biosci20038e1e1312456322
- HorbinskiCHobbsJCieplyKDacicSHamiltonRLEGFR expression stratifies oligodendroglioma behaviorAm J Pathol201117941638164421839716
- QuarantaMDivellaRDanieleAEpidermal growth factor receptor serum levels and prognostic value in malignant gliomasTumori200793327528017679463
- ParmarMKTorriVStewartLExtracting summary statistics to perform meta-analyses of the published literature for survival endpointsStat Med19981724281528349921604
- TierneyJFStewartLAGhersiDBurdettSSydesMRPractical methods for incorporating summary time-to-event data into meta-analysisTrials200781617555582
- LauJIoannidisJPSchmidCHQuantitative synthesis in systematic reviewsAnn Intern Med199712798208269382404
- SrividyaMRThotaBArivazhaganAAge-dependent prognostic effects of EGFR/p53 alterations in glioblastoma: study on a prospective cohort of 140 uniformly treated adult patientsJ Clin Pathol201063868769120702468
- Viana-PereiraMLopesJMLittleSAnalysis of EGFR overexpression, EGFR gene amplification and the EGFRvIII mutation in Portuguese high-grade gliomasAnticancer Res2008282a91392018507036
- UmeshSTandonASantoshVClinical and immunohistochemical prognostic factors in adult glioblastoma patientsClin Neuropathol200928536237219788052
- ChoiYSongYJLeeHSEpidermal growth factor receptor is related to poor survival in glioblastomas: single-institution experienceYonsei Med J201354110110723225805
- NabikaSKiyaKSatohHPrognostic significance of expression patterns of EGFR family, p21 and p27 in high-grade astrocytomaHiroshima J Med Sci2010594657021361082
- KorshunovAGolanovASychevaRProninIPrognostic value of tumour associated antigen immunoreactivity and apoptosis in cerebral glioblastomas: an analysis of 168 casesJ Clin Pathol199952857458010645226
- SenettaRMiraccoCLanzafameSEpidermal growth factor receptor and caveolin-1 coexpression identifies adult supratentorial ependymomas with rapid unfavorable outcomesNeuro Oncol201113217618321059755
- TiniPCeraseACeveniniGCarboneSFMiraccoCPirtoliLEpidermal growth factor receptor expression may correlate with survival through clinical and radiological features of aggressiveness in glioblastoma treated with radiochemotherapyAnticancer Res20153574117412426124364
- VarelaMRanuncoloSMMorandiAEGF-R and PDGF-R, but not bcl-2, overexpression predict overall survival in patients with low-grade astrocytomasJ Surg Oncol2004861344015048678
- SimmonsMLLambornKRTakahashiMAnalysis of complex relationships between age, p53, epidermal growth factor receptor, and survival in glioblastoma patientsCancer Res20016131122112811221842
- SahaRChatterjeeUMandalSSahaKChatterjeeSGhoshSExpression of phosphatase and tensin homolog, epidermal growth factor receptor, and Ki-67 in astrocytoma: a prospective study in a tertiary care hospitalIndian J Med Paediatr Oncol201435214915525197177
- AbdullahKGRamayyaAThawaniJPFactors associated with increased survival after surgical resection of glioblastoma in octogenariansPLoS One2015105e012720225978638
- AnderssonUGuoDMalmerBEpidermal growth factor receptor family (EGFR, ErbB2–4) in gliomas and meningiomasActa Neuropathol2004108213514215148612
- EtienneMCFormentoJLLebrun-FrenayCEpidermal growth factor receptor and labeling index are independent prognostic factors in glial tumor outcomeClin Cancer Res1998410238323909796969
- MichaelsenSRChristensenIJGrunnetKClinical variables serve as prognostic factors in a model for survival from glioblastoma multiforme: an observational study of a cohort of consecutive non-selected patients from a single institutionBMC Cancer20131340224004722
- MendrzykFKorshunovABennerAIdentification of gains on 1q and epidermal growth factor receptor overexpression as independent prognostic markers in intracranial ependymomaClin Cancer Res2006127 pt 12070207916609018
- ChakravartiASeiferheldWTuXImmunohistochemically determined total epidermal growth factor receptor levels not of prognostic value in newly diagnosed glioblastoma multiforme: report from the Radiation Therapy Oncology GroupInt J Radiat Oncol Biol Phys200562231832715890570
- MeertAPMartinBDelmottePThe role of EGF-R expression on patient survival in lung cancer: a systematic review with meta-analysisEur Respir J200220497598112412692
- MaXHuangJWuXEpidermal growth factor receptor could play a prognostic role to predict the outcome of nasopharyngeal carcinoma: a meta-analysisCancer Biomark201414426727724934370
- LuoGLongJQiuLLiuCXuJYuXRole of epidermal growth factor receptor expression on patient survival in pancreatic cancer: a meta-analysisPancreatology201111659560022261712
- GuoYMYuWWZhuMGuoCYClinicopathological and prognostic significance of epidermal growth factor receptor overexpression in patients with esophageal adenocarcinoma: a meta-analysisDis Esophagus201528875075624961755
- HongLHanYYangJPrognostic value of epidermal growth factor receptor in patients with gastric cancer: a meta-analysisGene20135291697223954221
- Reis-FilhoJSFaoroLNCarrilhoCBleggi-TorresLFSchmittFCEvaluation of cell proliferation, epidermal growth factor receptor, and bcl-2 immunoexpression as prognostic factors for patients with World Health Organization grade 2 oligodendrogliomaCancer200088486286910679656
- Bouvier-LabitCChinotOOchiCGambarelliDDufourHFigarella-BrangerDPrognostic significance of Ki67, p53 and epidermal growth factor receptor immunostaining in human glioblastomasNeuropathol Appl Neurobiol19982453813889821169
- SmithJSTachibanaIPasseSMPTEN mutation, EGFR amplification, and outcome in patients with anaplastic astrocytoma and glioblastoma multiformeJ Natl Cancer Inst200193161246125611504770
- DorwardNLHawkinsRAWhittleIREpidermal growth factor receptor activity and clinical outcome in glioblastoma and meningiomaBr J Neurosurg1993721971998388222
- JiangHRenXZhangWA new prognostic scoring scale for patients with primary WHO grade III gliomas based on molecular predictorsJ Neurooncol2013111336737523269453
- JarosEPerryRHAdamLPrognostic implications of p53 protein, epidermal growth factor receptor, and Ki-67 labelling in brain tumoursBr J Cancer19926623733851503912
- ZhuAShaefferJLeslieSKolmPEl-MahdiAMEpidermal growth factor receptor: an independent predictor of survival in astrocytic tumors given definitive irradiationInt J Radiat Oncol Biol Phys19963448098158598357
- SaitoTHamaSKajiwaraYPrognosis of cerebellar glioblastomas: correlation between prognosis and immunoreactivity for epidermal growth factor receptor compared with supratentorial glioblastomasAnticancer Res2006262b1351135716619544
- TiniPBelmonteGToscanoMCombined epidermal growth factor receptor and beclin1 autophagic protein expression analysis identifies different clinical presentations, responses to chemo- and radiotherapy, and prognosis in glioblastomaBiomed Res Int2015201520807625821789
- KorshunovAGolanovASychevaRImmunohistochemical markers for prognosis of cerebral glioblastomasJ Neurooncol200258321723612187957
- HurttMRMoossyJDonovan-PelusoMLockerJAmplification of epidermal growth factor receptor gene in gliomas: histopathology and prognosisJ Neuropathol Exp Neurol199251184901311022
- ZhaoLLXuKLWangSWHuBLChenLRPathological significance of epidermal growth factor receptor expression and amplification in human gliomasHistopathology201261472673622978472
- DehaisCLaigle-DonadeyFMarieYPrognostic stratification of patients with anaplastic gliomas according to genetic profileCancer200610781891189716986124
- KorshunovASychevaRGolanovAThe prognostic relevance of molecular alterations in glioblastomas for patients age <50 yearsCancer2005104482583215981281
- HouillierCLejeuneJBenouaich-AmielAPrognostic impact of molecular markers in a series of 220 primary glioblastomasCancer2006106102218222316568472
- JainRPoissonLMGutmanDOutcome prediction in patients with glioblastoma by using imaging, clinical, and genomic biomarkers: focus on the nonenhancing component of the tumorRadiology2014272248449324646147
- LayfieldLJWillmoreCTrippSJonesCJensenRLEpidermal growth factor receptor gene amplification and protein expression in glioblastoma multiforme: prognostic significance and relationship to other prognostic factorsAppl Immunohistochem Mol Morphol2006141919616540738
- HobbsJFardoDWCieplyKDacicSHamiltonRLHorbinskiCGlioblastoma survival varies according to degree of EGFR amplificationNeuro Oncol201113iii92
- CostaBMViana-PereiraMFernandesRImpact of EGFR genetic variants on glioma risk and patient outcomeCancer Epidemiol Biomarkers Prev201120122610261721960689
- LiBZhaoWLiJEffect of epidermal growth factor receptor gene polymorphisms on prognosis in glioma patientsOncotarget2016739630546306427437777
- TrabelsiSChabchoubIKsiraIMolecular diagnostic and prognostic subtyping of gliomas in Tunisian populationMol Neurobiol20175442381239426957305
- BredelMPollackIFHamiltonRLJamesCDEpidermal growth factor receptor expression and gene amplification in high-grade non-brainstem gliomas of childhoodClin Cancer Res1999571786179210430083
- GanigiPMSantoshVAnandhBChandramouliBASastry KolluriVRExpression of p53, EGFR, pRb and bcl-2 proteins in pediatric glioblastoma multiforme: a study of 54 patientsPediatr Neurosurg200541629229916293948
- ChenJRXuHZYaoYQinZYPrognostic value of epidermal growth factor receptor amplification and EGFRvIII in glioblastoma: meta-analysisActa Neurol Scand2015132531032225846813
- AnilRColenRRImaging genomics in glioblastoma multiforme: a predictive tool for patients prognosis, survival, and outcomeMagn Reson Imaging Clin N Am201624473174027742113
- PreusserMGelpiERottenfusserAEpithelial growth factor receptor inhibitors for treatment of recurrent or progressive high grade glioma: an exploratory studyJ Neurooncol200889221121818458820