
Abstract
Extrapulmonary small cell neuroendocrine carcinoma (SNEC) is an extremely rare and highly malignant tumor with a poor prognosis. Multiple metastases of SNEC are even more rare, and patients with locally advanced and metastatic disease generally face a poor outcome. To date, only a few cases of SNEC have been reported. Here, we describe a rare case of a 70-year-old female patient with SNEC of the tonsil who presented with multiple metastases and had achieved a complete response (CR) of the primary lesion and cervical lymph nodes for more than 1 year after receiving palliative chemotherapy. Initially, the patient presented with a 2-month history of throat pain. Magnetic resonance imaging and computed tomography revealed a soft mass with moderate enhancement on the left tonsil, which was confirmed by incisional aspiration biopsy. She was additionally sent for a positron emission tomography scan to evaluate small metastases in the left cervical lymph node, right lung, multiple mediastinal lymph nodes, and the fourth lumbar (L4) vertebra body metastases. Histopathological examination of the SNEC confirmed a nested, typical endocrine appearance with small round cells containing ovoid-shaped nuclei and high mitotic activity. Immunohistochemically, the tumor cells were positive for cytokeratin 8/18+, synaptophysin+, CD56+, and Ki-67 (<50%). The patient received 6 cycles of cisplatin combined with etoposide and was subsequently placed under close observation (<12 months). To date, she has achieved a CR of the primary lesion and cervical lymph nodes. In summary, we have described a case of successful treatment after chemotherapy for SNEC and have elucidated professional knowledge regarding the relevant aspects of SNEC.
Introduction
Neuroendocrine carcinomas are included among the heterogeneous group of the malignant small cell tumors, which also include carcinoid, atypical carcinoid, and small cell carcinoma. Small cell neuroendocrine carcinoma (SNEC) is a highly invasive neuroendocrine tumor that commonly originates in the pulmonary tissue, whereas extrapulmonary SNEC accounts for only 2.5%–5% of cases.Citation1,Citation2 Despite the extreme rarity of extrapulmonary SNEC, sinonasal, laryngeal, cervix, parotid, and even lower gingival tumors have been reported.Citation3–Citation5 Many of the reported cases involved high-grade carcinomas, a highly invasive form of cancer with distant metastasis.Citation6 Some smaller series have reported that 14.5%–25% of patients present with distant metastatic disease.Citation7,Citation8 Patients with a locally advanced stage and metastatic disease often have a low median survival rate, according to previous reports.Citation9
To date, reports of a patient with multiple metastases of SNEC have been rare. Additionally, such cases have not previously involved the head and neck. Therefore, clinical research is scarce, especially with regard to the point of treatment. In this report, we describe our experience with the successful achievement of a complete response (CR) of the primary tumor and cervical lymph nodes in a woman with extrapulmonary SNEC.
Case report
In May 2016, a 70-year-old woman with no history of smoking was referred to the hospital with a 2-month history of persistent throat pain which had been accompanied by disordered eating for 1 week. Her medical history included long-term hypertension and type 2 diabetes mellitus. At admission, a physical examination revealed a tender mass in the left tonsil () and a 1.1×1.3 cm lymph node at the left-side level II upon careful neck palpation. All other head and neck findings were normal. All laboratory data were within the normal limits.
Figure 1 Laryngoscopy image showing a tender mass in the left tonsil (arrow).

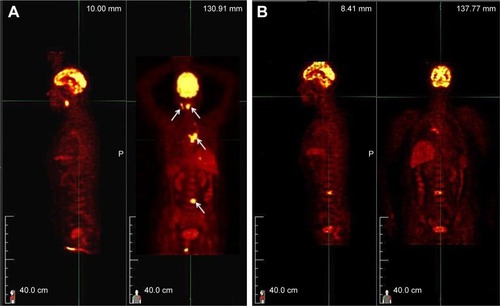
Magnetic resonance imaging (MRI) of the oropharyngeal region revealed a well-defined oval-shaped mass lesion measuring 2.5×2×1.2 cm on the left tonsil, as well as metastatic enlargement of the cervical lymph nodes (). A computed tomography (CT) scan of the chest revealed a polypoidal lesion in the upper lobe of the right lung and enlargement of the multiple mediastinal lymph nodes. Additionally, positron emission tomography (PET)-CT identified a heterogeneously enhanced and highly metabolic mass lesion on the left tonsil, as well as metastatic spread to the right lung, mediastinal lymph nodes, left cervical lymph node, and fourth lumbar (L4) vertebra body ().
Figure 2 Oropharyngeal magnetic resonance images obtained before (A) and after (B) treatment. The images depict a complete regression of the left tonsillar mass after 1 month of chemotherapy (arrows).
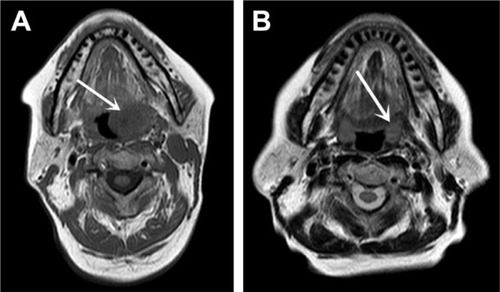
Figure 3 Positron emission tomography scans obtained before (A) and after (B) chemotherapy reveal decreases in hypermetabolism in the primary lesion and metastases (arrows).
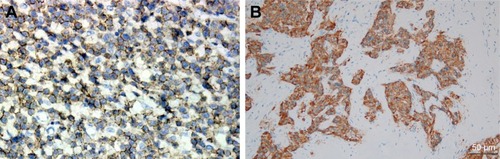
A biopsy specimen was then collected from the primary lesion under local anesthesia. Pathological findings of the lesion in the left tonsil confirmed a single tumor type. Histologically, the biopsy specimens of the primary lesion revealed small round-to-oval-shaped tumor cells scattered in irregular nests (). At high magnification, these malignant neoplasms were found to have crowded nuclei with hyperchromatism and scant cytoplasm (). The immunohistochemistry findings were as follows: the cells showed positivity for synaptophysin, CD56, and cytokeratin 8/18 and negativity for vimentin, S-100, CD10, and P63 (), as well as a Ki-67 proliferation index of >50% (+).
Figure 4 Pathological findings of hematoxylin and eosin-stained tumor sections.
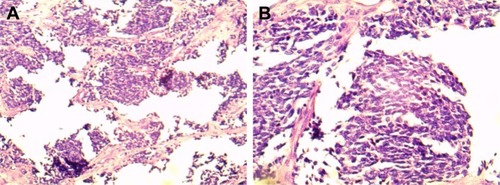
Figure 5 The tumor cells exhibited positive immunoreactivity for (A) CD56 and (B) synaptophysin (magnification: 200×).
From the medical history, clinicopathologic data, and PET-CT findings, the abnormalities in the lymph nodes and L4 vertebral body were considered to be metastatic carcinomas. Accordingly, a final diagnosis of SNEC with multiple metastases was confirmed. The patient refused surgery and radiotherapy and was administered 6 cycles of adjuvant chemotherapy comprising 60 mg/m2 etoposide on days 1–3 and 50 mg/m2 cisplatin on day 1 at 21-day intervals. MRI of the oropharyngeal region verified an excellent tumor response after 1 month of treatment (). PET-CT revealed significant decreases in the standardized uptake value (SUV) of the fluorodeoxyglucose tracer () in the right lung and L4 vertebra body, as well as a decrease in the SUV of the primary lesion from 8.7 to 1.9. Surprisingly, the patient has been followed regularly for 1 year and has achieved a CR of the tonsil and cervical lymph node lesions.
Discussion
As noted above, primary SNEC is an unusual type of neuroendocrine tumor, particularly in the head and neck, and is rarely described in the literature. SNEC accounts for only 11%–16% of all extrapulmonary small cell carcinomas,Citation2 and oropharyngeal tumors account for only 12.3% of all cancers in the head and neck.Citation6 SNEC often presents in older patients (age: 50–66 years) without sex bias; however, the majority of cases in the tonsil involve male patients, with a male to female ratio of 1.75:1.Citation10 Therefore, our current case is not consistent with the existing pattern.
The clinical symptoms of SNEC vary, although patients commonly experience pain, dysphagia, and obstructive sleep apnea syndrome. In the present case, the patient only experienced throat pain without specific clinical characteristics and was misdiagnosed with a peritonsillar abscess. Given these nonspecific symptoms and broad clinical spectrum of manifestation, the diagnosis of SNEC mainly depends on a histologic and immunohistochemical examination.Citation11,Citation12 Here, the expression of neuroendocrine markers such as synaptophysin, CD56, and chromogranin A will facilitate a diagnosis.Citation13 In the present case, the tumor met the necessary histological criteria and exhibited high levels of synaptophysin, CD56, and Ki-67 upon immunohistochemical analysis.
Previously, SNEC has been observed to follow a short course and tend to metastasize at an early stage, in contrast to other head and neck cancers.Citation14 To the best of our knowledge, only 15 cases of SNEC of the tonsil have been reported in the English literature, of which 9 had metastasized from primary sites.Citation6,Citation10 Accordingly, few data are available concerning primary tumors of the head and neck with multiple metastases.
Image detection plays an important role in the diagnosis of head and neck lesions, particularly in the exclusion of regional invasion or distant metastasis. PET-CT is highly valuable for diagnosis and treatment planning because it can confirm the presence of both the primary tumor and metastatic lesions based on tracer uptake.Citation15 In this case, PET-CT confirmed a metabolically active mass on the left tonsil, as well as extensive metastases affecting the right lung, mediastinal lymph nodes, left cervical lymph node, and L4 vertebral body. Last but not least, PET-CT can be used as the primary means of evaluating the effects of treatment.Citation16,Citation17
Kao et al reported a 5-year relative survival of only 20.8% among SNEC patients.Citation18 The rarity of SNEC of the oropharyngeal region and relatively worse prognosis when compared to other cancers affecting this region have hindered the identification of treatments that effectively improve survival. Currently, SNEC is mainly treated via surgical excision,Citation6 although other treatments may be required depending on the tumor size, location, and systemic condition of the patient. In the present case, treatment planning is based on the poor general condition and preferences of the patient and the locations of primary and metastatic lesions. Previously, Johnson et al concluded that etoposide is among the most active agents against small cell lung cancer,Citation19 and another study found a new therapeutic option for lung neuroendocrine tumors.Citation20 In the present case, the patient received 6 courses of etoposide-cisplatin chemotherapy. Following this regimen, she has achieved a CR for more than 1 year and experiences an excellent quality of life.
Conclusion
SNECs of the tonsil are rare and have not previously been reported with multiple metastases. Our findings suggest that an etoposide-based multiagent chemotherapy regimen could be an effective therapeutic strategy for unresectable SNEC in the head and neck region.
Acknowledgments
Our study received approval from the ethics committee of the Affiliated Xuzhou Hospital, College of Medicine, Southeast University. The patient and family members also provided written informed consent to publish the case report details. This study was supported by Jiangsu Province Medical Youth Talent Project (QNRC2016390) and Xuzhou Medical Creative Team Program (XWCX201604).
Disclosure
The authors report no conflicts of interest in this work.
References
- RemickSCRuckdeschelJCExtrapulmonary and pulmonary small-cell carcinoma: tumor biology, therapy, and outcomeMed Pediatr Oncol199220289991310345
- RennerGSmall cell carcinoma of the head and neck: a reviewSemin Oncol200734131417270660
- ChaiLYingHFWuTTClinical features and hypoxic marker expression of primary sinonasal and laryngeal small-cell neuroendocrine carcinoma: a small case seriesWorld J Surg Oncol20141219924980293
- GanesanRHirschowitzLDawsonPNeuroendocrine carcinoma of the cervix: review of a series of cases and correlation with outcomeInt J Surg Pathol201624649049627098591
- ZengMYangSDZhangJLChenXMPrimary small cell neuroen-docrine carcinoma of the oral cavity: a case report and review of the literatureOncol Lett201510288789026622589
- PointerKBKoHCBrowerJVSmall cell carcinoma of the head and neck: an analysis of the National Cancer DatabaseOral Oncol201769929828559027
- AguilarEA3rdRobbinsKTStephensJDimeryIWBatsakisJGPrimary oat cell carcinoma of the larynxAm J Clin Oncol198710126323030091
- HatoumGFPattonBTakitaCSmall cell carcinoma of the head and neck: the university of Miami experienceInt J Radiat Oncol Biol Phys200974247748119004574
- VermorkenJBMesiaRRiveraFPlatinum-based chemotherapy plus cetuximab in head and neck cancerN Engl J Med2008359111116112718784101
- WangHYZouJZhouGYYanJQLiuSXPrimary small cell neu-roendocrine carcinoma of the tonsil: a case report and review of the literatureInt J Clin Exp Pathol2014752678268224966986
- LamAKUpdate on Adrenal Tumours in 2017 World Health Orga-nization (WHO) of endocrine tumoursEndocr Pathol201728321322728477311
- XuBChettyRPerez-OrdoñezBNeuroendocrine neoplasms of the head and neck: some suggestions for the new WHO classification of head and neck tumorsHead Neck Pathol201481243224595420
- ThompsonLWorld Health Organization classification of tumours: pathology and genetics of head and neck tumoursEar Nose Throat J20068527416579185
- DuanYFTanYYuanBZhuFSpontaneous rupture of hepatic metastasis from small cell neuroendocrine carcinoma of maxillary sinusWorld J Surg Oncol20141212624767405
- ChenXHBaoYYZhouSHWangQYZhaoKPalatine tonsillar metastasis of small-cell neuroendocrine carcinoma from the lung detected by FDG-PET/CT after tonsillectomy: a case reportIran J Radiol201310314815124348600
- SchoutenCSde GraafPAlbertsFMResponse evaluation after chemoradiotherapy for advanced nodal disease in head and neck cancer using diffusion-weighted MRI and 18F-FDG-PET-CTOral Oncol201551554154725725587
- JohnsonJTBranstetterBF4thPET/CT in head and neck oncology: state-of-the-art 2013Laryngoscope2014124491391524515562
- KaoHLChangWCLiWYChia-Heng LiAFen-Yau LiAHead and neck large cell neuroendocrine carcinoma should be separated from atypical carcinoid on the basis of different clinical features, overall survival, and pathogenesisAm J Surg Pathol201236218519222082601
- JohnsonDHHainsworthJDHandeKRGrecoFACurrent status of etoposide in the management of small cell lung cancerCancer1991671 Suppl2312441845846
- MalapelleUMorraFIlardiGUSP7 inhibitors, downregulating CCDC6, sensitize lung neuroendocrine cancer cells to PARP-inhibitor drugsLung Cancer2017107414927372520