
Abstract
Purpose
The great efficacy of EGFR tyrosine kinase inhibitors (EGFR-TKIs) has been identified in patients with advanced non-small-cell lung cancer (NSCLC) who harbor EGFR mutations. However, it has not yet been established in postoperative adjuvant therapy.
Patients and methods
To compare the prognosis and toxicity of EGFR-TKI-based adjuvant therapy and non-EGFR-TKI-based adjuvant therapy in resected NSCLC with sensitive EGFR mutations, we performed this meta-analysis of all eligible randomized controlled trials (RCTs).
Results
A comprehensive literature search of electronic databases (from inception to December 31, 2017) was performed. Additionally, abstracts presented at the American Society of Clinical Oncology conferences and World Conference on Lung Cancer held between January 2000 and November 2017 were searched to identify relevant trials. Disease-free survival (DFS), overall survival (OS), and grade 3 or 4 toxicities were analyzed. Five RCTs were selected, and 560 participants were included. This meta-analysis demonstrated that EGFR-TKI-based adjuvant therapy was associated with better DFS compared with non-EGFR-TKI-based therapy (HR =0.52, 95% CI 0.34–0.78, P=0.002). Pooled estimate has showed the trend of superiority of EGFR-TKI-based therapy in the aspect of OS (HR =0.65, 95% CI 0.22–1.91, P=0.43); however, the difference was not significant. The incidence rate of grade 3–4 toxicities of EGFR-TKI-based regimens was significantly higher for rash (OR =10.17, 95% CI 2.37–43.63, P=0.002) but lower for vomiting (OR =0.08, 95% CI 0.01–0.61, P=0.02).
Conclusion
EGFR-TKI-based therapy was associated with better DFS compared with non-EGFR-TKI-based adjuvant therapy in patients with NSCLC harboring EGFR mutations. A trend was found that EGFR-TKI-based regimen improved the OS, though the difference was not significant. Although more OS data are needed, EGFR-TKI-based treatment has the potential to be an alternative of adjuvant therapy for NSCLC with a sensitive EGFR mutation.
Introduction
Lung cancer is one of the most common cancers and remains the leading cause of cancer-related death worldwide.Citation1,Citation2 At present, standard postoperative therapy for non-small-cell lung cancer (NSCLC) is platinum-based chemotherapy, supplemented by radiotherapy.Citation3 Although the result from a meta-analysis containing 35 trials confirmed that adjuvant chemotherapy improved 5-year survival, only 64% of patients survived 5 years after surgery.Citation4 The adverse effects of cytotoxic agents limit its application. Efforts to improve patient’s survival are currently concentrated on innovative targeted therapies directed against signaling pathways involved in the proliferation, growth, and invasion of tumor cell. EGFR tyrosine kinase inhibitors (EGFR-TKIs) would be an attractive alternative, but their efficiency and toxicities for the treatment of resected NSCLC with sensitive EGFR mutations are still obscure as compared with platinum-based chemotherapy.
The most common mutations of EGFR are divided into sensitive mutations (such as EGFR exon 19 deletions and exon 21 L858R activating mutation) and resistant mutation (EGFR exon 20 T790M point mutation). The role of first-generation of EGFR-TKIs including gefitinib, erlotinib, and icotinib has been identified in patients with advanced NSCLC.Citation5–Citation9 However, they have not yet been established in adjuvant therapy.
There were several randomized controlled trials (RCTs) investigating EGFR-TKIs based treatment vs non-EGFR-TKIs based therapy for the purpose to evaluate these two strategies in adjuvant treatment of NSCLC, whereas inconsistencies were found in previous trials.Citation10–Citation12 Until recently, head-to-head research studies such as the ADJUVANT studyCitation13 and EVAN studyCitation14 focus on sensitive EGFR mutants’ cohorts and reported surprising results. To compare the efficacy, prognosis, and toxicity of EGFR-TKI-based adjuvant therapy and non-EGFR-TKI-based adjuvant therapy for NSCLC with EGFR activating mutations, we performed this meta-analysis.
Methods
Search strategy
We searched PubMed, Embase, Web of Science, and Cochrane Database for RCTs from inception to December 31, 2017. Additionally, abstracts presented at the American Society of Clinical Oncology (ASCO) conferences and World Conference on Lung Cancer (WCLC) held between January 2000 and December 2017 were searched to identify relevant trials, using the following search terms: 1) “non-small-cell lung cancer” or “non-small cell lung neoplasms” or “carcinoma, non-small-cell lung” or “NSCLC” or “lung adenocarcinoma”; 2) “epidermal growth factor receptor tyrosine kinase inhibitors” or “gefitinib” or “erlotinib” or “icotinib” or “afatinib”; and 3) “adjuvant therapy” or “adjuvant treatment” or “adjunctive treatment” or “adjunctive therapy”. Two authors (J-XW and QH) independently completed the tasks, if there were any disagreements; they were resolved by discussions among the other authors.
Inclusion and exclusion criteria
In this meta-analysis, we collected all eligible articles about RCTs comparing EGFR-TKI-based and non-EGFR-TKI-based adjuvant therapies in postoperative NSCLC patients who harboring sensitive EGFR mutations. Studies meeting the following inclusion criteria were included: 1) patients suffering from histological confirmed, completely resected NSCLC at baseline; 2) Phase II or Phase III RCT; 3) trials comparing EGFR-TKI-based and non-EGFR-TKI-based regimens given as adjuvant therapy and not confounded by additional interventions; and 4) if there were multiple articles based on similar patients, only the largest or the most recently article was included. The exclusion criteria included the following: 1) letters, reviews, case reports, editorials, and expert opinion and 2) nonprospective trials.
Data extraction
For each study, the following characteristics were extracted: the last name of the first author, year of publication, country, study design and period, duration of EGFR-TKI treatment, case number, follow-up time, regimen, ClinicalTrials.gov identifier, disease-free survival (DFS), overall survival (OS), and grade 3 or 4 toxicities (including rash, diarrhea, anorexia, nausea, vomiting, fever, anemia, leucopenia, and fatigue). If the HR or standard errors (SEs) were not reported in included studies, we calculate or estimate the HR from available data or Kaplan–Meier curves using the methods reported by Tierney et al.Citation15
Validity assessment
The risk of confounding and the design quality of selected studies were evaluated by two reviewers (QH and J-XW). We assessed the methodological quality of all eligible RCTs by the Cochrane Collaboration’s tool for assessing the risk of bias. This quality result was used as the basis for sensitivity analysis.
Statistical analysis
We executed and reported our findings in accordance with the PRISMA statements.Citation16,Citation17 DFS was determined from the date of operation to the date of tumor recurrence. The definition of OS was the time from random assignment to death from any cause, censoring patients who had not died at the date last known alive. Toxicity was assessed by the National Cancer Institute Common Terminology Criteria for Adverse Events.
Analysis was performed using the Review Manager 5.2 (Cochrane Collaboration, Oxford, UK) and Stata 12.0 (StataCorp LP, College Station, TX, USA). Comparison of dichotomous outcomes (toxicity) was performed by pooled estimates of ORs, together with their 95% CIs. The DFS and OS analyses were calculated with HR and 95% CI for HR. All the P-values were two sided, and P<0.05 was considered to be statistically significant.
Heterogeneity was tested using the chi-squared test with significance being set at P<0.10. The total variation among studies was estimated by I2, where ICitation2>50% was considered to indicate significant heterogeneity. If there was heterogeneity among studies, we used a random effect model to pool the OR. Otherwise, a fixed effect model was selected.
A sensitivity study was performed to identify any individual study that significantly affected the overall estimates by omitting each study repeatedly and calculating the pooled estimates for the remaining studies.
Publication bias was investigated through funnel plots and tested using Begger’s and Egger’s tests. We considered there to be publication bias if the intercept of the Egger’s regression line deviated from zero with a two-sided P-value of less than 0.10.
Results
The baseline characteristics of the eligible studies
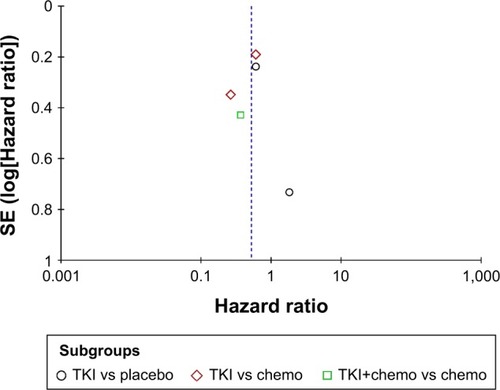
Five RCTs, including fourCitation10–Citation13 published and oneCitation14 unpublished studies, which involved a total of 560 patients, were eligible for analysis. A total of 301 patients were randomized to EGFR-TKI-based therapy, while 259 patients were randomized to non-EGFR-TKI-based regimens. The drugs used in the trials included gefitinib, erlotinib, cisplatin, vinorelbine, carboplatin, and pemetrexed. According to therapeutic strategies, enrolled studies can be divided into three subgroups, EGFR-TKI vs placebo, EGFR-TKI with chemotherapy vs chemotherapy, and EGFR-TKI vs chemotherapy. RCTs conducted by Goss et alCitation10 and Kelly et alCitation11 contrasted EGFR-TKI with placebo. However, the trial by Li et alCitation12 investigated the therapy of EGFR-TKI with chemotherapy and chemotherapy alone. In addition, two latest studiesCitation13,Citation14 compared EGFR-TKI directly with platinum-based chemotherapy. Only the data meeting the inclusion criteria were taken into current analysis. Flow chart of study selection is shown in , and the characteristics of these trials are listed in .
Table 1 Baseline characteristics of included studies
Figure 1 Flow chart for selection of studies.
DFS
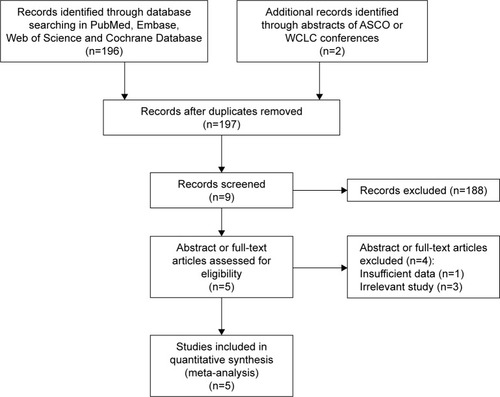
A total of 560 patients from five trials were recruited. The heterogeneity test for DFS indicated that a random effect model should be selected (I2=51%, P=0.08). The meta-analysis showed that the pooled HR was 0.52 (95% CI 0.34–0.78), and statistical significance was identified in terms of DFS (P=0.002, ).
Figure 2 Forest plot of hazard ratio for disease-free survival of resected non-small-cell lung cancer with EGFR mutations.
In subgroup analysis, the stratified group based on different therapeutic strategies revealed that elevated DFS were still observed except in the subgroup of EGFR-TKI vs placebo (HR =1.41, 95% CI 0.58–3.43, P=0.45, ).
OS
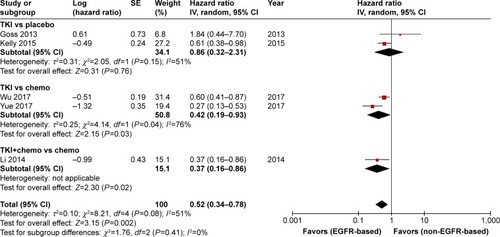
Four trials were eligible for the analysis of OS. No significant OS benefit was observed from EGFR-TKI-based adjuvant therapy in NSCLC (HR =0.65, 95% CI 0.22–1.91, P=0.43, ). Comparison was performed under the random-effects model, because the heterogeneity was observed (P=0.01, I2=73%).
Figure 3 Forest plot of hazard ratio for OS of resected non-small-cell lung cancer with EGFR mutations.
In subgroup analysis, improved OS was found in the subgroup of EGFR-TKI vs chemotherapy (HR =0.17, 95% CI 0.05– 0.58, P=0.005, ), which included only one research.
Toxicities
The results of toxicities are listed in (forest plots not shown). Only grade 3 or greater adverse events (AEs) were collected. In EGFR-TKI-based regimen, the common severe AEs were rash (incidence 8.4%; OR =10.17, 95% CI 2.37–43.63) and diarrhea (incidence 2.8%; OR =3.88, 95% CI 0.82–18.23). Leukopenia (10.0%) and vomiting (4.8%) were the top two AEs of non-EGFR-TKI-based therapy. Other severe toxicities were not significantly different between these two arms, except for rash and vomiting.
Table 2 Outcome of toxicity meta-analysis comparing EGFR-TKI-based therapy vs non-EGFR-TKI-based therapy as adjuvant treatment in advanced NSCLC
Sensitivity analysis and publication bias
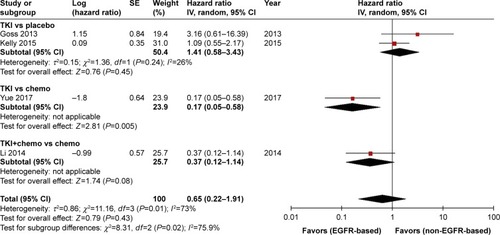
In sensitivity analysis, the corresponding pooled ORs and HRs were not significantly altered, suggesting the stability of our results. No publication bias was observed in the meta-analysis. We showed funnel plots of DFS (Begg’s test P=1.000 and Egger’s test P=0.986, ).
Figure 4 Funnel plot of publication bias of hazard ratio for disease-free survival in the meta-analysis.
Discussion
A meta-analysisCitation18 performed in 2015 assessing the efficacy of EGFR-TKIs in adjuvant therapy of NSCLC showed that there was significant DFS benefit in favor of EGFR-TKI-based treatment. Recently, results of two RCTs (NCT1405079 and NCT1683175)Citation13,Citation14 provide latest data to evaluate the role of EGFR-TKIs in postoperative treatment. With the updated data, we enhanced the results of previous meta-analysis in mutant participants.
Most included RCTs display increased DFS by treatment based on EGFR-TKIs, except the research of BR21 by Goss et al.Citation10 As shown in , HR value of DFS for patients with EGFR mutations in this study is greater than 1 and the squares are located on the right side of the vertical line corresponding to the value 1 on the abscissa (HR =1.84; 95% CI 0.44–7.70). The small sample size (only 15 patients had EGFR mutations) might lead to this negative result. Besides the early closure of the study resulted in a shorter treatment duration for EGFR-TKI, which might also be the reason for the failure to obtain a positive outcome.
Our meta-analysis suggested that DFS in the EGFR-TKI group is superior to non-EGFR-TKI group, consistent with previous meta-analysis.Citation18 The difference between current research and previous meta-analysis lies in the design of study: trials we included are all RCTs, only patients with EGFR-sensitive mutations were selected, and results of two head-to-head research studies were added. However, previous meta-analysis did not select a specific population and the eligible studies included two retrospective research studies.Citation19,Citation20
A trial by Feng et alCitation21 suggested that chemotherapy with orally icotinib displayed better DFS compared with chemotherapy only, yet the statistic difference in DFS was not significant. In this trial, the time (4–8 months) of icotinib treatment was too short to calculate the HR, which was the reason that led to the absence of significant differences and why we did not include this study. However, a retrospective study,Citation22 which analyzed 20 patients with 30 months median follow-up time, had demonstrated that the 2-year DFS rate was 85%; therefore, we still cannot negate the efficacy of icotinib in adjuvant therapy.
Current analysis confirmed that there was no OS benefit with EGFR-TKI-based regimens in adjuvant treatment. A total of 338 patients in four trials provided the OS data (). Insufficient sample size might result in the inability to detect differences between EGFR-TKI-based and non-EGFR-TKI-based therapies. Otherwise various subsequent treatments in relapsed patients may also blur the distinction of OS. Heterogeneity was found among the four trials, which might be caused by difference in characters of patients, regimens, and follow-up time. Various and insufficient data might have produced possible clinical heterogeneity. However, the conclusion was supported by the sensitivity analyses.
A subgroup analysis based on different therapeutic strategies was also performed. Because only five RCTs were enrolled, the subgroup analyses relied on a small number of subjects. Elevated DFS was still observed except in the subgroup of TKI vs placebo. In this subgroup, only 15 patients were included in the study by Goss et al.Citation10 Improved OS was only found in the subgroup of TKI vs chemotherapy, which included only one research. Small sample size may be the cause of discordant results.
Significant prominent grade 3–4 rashes in EGFR-TKI-based therapy and vomiting in non-EGFR-TKI-based therapy were observed in our analysis, where as equivalent tolerance was found regard to other grade 3–4 hematological and non-hematological toxicities. The result was similar to previous meta-analysis.Citation18 Though most enrolled patients in the non-EGFR-TKI-based group received chemotherapy, leucopenia, anorexia, nausea, and anemia were not observed more common. The result was beyond our expectation, which may be due to the small sample size, different compatibility of agents.
Efforts were made to conduct a comprehensive analysis, but limitations of our analysis still should be acknowledged. First, the compatibility of agents was quite different among studies, no matter in EGFR-TKI-based arms or non-EGFR-TKI-based arms. EGFR-TKIs were not only compared with placebo or chemotherapy head-to-head but also be added to chemotherapy to found the effect of the supplement. It increased the difficulty for assessing the role of EGFR-TKI in adjuvant therapy of NSCLC. Though subgroup analysis was performed, the results were still limited because of small sample size. Second, the treatment time of EGFR-TKIs was not enough. In the trial by Li et al,Citation12 gefitinib was administered for only 6 months. Besides, the median treatment duration in the BR19 (4.8 months)Citation10 and RADIANT (11.9 months),Citation11 trials was much shorter than planned. Insufficient administration of EGFR-TKI may lead to the underestimation of its efficacy. Third, imbalance between arms of study was observed. The differences found in patient characteristics would cause bias, such as there were more patients in the erlotinib arm with stage IB NSCLC and more patients in the placebo arm with stage IIIA disease in the RADIANT trial.Citation11
Conclusion
Our meta-analysis indicated that EGFR-TKI-based therapy was associated with better DFS compared with non-EGFR-TKI-based therapy as adjuvant treatment for NSCLC harboring sensitive EGFR mutations. A trend was found that EGFR-TKI-based regimen improved the OS, though the difference was not significant. Although more OS data are needed, EGFR-TKI-based treatment has the potential to be an alternative of adjuvant therapy for NSCLC with a sensitive EGFR mutation. In the future, large sample, longer treatment duration of EGFR-TKI, and high-quality RCTs should be performed to provide more information.
Disclosure
The authors report no conflicts of interest in this work.
References
- ChenWZhengRBaadePDCancer statistics in China, 2015CA Cancer J Clin201666211513226808342
- SiegelRLMillerKDJemalACancer statistics, 2016CA Cancer J Clin201666173026742998
- National Comprehensive Cancer NetworkThe NCCN Clinical Practice Guidelines in Oncology (NCCN guidelines) for Non-Small Cell Lung Cancer. Version 62018 Available from: https://www.nccn.org/professionals/physician_gls/pdf/nscl.pdfAccessed October 3, 2018
- BurdettSPignonJPTierneyJNon-Small Cell Lung Cancer Collaborative GroupAdjuvant chemotherapy for resected early-stage non-small cell lung cancerCochrane Database Syst Rev20153CD011430
- MokTSWuYLThongprasertSGefitinib or carboplatin-paclitaxel in pulmonary adenocarcinomaN Engl J Med20093611094795719692680
- ShepherdFARodrigues PereiraJNational Cancer Institute of Canada Clinical Trials GroupErlotinib in previously treated non-small-cell lung cancerN Engl J Med2005353212313216014882
- ZhouCWuYLChenGErlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 studyLancet Oncol201112873574221783417
- RosellRCarcerenyEGervaisRSpanish Lung Cancer Group in collaboration with Groupe Français de Pneumo-Cancérologie and Associazione Italiana Oncologia ToracicaErlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trialLancet Oncol201213323924622285168
- ShiYZhangLLiuXIcotinib versus gefitinib in previously treated advanced non-small-cell lung cancer (ICOGEN): a randomised, double-blind phase 3 non-inferiority trialLancet Oncol2013141095396123948351
- GossGDO’CallaghanCLorimerIGefitinib versus placebo in completely resected non-small-cell lung cancer: results of the NCIC CTG BR19 studyJ Clin Oncol201331273320332623980091
- KellyKAltorkiNKEberhardtWEAdjuvant Erlotinib Versus Placebo in Patients With Stage IB-IIIA Non-Small-Cell Lung Cancer (RADIANT): A Randomized, Double-Blind, Phase III TrialJ Clin Oncol201533344007401426324372
- LiNOuWYeXPemetrexed-carboplatin adjuvant chemotherapy with or without gefitinib in resected stage IIIA-N2 non-small cell lung cancer harbouring EGFR mutations: a randomized, phase II studyAnn Surg Oncol20142162091209624585406
- ZhongWZWangQMaoWMADJUVANT investigatorsGefitinib versus vinorelbine plus cisplatin as adjuvant treatment for stage II–IIIA (N1–N2) EGFR-mutant NSCLC (ADJUVANT/CTONG1104): a randomised, open-label, phase 3 studyLancet Oncol201819113914829174310
- YueDXuSWangQEfficacy and safety of Erlotinib vs Vinore-lbine/Cisplatin as adjuvant therapy for stage IIIA EGFR mutant NSCLC patients (EVAN, NCT1683175)IASLC 18th World Conference on Lung Cancer2017Yokohama.
- TierneyJFStewartLAGhersiDBurdettSSydesMRPractical methods for incorporating summary time-to-event data into meta-analysisTrials2007811617555582
- LiberatiAAltmanDGTetzlaffJThe PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaborationBMJ2009339b270019622552
- MoherDLiberatiATetzlaffJAltmanDGPRISMA GroupPreferred reporting items for systematic reviews and meta-analyses: the PRISMA statementInt J Surg20108533634120171303
- HuangQLiJSunYWangRChengXChenHEfficacy of EGFR Tyrosine Kinase Inhibitors in the Adjuvant Treatment for Operable Non-small Cell Lung Cancer by a Meta-AnalysisChest201614961384139226836897
- D’AngeloSPJanjigianYYAhyeNDistinct clinical course of EGFR-mutant resected lung cancers: results of testing of 1118 surgical specimens and effects of adjuvant gefitinib and erlotinibJ Thorac Oncol20127121815182223154553
- LvCAnCFengQA Retrospective Study of Stage I to IIIa Lung Adenocarcinoma After Resection: What Is the Optimal Adjuvant Modality for Patients With an EGFR Mutation?Clin Lung Cancer2015166e173e18125958850
- FengSWangYCaiKRandomized Adjuvant Chemotherapy of EGFR-Mutated Non-Small Cell Lung Cancer Patients with or without Icotinib Consolidation TherapyPLoS One20151010e014079426474174
- YaoSZhiXWangRQianKHuMZhangYRetrospective study of adjuvant icotinib in postoperative lung cancer patients harboring epidermal growth factor receptor mutationsThorac Cancer20167554354827766784