Abstract
Malignant pleural mesothelioma is a rare and aggressive malignancy of the pleura correlated with exposure to asbestos, with a medium survival of 11–12 months after diagnosis. A case of a 67-year-old male who had previously worked in the asbestos industry and is a current smoker is reported. The computed tomography evaluation revealed a right pleural mass with pleural thickening, and the pleural biopsy confirmed a diagnosis of malignant pleural mesothelioma. He was treated with chemotherapy consisting of etoposide, paclitaxel, and pegylated liposomal doxorubicin hydrochloride. After completion of chemotherapy, radiologic evaluation confirmed a reduction of pleural thickening and improvement in his symptoms. A complete presentation of each drug formulation and characteristics are also included in this paper. The patient’s follow-up is continuing, and computed tomography reveals stable disease 9 years after initial examination.
Introduction
Malignant pleural mesothelioma (MPM) is a rare and highly aggressive tumor that derives from pluripotential mesothelial cells.Citation1 Histologically, it is divided into three subtypes: epithelioid, which is the most common type, sarcomatoid, and mixed type. The main risk factor of MPM is the exposure to asbestos, a group of crystalline-hydrated silicate minerals that, due to its mineral properties such as thermal and cold resistance, tensile strength, and low cost, are used in a variety of manufacturing goods such as tiles, ceilings, cement products, and fabrics. Asbestos is divided into two groups: the serpentine form composed of spiral fibers (chrysotile), which is suitable for making fabrics, and the amphibole form composed of short and linear fibers (anthophyllite, crocidolite, tremolite, actinolite, and amosite), which is most suitable for the construction of tiles and pipes. It is believed that the amphibole form is more likely to cause chronic irritation that can lead to malignant mesothelioma. To a lesser degree, other risk factors include the exposure to other mineral fibers such as erionite, simian virus 40, and radiation. This type of neoplasm is not correlated with smoking, in contrast to the majority of other types of lung cancers.Citation2,Citation3
MPM demonstrates increasing incidence worldwide especially in industrialized countries, due to previous exposure to asbestos.Citation4 The prognosis of these patients is poor, with a median survival of 11–12 months and only a small proportion of patients surviving 2 years after diagnosis. Differences in survival are associated with environmentally correlated factors such as the duration and quality of asbestos exposure, and are also correlated with age at the time of diagnosis, gender, health status, and histological subtype of the tumor. Poor performance status, advanced age, male sex, and sarcomatoid subtype are all poor prognostic factors.Citation5,Citation6 The disease usually manifests with thoracic pain and dyspnea, and the chest X-ray shows pleural effusion – a widespread pleural thickening and reduction in volume of the hemithorax. Thoracoscopy or open pleural biopsy is necessary for diagnosis.Citation7 The immunochemistry of the biopsy specimen is also very important and can help determine the differential diagnosis between MPM and metastatic lung adenocarcinomas. Markers such as keratin-5, calretinin, podoplanin, and Wilms tumor gene-1 are sensitive for MPM – particularly for the epithelioid and mixed subtypes. In contrast, polyclonal carcinoembryonic antigen, thyroid transcription factor-1, and monoclonal antibody-31 (MOC-31) are markers sensitive for adenocarcinoma but negative for MPM.Citation8 The therapeutic options in patients with MPM usually include surgery, chemotherapy, and adjuvant radiotherapy. In selected patients, multimodality treatment with surgical resection followed by radiation and systemic chemotherapy seems to have benefits, but the standard therapy for advanced-stage patients is still pemetrexed and cisplatin as first-line chemotherapy. However, several other chemotherapy regimens have been used as the first-line treatment alone or in combination, with positive results, indicating possible alternatives.Citation9–Citation13
In the current case presentation, Caelyx® (pegyliertes liposomales doxorubicin; Janssen Pharmaceuticals, Inc., Titusville, NJ) 20 mg was used as the first-line treatment in combination with paclitaxel (175 mg/m2) and etoposide (200 mg/m2 on days one to three), which presented a favorable outcome as a first-line treatment. The characteristics of the three drugs are presented along with the characteristics of the malignant mesothelioma disease. Most recent studies have focused on demonstrating better genetic and molecular events that occur during asbestos exposure with the hope of leading to a new class of anticancer agents.Citation2,Citation4 This paper presents a long-term survivor through the combination of an anthracycline agent, taxane, etoposide, and cyclophosphamide; this combination treatment has previously demonstrated prolonged survival.Citation14
Case presentation
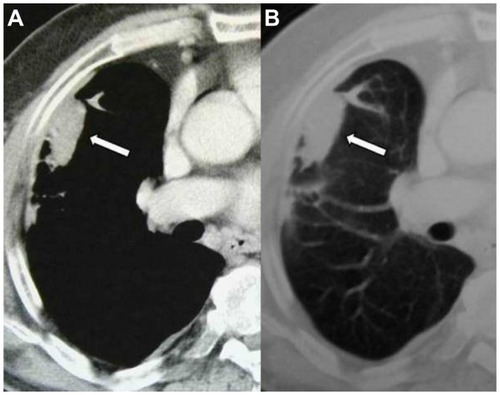
A 67-year-old male pensioner attended the emergency department complaining of chest pain, especially in the right hemithorax, and dyspnea. The symptoms first presented 1 month prior to initial examination. The patient did not mention any cough, hemoptysis, fever, or weight loss. His medical history did not include any comorbidities and he was not taking any medication. The social history demonstrated that the patient was an ex-worker in the asbestos industry and a current smoker (30 cigarettes per day for 47 years). Lung auscultation showed that there was a reduction of respiratory sound in the right lung. The X-ray showed thickening of the right pleura and the patient was sent for a computed tomography (CT) scan. The contrast-enhanced chest CT scan showed a right peripheral pleural mass with pleural thickening and areas with braces, especially in the medium and lower right lobe, with small pretracheal lymph nodes (). Round atelectasis subpleural focuses were revealed in the right medium and lower lobe. An abdomen CT showed a hypodense mass in the right adrenal gland (5 × 3 cm). At this point the possibility of MPM (epithelial) with metastasis in the left adrenal gland was considered. To confirm the diagnosis, thoracoscopy was performed to obtain a pleural biopsy, with a positive result for MPM. A bone scan was also performed and was negative for disease.
Figure 1 Axial computed tomography images of the right lung in the (A) mediastinal and (B) pulmonary window demonstrate the pleural mass corresponding to mesothelioma (initial examination). antigen, and thyroid transcription factor-1. Metastasis in the adrenal gland remained stable. Bone scans and brain CT scans were not pathological. No confirmation was made on the malignancy of the adrenal gland. Pleural thickness at diagnosis was 90 mm × 20 mm, and 40 mm × 15 mm at the end of the first-line treatment. Follow-up has continued for 9 years; the disease is stable without any disease progression.
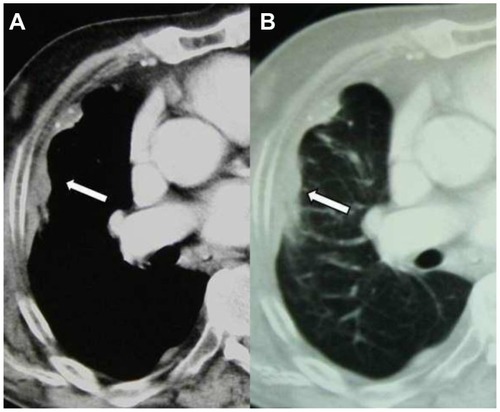
The patient was treated in the authors’ department with eight cycles of paclitaxel (175 mg/m2), pegylated liposomal doxorubicin hydrochloride (Caelyx 20 mg/m2), and etoposide (200 mg/m2), and he continued with three cycles of maintenance therapy with etoposide (100 mg/m2 on days one to five) and three cycles of cyclophosphamide (150 mg/m2 on days one to seven). The patient refused to complete the maintenance therapy and so he entered the follow-up period. The chest CT scans showed a reduction of the pleural thickening, and no pathological lymph nodes were observed (). An additional biopsy was performed 5 years after the initial examination and the immunohistochemistry was positive for the following staining profile: Anti-pan Cytokeratin antibody (AE1/AE3), Wilms tumor gene-1, calretinin, D2-40, negative polyclonal carcinoembryonic
Figure 2 Axial computed tomography images of the right lung in the (A) mediastinal and (B) pulmonary window 9 years after initial examination show that the bulky side of the mesothelioma has slightly decreased.
Discussion
MPM is an uncommon but aggressive tumor of the pleura that is strongly correlated with chronic exposure to asbestos, with prevalence in males. MPM usually invades locally; however, metastases can be observed in the contralateral lung, bones, liver, or peritoneum.Citation15 Patients usually manifest chest pain, dyspnea, and pleural effusion. Imaging examination is very important for diagnosis and during the follow-up period. To confirm the diagnosis, it is necessary to obtain a pleural biopsy with thoracoscopy and to examine the biopsy with immunohistochemistry. There are six types of asbestos fibrous silicates (actinolite, grunerite, anthophyllite, chrysotile, crocidolite, and tremolite). All types of asbestos fibers are capable of causing mesothelioma; however, only three types have been used commercially (white asbestos [chrysotile], brown asbestos [amosite], and blue asbestos [crocidolite]).
MPM incidence has been reported to be increasing in developing industrialized countries; new data indicate an escalation in Brazil, Thailand, and Egypt. In Greece, there is a 2% occupational morbidity attributed to pleural mesothelioma. The disease is still underreported by the national health agencies.Citation16 Until 1995, Greece was one of the world’s top seven suppliers of asbestos (chrysotile). More than 150,000 tons were produced and processed at various asbestos cement factories. Several products such as asbestos-containing brakes and fireproofing materials were also produced in Greece. Blue asbestos usage was banned by law in Greece (article 1154/93) on December 31, 2004; Greece became the last of the 15 European Union member states to ban the use of all forms of asbestos as per the European Union directive.Citation16,Citation17
The patient in the current report was treated with etoposide, paclitaxel, and pegylated liposomal doxorubicin as first-line treatment. This type of doxorubicin is coated with methoxy polyethylene glycol that decreases the interaction of the lipid membrane with the plasma components and with the reticuloendothelial system. The liposomal encapsulation and “stealth” ability has added additional advantages to the drug formulation. This drug formulation increases the half-life of doxorubicin and also the liposomal deposition in the tumor tissue by 100-fold, so drug toxicity is reduced, especially cardiac toxicity and palmar-plantar erythrodysesthesia. Previously published phase I and II studies have shown good tolerance in patients with a dose of 45 mg/m2 Caelyx every 28 days.Citation18,Citation19 A previous study using first-generation anthracyclines presented adverse effects, restricting their usage due to cardiotoxicity and general intolerance.Citation20 The polyethylene glycol coating (dual layer) augmented the efficacy of the drug formulation by adding a sustained-release effect. With this mode of drug release, the concentration of the formulation did not peak instantly after administration and therefore reduced the side effects; however, acute hypersensitivity reaction to the compound has been observed.Citation21 Polymers have the ability to inhibit opsonization of the liposomes by plasma proteins and therefore increase the half-life of liposomal drugs.Citation22–Citation24 Prolonged systemic circulation enhances micrometastasis control. In addition, polyethylene glycol reduces endothelial cell interaction, and in turn the rate of extravasation is reduced.Citation25 Pegylated liposomal doxorubicin is extensively used for the treatment of cancer, especially breast cancer, ovarian cancer, and Kaposi’s sarcoma, and has shown to be an active drug for MPM treatment in phase II studies.Citation9–Citation11,Citation21 Pegylated liposomal doxorubicin should not be disregarded, and should be used as an alternative in patients who cannot tolerate other first-line chemotherapy regimens.
On the other hand, taxanes (paclitaxel, docetaxel) are a group of chemotherapy drugs with antiproliferative action. In particular, they arrest cells in the G2/M phase of the cell cycle, inhibit microtubule depolymerization, and reduce tumor angiogenesis. In addition, it is possible that paclitaxel is able to induce the gene expression of tumor necrosis factor-α, and thus cell death. Taxanes are used with good results in the treatment of locally advanced nonsmall cell lung cancer, in combination with cisplatin or radiotherapy.Citation26 In MPM, taxanes in combination with cisplatin also seem to have good results in inhibiting cell proliferation.Citation27,Citation28 The patient in the current report showed improvement in his symptoms and, after the completion of chemotherapy, a reduction of pleural thickening and elimination of the pathological lymph nodes.
Etoposide (VP1 6-2 13) is a semisynthetic podophyllotoxin derivative and an inhibitor of DNA topoisomerase II. It has the ability to stabilize DNA strand breaks.Citation29 Etoposide has presented favorable results in a variety of malignancies.Citation30 The drug is schedule dependent and acts on the late S and early G2 phases of the cell cycle.Citation31 This compound has demonstrated efficiency in small cell lung cancer and is administered orally or by intravenous infusion.Citation32–Citation34 Modest leukopenia was observed in the oral route of administration.Citation35 In mesothelioma, there are scarce data available of the efficacy of etoposide, nevertheless the European Organization for Research and Treatment of Cancer Lung Cancer Cooperative Group initiative presented efficacy data (intravenous and oral) with two phase II trials.Citation35,Citation36 Data presented in these trials and in another study are in favor of etoposide administered orally for MPM within a combination.Citation35–Citation37
Cyclophosphamide is a nitrogen mustard alkylating agent. It is used in a variety of diseases including cancer and autoimmune disorders. It is converted in the liver from the prodrug to the active chemotherapeutic agent. The cytotoxicity of cyclophosphamide is dose dependent.Citation38 Cyclophosphamide has presented efficacy in combination with cisplatin and doxorubicin in MPM.Citation14,Citation39 Cyclophosphamide has the additional benefit of acting as an immunomodulatory agent. There are published data indicating that this drug formulation sensitizes tumor cells for T cell-mediated, and possibly natural killer cell-mediated, apoptosis.Citation40 Van der Most et al presented data demonstrating that immune sensitization from cyclophosphamide can augment treatment efficiency within combination therapy.Citation40 Nevertheless, there are insufficient data on the proper time of initiation (ie, first-line, second-line).
MPM treatment has evolved during the past 20 years. In a previously published study, patients who received immediately initiated chemotherapy were associated with improved overall survival: 66% at 1 year compared to the “delayed” patients (36%), whose quality of life was less well maintained.Citation12 A new generation of chemotherapy drugs has been studied to improve survival benefits, but only pemetrexed in combination with cisplatin is an efficient first-line treatment, confirmed in phase III trials. This type of chemotherapy is the current standard therapy in advanced MPM.Citation13 Multimodality treatment protocols have demonstrated a median survival of 19–46 months depending on the stage, histology, and completeness of the surgical resection.Citation41–Citation45 In regard to epithelial type, no lymph node involvement and complete surgical resection occasional long-term survival has been observed.Citation41 Local disease control has been achieved with acceptable morbidity and mortality through extrapleural pneumonectomy and adjuvant high-dose hemithoracic irradiation.Citation42,Citation43,Citation46
Conclusion
Despite the progression of clinical treatment, the data for MPM are not yet promising. The main clinical problem is probably the short duration of the response in chemotherapy and the early relapse of the disease due to chemoresistance. Most recent studies have focused on understanding the genetic events that contribute to the process of carcinogenesis from asbestos fibers and the molecular mechanisms responsible for the growth of cancer cells. Asbestos is responsible for the production of nitrogen species and active oxygen that can cause DNA damage and chromosome alterations.Citation3,Citation47 Its fibers may limit drug penetration by causing alterations of the stromal composition in neoplastic tissues.Citation9 A better understanding of the molecular and immune pathways of carcinogenesis in MPM can lead to new targeted drugs and to a better medical treatment of the disease.
Disclosure
The authors report no conflicts of interest in this work. The authors acquired written informed consent from the patient to publish data and figures from his medical file.
References
- SuemitsuRTakeoSHamatakeMFuruyaKUesugiNA case of diffused malignant pleural mesothelioma forming small multiple disseminations with intraoperatively suspicious carcinoid tumorsAnn Thorac Cardiovasc Surg201117329029221697793
- RascoePAJupiterDCaoXLittlejohnJESmytheWRMolecular pathogenesis of malignant mesotheliomaExpert Rev Mol Med201214e1222622048
- MatsuzakiHMaedaMLeeSAsbestos-induced cellular and molecular alteration of immunocompetent cells and their relationship with chronic inflammation and carcinogenesisJ Biomed Biotechnol2012201249260822500091
- PaselloGAltavillaGBonannoLReaFFavarettoAGA pathological complete response after preoperative chemotherapy with carboplatin and pemetrexed in malignant pleural mesothelioma: a case reportJ Thorac Dis20102425422263055
- PintonGManenteAGAngeliGMuttiLMoroLPerifosine as a potential novel anti-cancer agent inhibits EGFR/MET-AKT axis in malignant pleural mesotheliomaPLoS One201275e3685622590625
- van der BijSKoffijbergHBurgersJAPrognosis and prognostic factors of patients with mesothelioma: a population-based studyBr J Cancer2012107116116422644294
- BagheriRHaghiSZRahimMBAttaranDToosiMSMalignant pleural mesothelioma: clinicopathologic and survival characteristic in a consecutive series of 40 patientsAnn Thorac Cardiovasc Surg201117213013621739769
- BettaPGMagnaniCBensiTTrincheriNFOrecchiaSImmunohistochemistry and molecular diagnostics of pleural malignant mesotheliomaArch Pathol Lab Med2012136325326122372901
- ArrietaOMedinaLAEstrada-LobatoEFirst-line chemotherapy with liposomal doxorubicin plus cisplatin for patients with advanced malignant pleural mesothelioma: phase II trialBr J Cancer201210661027103222353806
- GabizonAShmeedaHGrenaderTPharmacological basis of pegylated liposomal doxorubicin: impact on cancer therapyEur J Pharm Sci201245438839821933707
- HillegassJMBlumenSRChengKIncreased efficacy of doxorubicin delivered in multifunctional microparticles for mesothelioma therapyInt J Cancer2011129123324420830711
- SugarbakerDJFloresRMJaklitschMTResection margins, extrapleural nodal status, and cell type determine postoperative long-term survival in trimodality therapy of malignant pleural mesothelioma: results in 183 patientsJ Thorac Cardiovasc Surg1999117154639869758
- VogelzangNJStandard therapy for the treatment of malignant pleural mesotheliomaLung Cancer200550Suppl 1S23S2416291429
- UmsawasdiTDhingraHMCharnsangavejCLunaMAA case report of malignant pleural mesothelioma with long-term disease control after chemotherapyCancer199167148541898706
- ZaudererMGKrugLMThe evolution of multimodality therapy for malignant pleural mesotheliomaCurr Treat Options Oncol201112216317221404104
- AlexopoulosECOccupational health services in Greek hospitalsMed Sci Monit20061210LE20LE2117006411
- GogouEKerenidiTChamosVZintzarasEGourgoulianisKIMesothelioma mortality in Greece from 1983 to 2003Int J Clin Pract200963694494817573841
- NorthfeltDWDezubeBJThommesJAEfficacy of pegylated-liposomal doxorubicin in the treatment of AIDS-related Kaposi’s sarcoma after failure of standard chemotherapyJ Clin Oncol19971526536599053490
- UzielyBJeffersSIsacsonRLiposomal doxorubicin: antitumor activity and unique toxicities during two complementary phase I studiesJ Clin Oncol1995137177717857602367
- SorensenPGBachFBorkEHansenHHRandomized trial of doxorubicin versus cyclophosphamide in diffuse malignant pleural mesotheliomaCancer Treat Rep19856912143114323907825
- BaasPvan MeerbeeckJGroenHCaelyx in malignant mesothelioma: a phase II EORTC studyAnn Oncol200011669770010942058
- AllenTMChonnALarge unilamellar liposomes with low uptake into the reticuloendothelial systemFEBS Lett1987223142463666140
- GabizonAPapahadjopoulosDLiposome formulations with prolonged circulation time in blood and enhanced uptake by tumorsProc Natl Acad Sci U S A19888518694969533413128
- PapahadjopoulosDGabizonATargeting of liposomes to tumor cells in vivoAnn N Y Acad Sci198750764743327419
- HuangSKMartinFJJayGVogelJPapahadjopoulosDFriendDSExtravasation and transcytosis of liposomes in Kaposi’s sarcoma-like dermal lesions of transgenic mice bearing the HIV tat geneAm J Pathol1993143110148317543
- ZarogoulidisKKontakiotisTHatziapostolouPA Phase II study of docetaxel and carboplatin in the treatment of non-small cell lung cancerLung Cancer200132328128711390009
- de CupisASeminoCPiraniPLopreviteMArdizzoniAFavoniREEnhanced effectiveness of last generation antiblastic compounds vs cisplatin on malignant pleural mesothelioma cell linesEur J Pharmacol20034732–3839512892825
- HuangZByunBMatsubaraTMoskowitzMATime-dependent blockade of neurogenic plasma extravasation in dura mater by 5-HT1B/D agonists and endopeptidase 24.11Br J Pharmacol199310823313358383561
- ChenGLYangLRoweTCHalliganBDTeweyKMLiuLFNonintercalative antitumor drugs interfere with the breakage-reunion reaction of mammalian DNA topoisomerase IIJ Biol Chem19842592113560135666092381
- O’DwyerPJLeyland-JonesBAlonsoMTMarsoniSWittesREEtoposide (VP-16-213). Current status of an active anticancer drugN Engl J Med1985312116927002983208
- ClarkPISlevinMLThe clinical pharmacology of etoposide and teniposideClin Pharmacokinet19871242232523297462
- SlevinMLClarkPIJoelSPA randomized trial to evaluate the effect of schedule on the activity of etoposide in small-cell lung cancerJ Clin Oncol198979133313402549204
- ClarkPISlevinMLJoelSPA randomized trial of two etoposide schedules in small-cell lung cancer: the influence of pharmacokinetics on efficacy and toxicityJ Clin Oncol1994127142714358021734
- ZarogoulidisKMylonakiEKakavelasPTopotecan-carboplatin-etoposide combination as 1st line treatment in patients with small cell lung cancerLung Cancer200966222623019321222
- SahmoudTPostmusPEvan PottelsbergheCEtoposide in malignant pleural mesothelioma: two phase II trials of the EORTC Lung Cancer Cooperative GroupEur J Cancer19973313221122159470808
- PlantingASvan der BurgMEGoeySHPhase II study of a short course of weekly high-dose cisplatin combined with long-term oral etoposide in pleural mesotheliomaAnn Oncol1995666136158573543
- TammilehtoLMaasiltaPMantylaMSaloJMattsonKOral etoposide in the treatment of malignant mesothelioma. A phase II studyAnn Oncol19945109499507696167
- AndersonHHasletonPMichieABJohnsonRJThatcherN24-hour cyclophosphamide infusion therapy for malignant mesothelioma of the pleuraBr J Dis Chest198882164693166920
- ShinDMFossellaFVUmsawasdiTProspective study of combination chemotherapy with cyclophosphamide, doxorubicin, and cisplatin for unresectable or metastatic malignant pleural mesotheliomaCancer19957611223022368635025
- van der MostRGCurrieAJCleaverALCyclophosphamide chemotherapy sensitizes tumor cells to TRAIL-dependent CD8 T cell-mediated immune attack resulting in suppression of tumor growthPLoS One200949e698219746156
- RuschVWRosenzweigKVenkatramanEA phase II trial of surgical resection and adjuvant high-dose hemithoracic radiation for malignant pleural mesotheliomaJ Thorac Cardiovasc Surg2001122478879511581615
- ReaFMarulliGBortolottiLInduction chemotherapy, extrapleural pneumonectomy (EPP) and adjuvant hemi-thoracic radiation in malignant pleural mesothelioma (MPM): feasibility and resultsLung Cancer2007571899517403553
- PaganVCeronLPaccagnellaAPizziG5-year prospective results of trimodality treatment for malignant pleural mesotheliomaJ Cardiovasc Surg (Torino)2006475595601
- FloresRMZakowskiMVenkatramanEPrognostic factors in the treatment of malignant pleural mesothelioma at a large tertiary referral centerJ Thorac Oncol200721095796517909360
- FloresRMKrugLMRosenzweigKEInduction chemotherapy, extrapleural pneumonectomy, and postoperative high-dose radiotherapy for locally advanced malignant pleural mesothelioma: a phase II trialJ Thorac Oncol20061428929517409872
- AhamadAStevensCWSmytheWRPromising early local control of malignant pleural mesothelioma following postoperative intensity modulated radiotherapy (IMRT) to the chestCancer J20039647648414740977
- CarboneMLyBHDodsonRFMalignant mesothelioma: facts, myths, and hypothesesJ Cell Physiol20122271445821412769