
Abstract
Chronic lymphocytic leukemia (CLL) is a hematologic malignancy derived from a clonal population of mature B-lymphocytes characterized by relatively low CD20 antigen expression. Although the disease often takes an indolent course, the majority of patients will eventually require therapy. Standard treatment for medically fit patients includes purine analogs and/or alkylating agents in addition to the type I anti-CD20 monoclonal antibody, rituximab. This therapy is inherently myelosuppressive and can result in significant morbidity and even mortality in patients with impaired performance status due to age and/or medical comorbidities. Historically, treatment options for the elderly or frail patient population were limited to mono-therapy with the oral alkylating agent, chlorambucil, rituximab, or another type I anti-CD20 monoclonal antibody ofatumumab. Recently, a newer-generation anti-CD20 monoclonal antibody, obinutuzumab, was developed for patients with CLL. Obinutuzumab is a humanized type II monoclonal antibody that appears to have more direct antibody-dependent cell-mediated cytotoxicity (ADCC) and possibly more direct cytotoxicity in vitro than previously available type I antibodies. A large Phase III prospective randomized clinical trial for older patients with impaired renal function and/or significant medical comorbidities demonstrated that when compared to conventionally-dosed rituximab and chlorambucil, the combination of chlorambucil and obinutuzumab administered at a dose and schedule involving early loading doses improved response rates and progression-free survival without significantly increasing toxicity. Results of this pivotal trial led to the FDA (US Food and Drug Administration) approval of obinutuzumab in combination with chlorambucil for frontline treatment of CLL. Obinutuzumab expands the armamentarium of active and less-toxic targeted agents in the evolving treatment landscape of CLL, providing physicians and patients with an additional therapeutic option.
Historical perspective: conventional chemotherapy
Chronic lymphocytic leukemia (CLL) is diagnosed in more than 15,000 new patients annually in the United States. Median age at diagnosis is 73 years.Citation1,Citation2 Although many patients have an indolent course and may never require therapy, the majority of patients with CLL will eventually need treatment due to progressive bone marrow failure, compressive lymphadenopathy/organomegaly, and/or “B” symptoms including fevers, night sweats, or unintentional weight loss. Initial therapy for patients in need of treatment for CLL has historically utilized a purine nucleoside analog such as fludarabine or pentostatin and/or an alkylating agent such as chlorambucil or cyclophosphamide. Combining agents from both of these classes of drugs has additive clinical benefit: fludarabine and cyclophosphamide (FC) demonstrated improved response rates and incremental progression-free survival (PFS) improvement when compared to fludarabine monotherapy.Citation3–Citation5 Treatment-related adverse events are common with FC, particularly grade 3/4 hematologic toxicities and infection. FC was frequently used for medically fit patients with CLL, but overall survival (OS) of CLL patients was not improved relative to single-agent treatment. Of note, the patients with deletion of chromosome 11q appeared to benefit the most from the addition of the alkylating agent cyclophosphamide.
Benefit to addition of monoclonal antibody to CLL treatment
One of the most significant advances in combination regimens for up-front treatment of CLL in the past decade was the addition of the first monoclonal antibody against CD20, rituximab. Rituximab is a conventional type I monoclonal antibody. It elicits its antitumor effects through multiple mechanisms, including antibody-dependent cell-mediated cytotoxicity (ADCC), complement-mediated cytotoxicity (CMC), and possibly direct cytotoxicity by induction of apoptosis.Citation6,Citation7
In follow-up to the recognition of the strong additional clinical benefit of rituximab when added to chemotherapy for non-Hodgkin lymphoma (NHL), Phase I–II trials in CLL demonstrated clinical activity of rituximab in CLL alone or in combination with fludarabine.Citation8,Citation9 Given these encouraging results, rituximab was added to the fludarabine and cyclophosphamide chemotherapy backbone (FCR) for up-front treatment of medically fit CLL patients. The FCR combination utilizes rituximab at standard doses used in NHL (375 mg/m2) during the first cycle of therapy followed by an escalated dose of 500 mg/m2 for subsequent cycles. Initial study of the FCR regimen found that it produced a very high overall response rate (ORR) of 95%.Citation10 This led to a randomized Phase III trial through the German CLL Study Group (CLL 8) comparing FCR vs FC, which demonstrated improved ORR (90% vs 80%, P<0.001) and PFS (median, 51.8 months [95% confidence interval (CI), 46.2–57.6] vs 32.8 months [95% CI, 29.6–36.0]; P<0.0001) with FCR.Citation11 A major conclusion of this study was that – for the first time – introduction of an additional agent to an existing treatment regimen for CLL resulted in an improvement in OS (3-year survival, 87% vs 83%, respectively; hazard ratio [HR], 0.67 [95% CI, 0.48–0.92]; P=0.01). Treatment was significantly less effective for the subset of patients with the high-risk cytogenetic abnormality in which the tumor suppressor gene p53 is absent due to deletion of chromosome 17p. Severe infections and grade 3/4 myelosuppression were common, and treatment-related mortality was >2%, but comparable in the FCR and FC groups.
Subsequently, rituximab has been added to other CLL chemotherapy regimens, including bendamustine (BR), pentostatin, and others.Citation12,Citation13 More recently, a head-to-head prospective Phase III trial of FCR vs BR for medically fit patients with CLL in need of treatment was performed by the German CLL Study Group (CLL 13).Citation14 Enrolled patients were devoid of major comorbidities and had normal renal function. Median age was 62 years. The ORR in both arms was 97.8%. The complete response (CR) rate was 40.7% with FCR compared to 31.5% with BR (P=0.026). More patients treated with FCR achieved negative testing for minimal residual disease (MRD). Median PFS was 53.7 months for the FCR arm and 43.2 months for the BR arm (HR, 1.589 [95% CI, 1.25–2.079]; P=0.001). However, the PFS difference was not statistically significant for patients over the age of 65 or in patients with comorbidities, and OS was not significantly different between the two groups. Treatment-related mortality was 3.9% (FCR) and 2.1% (BR), respectively. These results have led different investigators to alternative conclusions regarding the optimal frontline therapy for CLL. While FCR may offer higher response rates, it is associated with more toxicity without an OS benefit, and the PFS for patients with advanced age or comorbidities is comparable to BR.
Optimizing CD20-targeted monoclonal antibody
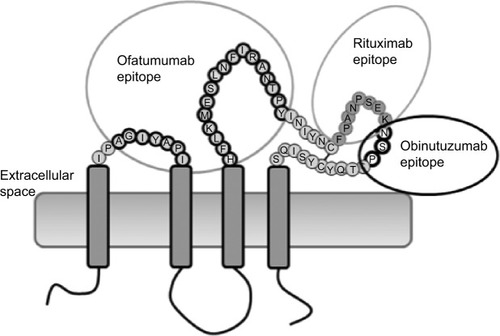
Given the additive benefit of rituximab to chemotherapy regimens, there has been considerable interest in improving anti-CD20 monoclonal antibody technology for therapeutic benefit. In particular, rituximab may not be the optimal agent to target CLL cells, which are characterized by relatively low cell surface expression of CD20. The first so-called second-generation anti-CD20 monoclonal antibody was ofatumumab. Ofatumumab is a fully humanized anti-CD20 monoclonal antibody whose epitope is a small loop of the extracellular domain of CD20, distinct from the binding site for rituximab ().Citation6,Citation15 Preclinical studies suggested that ofatumumab has higher CD20 avidity than rituximab, possibly leading to more CMC.Citation16
Figure 1 Structure of CD20 and epitope targets of ofatumumab, rituximab, and obinutuzumab (GA101).
In the case of relapsed/refractory CLL, a large Phase II study of ofatumumab established this agent as having clinical activity in previously treated patients.Citation17 Ofatumumab was administered as a lead-in flat dose of 300 mg during the 1st week, followed by weekly doses of 2,000 mg for 7 doses during the first 2 months, and then monthly for an additional 4 doses. The ORR was 51% in the entire cohort, including those with bulky disease, and did not appear different in patients with or without prior rituximab exposure. Responses were almost exclusively partial remissions with a single CR. The median duration of response was approximately 6 months.
Obinutuzumab: first FDA-approved anti-CD20 type II monoclonal antibody
In contrast to ofatumumab and rituximab, which are type I monoclonal antibodies targeted against CD20, obinutuzumab (formerly GA101) is a type II antibody. Type I antibodies are strong activators of complement. Preclinical evidence suggests that a large part of the cytotoxic effect of the type I antibodies is in fact due to CMC. In contrast, type II antibodies have minimal CMC but appear to have more direct cellular cytotoxicity. Both type I and type II antibodies have some level of ADCC. Rituximab induces caspase-dependent changes suggestive of induction of apoptosis in vitro, but it has not been convincingly established that this mechanism of action is relevant in vivo.Citation6 Type II monoclonal antibodies induce cell death via release of cytotoxic contents of intracellular lysosomes in the target cells, bypassing the antiapoptotic Bcl-2 family of proteins that may be responsible for significant chemotherapy resistance.Citation18 Obinutuzumab is a humanized monoclonal antibody that targets the same extracellular domain in the CD20 antigen as does rituximab but recognizes a nonoverlapping epitope ().Citation15 However, the Fc region of obinutuzumab was modified with additional carbohydrate groups (“glyco-engineered”) to improve binding capacity to effector cells, including neutrophils, natural killer cells, thereby possibly enhancing ADCC.Citation19,Citation20
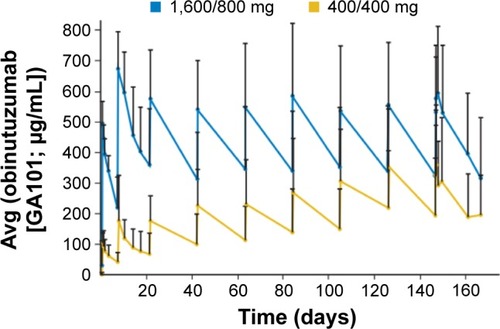
The activity of obinutuzumab was evaluated in a Phase I/II trial in patients with relapsed/refractory indolent NHL or aggressive NHL (diffuse large B-cell lymphoma and mantle cell lymphoma) most of whom were previously treated with rituximab.Citation21,Citation22 There appeared to be a dose-dependent response with ORR of 55% for subjects with indolent NHL and 37% for patients with aggressive NHL receiving two loading doses of 1,600 mg, followed by doses of 800 mg every 2 weeks. The therapy was well tolerated, with a high frequency of infusion-related reactions (IRRs) that were predominantly grade 1–2. Premedication with acetaminophen and antihistamine was required, and glucocorticoid was given to high-risk patients. Serum concentrations of obinutuzumab were significantly higher, earlier in the course of therapy, for patients treated with loading doses rather than continuous dosing at 400 mg every 2 weeks (). This is particularly important, as it provided direct clinical evidence for the pharmacodynamic and pharmacokinetic models in which early doses of monoclonal antibody do not necessarily reach their target, as the initial drug is absorbed by both target cells and off-target immune effector cells.
Figure 2 Pharmacokinetics of obinutuzumab.
Abbreviation: NHL, non-Hodgkin lymphoma.
Less-toxic therapy for older/frail CLL patients: role of chlorambucil alone or in combination with monoclonal antibody
For patients unfit for aggressive cytotoxic chemotherapy regimens, treatment for CLL has historically been considered palliative. For many years, oral chlorambucil monotherapy was often used as an inexpensive and minimally toxic regimen. Previous prospective studies in the frontline setting demonstrated that when used alone, chlorambucil has an ORR of approximately 30%–50%, with very few complete remissions, and PFS <2 years.Citation5,Citation23–Citation26 The dose and schedule of the administration of chlorambucil are variable and have not been subjected to intense optimization strategies.
Because addition of monoclonal antibody provides significant additional therapeutic benefit to most chemotherapeutic agents for B-cell malignancies, Phase II trials were conducted to test the combination of chlorambucil with rituximab.Citation27,Citation28 This treatment strategy was designed for older or frail CLL patients in whom intensive chemoimmunotherapy was contraindicated due to potential toxicity. ORR in these trials was >80%, with PFS of approximately 2 years or longer with the addition of rituximab maintenance.Citation28
In addition, a Phase III trial for the first-line treatment of CLL patients compared ofatumumab in combination with chlorambucil to chlorambucil alone.Citation29 For patients with a median age of 69, the majority of whom had comorbidities, PFS was significantly longer in the patients treated with ofatumumab and chlorambucil relative to chlorambucil alone (22.4 months vs 13.1 months, P<0.001). ORR was 82% vs 69%, P=0.001, favoring the combination therapy group, and CR rates were also higher (12% vs 1%). MRD testing in the peripheral blood or bone marrow was negative in 37% patients treated with the combination therapy. Toxicities included IRRs and neutropenia, but the incidence of grade 3/4 infection was low and not different between the two groups. Subsequent to the presentation of these data, ofatumumab gained a new indication from the FDA (US Food and Drug Administration) for frontline treatment of CLL.
Obinutuzumab for previously untreated CLL
The clinical efficacy of the single-agent obinutuzumab was tested at two different dose levels in previously untreated CLL in a randomized Phase II study.Citation30 Obinutuzumab was given at either 1,000 mg on days 1 and 2 (dose was split into 100 mg on day 1 and 900 mg on day 2 to mitigate IRRs), then 1,000 mg on days 8 and 15 of cycle 1 and every 21 days for cycles 2–8 thereafter, or at 2,000 mg on days 1–3 (100 mg on day 1, 900 mg on day 2, 1,000 mg on day 3), then on days 8 and 15 of cycle 1, followed by once every 21 days for cycles 2–6. The ORR was 67% in the higher-dose group vs 49% in the lower-dose group (P=0.08), in this 80-patient study. CR was achieved in 8 out of 39 patients in the high-dose group (21%) and 2 out of 41 patients (5%) in the low-dose group.
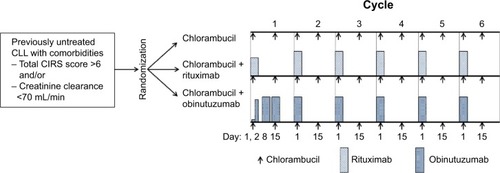
The German CLL Study Group studied the efficacy of obinutuzumab in combination with chlorambucil in a pivotal Phase III three-arm prospective clinical trial for previously untreated CLL patients in need of therapy.Citation31 Importantly, inclusion criteria were designed to specifically enroll patients who were not candidates for more intensive therapy. Thus, the Cumulative Illness Rating Scale was used, which quantifies comorbidities and functional status to provide objective assessment of subjects’ burden of medical conditions.Citation32 This score ranges from 0 to 56, with high scores indicating poorer overall health status. To qualify for inclusion in the study, patients were required to have a score of higher than 6 or to have a creatinine clearance less than 70 mL/minute (but ≥30). Patients were randomly assigned to either chlorambucil monotherapy or chlorambucil in combination with either rituximab or obinutuzumab. The dose and schedule of administration are shown in . The study enrolled 281 patients. The median age was 73 years, which is the median age of patients at the time of diagnosis of CLL. The significant majority of patients (82%) had three or more comorbid conditions.
Figure 3 Schematic representation of pivotal Phase III German CLL13 trial.
Abbreviations: CLL, chronic lymphocytic leukemia; CIRS, Cumulative Illness Rating Scale.
Although there was a higher incidence of grade 3/4 neutropenia in the patients treated with obinutuzumab and chlorambucil, this did not translate into a significant difference in infection rates, which were similar between the three treatment groups. The rate of grade 3/4 IRR was higher in the obinutuzumab and chlorambucil arm relative to the rituximab and chlorambucil arm (20% vs 4%, respectively). Interestingly, IRRs beyond the initial infusion were relatively uncommon in obinutuzumab-treated patients, relative to rituximab. There were 15 cases of tumor lysis syndrome (6 cases were grade ≥3); all except one occurred in patients treated with chlorambucil and obinutuzumab. The median number or cycles completed was 6 in each arm. The median cumulative dose of chlorambucil was comparable in the three treatment arms.
The ORR was higher in the obinutuzumab + chlorambucil arm relative to the rituximab + chlorambucil arm (77.7% vs 65.1%, P<0.001), with higher rates of CR (20.7% vs 7.0%) favoring obinutuzumab + chlorambucil. MRD negativity in bone marrow was significantly higher in those patients treated with obinutuzumab and chlorambucil compared to rituximab and chlorambucil (19.5% vs 2.6%).
These response rates translated into a PFS benefit for obinutuzumab and chlorambucil as compared with chlorambucil alone (median PFS, 26.7 months vs 11.1 months). The HR for progression or death was 0.18 (95% CI, 0.13–0.24; P<0.001). The median PFS of 26.7 months in the group treated with obinutuzumab and chlorambucil was statistically significantly longer than that in the group treated with rituximab and chlorambucil (15.2 months, HR, 0.39 [95% CI, 0.31–0.49]). The PFS benefit of obinutuzumab and chlorambucil did translate into an OS benefit relative to chlorambucil, but not the combination of rituximab and chlorambucil.
Perspective
Therapy for CLL has advanced significantly over recent decades but has tended to build on more aggressive chemoimmunotherapy regimens. This has culminated with the advent of FCR, which produces nearly 100% response rates when used in first-line treatment of patients without 17p deletion. PFS is long with FCR – over 4 years – but the cost of this high level of efficacy is significant toxicity, with treatment-related mortality exceeding 4%. Although the benefit of FCR in terms of response rates and PFS relative to BR is observed for young, fit patients, there is no OS benefit and the PFS and ORR advantage is not maintained for patients older than 65 years or with comorbidities. In addition, there is a significant risk of protracted myelosuppression and secondary malignancies, including myelodysplastic syndrome and treatment-related acute leukemia. In total, given that the median age of CLL is 73 years at the time of diagnosis, and there is a significant lag time between diagnosis and indication for therapy, it is fair to say that the majority of CLL patients in need of treatment are not good candidates for FCR. Although BR is less toxic, it is highly myelosuppressive and, therefore, still difficult to deliver in older patients. Given the additional burdens of comorbid conditions with advanced age, a highly effective regimen for the frail CLL patient population has been an unmet medical need for many years.
There now exists level I evidence that all of the monoclonal antibodies (rituximab, ofatumumab, and obinutuzumab) significantly improve ORR and PFS when added to minimally myelosuppressive doses of chlorambucil.Citation29,Citation31 Furthermore, in head-to-head comparison, the obinutuzumab and chlorambucil regimen outperforms the rituximab and chlorambucil regimen.Citation31 It is noteworthy that the regimen utilized of obinutuzumab and chlorambucil three loading doses (with the first dose split over days 1 and 2) during the first cycle of therapy, whereas the protocol for rituximab + chlorambucil relied on a more traditional “step-up” dosing of rituximab, in which the antibody was given at 375 mg/m2 on day 1 of the first cycle, followed by 500 mg/m2 on day 1 of cycles 2–6. Given the known pharmacokinetics of monoclonal antibodies with high clearance early in the course of treatment, this dosing schedule clearly favored obinutuzumab, conferring a higher ORR and CR rate when administered at higher doses earlier.Citation30 Therefore, one must be cautious in concluding that obinutuzumab is truly a superior monoclonal antibody than rituximab. In fact, when compared to the outcomes of treatment with ofatumumab and chlorambucil combination, those with the obinutuzumab and chlorambucil combination appear similar (ORR, 82% vs 78.4%; PFS, 22.4 vs 26.7 months, respectively).Citation29,Citation31 Therefore, the most accurate statement based on available data is that when combined with chlorambucil, obinutuzumab given at the dose and schedule of the German CLL11 trial produced superior response rates and PFS relative to chlorambucil in combination with conventionally-dosed rituximab.
It is premature to extrapolate from this experience to conclude that obinutuzumab should replace rituximab with intensive chemotherapeutic regimens (FC or BR). In particular, the early experience with these combinations has been noteworthy for relatively high rates of grade 3/4 hematologic toxicity requiring treatment delays or discontinuations.Citation33 Clearly, more safety and efficacy data are needed with more intensive chemotherapy regimens in the frontline setting.
With the B-cell receptor pathway inhibitors ibrutinib and idelalisib now available, and other highly active agents in development, including the very promising Bcl-2 inhibitor, Venetoclax, the tides are shifting in the management of CLL toward more targeted, less-toxic therapies. For now, these drugs are available only at the time of relapse or, in the relatively uncommon case of 17p deletion, at the time of diagnosis. The availability of obinutuzumab for the frontline treatment of CLL is a welcome addition to the treatment landscape and is particularly appealing for the older/frailer patient for whom intensive therapy is not a viable option.
Disclosure
The authors report no conflicts of interest in this work.
References
- HowladerNNooneAMKrapchoMSEER Cancer Statistics Review, 1975–2010Bethesda, MDNational Cancer Institute2012
- SlagerSLBenaventeYBlairAMedical history, lifestyle, family history, and occupational risk factors for chronic lymphocytic leukemia/small lymphocytic lymphoma: the InterLymph Non-Hodgkin Lymphoma Subtypes ProjectJ Natl Cancer Inst Monogr2014201448415125174025
- FlinnIWNeubergDSGreverMRPhase III trial of fludarabine plus cyclophosphamide compared with fludarabine for patients with previously untreated chronic lymphocytic leukemia: US Intergroup Trial E2997J Clin Oncol200725779379817283364
- EichhorstBFBuschRHopfingerGFludarabine plus cyclophosphamide versus fludarabine alone in first-line therapy of younger patients with chronic lymphocytic leukemiaBlood2006107388589116219797
- CatovskyDRichardsSMatutesEAssessment of fludarabine plus cyclophosphamide for patients with chronic lymphocytic leukaemia (the LRF CLL4 Trial): a randomised controlled trialLancet2007370958323023917658394
- BeersSAChanCHFrenchRRCraggMSGlennieMJCD20 as a target for therapeutic type I and II monoclonal antibodiesSemin Hematol201047210711420350657
- DalleSDumontetCRituximab: mechanism of action and resistanceBull Cancer2007942198202 French17337389
- ByrdJCMurphyTHowardRSRituximab using a thrice weekly dosing schedule in B-cell chronic lymphocytic leukemia and small lymphocytic lymphoma demonstrates clinical activity and acceptable toxicityJ Clin Oncol20011982153216411304767
- ByrdJCPetersonBLMorrisonVARandomized phase 2 study of fludarabine with concurrent versus sequential treatment with rituximab in symptomatic, untreated patients with B-cell chronic lymphocytic leukemia: results from Cancer and Leukemia Group B 9712 (CALGB 9712)Blood2003101161412393429
- KeatingMJO’BrienSAlbitarMEarly results of a chemoimmunotherapy regimen of fludarabine, cyclophosphamide, and rituximab as initial therapy for chronic lymphocytic leukemiaJ Clin Oncol200523184079408815767648
- HallekMFischerKFingerle-RowsonGAddition of rituximab to fludarabine and cyclophosphamide in patients with chronic lymphocytic leukaemia: a randomised, open-label, phase 3 trialLancet201037697471164117420888994
- FischerKCramerPBuschRBendamustine in combination with rituximab for previously untreated patients with chronic lymphocytic leukemia: a multicenter phase II trial of the German Chronic Lymphocytic Leukemia Study GroupJ Clin Oncol201230263209321622869884
- KayNEGeyerSMCallTGCombination chemoimmunotherapy with pentostatin, cyclophosphamide, and rituximab shows significant clinical activity with low accompanying toxicity in previously untreated B chronic lymphocytic leukemiaBlood2007109240541117008537
- EichhorstBFinkAMBuschRFrontline chemoimmunotherapy with fludarabine (F), cyclophosphamide (C), and rituximab (R) (FCR) shows superior efficacy in comparison to bendamustine (B) and rituximab (BR) in previously untreated and physically fit patients (pts) with advanced chronic lymphocytic leukemia (CLL): final analysis of an international, randomized study of the German CLL Study Group (GCLLSG) (CLL10 Study)Poster presented at: American Society of Hematology Annual Meeting2014Washington, DC
- KleinCLammensASchaferWEpitope interactions of monoclonal antibodies targeting CD20 and their relationship to functional propertiesMAbs201351223323211638
- TeelingJLFrenchRRCraggMSCharacterization of new human CD20 monoclonal antibodies with potent cytolytic activity against non-Hodgkin lymphomasBlood200410461793180015172969
- WierdaWGKippsTJMayerJOfatumumab as single-agent CD20 immunotherapy in fludarabine-refractory chronic lymphocytic leukemiaJ Clin Oncol201028101749175520194866
- IvanovABeersSAWalsheCAMonoclonal antibodies directed to CD20 and HLA-DR can elicit homotypic adhesion followed by lysosome-mediated cell death in human lymphoma and leukemia cellsJ Clin Invest200911982143215919620786
- GolayJDa RoitFBolognaLGlycoengineered CD20 antibody obinutuzumab activates neutrophils and mediates phagocytosis through CD16B more efficiently than rituximabBlood2013122203482349124106207
- MossnerEBrunkerPMoserSIncreasing the efficacy of CD20 antibody therapy through the engineering of a new type II anti-CD20 antibody with enhanced direct and immune effector cell-mediated B-cell cytotoxicityBlood2010115224393440220194898
- MorschhauserFACartronGThieblemontCObinutuzumab (GA101) monotherapy in relapsed/refractory diffuse large b-cell lymphoma or mantle-cell lymphoma: results from the phase II GAUGUIN studyJ Clin Oncol201331232912291923835718
- SallesGAMorschhauserFSolal-CelignyPObinutuzumab (GA101) in patients with relapsed/refractory indolent non-Hodgkin lymphoma: results from the phase II GAUGUIN studyJ Clin Oncol201331232920292623835715
- EichhorstBFBuschRStilgenbauerSFirst-line therapy with fludarabine compared with chlorambucil does not result in a major benefit for elderly patients with advanced chronic lymphocytic leukemiaBlood2009114163382339119605849
- RaiKRPetersonBLAppelbaumFRFludarabine compared with chlorambucil as primary therapy for chronic lymphocytic leukemiaN Engl J Med2000343241750175711114313
- HillmenPSkotnickiABRobakTAlemtuzumab compared with chlorambucil as first-line therapy for chronic lymphocytic leukemiaJ Clin Oncol200725355616562317984186
- KnaufWULissichkovTAldaoudAPhase III randomized study of bendamustine compared with chlorambucil in previously untreated patients with chronic lymphocytic leukemiaJ Clin Oncol200927264378438419652068
- HillmenPGribbenJGFollowsGARituximab plus chlorambucil as first-line treatment for chronic lymphocytic leukemia: final analysis of an open-label phase II studyJ Clin Oncol201432121236124124638012
- FoaRDel GiudiceICuneoAChlorambucil plus rituximab with or without maintenance rituximab as first-line treatment for elderly chronic lymphocytic leukemia patientsAm J Hematol201489548048624415640
- HillmenPRobakTJanssensAGovindbabuKOfatumumab + chlorambucil versus chlorambucil alone in patients with untreated chronic lymphocytic leukemia (CLL): results of the phase III Study Complement 1Poster presented at: American Society of Hematology Annual Meeting2013Washington, DC
- FlynnJMByrdJCKippsTJBoxerMObinsutuzumab (GA101) 1,000 mg versus 2,000 mg in patients with chronic lymphocytic leukemia (CLL): results of the phase II GAGE (GAO4768g) trialPoster presented at: American Society of Clinical Oncology Annual Meeting2014Alexandria, VA
- GoedeVFischerKBuschRObinutuzumab plus chlorambucil in patients with CLL and coexisting conditionsN Engl J Med2014370121101111024401022
- ParmeleePAThurasPDKatzIRLawtonMPValidation of the Cumulative Illness Rating Scale in a geriatric residential populationJ Am Geriatr Soc19954321301377836636
- BrownJRO’BrienSKingsleyDEradatHSafety and efficacy of obinutuzumab (GA101) with fludarabine/cyclophosphamide (G-FC) or bendamustine (G-B) in the initial therapy of patients with chronic lymphocytic leukemia (CLL): results from the Phase 1b Galton Trial (GAO4779g)Poster presented at: American Society of Hematology Annual Meeting2013Washington, DC
- GolayJSemenzatoGRambaldiALessons for the clinic from rituximab pharmacokinetics and pharmacodynamicsMAbs20135682683723933992