
Abstract
Angiogenesis is an essential process for tumor growth and metastasis, and remains a promising therapeutic target process in cancer treatment for several cancer types. Bevacizumab, a monoclonal antibody that targets vascular endothelial growth factor (VEGF), was the first antiangiogenic agent approved for cancer therapy. Novel antiangiogenic agents, such as sunitinib, sorafenib, pazopanib, or vandetanib that target additional proangiogenic signaling pathways beyond VEGF, have also been approved for the treatment of various malignant diseases. While most of these agents are approved in combination with cytotoxic chemotherapy for indications including metastatic colorectal cancer, non-small-cell lung cancer, breast cancer, renal cell carcinoma (RCC), and gastric cancer, some are used as approved monotherapy for advanced RCC, hepatocellular carcinoma and medullary thyroid cancer. Major challenges to the success of antiangiogenic therapy include associated toxicity risks, limitation of efficacy through the possible development of resistance and induction or promotion of metastatic progression. Nintedanib (formally known as BIBF 1120) is a triple angiokinase inhibitor of VEGF, fibroblast growth factor, platelet-derived growth factor signaling with lesser activity against RET, Flt-3, and Src. Through this unique targeting profile nintedanib has demonstrated significant antitumor activity in several tumor types in preclinical studies. Nintedanib has also shown promising clinical efficacy in combination with docetaxel and has been approved for treating patients with locally advanced and metastatic non-small-cell lung cancer in Europe. Nintedanib has also been found to be clinically promising in terms of efficacy and safety in several other solid tumors including ovarian cancer (Phase III), RCC (Phase II), and prostate cancer (Phase II). This review article provides a comprehensive summary of the preclinical and clinical efficacy of nintedanib in the treatment of solid tumors.
Introduction
Angiogenesis, the process of new blood vessel development from existing vasculature, is a hallmark of cancer progression and metastasis that has long been considered an attractive therapeutic target.Citation1 Tumor angiogenesis is a complex process that represents a highly regulated yet disturbed balance between proangiogenic and antiangiogenic mechanisms.Citation2 Among several proangiogenic signaling molecules, vascular endothelial growth factor (VEGF) is considered to be one of the most important factors involved in tumor angiogenesis.Citation3 VEGF is frequently highly expressed in human solid cancers and plays a fundamental role in tumor-mediated blood vessel growth by mediating vasculogenesis, angiogenic remodeling, angiogenic sprouting, and vascular permeability.Citation3–Citation5 Thus, initial antiangiogenic therapy attempts have largely focused on inhibiting VEGF signaling. Bevacizumab, a monoclonal antibody that blocks angiogenesis by binding VEGF-A (a ligand for VEGFR1 and VEGFR2), was the first antiangiogenic agent approved in 2004 that showed clinical efficacy in combination with chemotherapy in some solid tumors including metastatic colorectal cancer (CRC),Citation6 non-small-cell lung cancer (NSCLC),Citation7 breast cancer,Citation8 and renal cell carcinoma (RCC).Citation9 Since then, several antiangiogenic agents, such as sunitinib,Citation10 sorafenib,Citation11 pazopanib,Citation12 vandetanib,Citation13 axitinib,Citation14 regorafenib,Citation15 aflibercept,Citation16 cabozantinib,Citation17 and ramucirumabCitation18 that target VEGF signaling and/or some additional proangiogenic signaling activity have been approved for the treatment of various malignant diseases. These anti-angiogenic agents, either as monotherapy or in combination with chemotherapy, generally have only provided limited clinical benefits in some tumor types. Furthermore, in certain advanced metastatic cancers, VEGF inhibition alone was insufficient to prevent progression, induced resistance and in some cases may have contributed to increased invasion and metastasis.Citation19,Citation20 One of the main reasons for the limited and transient response of the anti-VEGF therapies is that tumor angiogenesis is regulated by multiple pathways that are able to compensate for each other when single pathways are inhibited. The fibroblast growth factor (FGF) and its receptors (FGFR1/2/3),Citation21 platelet-derived growth factor (PDGF), and its receptors (PDGFRα and PDGFRβ),Citation22 epidermal growth factor and its receptor,Citation23 angiopoietin-2,Citation24 placenta-derived growth factor,Citation25 and neuropilinCitation26 are key components within the main signaling pathways that provide potential escape mechanisms from anti-VEGF therapy leading to resistance development and facilitate resumption of tumor growth.Citation27
The FGF/FGFR signaling axis plays an important role in tissue homeostasis, tissue repair, angiogenesis, and inflammation. Deregulation of FGF/FGFR signaling through genetic modification or over-expression of its ligands/receptors has been observed to promote cell proliferation, survival, and tumor angiogenesis in numerous tumor settings including pancreatic cancer, prostate cancer, and some squamous cell carcinomas.Citation28,Citation29 Several preclinical studies demonstrated that inhibition of FGF/FGFR signaling has antiproliferative, proapoptotic, and antiangiogenic effects, supporting the validity of this signaling axis as a potential therapeutic target. PDGF is another important growth factor that can be crucial for tumor growth and progression. PDGF itself is a potent mitogen in both normal and tumor cells,Citation30 but it also has significant angiogenic effects on endothelial cells. PDGF/PDGFR signaling has been shown to promote cell division,Citation31,Citation32 cell migration,Citation33 and angiogenesis.Citation34 In addition, recruitment of pericytes such as vascular smooth muscle cells by PDGF is essential for maintenance of tumor angiogenesis.Citation35 The PDGF/PDGFR signaling has been overactive in several malignancies such as brain tumor, sarcomas, prostate cancer, liver cancer, NSCLC, breast cancer, and CRCCitation36,Citation37 and therapeutic targeting of this pathway reduced tumor growth in many tumor types.Citation37–Citation39
As multiple proangiogenic factors contribute to tumor angiogenesis, and the fact that inhibition of one angiogenic signaling pathway induces compensatory mechanisms leading to the development of resistance,Citation40–Citation42 more recent therapeutic strategies have focused on developing multi-targeted tyrosine kinase receptors (TKIs) that have the ability to block multiple signaling pathways simultaneously, but at the same time maintain some selectivity profile of kinases in terms of safety and tolerability. This review summarizes the antitumor profile of nintedanib, a triple angiokinase inhibitor, which targets proangiogenic signaling of VEGFR, FGFR, and PDGFR.
Nintedanib: advantages and mechanism of action
The first commercially available antiangiogenic drug was bevacizumab, a monoclonal antibody against VEGF-A.Citation43 Bevacizumab is currently approved in combination with standard chemotherapy for the treatment of several cancers including metastatic CRC,Citation6 NSCLC,Citation7 and RCC.Citation6,Citation7,Citation19 While bevacizumab demonstrates some promising antitumor activity, its clinical use may also be limited by its side-effect profile that includes hypertension, proteinuria, bleeding, thrombotic events, and hemorrhage.Citation44,Citation45 Efforts beyond bevacizumab have focused on a second class of antiangiogenic agents, namely small molecules that are orally available and have the ability to target multiple TKIs. Most of these broad-spectrum TKIs such as sunitinib, sorafenib, pazopanib, vandetanib have complex efficacy data, but in many cases the use of these drugs is associated with a significant increase in the incidence and risk of side effects.Citation46–Citation48 Most of these TKIs that affect multiple kinases have lower specificity toward some of their therapeutic targets, particularly at the FGF/FGFR axis, requiring higher doses for efficacy.Citation49 Therefore, these TKIs have increased risk for on-target toxicities (such as hypertension, skin toxicity, and diarrhea) and presumed off-target toxicities (such as cardiac impairment).Citation49,Citation50
Nintedanib is a next generation, oral, and potent triple angiokinase inhibitor that inhibits the proangiogenic pathways mediated by VEGFR1/2/3 (IC50 13–34 nmol/L), FGFR1/2/3 (IC50 37–108 nmol/L), and PDGFRα/β (IC50 59–65 nmol/L) to a high degree of specificity (). Nintedanib competitively binds to the ATP binding-pocket of these receptors, resulting in interference with receptor dimerization and blocking intracellular signaling critical for the proliferation and survival of angiogenesis-related endothelial cells, pericytes, and vascular smooth muscle cells (). Nintedanib also inhibits some non-receptor kinases such as Fms-like tyrosine protein kinase (Flt-3, IC50 26 nmol/L), proto-oncogene ret (Ret, IC50 35 nmol/L), lymphocyte-specific tyrosine kinase (Lck, IC50 16 nmol/L), tyrosine-protein kinase lyn (Lyn IC50 195 nmol/L), and proto-oncogene tyrosine protein kinase src (Src, IC50 156 nmol/L)Citation51,Citation52 (). In addition, nintedanib has recently been approved for the treatment of idiopathic pulmonary fibrosis based on results from the replicate Phase III trials involving 1,066 patients from 24 countries.Citation53 Nintedanib is thus the first targeted treatment for idiopathic pulmonary fibrosis, indicating the therapeutic potential of TKIs in non-malignant diseases.
Figure 1 Summary of nintedanib.
Abbreviations: VEGFR, vascular endothelial growth factor receptor; FGFR, fibroblast growth factor receptor; PDGFR, platelet-derived growth factor receptor; IGF1R, insulin-like growth factor 1 receptor; InsR, insulin receptor; Flt-3, fms-like tyrosine protein kinase 3; Lck, lymphocyte-specific tyrosine kinase; Src, proto-oncogene tyrosine protein kinase src; Lyn, tyrosine-protein kinase lyn; EGFR, epidermal growth factor receptor; HER2, human epidermal growth factor receptor 2; CDK, cyclin-dependent kinase.
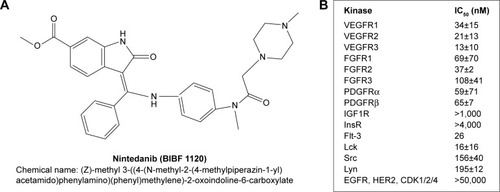
Figure 2 Triple angiokinase inhibition mechanism of nintedanib targeting tumor angiogenesis.
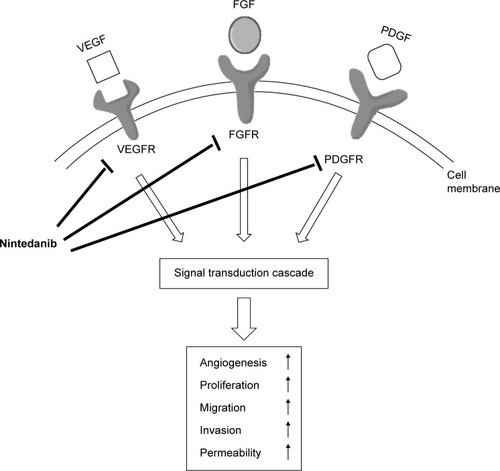
A major challenge in the success of VEGF signaling blocking antiangiogenic therapy is the development of resistance in the primary tumor, probably due to induction of tumor escape mechanisms through upregulated FGFR and PDGFR signaling.Citation54–Citation56 This mechanism of the development of antiangiogenic drug resistance provides a potential rationale for efficacy of nintedanib, which can prevent tumor growth and metastasis via its triple inhibition of VEGFR, FGFR and PDGFR, and also provide a therapeutic alternative for patients with intrinsic and acquired resistance to single or dual target antiangiogenic drugs.
Nintedanib: preclinical studies to date
In vitro studies demonstrated that nintedanib treatment inhibited the proliferation of VEGF-stimulated human umbilical vein endothelial cells and human skin microvascular endothelial cells. Nintedanib also inhibited the proliferation of PDGF-stimulated smooth muscle cells and pericytes.Citation52 Although Kutluk Cenik et alCitation57 showed that nintedanib has no antiproliferative activity on selected lung and pancreatic cancer cell lines, recent reports suggest that nintedanib effects are not generally limited to stromal cells as it also differentially inhibited the proliferation of hepatocellular carcinoma (HCC) cellsCitation58 and pancreatic ductal adenocarcinoma (PDAC) cells.Citation59 Tai et alCitation58 demonstrated that nintedanib treatment caused a significant antiproliferative effect in a panel of four HCC cell lines (PLC5, Hep3B, SK-Hep1, and HuH7) and one hepatoblastoma cell line (Hepg2). Awasthi et alCitation59 demonstrated that nintedanib not only inhibited the proliferation of human umbilical vein endothelial cells, fibroblast WI-38 cells and pancreatic cancer stromal cells, but it also inhibited the proliferation of human PDAC cells (AsPC-1, BxPC-3, MIA PaCa-2, and Panc-1) and murine PDAC cells PanO2.
In vivo, nintedanib demonstrated potent antitumor effects in all human tumor xenografts reported to date, including NSCLC, RCC, CRC, ovarian cancer, prostate cancer, and PDAC.Citation52,Citation57,Citation59 More importantly, nintedanib treatment augmented the antitumor response of standard cytotoxic agents. In NSCLC xenografts (H460 cells), nintedanib treatment caused synergistic antitumor effects in combination with cytotoxic agents docetaxel or pemetrexed.Citation60 Kutluk Cenik et alCitation57 demonstrated significant antitumor activity of nintedanib monotherapy and in combination with standard cytotoxic chemotherapy in several xenograft models of lung and pancreatic cancer.Citation57 Recently, Awasthi et alCitation59 demonstrated that nintedanib significantly enhanced gemcitabine response in pancreatic cancer: net local tumor growth compared to controls (100%) was 60.8%±10.5% in the gemcitabine group, −2.1%±9.9% after nintedanib monotherapy and −12.4%±16% after gemcitabine plus nintedanib combination therapy. In addition, this study demonstrated that compared with controls, the increase in median animal survival was 56% with gemcitabine (P=0.036), 94% for nintedanib (P=0.004) and 138% after gemcitabine + nintedanib (P=0.001).Citation59 In human tumor xenografts, intratumoral antitumor mechanism of nintedanib involves reduced microvessel density, pericyte coverage, vessel permeability, tumor perfusion, and induced hypoxia, as well as inhibition of phosphatidylinositol 3-kinase (PI3K)-AKT and mitogen-activated protein kinase (MAPK) signaling pathways.Citation52,Citation57,Citation59
Nintedanib: clinical studies to date
The clinical pharmacokinetic profile studies of nintedanib demonstrated that it is rapidly absorbed as its maximum plasma concentrations occur within 1–3 hours after oral administration.Citation61,Citation62 The terminal half-life of nintedanib was observed to be ~13–19 hours.Citation61,Citation62 The first Phase I dose-escalation study with single agent nintedanib therapy was reported in 61 patients with different advanced solid tumors.Citation62 Twenty-five patients received nintedanib 50–450 mg once daily (od) and 36 patients received nintedanib 150–300 mg twice daily (bid) in 4-week cycles with a week off. The most common drug-related adverse events (AEs) were mild to moderate; grade 3 or more AEs for nintedanib od vs bid occurring in >5% patients were reversible hepatic enzyme elevation (12% grade 3 and 4% grade 4 vs 0% grade 3 and 2.8% grade 4), increase in aspartate aminotransferase (AST; grade 3, 8% vs 2.8%), increase in alanine aminotransferase (ALT; grade 3, 0% vs 5.6%), increase in γ-glutamyl transpeptidase (grade 3, 4% vs 5.6%), decrease in CD-4 lymphocyte (grade 3, 16% vs 5.6%), hypertension (grade 3, 4% vs 0%), diarrhea (grade 3, 0% vs 2.8%), nausea (grade 3, 0% vs 5.6%), and vomiting (grade 3, 0% vs 2.8%). The maximum tolerable dose (MTD) of nintedanib was defined as 250 mg for both od and bid dosing.Citation62 In another Phase I dose-escalation study, 21 Japanese patients with advanced refractory solid tumors were treated with bid nintedanib doses of 150 mg (n=3), 200 mg (n=12), or 250 mg (n=6).Citation63 This study reported that the dose-limiting grade 3 or 4 toxicity elevation of liver enzymes occurred in 3 of 12 patients at 200 mg bid and 3 of 6 patients at 250 mg bid dose. Stable disease (SD) was reported in 76.2% of patients (n=16). The MTD of nintedanib in this study was determined to be 200 mg bid.
Nintedanib in NSCLC
In NSCLC patients, two Phase I dose-escalation studies have been conducted investigating nintedanib in combination with a standard chemotherapy regimen. The first study investigated the MTD of continuous nintedanib oral treatment in combination with standard-dose pemetrexed (500 mg/m2) in patients who had been previously treated with one platinum-based chemotherapy regimen.Citation64 In this study, one patient achieved a complete response after 44 days for more than 3 years; otherwise, the best overall response was SD in 50% patients (n=13). The second trial investigated the safety, tolerability, and MTD of nintedanib in combination with carboplatin and paclitaxel in patients with advanced NSCLC who were previously untreated.Citation65 In these two Phase I studies, the recommended dose of nintedanib was determined as 200 mg bid when used in combination with the mentioned standard chemotherapy regimens of NSCLC. The most frequent AEs in these studies were comparable to the nintedanib monotherapy trials.
A Phase II double-blind trial evaluated the efficacy of nintedanib monotherapy (150 mg bid, n=36 or 250 mg bid, n=37) in patients with relapsed, advanced NSCLC (any histology) with an Eastern Cooperative Oncology Group performance status 0–2. This study reported a median progression free survival (PFS) of 6.9 weeks, the median overall survival (OS) was 21.9 weeks, and SD was observed in 46% of the patients (). In 56 patients with Eastern Cooperative Oncology Group performance status 0–1, median PFS was 11.6 weeks with a median OS of 37.7 weeks. Most commonly reported drug-related AEs included nausea, diarrhea, vomiting, anorexia, and abdominal pain.Citation66
Table 1 Summary of key efficacy and safety results from Phase II and III studies with nintedanib in patients with NSCLC
A Phase III, double-blind, randomized trial of nintedanib (200 mg, bid, n=565) or placebo (n=569) on days 2–21, in combination with docetaxel (75 mg/m2 on day 1) in patients with previously treated NSCLC (LUME-Lung 1 trial), reported that median PFS was significantly improved in the docetaxel plus nintedanib group compared with the docetaxel plus placebo group (3.4 months vs 2.7 months, hazard ratio (HR) 0.79, P=0.0019). The median OS was also significantly improved in the docetaxel plus nintedanib group compared with docetaxel alone group (12.6 months vs 10.3 months; HR 0.83, P=0.0359) for all patients with adenocarcinoma histology. In the total study population, median OS in the docetaxel plus nintedanib group and docetaxel alone group was 10.1 and 9.1 months (HR 0.94, P=0.2720), respectively. Nintedanib plus docetaxel had a manageable safety profile as AEs more common in the combination group than in the docetaxel alone group included diarrhea (42.3% vs 21.8%), increases in ALT (28.5% vs 8.4%), increase in AST (22.5% vs 6.6%), nausea (24.2% vs 18%), and vomiting (16.9% vs 9.3%) (). Most of these AEs were manageable by symptom management and/or dose reduction.Citation67 Based on the positive results of this study of 1,300 patients in 27 countries, the European Union granted approval for nintedanib in combination with docetaxel for use in patients with locally advanced, metastatic, or locally recurrent NSCLC with adenocarcinoma histology and progression after first-line chemotherapy. Another Phase III study (LUME-Lung 2) trial investigated the efficacy and safety of nintedanib (200 mg, bid on 2–21 days) in combination with standard pem-etrexed (500 mg/m2 on day 1) compared with pemetrexed alone (500 mg/m2 on day 1) in patients with advanced or recurrent nonsquamous NSCLC after relapse or failure of first-line chemotherapy. In this study, patient enrollment was halted after 713 patients based on a pre-defined futility analysis of investigator-assessed PFS by an independent data monitoring committee. This decision was based on the likelihood that the primary endpoint of centrally assessed PFS would not be met, and was not safety related. Interestingly, a subsequent analysis of the 713 patients who were enrolled, demonstrated that the primary end-point of centrally reviewed PFS was met even though the study was stopped prematurely. This analysis showed that median PFS was significantly improved in the pemetrexed plus nintedanib group compared with pemetrexed alone (4.4 vs 3.6 months, HR 0.83, P=0.0435). There was no difference in OS between the two treatment groups (12.2 vs 12.7 months, HR 1.03, P=0.7921) and overall response rates were also comparable (9.1% vs 8.3%). There was a higher incidence of grade 3/4 AEs (increase in liver enzymes and gastrointestinal events, overall 58.5% vs 42.3%), serious AEs were 30% vs 32.8% and grade 5 AEs were 9.8% vs 12% in the nintedanib arm vs placebo ().Citation68 A Phase II study (a biomarker-driven study: FGFR1 amplification as predictive of efficacy) of nintedanib in advanced squamous cell lung cancer patients who have failed up to two prior chemotherapy regimens is currently ongoing (NCT01948141). Another placebo-controlled, Phase III trial of nintedanib plus docetaxel in patients with stage IIIB/IV or recurrent adenocarcinoma NSCLC after failure of first line chemotherapy is also ongoing (LUME-Columbus, NCT02231164).
Nintedanib in ovarian cancer
In a Phase II double-blind, randomized trial of 83 patients who had just completed chemotherapy for relapsed ovarian cancer with evidence of response but at high risk of further early recurrence, patients were randomized to receive either nintedanib 250 mg (n=43) or placebo (n=40), bid, continuously for 36 weeks. The PFS rates at 36 weeks were 16.3% and 5% in the nintedanib and placebo groups, respectively (HR 0.65, 95% CI: 0.42–1.02, P=0.06). Grade 3 or 4 AEs were similar between the nintedanib group and placebo (34.9% vs 27.5%, P=0.49) (). This study concluded that nintedanib is well tolerated and it is associated with a potential improvement in survival.Citation69
Table 2 Summary of key efficacy and safety results from Phase II and III studies with nintedanib in solid tumors other than NSCLC
In a Phase III study (LUME-Ovar 1 or AGO-OVAR 12), nintedanib 200 mg bid was added to standard first-line chemotherapy (carboplatin and paclitaxel) followed by nintedanib maintenance therapy for a maximum of 120 weeks as first-line treatment in patients with advanced epithelial ovarian cancer. This study demonstrated a significant improvement in median PFS in the nintedanib plus chemotherapy group compared with placebo/chemotherapy alone (17.3 vs 16.6 months, HR 0.84, 95% CI: 0.72–0.98, P=0.0239) (). In a subgroup analysis, a more pronounced PFS benefit was observed with nintedanib compared with the placebo arm in patients with <1 cm postsurgical residual tumor deposits (27.1 vs 20.8 months, HR 0.75, 95% CI: 0.61–0.92, P=0.005). This study is still ongoing.Citation70 Three Phase II trials of nintedanib are currently ongoing: one with and without metronomic dose of cyclophosphamide in advanced ovarian cancer (NCT01610869), one in combination with first line chemotherapy with interval debulking surgery in patients with ovarian cancer (NCT01583322), and another in bevacizumab resistant, persistent, or recurrent epithelial ovarian cancer (NCT01669798).
Nintedanib in renal cell carcinoma
The efficacy and safety of nintedanib (200 mg, bid, given in 4 week cycle, n=64) was assessed in a Phase II study of previously untreated advanced RCC patients and compared with the standard of care agent sunitinib (50 mg od, 4 weeks on, 2 weeks off schedule, n=32) as first-line systemic therapy. No significant difference in median PFS was observed between nintedanib and sunitinib treated groups (8.44 vs 8.38 months, HR 1.16, 95% CI: 0.71–1.89, P=0.56). Also, no significant difference was observed between the two therapy groups in terms of median OS (20.37 vs 21.22 months, HR 0.92, 95% CI: 0.54–0.156, P=0.63) or 9 month PFS (43% vs 45%, P=0.85). The overall incidence of AE (any grade) was similar between nintedanib and sunitinib groups (90.6% vs 93.8%). However, grade 3 or more AEs occurred in 47% of patients after nintedanib compared with 56% after sunitinib. Most common AEs of all grades after nintedanib compared to sunitinib included diarrhea (61% vs 50%), nausea (38% vs 34%), fatigue (both 25%), and vomiting (16% vs 22%). However, dermatologic AEs (8% vs 47%) and other common AEs associated with antiangiogenic agents such as hypertension (3.1% vs 15.6%), hand–foot syndrome (0% vs 31.3%), and stomatitis (0% vs 31.3%), were less common in nintedanib treated patients compared with sunitinib therapy ().Citation71
Nintedanib in HCC
Two Phase II studies evaluated the efficacy and safety of nintedanib (200 mg, bid) in comparison with sorafenib (400 mg, bid) continuously in 28-day cycle, in patients with unresectable, advanced HCC in Europe (NCT0100434003) and Asia (NCT00987935). Pooled analysis of these two trials (180 patients) in Caucasian and Asian patients showed similar efficacy between nintedanib and sorafenib therapy groups in terms of median time to progression (TTP; 3.7 vs 3.9 months, HR 1.31, 95% CI: 0.89–1.91), median OS (11.4 vs 11 months, HR 0.91, 95% CI: 0.65–1.29), and overall response rates (4% vs 5%). The most frequent (>5% of patients in any group) grade ≥3 AEs after nintedanib compared to sorafenib included diarrhea (10% vs 6%), fatigue (7% vs 2%), anemia (7% vs 6%), increased AST (8% vs 13%) and ALT (6% vs 8%), thrombocytopenia (5% vs 8%), and skin reaction (1% vs 6%). However, the rates of grade ≥3 AEs (62% vs 87%) and AEs leading to dose reduction (19% vs 51%) were lower in the nintedanib group compared to sorafenib ().Citation72
Nintedanib in prostate cancer
Two doses of nintedanib (150 and 250 mg, bid) were evaluated in a randomized Phase II study in metastatic castration-resistant prostate cancer patients after progression with docetaxel.Citation73 The primary endpoint, prostate-specific antigen (PSA) response rate (≥20% decline in PSA from baseline), was 0% in the nintedanib 150 mg group and 11.1% in the nintedanib 250 mg group (P=0.12). However, nintedanib at 250 mg showed at least 50% PSA reduction in 5.6% patients and the rate of PSA increase in this group was significantly decelerated on treatment vs before treatment (P=0.002). The median PFS was similar between the two groups (73.5 vs 76 days, P=0.3). AEs included gastrointestinal disorders, asthenia, hypertension, and reversible transaminase elevation. The incidence of serious AEs for nintedanib 150 mg vs 250 mg, were 20% vs 24.4% ().Citation73
Another Phase II study evaluated nintedanib and afatinib, an ErbB family blocker, in advanced castration-resistant prostate cancer patients; dosing included nintedanib (250 mg, bid, n=27), afatinib (40 mg od, n=13), or alternating sequential 7-day nintedanib (250 mg, bid) and afatinib (70 mg od; Combi70), which was later termed Combi40 (n=10) because the afatinib dose was reduced to 40 mg od due to AEs. The primary end-point of the study, the progression-free rate at 12 weeks was 26% for nintedanib and 0% for the afatinib and Combi40 groups (). However, the median TTP was 31 days (95% CI: 29–84) for nintedanib monotherapy, 29 days (95% CI: 29–54) for afatinib monotherapy, and 57 days (95% CI: 29–78) for Combi40. The median PFS results were the same as for median TTP. Two patients had a ≥50% decline in PSA, one each in the nintedanib and the Combi40 groups. The most common drug-related AEs were diarrhea, nausea, vomiting, and lethargy; the majority of patients (>90%) in each group had at least one therapy-related AE. Rash was more frequent with afatinib and elevation in transaminase was more frequent with nintedanib monotherapy. The frequency of therapy-related AEs did not increase in Combi40 compared with monotherapy.Citation74
Nintedanib in CRC
In a Phase II study an alternating regimen of nintedanib (250 mg, bid) and then afatinib (50 mg, od) was evaluated in patients with advanced pretreated CRC. In this study, the best response was SD in 20 patients (43.5%) but no objective responses were observed. Seven patients (15.2%) remained progression-free for ≥16 weeks. Median PFS was 1.9 months; median OS was 5.5 months. The most common AEs were diarrhea (80.4%), asthenia (47.8%), nausea (43.5%), and rash (41.3%) ().Citation75 In another Phase II study, nintedanib plus mFOLFOX6 compared to bevacizumab plus mFOLFOX6 were evaluated in 126 patients with previously untreated metastatic CRC. The primary endpoint of this study was the kaplan-meier (KM) estimate of PFS at 9 months, which was 62.1% for the nintedanib regimen and 70.2% for the bevacizumab regimen; a numerical difference in PFS between treatments was −8.1% (95% CI: −27.8 to 11.5). The results for best confirmed overall response were 63.5% (95% CI: 52.4–73.7) for the nintedanib and 56.1% (95% CI: 39.7–71.5) for the bevacizumab group. SD frequency was lower in the nintedanib than in the bevacizumab group (27.1% vs 36.6%). The final analysis of this study demonstrated that the median PFS was 10.5 months in the nintedanib group (95% CI: 9.4–12.4) and 15.4 months in the bevacizumab group (95% CI: 9.6–18.9), which contrasted with a median PFS at the time of the interim analysis (nintedanib: 10.6 months, bevacizumab: 9.2 months). The most frequent AEs (>40% in either group) in the nintedanib vs bevacizumab groups were diarrhea (77.6% vs 68.3%), nausea (70.6% vs 58.5%), asthenia (55.3% vs 61%), neutropenia (47.1% vs 36.6%), vomiting (45.9% vs 34.1%), decreased appetite (31.8% vs 41.5%), and constipation (18.8% vs 46.3%). Incidences of AEs leading to discontinuation of nintedanib or bevacizumab, with or without discontinuation of mFOLFOX, were 27.1% for nintedanib and 31.7% in the bevacizumab group. The overall incidence of serious AEs was lower for the nintedanib group than for the bevacizumab group (37.6% vs 53.7%) ().Citation76,Citation77 A double-blind, randomized, Phase III study of nintedanib vs placebo in refractory CRC is currently ongoing (NCT02149108). Another Phase I/II study of nintedanib in combination with capecitabine in treating patients with refractory metastatic CRC is currently ongoing (NCT02393755).
Nintedanib in breast cancer
In a Phase I study, the combination of nintedanib (150 mg, bid) with a standard preoperative treatment for breast cancer (weekly 80 mg/m2 paclitaxel, followed by adriamycin plus cyclophosphamide) was evaluated in HER-2-negative breast cancer patients.Citation78 At this dose level, the observed toxicity was not different from that reported with paclitaxel alone therapy. The dose-limiting toxicity was transaminase elevation. The dose intensity of both initial drugs, nintedanib and paclitaxel, was 99.9% and 97.4%, respectively. Despite the low number of patients (n=8), the efficacy at this dose level was very promising with a pathological complete response of 50%. Based on these trial data, a randomized Phase II study of docetaxel with or without nintedanib in patients receiving a second-line of chemotherapy for neoadjuvant HER-2-negative breast cancer patients is ongoing (NCT01658462). Another Phase II study of nintedanib monotherapy for patients with metastatic HER2-negative inflammatory breast cancer is also ongoing (NCT02389764).
Based on promising efficacy and safety results of nintedanib in the above-mentioned solid tumors, nintedanib is currently under investigation in several other solid tumors including thyroid cancer (NCT01788982), neuroendocrine tumors (NCT02399215), cervix cancer (NCT02009579), endometrial cancer (NCT01225887), esophagogastric cancer (NCT02234596), urothelial carcinoma (NCT02278978), and glioblastoma (NCT01666600).
Conclusion
Increased understanding of the complexity of tumor angiogenesis pathways indicated the importance of multitargeted antiangiogenic agents to increase tumor response and overcome or delay resistance development. By simultaneous targeting of VEGF, FGF, and PDGF signaling, nintedanib may offer a better approach for the treatment of several solid tumors. The clinical efficacy of nintedanib in combination with docetaxel in NSCLC was recognized by its approval in the European Union. Nintedanib also demonstrated rather encouraging clinical efficacy and tolerability data in patients with different solid tumors, and several additional clinical studies are currently ongoing. There is a good possibility that nintedanib will be approved for at least some of these tumor types in the near future. However, more understanding of nintedanib’s molecular mechanism of action and identifying molecular biomarkers to predict nintedanib response is highly desired to maximize clinical benefits.
Disclosure
The authors report no conflicts of interest in this work.
References
- FolkmanJTumor angiogenesis: therapeutic implicationsN Engl J Med197128521118211864938153
- Al-HuseinBAbdallaMTrepteMDeremerDLSomanathPRAntiangiogenic therapy for cancer: an updatePharmacotherapy201232121095111123208836
- MoreiraISFernandesPARamosMJVascular endothelial growth factor (VEGF) inhibition – a critical reviewAnticancer Agents Med Chem20077222324517348829
- FerraraNVascular endothelial growth factor as a target for anticancer therapyOncologist20049Suppl 121015178810
- ShojaeiFFerraraNAntiangiogenic therapy for cancer: an updateCancer J200713634534818032969
- GiantonioBJCatalanoPJMeropolNJBevacizumab in combination with oxaliplatin, fluorouracil, and leucovorin (FOLFOX4) for previously treated metastatic colorectal cancer: results from the Eastern Cooperative Oncology Group Study E3200J Clin Oncol200725121539154417442997
- SandlerAGrayRPerryMCPaclitaxel-carboplatin alone or with bevacizumab for non-small-cell lung cancerN Engl J Med2006355242542255017167137
- MillerKWangMGralowJPaclitaxel plus bevacizumab versus paclitaxel alone for metastatic breast cancerN Engl J Med2007357262666267618160686
- RiniBIHalabiSRosenbergJEPhase III trial of bevacizumab plus interferon alfa versus interferon alfa monotherapy in patients with metastatic renal cell carcinoma: final results of CALGB 90206J Clin Oncol201028132137214320368558
- MotzerRJHutsonTETomczakPSunitinib versus interferon alfa in metastatic renal-cell carcinomaN Engl J Med2007356211512417215529
- EscudierBEisenTStadlerWMSorafenib in advanced clear-cell renal-cell carcinomaN Engl J Med2007356212513417215530
- SternbergCNDavisIDMardiakJPazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trialJ Clin Oncol20102861061106820100962
- WellsSAJrRobinsonBGGagelRFVandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized, double-blind phase III trialJ Clin Oncol201230213414122025146
- MotzerRJEscudierBTomczakPAxitinib versus sorafenib as second-line treatment for advanced renal cell carcinoma: overall survival analysis and updated results from a randomised phase 3 trialLancet Oncol201314655256223598172
- GrotheyAVan CutsemESobreroARegorafenib monotherapy for previously treated metastatic colorectal cancer (CORRECT): an international, multicentre, randomised, placebo-controlled, phase 3 trialLancet2013381986330331223177514
- Van CutsemETaberneroJLakomyRAddition of aflibercept to fluorouracil, leucovorin, and irinotecan improves survival in a phase III randomized trial in patients with metastatic colorectal cancer previously treated with an oxaliplatin-based regimenJ Clin Oncol201230283499350622949147
- EliseiRSchlumbergerMJMullerSPCabozantinib in progressive medullary thyroid cancerJ Clin Oncol201331293639364624002501
- FuchsCSTomasekJYongCJRamucirumab monotherapy for previously treated advanced gastric or gastro-oesophageal junction adenocarcinoma (REGARD): an international, randomised, multicentre, placebo-controlled, phase 3 trialLancet20143839911313924094768
- RiniBIMichaelsonMDRosenbergJEAntitumor activity and biomarker analysis of sunitinib in patients with bevacizumab-refractory metastatic renal cell carcinomaJ Clin Oncol200826223743374818669461
- EbosJMLeeCRCruz-MunozWBjarnasonGAChristensenJGKerbelRSAccelerated metastasis after short-term treatment with a potent inhibitor of tumor angiogenesisCancer Cell200915323223919249681
- RusnatiMPrestaMFibroblast growth factors/fibroblast growth factor receptors as targets for the development of anti-angiogenesis strategiesCurr Pharm Des200713202025204417627537
- WuEPalmerNTianZComprehensive dissection of PDGF-PDGFR signaling pathways in PDGFR genetically defined cellsPLoS One2008311e379419030102
- CasconeTHerynkMHXuLUpregulated stromal EGFR and vascular remodeling in mouse xenograft models of angiogenesis inhibitor-resistant human lung adenocarcinomaJ Clin Invest201112141313132821436589
- RigamontiNKadiogluEKeklikoglouIWyser RmiliCLeowCCDe PalmaMRole of angiopoietin-2 in adaptive tumor resistance to VEGF signaling blockadeCell Rep20148369670625088418
- FischerCJonckxBMazzoneMAnti-PlGF inhibits growth of VEGF(R)-inhibitor-resistant tumors without affecting healthy vesselsCell200713134647517923087
- EllisLMHicklinDJPathways mediating resistance to vascular endothelial growth factor-targeted therapyClin Cancer Res200814206371637518927275
- AbdullahSEPerez-SolerRMechanisms of resistance to vascular endothelial growth factor blockadeCancer2012118143455346722086782
- BeenkenAMohammadiMThe FGF family: biology, pathophysiology and therapyNat Rev Drug Discov20098323525319247306
- PrestaMDell’EraPMitolaSMoroniERoncaRRusnatiMFibroblast growth factor/fibroblast growth factor receptor system in angiogenesisCytokine Growth Factor Rev200516215917815863032
- HeldinCHWestermarkBMechanism of action and in vivo role of platelet-derived growth factorPhysiol Rev19997941283131610508235
- XieJAszterbaumMZhangXA role of PDGFRalpha in basal cell carcinoma proliferationProc Natl Acad Sci U S A200198169255925911481486
- FunaKPapanicolaouVJuhlinCExpression of platelet-derived growth factor beta-receptors on stromal tissue cells in human carcinoid tumorsCancer Res19905037487532153446
- BornfeldtKERainesEWNakanoTGravesLMKrebsEGRossRInsulin-like growth factor-I and platelet-derived growth factor-BB induce directed migration of human arterial smooth muscle cells via signaling pathways that are distinct from those of proliferationJ Clin Invest1994933126612748132765
- KerbelRSTumor angiogenesisN Engl J Med2008358192039204918463380
- HellstromMKalenMLindahlPAbramssonABetsholtzCRole of PDGF-B and PDGFR-beta in recruitment of vascular smooth muscle cells and pericytes during embryonic blood vessel formation in the mouseDevelopment1999126143047305510375497
- PietrasKSjoblomTRubinKHeldinCHOstmanAPDGF receptors as cancer drug targetsCancer Cell20033543944312781361
- HeldinCHTargeting the PDGF signaling pathway in tumor treatmentCell Commun Signal2013119724359404
- TaegerJMoserCHellerbrandCTargeting FGFR/PDGFR/VEGFR impairs tumor growth, angiogenesis, and metastasis by effects on tumor cells, endothelial cells, and pericytes in pancreatic cancerMol Cancer Ther201110112157216721885862
- KinoshitaKNakagawaKHamadaJImatinib mesylate inhibits the proliferation-stimulating effect of human lung cancer-associated stromal fibroblasts on lung cancer cellsInt J Oncol201037486987720811709
- ErberRThurnherAKatsenADCombined inhibition of VEGF and PDGF signaling enforces tumor vessel regression by interfering with pericyte-mediated endothelial cell survival mechanismsFASEB J200418233834014657001
- BergersGSongSMeyer-MorseNBergslandEHanahanDBenefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitorsJ Clin Invest200311191287129512727920
- CasanovasOHicklinDJBergersGHanahanDDrug resistance by evasion of antiangiogenic targeting of VEGF signaling in late-stage pancreatic islet tumorsCancer Cell20058429930916226705
- FerraraNHillanKJGerberHPNovotnyWDiscovery and development of bevacizumab, an anti-VEGF antibody for treating cancerNat Rev Drug Discov20043539140015136787
- Afranie-SakyiJAKlementGLThe toxicity of anti-VEGF agents when coupled with standard chemotherapeuticsCancer Lett201535711725449430
- HerbstRSToxicities of antiangiogenic therapy in non-small-cell lung cancerClin Lung Cancer20068Suppl 1S23S3017239287
- IacovelliRPalazzoAProcopioGIncidence and relative risk of hepatic toxicity in patients treated with anti-angiogenic tyrosine kinase inhibitors for malignancyBr J Clin Pharmacol201477692993823981115
- CabebeEFisherGAClinical trials of VEGF receptor tyrosine kinase inhibitors in pancreatic cancerExpert Opin Investig Drugs2007164467476
- AroraAScholarEMRole of tyrosine kinase inhibitors in cancer therapyJ Pharmacol Exp Ther2005315397197916002463
- CapdevilaJCarratoATaberneroJGrandeEWhat could Nintedanib (BIBF 1120), a triple inhibitor of VEGFR, PDGFR, and FGFR, add to the current treatment options for patients with metastatic colorectal cancer?Crit Rev Oncol Hematol2014928310624924525
- BroekmanFGiovannettiEPetersGJTyrosine kinase inhibitors: multi-targeted or single-targeted?World J Clin Oncol201122809321603317
- RothGJHeckelAColbatzkyFDesign, synthesis, and evaluation of indolinones as triple angiokinase inhibitors and the discovery of a highly specific 6-methoxycarbonyl-substituted indolinone (BIBF 1120)J Med Chem200952144466448019522465
- HilbergFRothGJKrssakMBIBF 1120: triple angiokinase inhibitor with sustained receptor blockade and good antitumor efficacyCancer Res200868124774478218559524
- RicheldiLdu BoisRMRaghuGEfficacy and safety of nintedanib in idiopathic pulmonary fibrosisN Engl J Med2014370222071208224836310
- EbosJMKerbelRSAntiangiogenic therapy: impact on invasion, disease progression, and metastasisNat Rev Clin Oncol20118421022121364524
- Paez-RibesMAllenEHudockJAntiangiogenic therapy elicits malignant progression of tumors to increased local invasion and distant metastasisCancer Cell200915322023119249680
- SenninoBIshiguro-OonumaTWeiYSuppression of tumor invasion and metastasis by concurrent inhibition of c-Met and VEGF signaling in pancreatic neuroendocrine tumorsCancer Discov20122327028722585997
- Kutluk CenikBOstapoffKTGerberDEBrekkenRABIBF 1120 (nintedanib), a triple angiokinase inhibitor, induces hypoxia but not EMT and blocks progression of preclinical models of lung and pancreatic cancerMol Cancer Ther2013126992100123729403
- TaiWTShiauCWLiYSNintedanib (BIBF-1120) inhibits hepatocellular carcinoma growth independent of angiokinase activityJ Hepatol2014611899724657398
- AwasthiNHinzSBrekkenRASchwarzMASchwarzRENintedanib, a triple angiokinase inhibitor, enhances cytotoxic therapy response in pancreatic cancerCancer Lett20153581596625527450
- HilbergFBrandstetterIEfficacy of BIBF 1120, a potent triple angiokinase inhibitor, in models of human non-small cell lung cancer is augmented by chemotherapyEur J Cancer20072S380
- StopferPRathgenKBischoffDPharmacokinetics and metabolism of BIBF 1120 after oral dosing to healthy male volunteersXenobiotica201141429731121204634
- MrossKStefanicMGmehlingDPhase I study of the angiogenesis inhibitor BIBF 1120 in patients with advanced solid tumorsClin Cancer Res201016131131920028771
- OkamotoIKanedaHSatohTPhase I safety, pharmacokinetic, and biomarker study of BIBF 1120, an oral triple tyrosine kinase inhibitor in patients with advanced solid tumorsMol Cancer Ther20109102825283320688946
- EllisPMKaiserRZhaoYStopferPGyorffySHannaNPhase I open-label study of continuous treatment with BIBF 1120, a triple angiokinase inhibitor, and pemetrexed in pretreated non-small cell lung cancer patientsClin Cancer Res201016102881288920460487
- DoebeleRCConklingPTraynorAMA phase I, open-label dose-escalation study of continuous treatment with BIBF 1120 in combination with paclitaxel and carboplatin as first-line treatment in patients with advanced non-small-cell lung cancerAnn Oncol20122382094210222345119
- ReckMKaiserREschbachCA phase II double-blind study to investigate efficacy and safety of two doses of the triple angiokinase inhibitor BIBF 1120 in patients with relapsed advanced non-small-cell lung cancerAnn Oncol20112261374138121212157
- ReckMKaiserRMellemgaardADocetaxel plus nintedanib versus docetaxel plus placebo in patients with previously treated non-small-cell lung cancer (LUME-Lung 1): a phase 3, double-blind, randomised controlled trialLancet Oncol201415214315524411639
- HannaNKKaiserRSullivanRNLume-lung 2: a multicenter, randomized, double-blind, phase III study of nintedanib plus pem- etrexed versus placebo plus pemetrexed in patients with advanced nonsquamous non-small cell lung cancer (NSCLC) after failure of first-line chemotherapyJ Clin Oncol201331Suppl:8034
- LedermannJAHackshawAKayeSRandomized phase II placebo-controlled trial of maintenance therapy using the oral triple angiokinase inhibitor BIBF 1120 after chemotherapy for relapsed ovarian cancerJ Clin Oncol201129283798380421859991
- du BoisAKristensenGRay-CoquardIAGO-Ovar 12: a randomized placebo-controlled GCIG/ENGOT-intergroup phase III trial of standard frontline chemotherapy ± nintedanib for advanced ovarian cancerInt J Gynecol Cancer201323PL01
- EisenTShparykYJonesRPhase II efficacy and safety study of nintedanib versus sunitinib in previously untreated renal cell carcinoma (RCC) patientsJ Clin Oncol201331abstract 4506
- MeyerTPalmerDHChaoYEfficacy and safety study of nintedanib (N) versus sorafenib (S) in Caucasian and Asian patients with advanced hepatocellular carcinoma (HCC): pooled analysis of two randomized phase II trialsJ Clin Oncol201533abstract 4074
- DrozJPMedioniJChevreauCRandomized phase II study of nintedanib in metastatic castration-resistant prostate cancer postdocetaxelAnticancer Drugs20142591081108824849708
- MolifeLROmlinAJonesRJRandomized Phase II trial of nintedanib, afatinib and sequential combination in castration-resistant prostate cancerFuture Oncol201410221923124490608
- BoucheOMaindrault-GoebelFDucreuxMPhase II trial of weekly alternating sequential BIBF 1120 and afatinib for advanced colorectal cancerAnticancer Res20113162271228121737652
- Van CutsemEPrenenHGuillen-PonceCA phase I/II, open-label, randomised study of BIBF 1120* plus mFOLFOX6 compared to bevacizumab plus mFOLFOX6 in patients with metastatic colorectal cancerEur J Cancer2011478921095116
- Boehringer Ingelheim BTNFRA phase I-II study of BIBF 1120 and Folfox compared to Bevacizumab and Folfox in first line metastatic colorectal cancer patients NLM identifier: 2008-005364-14. Available from: http://trials.boehringer-ingelheim.com/content/dam/internet/opu/clinicaltrial/com_EN/results/1199/1199.51_U12-2578-02_DR.pdfAccessed June 3, 2013
- Quintela-FandinoMUrruticoecheaAGuerraJPhase I clinical trial of nintedanib plus paclitaxel in early HER-2-negative breast cancer (CNIO-BR-01-2010/GEICAM-2010-10 study)Br J Cancer201411161060106425058346