
Abstract
This retrospective study was conducted to evaluate the prognostic significance of the preoperative plasma D-dimer levels and platelet counts in patients with pancreatic adenocarcinoma. A total of 168 consecutive locally advanced pancreatic adenocarcinoma patients who underwent intensity modulated radiation therapy with or without chemotherapy were enrolled in this study. Plasma D-dimer levels were measured by a latex-enhanced immunoturbidimetric assay. Of the 168 patients enrolled, 106 patients were males and 62 patients were females. There was significant difference between plasma D-dimer levels and clinical responses (P=0.001). The 1-year, 2-year, and 3-year cumulative overall survival rates were 50.6%, 15.0%, and 4.9%, respectively. Plasma D-dimer levels (P<0.001) and platelet counts (P=0.010) were significantly related with overall survival in univariate analysis. The Cox proportional hazards regression indicated that plasma D-dimer levels (P=0.028), platelet counts (P=0.004), and treatment response (P<0.001) were independent prognostic factors for overall survival. Elevated pretreatment plasma D-dimer levels and platelet counts predict poor prognosis in pancreatic adenocarcinoma.
Introduction
Pancreatic adenocarcinoma is one of the most extremely malignant neoplasms among all types of cancer in both developing and developed countries.Citation1 The prognosis remains quite poor, with a great number of patients experiencing disease progression in a very short time. Radical surgery is thought to be the only therapy that can provide opportunity for cure and long-time survival.Citation2 However, only 10%–20% of the patients could be candidate for surgical pancreatectomy according to previous reports.Citation3,Citation4 For locally advanced pancreatic adenocarcinoma, combined or sequential chemotherapy and radiotherapy is the standard treatment.Citation5 Several studies have attempted to discover molecular biomarkers to predict the prognosis of pancreatic adenocarcinoma.Citation6,Citation7 However, to date, most of these markers had not been proven to be sufficiently effective.Citation8
The relationship between coagulation and cancer has been studied for more than a century. Recently, coagulation activation, in particular fibrin formation and dissolution, has been implicated in tumor invasion, metastases, and eventual worse outcome in pancreatic adenocarcinoma.Citation9,Citation10 Several studies reported that pretreatment plasma D-dimer levels or platelet counts were prognostic factors in pancreatic adenocarcinoma.Citation10,Citation11 However, majority of these reports focused on metastatic pancreatic adenocarcinoma and the sample was relatively small (less than 80 patients). Therefore, the aim of this study was to determine whether the plasma D-dimer levels and platelet counts before chemoradiotherapy are predictors of mortality in patients with locally advanced unresectable pancreatic adenocarcinoma.
Patients and methods
This survival study was carried out in 168 locally advanced unresectable consecutive pancreatic adenocarcinoma patients who received gemcitabine-based chemoradiotherapy in Zhejiang cancer hospital. All patients were newly confirmed to have pancreatic adenocarcinoma and had not received treatment previously. Patients with other malignancies were excluded from this study. Each case was reassigned for tumor, regional lymph node metastases, and distant organ metastases (tumor node metastasis [TNM] stage) classification and clinical stage according to the American Joint Committee on Cancer (AJCC) staging system.Citation12 The following detail clinical information was retrospectively collected and analyzed for each case: sex, age at treatment, smoking status, tumor location, clinical TNM stage, treatment response, and overall survival (OS) after treatment. Our study was approved by the institutional review board and ethics committee of the hospital. All patients provided informed consent before chemoradiotherapy. OS was calculated as the time from radiotherapy to death or censoring.
Each patient provided two 5 mL blood samples pretreatment. Plasma D-dimer levels were measured by a latex-enhanced immunoturbidimetric assay using a Sysmex CA 7000 (Sysmex Corp, Kobe, Japan) analyzer in Zhejiang cancer hospital. Plasma D-dimer levels ≤0.5 µg/mL was used as cutoff for normal versus high D-dimer values, according to the manufacture’s recommendation. A complete blood count was regularly taken, and high group was defined as platelet count greater than 300×109/L.
Treatment schedule
All patients were treated with intensity modulated radiation therapy (IMRT). Patients were immobilized in a supine position, arms overhead, with thermoplastic cast. Patients underwent CT-simulation on CT scanner (GE, Lightspeed, USA), using 5 mm slices with contrast enhancement. Radiation plans for IMRT were generated using Pinnacle Version 8.0. All patients underwent external beam radiation therapy with 6 MV X-rays. The area of solid macroscopic tumors in pancreas, the surrounding tissue infiltrated, and the regional lymph node metastases were defined as the gross tumor volume (GTV). The GTV plus a margin of at least 5 mm, including any areas of microscopic spread and the regional lymph nodes (peripancreatic, celiac, superior mesenteric, portal hepatic, retroperitoneal), was defined as the clinical target volume (CTV). The plan target volume (PTV) was defined as the CTV plus 0.5–1.0 cm to account for the daily setup variation and respiratory movement. A fractional daily dose of 1.8 Gy (Gray) (5 days per week, over 5 weeks) at an isocenter was prescribed. The median delivered dose of IMRT was 50 Gy (range: 44.0–55.8 Gy). The dose to the adjacent normal structures was constrained as follows: The liver dose was limited to V5<75%, V20<50%, V30<30%, and a mean dose less than 28 Gy. The kidney dose was limited to V12<50% and V22.5<30%. Spinal cord maximum dose was held to 45 Gy. The CTV encompassed at least 95% isodose line. The dose volume histogram (DVH) was obtained for CTV, PTV, spinal cord, liver, and kidney. The small bowel contour was confined to the small bowel loops within 3 cm of the PTV and was limited to maximal dose <54 Gy.
Concurrent chemoradiotherapy, with or without adjuvant chemotherapy, was used in 103 patients. The chemotherapy regimens consisted of S1 at 50 mg/m2 twice daily from days 1 to 14 or gemcitabine at 1,000 mg/m2 on day 1 and day 8 of a 21 days cycle. The CR (complete response), PR (partial response), SD (stable disease), and PD (progressive disease) were assessed at an interval of at least 4 weeks to confirm the objective response. All patients received standardized follow-up, occurring at 3 months interval for 2 years, 6 months interval the 3rd year, and yearly thereafter. Evaluations comprised a physical examination, pancreatic CT, complete blood count, liver and kidney function tests, abdominal ultrasound, chest radiography, and pelvic CT.
Statistical analysis
Data was presented as median ± standard error. The chi-square test was performed to evaluate the association between the clinicopathological variables and plasma D-dimer levels or platelet counts. OS time was defined as the time interval from the initial event (radiotherapy) to the death or censoring. Survival curves were estimated by the univariate Kaplan–Meier method. The log-rank test was applied to check the significant difference in the curves among groups. Furthermore, we used the Cox proportional hazards model with the backward selection method for multivariate analysis. All statistical calculations were performed with SPSS 13.0 software for Windows (Chicago, IL, USA). Two-sided t-test P-values of <0.05 were considered to be statistically significant.
Results
Characteristics of patients
The characteristics of these patients are summarized in . Of the 168 patients enrolled, 106 patients were males and 62 patients were females. The study population had a median age of 61 years (range: 34–83 years). On the basis of image parameters, tumor was found with regional lymph node metastases in 89 (53.0%) patients. The numbers of T1, T2, T3, and T4 tumor patients were 17 (10.1%), 28 (16.7%), 77 (45.8%), and 46 (27.4%), respectively. The size of tumor was between 2.2 and 10 cm in most pancreatic adenocarcinomas.
Table 1 Relationship between clinicopathological parameters, plasma D-dimer levels (>0.5 µg/mL vs ≤0.5 µg/mL), and platelet counts (>300×109/L vs ≤300×109/L) in 168 patients with pancreatic adenocarcinoma
Plasma D-dimer levels, platelet counts, and characteristics of patients
The median of plasma D-dimer levels and platelet counts in total patients was 1.03 µg/mL (range: 0.11–6.45 µg/mL) and 169×109/L (range: 54–696×109/L). Plasma D-dimer levels were above 0.5 µg/mL in 125 patients (74.4%). The incidence of high platelet counts was 13.1% (22/168). No significant correlation was observed between clinical parameters (like sex, age, tumor location, tumor size, T stage, and N stage) and plasma D-dimer levels or platelet counts (P>0.05, ). There were 14 patients who had a CR, and 48, 99, and 7 patients had PR, SD, and PD, respectively. There was significant difference between plasma D-dimer levels and clinical responses (P<0.001). There was a higher ratio of SD and PD for the patients with high plasma D-dimer levels (83.0%) than those with normal plasma D-dimer levels (17.0%). However, no significant difference was observed between platelet counts and treatment response (P>0.05).
Prognostic relevance of clinicopathological parameters, plasma D-dimer, and platelet counts
The follow-up was conducted from 3 to 48 months with a median period of 14 months. During the follow-ups, 148 patients (88.1%) died of disease progression. The 1-year, 2-year, and 3-year cumulative OS rates were 50.6%, 15.0%, and 4.9%, respectively. We evaluated the prognostic values of the pretreatment plasma D-dimer, platelet counts, and other clinicopathological parameters, as shown in . Compared with high levels of plasma D-dimer, normal levels owned a better 2-year OS rate (18.1% vs 9.9%, P<0.001, ). The median OS time was shorter in patients with platelet counts >300×109/L than in those with platelet counts ≤300×109/L (9 months vs 12 months, P=0.010, ). Additionally, lymph node metastases (P=0.035), plasma CA 199 levels (P=0.023), and treatment response (P<0.001) were significantly related with OS in univariate analysis.
Figure 1 Cumulative survival curves for overall survival time according to pretreatment plasma D-dimer levels.
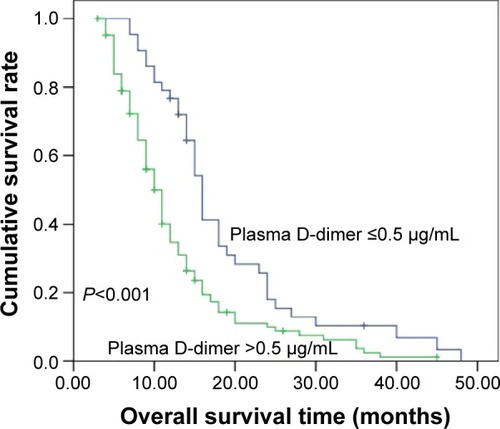
Figure 2 Cumulative survival curves for overall survival time according to pretreatment platelet counts.
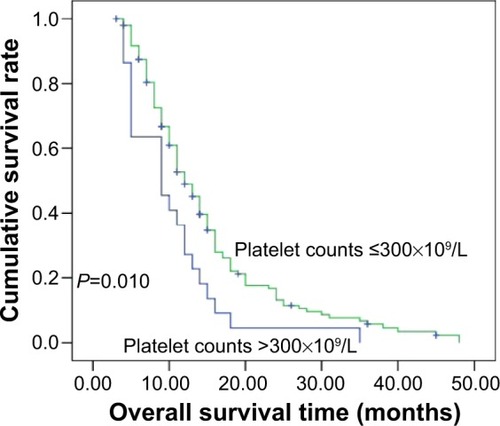
Table 2 Prognostic relevance of clinicopathological parameters, plasma D-dimer levels, and platelet counts in the univariate analysis
We performed multivariate analysis on the factors that were statistically significant in the univariate analysis. The results are shown in . The Cox proportional hazards regression indicated that plasma D-dimer levels (P=0.028), platelet counts (P=0.004), and treatment response (P<0.001) were independent prognostic factors for OS.
Table 3 Prognostic relevance of N stage, serum CA199 levels, plasma D-dimer levels, platelet counts, and treatment response in the multivariate analysis
Discussion
Recently, more attention has been given to the association between the progression of malignancies and coagulation. Hypercoagulability is a sign of a more aggressive disease. Elevated plasma D-dimer levels and platelet counts are correlated with worse outcome in patients with epithelial ovarian cancer,Citation13 lung cancer,Citation14 and colorectal cancer.Citation15 In this study, we find that elevated pretreatment plasma D-dimer levels and platelet counts were associated with poorer pro gnosis in pancreatic adenocarcinoma patients receiving IMRT. Patients with elevated plasma D-dimer levels had 1.65 times the risk of death compared with those with normal plasma D-dimer levels. Patients with platelet counts >300×109/L had 2.23 times the risk of death compared with those with platelet counts ≤300×109/L.
D-dimer is a stable fibrin degradation product. Plasma D-dimer is a marker of hypercoagulation, usually used for the assessment of suspect venous thromboembolism.Citation16 Increased plasma D-dimer levels are also observed in patients with myocardial infarction, infectious disease, trauma, and pre gnancy.Citation17 There are several reports regarding the role of plasma D-dimer in patients with pancreatic adenocarcinoma. Durczynski et alCitation18 analyzed 64 potentially resectable pancreatic tumor without detectable venous thrombosis. Only 45.3% of the patients enrolled were found to be resectable. High plasma D-dimer levels can predict the unresectability of pancreatic cancer. There have also been reports regarding the prognostic significance of the D-dimer level in patients with pancreatic cancer. In a retrospective study,Citation19 73 pancreatic cancer were followed over 2 years. Elevated plasma D-dimer levels are associated with poor prognosis according to multivariate survival analysis. However, this study did not determine whether the increased mortality among pancreatic cancer patients with elevated plasma D-dimer levels is independent of venous thromboembolism. Furthermore, the sample in this study is small. The author did not present the detailed information about the tumor stage and treatment regimen. Platelets serve various roles in physiological pathways, including coagulation and inflammation. Increased platelet counts at the time of diagnosis are associated with significantly short survival time among patients with solid tumors.Citation20 Brown et alCitation21 undertook a chart review of patients undergoing resection for pancreatic adenocarcinoma. They analyzed 109 patients with resected pancreatic adenocarcinoma and found that platelet counts are independent prognostic biomarkers for OS in operable pancreatic cancer. Similarly, Dominguez et alCitation22 reported the prognostic significance of the platelet count based on an analysis of operable 205 patients with pancreatic ductal adenocarcinoma. Although these results somewhat overlapped with present study, we have additionally adjusted for some strong prognostic factors, such as CA199 and treatment response. Therefore, the strength of the current study was direct comparison of plasma D-dimer levels and platelet counts in pancreatic adenocarcinoma under the same treatment. Also, it seems more homogeneous because no postoperative venous thromboembolism events were found during the follow-up.
However, the exact mechanism underlying D-dimer mediated pancreatic adenocarcinoma progression remains unclear. Tumor cells could convert fibrinogen to fibrin. D-dimer, which is a stable fibrinogen degradation product, was shown to be associated with tumor progression and an elevated plasma D-dimer levels may reflect ongoing fibrinogen metabolism within actively remodeling tumor stroma.Citation23 Second, increased expression of tissue factor, which is also expressed by tumor cells, will activate coagulation cascades and ultimately lead to fibrin deposition, tumor growth, and tumor cell metastases.Citation24 Furthermore, plasma D-dimer levels may reflect the presence of micrometastases or circular tumor cells, which may be responsible for tumor recurrence.Citation25 The formation of a clot around the tumor cells in the circulation also prevents the tumor cells from being killed by natural killer cells.Citation26 The exact reason for the association between elevated platelet counts and worse outcome of pancreatic adenocarcinoma still remains unknown. Increased platelet counts may promote tumor cell growth and angiogenesis. Platelets release various cytokines, including vascular endothelial growth factor (VEGF) and platelet-derived growth factor (PDGF), during blood clotting. The VEGF and PDGF family of proteins play significant roles in regulating angiogenesis. The invasiveness of the cancer cells may be enhanced by the plasma components in stored platelets.Citation20
Our study has several limitations. Our study may be limited by the relatively small sample analyzed and retrospective design. Second, plasma D-dimer levels and platelet counts were checked only once in each patient and were not examined during the follow-up. Furthermore, the follow-up time was relatively short and information on posttreatment recurrence was insufficient, which we are planning to analyze in the future.
Our results suggest that pretreatment plasma D-dimer levels and platelet counts could be served as new independent prognostic biomarkers for OS in pancreatic adenocarcinoma. Plasma D-dimer levels and platelet counts should be assessed in the workup of patients with pancreatic adenocarcinoma in future trials to confirm their prognostic significance.
Acknowledgments
We are grateful to the patients who are included in this study. This study was supported by grants from the Nature Science Foundation of Zhejiang province (No. LY14H160012).
Disclosure
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- SiegelRLMillerKDJemalACancer statistics, 2015CA: Cancer J Clin201565152925559415
- MiuraTHiranoSNakamuraTA new preoperative prognostic scoring system to predict prognosis in patients with locally advanced pancreatic body cancer who undergo distal pancreatectomy with en bloc celiac axis resection: a retrospective cohort studySurgery2014155345746724462074
- ReberHAGloorBRadical pancreatectomySurg Oncol Clin N Am1998711571639443993
- BeggCBCramerLDHoskinsWJBrennanMFImpact of hospital volume on operative mortality for major cancer surgeryJAMA199828020174717519842949
- HuguetFGirardNGuercheCSHennequinCMornexFAzriaDChemoradiotherapy in the management of locally advanced pancreatic carcinoma: a qualitative systematic reviewJ Clin Oncol: Official J Am Soc Clin Oncol2009271322692277
- ZhangLJWangKBLiuLSOverexpression of GOLPH3 is associated with poor prognosis and clinical progression in pancreatic ductal adenocarcinomaBMC Cancer20141457125104140
- HouYCChaoYJTungHLWangHCShanYSCoexpression of CD44-positive/CD133-positive cancer stem cells and CD204-positive tumor-associated macrophages is a predictor of survival in pancreatic ductal adenocarcinomaCancer2014120172766277724839953
- WinterJMYeoCJBrodyJRDiagnostic, prognostic, and predictive biomarkers in pancreatic cancerJ Surg Oncol20131071152222729569
- WangHGaoJBaiMThe pretreatment platelet and plasma fibrinogen level correlate with tumor progression and metastasis in patients with pancreatic cancerPlatelets201425538238724001199
- TasFKarabulutSBilginEKilicLCiftciRDuranyildizDClinical significance of coagulation assays in metastatic pancreatic adenocarcinomaJ Gastrointest Cancer201344440440923765155
- AliustaogluMBiliciASekerMThe association of pre-treatment peripheral blood markers with survival in patients with pancreatic cancerHepato Gastroenterol20105799–100640645
- RindiGFalconiMKlersyCTNM staging of neoplasms of the endocrine pancreas: results from a large international cohort studyJ Nat Cancer Inst20121041076477722525418
- ManYNWangYNHaoJPretreatment plasma d-dimer, fibrinogen, and platelet levels significantly impact prognosis in patients with epithelial ovarian cancer independently of venous thromboembolismInt J Gynecol Cancer: Official J Int Gynecol Cancer Soc20152512432
- AntoniouDPavlakouGStathopoulosGPPredictive value of D-dimer plasma levels in response and progressive disease in patients with lung cancerLung Cancer200653220521016769149
- StenderMTLarsenTBSorensenHTThorlacius-UssingOPreoperative plasma D-dimer predicts 1-year survival in colorectal cancer patients with absence of venous thromboembolism (VTE): a prospective clinical cohort studyJ Thrombosis Haemostasis: JTH2012101020272031
- PabingerIAyCBiomarkers and venous thromboembolismArteriosclerosis, thrombosis, and vascular biology: ATVB2009293332336
- LippiGFranchiniMTargherGFavaloroEJHelp me, Doctor! My D-dimer is raisedAnnal Med2008408594605
- DurczynskiAKumorAHogendorfPSzymanskiDGrzelakPStrzelczykJPreoperative high level of D-dimers predicts unresectability of pancreatic head cancerWorld J Gastroenterol: WJG201420361316713171
- AyCDunklerDPirkerRHigh D-dimer levels are associated with poor prognosis in cancer patientsHaematologica20129781158116422371182
- BuergyDWenzFGrodenCBrockmannMATumor-platelet interaction in solid tumorsInt J Cancer2012130122747276022261860
- BrownKMDominCAranhaGVYongSShoupMIncreased preoperative platelet count is associated with decreased survival after resection for adenocarcinoma of the pancreasAm J Surg2005189327828215792750
- DominguezICrippaSThayerSPPreoperative platelet count and survival prognosis in resected pancreatic ductal adenocarcinomaWorld J Surg20083261051105618224462
- BlackwellKHaroonZBroadwaterGPlasma D-dimer levels in operable breast cancer patients correlate with clinical stage and axillary lymph node statusJ Clin Oncol: Official J Am Soc Clin Oncol2000183600608
- KasthuriRSTaubmanMBMackmanNRole of tissue factor in cancerJ Clin Oncol: Official J Am Soc Clin Oncol2009272948344838
- FukumotoKTaniguchiTUsamiNThe preoperative plasma D-dimer level is an independent prognostic factor in patients with completely resected non-small cell lung cancerSurg Today2015451636724781600
- PalumboJSTalmageKEMassariJVPlatelets and fibrin(ogen) increase metastatic potential by impeding natural killer cell-mediated elimination of tumor cellsBlood2005105117818515367435