
Abstract
Aim
To investigate whether pretreatment assessment of experimental pain can predict the level of pain after archwire placement.
Methods
One hundred and twenty-one general university students seeking orthodontic treatment were enrolled in this study. A cold pressor test was performed to estimate the pain tolerance of subjects before treatment. Self-reported pain intensity was calculated using a 10 cm visual analog scale during the 7 days after treatment. The relationship between pain tolerance and orthodontic pain was analyzed using Spearman’s correlation analysis.
Results
The maximum mean level of pain intensity occurred at 24 hours after bonding (53.31±16.13) and fell to normal levels at day 7. Spearman’s correlation analysis found a moderate positive association between preoperative pain tolerance and self-reported pain after archwire placement (P<0.01). There was no significant difference in pain intensity between male and female patients at any time point (P>0.05).
Conclusion
A simple and noninvasive preoperative sensory test (the cold pressor test) was useful in predicting the risk of developing unbearable pain in patients after archwire placement. Self-reported pain after archwire placement decreased as individual pain tolerance increased.
Keywords:
Introduction
Mild-to-severe acute pain occurs in >90% of patients undergoing orthodontic treatment.Citation1,Citation2 Despite the developing technology in orthodontics, most patients still experience some discomfort or pain in relation to orthodontic treatment, especially during the 7 days after archwire placement.Citation3 The reasons for the wide variation in patients’ experience of pain after similar types of orthodontic treatment have been widely discussed. It is believed that the experience of pain consists of sensory perceptions of intensity and discomfort and can also be influenced by cognitive, emotional, and environmental factors.Citation4,Citation5 Previous researchers attributed the immediate and delayed pain response to inflammatory reactions causing changes in blood flow following orthodontic force application. This procedure makes the periodontal ligament sensitive to released algogens such as histamine, prostaglandins, bradykinin, and serotonin.Citation6,Citation7 The increased levels of these mediators elicit a pain response following orthodontic force application.
Various methods of pain control have been developed for use during orthodontic treatment, including nonsteroidal anti-inflammatory drugs (NSAIDs),Citation8 low-level laser therapy,Citation9,Citation10 transcutaneous electrical neural stimulation,Citation11 and vibratory stimulation.Citation12 Until now, the use of NSAIDs has been the preferred and most successful method of pain control. However, NSAIDs may cause side effects, including thrombocytopenia, headaches, and skin rashes. It is important to estimate the level of personal pain perception to gage how well a patient will tolerate postoperative pain in orthodontics. This may help the orthodontist select an appropriate method of pain control that tailors the risk–benefit ratio of using NSAIDs in particular patients. As a result, some patients could require lower doses of analgesic drugs with a lower risk of side effects. Nevertheless, prediction of pain is difficult because of various influencing factors. Some previous researchers have studied the relationship between orthodontic pain and psychological factors or personality traits,Citation13,Citation14 but such studies require extensive resources to collect and analyze the data for each patient. Furthermore, the reliability and validity of psychological assessment are difficult without the professional assistance of a psychologist.
The aim of this study was to investigate whether pretreatment assessment of experimental pain perception using a cold pressor test could predict the level of pain after archwire placement.
Methods
Ethical approval for the study was granted by the Health Research Ethics Board at Wenzhou Medical University. Each patient was given oral and written information and signed a written consent form before participating in the study.
The research was designed as a prospective study. A total of 121 general university students seeking orthodontic treatment were recruited from the Orthodontic Department of Wenzhou Medical University, Wenzhou, People’s Republic of China, between January 2014 and May 2015. The following exclusion criteria were applied: had undergone previous orthodontic treatment, was currently taking any antibiotics or analgesics, had a systemic disease, had third molars extracted, or experienced anxiety (trait anxiety inventory score: male patients ≥56 and female patients ≥57 or state anxiety inventory score: male patients ≥53 and female patients ≥55). All patients had moderate crowding (4–8 mm according to Little’s irregularity index) and agreed to have orthodontic treatment with fixed upper and lower appliances (0.022×0.028 inch, Victory Series™; 3M Company; Maplewood, MN, USA). Tooth alignment and leveling began with a 0.012-inch nickel–titanium archwire (Grikin Advanced Materials Co. Ltd, Beijing, People’s Republic of China), and the ligation was performed by one trained orthodontist using AlastiK™ (3M Unitek). All subjects needed four first premolars extracted. The right upper and lower premolars were extracted first, and the left upper and lower premolars were extracted 1 week later. All premolars were successfully extracted within 5 minutes after anesthesia. The archwire was placed at least 2 weeks after the extractions.
Before extraction of the premolars, a cold pressor test was performed to assess pain tolerance by measuring the time of immersion (in seconds) of the subject’s hand in ice water. All subjects were informed that the maximum test duration would be 240 seconds, and they were asked to remove their hand when they could no longer tolerate the pain. Cold water and ice cubes (v:v, 2:1; temperature, 0°C–1°C) were mixed 15 minutes before testing in an isolated tank. To ensure uniform temperature distribution within the tank, the mixture was stirred immediately before the test. A thermometer was placed in the water so that the water temperature could be monitored and maintained at 0°C–1°C. Subjects were asked to immerse their nondominant hand with the palm gently resting on the bottom of the tank.Citation15 An isolated room was used to ensure that subjects were not distracted and that the examiner did not communicate with the subjects verbally or nonverbally. The subjects were asked to rate the intensity of the most intense pain felt during the immersion period on a visual analog scale (VAS) record immediately after removing their hand from the water or after the maximum exposure of 240 seconds.
The state–trait anxiety inventory was used preoperatively to assess subjects’ anxiety before entering the dentist’s room. The test was conducted by the same investigator for all patients.
The participants were asked to report pain intensity by completing a VAS questionnaire at the first visit and 24 hours after the premolars were extracted. This take-home questionnaire consisted of a 10 cm line, and subjects were asked to mark a location on the line corresponding to the highest pain intensity experienced during the 24 hours after the extractions, from no pain “0” to severe/unbearable pain “100”. Subjects with baseline pain intensity ratings >5 mm were included. Then, the participants were asked again to complete the VAS questionnaire before bonding as “zero time” (T0), 24 hours after bonding (T1), 2 days after bonding (T2), 4 days after bonding (T3), and 7 days after bonding (T4). During the period of investigation, patients were asked to eat soft foods and not to use analgesics unless they were experiencing unbearable pain. All participants were informed of the possible occurrence of pain, ulcers, and difficulty in chewing.
Statistical Package for the Social Sciences (SPSS for Windows, version 15.0; SPSS Inc., Chicago, IL, USA) was used to analyze the research data. The Kolmogorov–Smirnov test was used to verify the distribution of the data. Variables with asymmetrical distribution were described using the median and interquartile range. The relationship between the experimental pain perception and orthodontic pain was analyzed using Spearman’s correlation analysis. The Wilcoxon signed-rank test was performed to observe differences between male and female patients. Comparisons between the different times were performed using the Friedman test. The results were evaluated within a 95% confidence interval. The statistical significance level was established at P<0.05.
Results
Nine patients used analgesics during the research, and eight patients quit or did not finish the questionnaire. Finally, a total of 121 subjects were recruited for the present research. The demographic characteristics of the participants are shown in . Eleven participants immersed their hand for the maximum test duration. The mean (interquartile range) preoperative pain tolerance of male and female patients was 71.3 (57–116) and 53.1 (35–81), respectively. Male patients had significantly better tolerance than female patients (P<0.01). The self-reported pain intensity during the cold pressor test was 65.13±19.26. There was no statistically significant sex difference in reported pain intensity during the cold pressor test (P=0.12). The state and trait anxiety scores in subjects were 38.83±5.02 and 38.12±4.82, respectively.
Table 1 Demographic characteristics of the subjects
Pain intensity as reported by subjects on a VAS (0–100) from extraction to orthodontic treatment is shown in . The Kolmogorov–Smirnov test showed that pain intensity only exhibited a normal distribution at T1, T2, and T3. Spearman’s correlation coefficient between preoperative pain tolerance scores and the highest pain experienced after extraction (r=0.57; P<0.01), pain intensity at T1 (r=0.71; P<0.01), T2 (r=0.69; P<0.01), T3 (r=0.73; P<0.01), and T4 (r=0.62; P<0.01) was significant, indicating a moderate positive association between preoperative pain tolerance scores and pain after archwire placement.
Table 2 Pain intensity on a visual analog scale (0–100) from extraction to orthodontic treatment
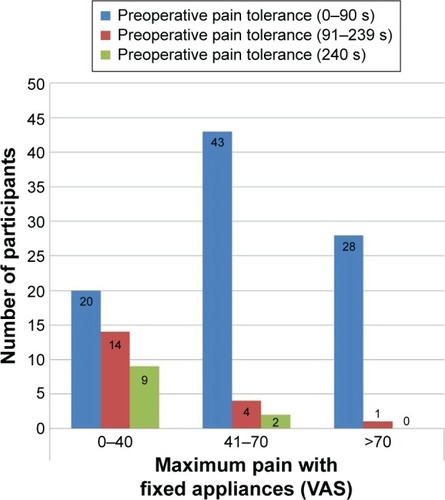
Differences in pain intensity at each time point after archwire placement are shown in . The maximum mean level of pain intensity occurred at 24 hours after bonding (53.31±16.13), and then the pain gradually reduced. shows the distribution of participants according to pain intensity and preoperative pain tolerance. Only one participant, who had a pain tolerance of >90 seconds in the cold pressor test, completed the VAS questionnaire with a score of >70. There was no significant difference in reported pain intensity between male and female patients at any time point (P>0.05).
Figure 1 Pain intensity at each time point as reported by subjects using a 10 cm visual analog scale.
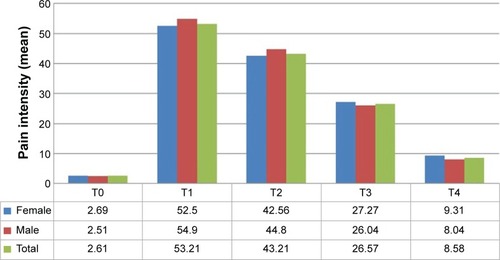
Figure 2 The distribution of participants according to pain intensity and preoperative pain tolerance.
Discussion
Different preoperative sensory tests have been shown to predict postoperative pain.Citation16–Citation19 Among these tests, the cold pressor test provides a valid and low-risk test for evaluating pain in patients and has been routinely used in pain research. This study was the first to use a cold pressor test as a preoperative pain assessment method to predict pain in orthodontic patients from East China and found a moderate positive association between preoperative pain tolerance scores and pain after archwire placement.
All participants included in this study were students with similar psychosocial characteristic and treatment plans; this design could have decreased the influence of cognitive differences, which might have affected pain perception. The cognitive component of pain includes attentional processes, anticipation, and memory of past experiences of pain.Citation20 Many affective states, including anxiety, fear, depression, stress, and panic, are potentially important in the experience and expression of pain.Citation21
In the cold pressor test, the water temperature was monitored and sustained at 0°C–1°C, because a 2°C difference in temperature can affect tolerance time and pain intensity.Citation19 The painful sensation was determined by a multitude of factors that included objective and subjective domains. It would be difficult to use a cross-sectional study to control impact factors of pain perception; therefore, we chose a self-controlled study to examine the prediction of pain in orthodontic patients. Most of the previous studies have focused on the sensory aspect of pain, asking participants to report pain intensity using the VAS,Citation13,Citation22,Citation23 which has been found to be reliable and valid;Citation24,Citation25 therefore, we also used it in this study.
An important limitation of previous studies of pain in orthodontics is that the orthodontic treatment procedures are usually not controlled, and various procedures may be performed. In this study, standardized procedures and materials were used by one researcher. Specifically, the standard procedure consisted of extracting four first premolars, placing an archwire, and performing ligation. It has been reported that subjects with superelastic nickel–titanium archwires experience significantly higher pain than those with multistranded stainless steel archwires at the peak level.Citation26 A randomized clinical trial found that self-ligating brackets resulted in lower pain intensity than conventional twin brackets;Citation27 however, a systematic review of self-ligating bracket studies concluded that currently there is insufficient evidence to support significant differences in subjective pain experience between self-ligating and conventional appliances.Citation28
Differences in pain perception between male and female patients have been increasingly studied in recent years. Mitchell et alCitation19 and Riley et al observed sex differences, with men having better tolerance for pain stimuli than women.Citation29 A similar phenomenon was observed in this study. It is generally assumed that gonadal hormones contribute to greater clinical and experimental pain experiences in female patients as compared with male patients.Citation30 However, inconsistent findings have been reported in more recent studies.Citation31,Citation32 In the orthodontic literature, some studies comparing pain perception with fixed appliances found that male patients reported lower pain intensity than female patients,Citation1,Citation33 while others found no statistically significant differences between sexes,Citation34,Citation35 and the latter case prevailed in our study. This finding may be related to the different study design and inclusion criteria of the participants. The maximum mean pain for subjects peaked at 24 hours, as reported in the previous research.Citation26 The mean preoperative pain tolerance of nine subjects who used analgesics during the research was 28.3 (range: 11–39), which is much lower than the normal mean value. The results of this research could help dentists use analgesic drugs more effectively and reasonably, and patients at high risk for pain might benefit from preemptive analgesic interventions. Conversely, patients at low risk could manage with less or no analgesic medication.
Limitations
A limitation of this study is that psychosocial metrics were not taken at the time of the cold pressor test, prior to extraction, postextraction, or at archwire bonding to ensure that the subjects were experiencing the same trait at each event; this may have influenced the results for self-reported pain. This study cannot completely explain the variable experiences of orthodontic pain because of the small sample. Therefore, further research involving larger samples is needed to obtain a more comprehensive result, together with analysis of other contributing factors such as anxiety and gonadal steroid hormones.
Conclusion
This research used a simple and noninvasive preoperative sensory test (the cold pressor test) to investigate the relationship between experimental pain and self-reported pain after archwire placement. The self-reported pain after archwire placement decreased as individual pain tolerance increased. There was no statistically significant sex difference in self-reported pain after archwire placement.
Disclosure
The authors report no conflicts of interest in this work.
References
- ScheurerPAFirestoneARBurginWBPerception of pain as a result of orthodontic treatment with fixed appliancesEur J Orthod19961843493578921656
- LewKKAttitudes and perceptions of adults towards orthodontic treatment in an Asian communityCommunity Dent Oral Epidemiol199321131358432102
- FarzaneganFZebarjadSMAlizadehSAhrariFPain reduction after initial archwire placement in orthodontic patients: a randomized clinical trialAm J Orthod Dentofacial Orthop2012141216917322284284
- MelzackRWallPDPain mechanisms: a new theoryScience196515036999719795320816
- BergiusMKiliaridisSBerggrenUPain in orthodontics. A review and discussion of the literatureJ Orofac Orthop200061212513710783564
- KrishnanVOrthodontic pain: from causes to management – a reviewEur J Orthod200729217017917488999
- PolatOKaramanAIPain control during fixed orthodontic appliance therapyAngle Orthod200575221421915825785
- PolatOKaramanAIDurmusEEffects of preoperative ibuprofen and naproxen sodium on orthodontic painAngle Orthod200575579179616279825
- EslamianLBorzabadi-FarahaniAHassanzadeh-AzhiriABadieeMRFekrazadRThe effect of 810-nm low-level laser therapy on pain caused by orthodontic elastomeric separatorsLasers Med Sci201429255956423334785
- LimHMLewKKTayDKA clinical investigation of the efficacy of low level laser therapy in reducing orthodontic postadjustment painAm J Orthod Dentofacial Orthop199510866146227503039
- AllgoodJPTranscutaneous electrical neural stimulation (TENS) in dental practiceCompend Contin Educ Dent1986796406426443490950
- MarieSSPowersMSheridanJJVibratory stimulation as a method of reducing pain after orthodontic appliance adjustmentJ Clin Orthod2003374205208 quiz 203–20412747073
- Abu AlhaijaESAldaikkiAAl-OmairiMKAl-KhateebSNThe relationship between personality traits, pain perception and attitude toward orthodontic treatmentAngle Orthod20108061141114920677967
- BergiusMBrobergAGHakebergMBerggrenUPrediction of prolonged pain experiences during orthodontic treatmentAm J Orthod Dentofacial Orthop20081333339.e1339.e818331926
- WalshNESchoenfeldLRamamurthySHoffmanJNormative model for cold pressor testAm J Phys Med Rehabil19896816112917058
- StrulovLZimmerEZGranotMTamirAJakobiPLowensteinLPain catastrophizing, response to experimental heat stimuli, and postcesarean section painJ Pain20078327327917113350
- PanPHCoghillRHouleTTMultifactorial preoperative predictors for postcesarean section pain and analgesic requirementAnesthesiology2006104341742516508387
- WernerMUDuunPKehletHPrediction of postoperative pain by preoperative nociceptive responses to heat stimulationAnesthesiology20041001115119 discussion 115A14695732
- MitchellLAMacDonaldRABrodieEETemperature and the cold pressor testJ Pain20045423323715162346
- PeyronRGarcia-LarreaLGregoireMCHaemodynamic brain responses to acute pain in humans: sensory and attentional networksBrain1999122pt 91765178010468515
- KeefeFJLumleyMAndersonTLynchTStudtsJLCarsonKLPain and emotion: new research directionsJ Clin Psychol200157458760711255208
- WangJTangXShenYThe correlations between health-related quality of life changes and pain and anxiety in orthodontic patients in the initial stage of treatmentBiomed Res Int2015201572591325685804
- SerglHGKlagesUZentnerAPain and discomfort during orthodontic treatment: causative factors and effects on complianceAm J Orthod Dentofacial Orthop199811466846919844209
- SeymourRASimpsonJMCharltonJEPhillipsMEAn evaluation of length and end-phrase of visual analogue scales in dental painPain19852121771853982841
- Abu-SaadHAssessing children’s responses to painPain19841921631716462728
- SandhuSSSandhuJA randomized clinical trial investigating pain associated with superelastic nickel-titanium and multistranded stainless steel archwires during the initial leveling and aligning phase of orthodontic treatmentJ Orthod201340427628524297959
- PringleAMPetrieACunninghamSJMcKnightMProspective randomized clinical trial to compare pain levels associated with 2 orthodontic fixed bracket systemsAm J Orthod Dentofacial Orthop2009136216016719651344
- FlemingPSJohalASelf-ligating brackets in orthodontics. A systematic reviewAngle Orthod201080357558420050755
- RileyJL3rdRobinsonMEWiseEAMyersCDFillingimRBSex differences in the perception of noxious experimental stimuli: a meta-analysisPain1998742–31811879520232
- FillingimRBKingCDRibeiro-DasilvaMCRahim-WilliamsBRileyJL3rdSex, gender, and pain: a review of recent clinical and experimental findingsJ Pain200910544748519411059
- KlatzkinRRMechlinBGirdlerSSMenstrual cycle phase does not influence gender differences in experimental pain sensitivityEur J Pain2010141778219217329
- KowalczykWJEvansSMBisagaAMSullivanMAComerSDSex differences and hormonal influences on response to cold pressor pain in humansJ Pain20067315116016516820
- JonesMChanCThe pain and discomfort experienced during orthodontic treatment: a randomized controlled clinical trial of two initial aligning arch wiresAm J Orthod Dentofacial Orthop199210243733811456222
- ErdincAMDincerBPerception of pain during orthodontic treatment with fixed appliancesEur J Orthod2004261798514994886
- NganPKessBWilsonSPerception of discomfort by patients undergoing orthodontic treatmentAm J Orthod Dentofacial Orthop198996147532750720