
Abstract
Background and objective
Adherence to treatment in patients with psoriasis is often poor. An investigation of patient preferences and satisfaction with treatment may be important, based on the expected correlation with therapy compliance. This paper aims to examine and describe the current literature on patient preferences, satisfaction and adherence to treatment for psoriasis in the European Union (EU).
Methods
Electronic searches were conducted using PubMed, ISI Web of Knowledge, Scopus, Spanish databases and Google Scholar. European studies published in English or Spanish between January 1, 2009 and December 31, 2014 regarding patient-reported outcomes in psoriatic patients were included. Studies conducted in non-EU countries, letters to the editor, editorials, experts’ opinions, case studies, congress proceedings, publications that did not differentiate between patients with psoriasis and psoriatic arthritis or studies related to specific treatment were excluded.
Results
A total of 1,769 titles were identified, of which 1,636 were excluded as they were duplicates or did not provide any relevant information. After a full-text reading and application of the inclusion/exclusion criteria, 46 publications were included. This paper will describe publications on adherence (n=4), preferences (n=5) and satisfaction with treatment (n=7). Results related to health-related quality of life articles (n=30) have been published elsewhere. Adherence rates are generally low in psoriasis patients regardless of the type of treatment, severity of disease or methods used to measure adherence. Biologic therapy is associated with greater clinical improvement. There is a direct association between physician recommendations, patient preferences and several domains of treatment satisfaction.
Conclusion
The results of this review support the conclusion that adherence rates in patients with psoriasis are suboptimal and highlight the need to improve patient compliance and satisfaction with treatment. Patients’ preferences should be taken into account in the treatment decision-making process in order to improve patients’ clinical outcomes by ensuring satisfaction and adherence.
Introduction
Psoriasis is a common chronic inflammatory disease of the skin and joints that is typically characterized by erythematous papules and plaques.Citation1–Citation3 Estimates of the worldwide prevalence of psoriasis range from 1% to 3%Citation4–Citation6 and it affects ~2% of the population in Europe.Citation7,Citation8 The disease can present at any age, but the mean age of onset for the first presentation of psoriasis ranges from 15 to 20 years, with a second peak occurring at 55–60 years.Citation9 Although psoriasis is not a life-threatening disease, it has a negative effect on patients’ health-related quality of life (HRQoL), similar to that of other major medical conditions.Citation9–Citation12
The severity of disease is related to the extension of the cutaneous manifestations and is defined by the Psoriasis Area and Severity Index (PASI) or as a percentage of the total body surface area (BSA).Citation13 The majority of psoriasis patients suffer from mild disease (PASI ≤10), which can often be managed with topical agents, while phototherapy or systemic therapies are usually used for patients with moderate-to-severe psoriasis (PASI >10). In the last decade, significant advances in the management and treatment of psoriasis have been made with the introduction of biologic agents,Citation14,Citation15 which have shown greater clinical benefit than traditional systemic therapies.Citation16–Citation22
With more than 90% of psoriasis patients having a chronic condition, adherence to treatment is crucial for successful disease management and reduction in clinical severity.Citation23 However, it is estimated that nearly 40% of patients with psoriasis do not use medication as prescribed.Citation4,Citation24,Citation25 In addition to non-adherence, psoriasis is consistently associated with treatment dissatisfaction.Citation3,Citation26–Citation28 As satisfaction is closely associated with patient preferences and compliance with treatment,Citation29 taking patients’ opinions about available treatment options into consideration may be crucial to improving satisfaction and adherence, thereby increasing the effectiveness of the treatment and HRQoL.
The introduction of biologic therapies over the past 10 years has further increased the therapeutic options for moderate-to-severe psoriasis. Although all of these biologic agents are highly effective and show a favorable risk–benefit profile, differences in efficacy, rapidity of action and sustainability do exist. This makes the decision-making process regarding the most suitable therapeutic strategy more complex for both patients and physicians, underlining the need to elucidate patients’ treatment preferences. This review aims to examine and describe the current literature on patient preferences, satisfaction and adherence to treatment for psoriasis in the European Union (EU).
Methods
We performed a systematic review of the literature on adherence to treatment, satisfaction with therapy, patient preferences for treatment and HRQoL in psoriatic patients in the EU. In order to obtain an accurate insight into how novel treatment options (available in European countries since 2005) have influenced patient-reported outcomes (PROs), studies from January 1, 2009 to December 31, 2014 were included. International (Medline/pubMed, cochrane Ligrary, ISI Web of knowledge [ISI WOK], SCOPUS) and Spanish electronic databases (Medicina en Español [MEDES], Índice Bibliográfico Español en Ciencias de la Salud [IBECS]) and Google Scholar were used to search the literature. The English and Spanish search terms used are summarized in .
Original articles, reviews and systematic reviews in English or Spanish that evaluated treatment adherence and satisfaction, patient preferences for treatment and HRQoL in psoriatic patients from a European perspective were included in the review. Publications about all of the treatments available for psoriasis (topical, systemic and biologic agents) were included. On the other hand, studies conducted in non-EU countries, original letters to the editor, editorials, experts’ opinions, case studies, congress proceedings, studies with mixed populations including patients with psoriasis (with or without psoriatic arthritis) and patients with psoriatic arthritis alone or studies related to specific treatments were excluded. The selection of publications was performed by two independent researchers and discrepancies were resolved by consensus.
The methodological quality of the studies was assessed by assigning a level of evidence and recommendation based on criteria developed by the Centre for Evidence-Based Medicine (CEBM).Citation30
Results
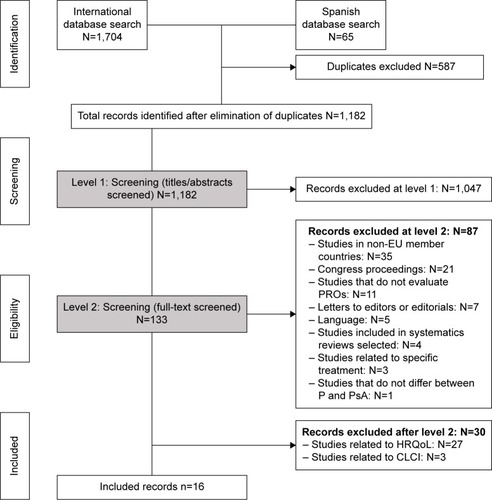
A total of 1,769 titles were identified, of which 587 (33.2%) were duplicates and therefore excluded. The other 1,182 (66.8%) were excluded because they did not provide any relevant information. After full-text reading and application of the inclusion/exclusion criteria, 46 of the remaining 133 publications were included in the review (). Twenty-seven (58.7%) articles were related to HRQoL, seven (15.2%) evaluated treatment satisfaction, five (10.9%) examined treatment preferences, four (8.7%) explored treatment adherence and three (6.5%) described cumulative life course impairment (CLCI). Results related to HRQoL (n=27) and CLCI articles (n=3) have been published elsewhere.Citation31
Figure 1 PRISMA diagram of systematic review process.
The present article examines and describes the 16 studies, published in the EU between January 1, 2009 and December 31, 2014, that were selected and which related to psoriasis patients’ preferences for treatment, adherence and satisfaction.
Characteristics of selected studies
These 16 studies included the following designs: 4 conjoint analyses, 2 reviews, 1 systematic review, 4 prospective studies, 3 cross-sectional studies and 1 retrospective study. Nearly half were conducted in Germany (n=7), two in the UK, two in Spain, two in the Netherlands, one in Italy and two were multicenter studies across different European countries. The level of evidence in the majority of the studies (n=12) was grade 2c and their CEBM recommendation was grade B, which indicates moderate evidence.
Treatment adherence in patients with psoriasis
Of the 16 studies, 4 (25%) examined adherence to medical therapies. Three of them were reviews, which evaluated rates and determinants of adherence, while the fourth article selected was a Delphi consensus study conducted in Spain.
The systematic review undertaken by Thorneloe et alCitation32 consistently reported low rates of treatment adherence, regardless of the type of treatment, disease severity or type of adherence measurement used (). Even though there were inconsistent findings with regard to the predictive factors of adherence, studies investigating the role of psychological factors revealed that increased psychological distress and low patient satisfaction with care or therapy were associated with lower levels of adherence. In line with these results, Bewley and PageCitation24 confirmed that rates of adherence to topical medications were low, with 39%–73% of psoriasis patients not using medications as prescribed and revealed that effectiveness and the characteristics of the treatment (cosmetic acceptability) were the main contributors for increasing adherence to psoriasis medication. Moreover, they identified that prescribing therapy in line with patient preferences or improving patient education may result in increased adherence. Similarly, Zschocke et alCitation33 established that the reasons for non-adherence to treatment amongst psoriasis patients revolve mainly around treatment vehicle, patient–physician relationship or patient motivation. These authors propose that given that the barriers to medication adherence are complex and varied, solutions to improve adherence should be multifaceted and allow tailoring according to each patient’s individual needs.
Table 1 Adherence rates
Finally, the Delphi study conducted by Puig et alCitation34 with a panel of experts from the Psoriasis Group of the Spanish Academy of Dermatology and Venereology reached a consensus that in order to improve adherence to topical treatment, it was necessary 1) to improve communication between patients and health care staff, 2) to provide written instructions and 3) to simplify treatment with easy-to-use and pleasant products that were preferably applied only once a day. In addition, the panelists agreed that treatment satisfaction increased adherence and tended to improve the HRQoL of psoriasis patients, highlighting the relationship between treatment satisfaction and treatment adherence.
Taken together, these studies draw attention to the low rates of adherence to psoriasis treatments and highlight the importance of involving patients in treatment decision-making, in order to improve their adherence to treatment.
Treatment satisfaction in patients with psoriasis
The following section summarizes seven articles related to treatment satisfaction of patients with psoriasis and to variations depending on type of treatment, demography and clinical factors. Five articles used study-specific questionnaires, while the other two studies assessed patient’s satisfaction using the Treatment Satisfaction Questionnaire for Medication (TSQM) ().
Table 2 Characteristics of treatment satisfaction studies reviewed
Schaarschmidt et alCitation35 revealed the high impact of the type of treatment on satisfaction scores. Participants receiving biologicals (TSQM: 323.3) and traditional systemic treatments (TSQM: 288.0) were more satisfied than those receiving phototherapy (TSQM: 260.6) or topical agents (TSQM: 266.8; P<0.001). These authors also observed that high disease-related HRQoL impairment, as measured by the Dermatology Life Quality Index (DLQI), and psoriatic arthritis were associated with decreased treatment satisfaction. In line with these results, van Cranenburgh et alCitation36 indicated that, overall, patients with psoriasis were moderately satisfied with their current treatment, with patients receiving biologic treatments being the most satisfied, compared to other groups (total satisfaction score [range from 5= not satisfied to 25= very satisfied]: topical [16.5], phototherapy [18.3], systemic [19.5], biologics [0.9]). These authors identified age (t[1182] =2.9; P=0.004) and disease severity (t[1882] =−18.6; P<0.001) as predictive factors of satisfaction. Similarly, Ragnarson Tennvall et alCitation37 described the highest treatment satisfaction, that is, 8.2 (scale of 0 not at all satisfied to 10 very satisfied) in patients who had been treated with biological drugs for 12 months, followed by patients who received systemic treatment for less than 12 months (6.5) and patients receiving topical treatment (5.7). Van den Reek et alCitation38 confirmed the high satisfaction rates achieved with biologic treatment, with statistically significant (P<0.05) improvements in the “efficacy”, “convenience” and “global satisfaction” domains of TSQM after 3 and 6 months initiation of biologic therapy.
Two studies assessed the relationship between psoriasis severity (PASI) and satisfaction. Schäfer et alCitation39 showed that, while most patients who achieved PASI 75 (92.3%) indicated that their expectations with the treatment were met, this applied to only half (53.1%) of patients with PASI 50 and to 36.4% of patients with lower clinical treatment success (PASI <50). In relation to satisfaction with the condition of their skin after therapy, 84.6% of patients who achieved PASI 75 were completely or predominantly satisfied; this proportion was reduced to 43.7% and 36.4% in the PASI 50 and PASI <50 groups, respectively. Christophers et alCitation40 observed that the percent of PASI reduction in patients with severe psoriasis who received biologic therapy was significantly greater than in patients who received topical therapy, phototherapy or traditional systemic therapy (79% vs 55%, 47%, 69%, P<0.001). Thus, a reduction in PASI contributed to an increase in treatment satisfaction. More patients receiving biologic therapy were satisfied (highly or completely) with their current treatment than patients receiving any other therapy (59% patients receiving biologic therapy vs 50% patients receiving traditional systemic therapy vs 34% patients receiving phototherapy vs 45% patients receiving topical agents only; P<0.001).
In line with these results, in a study published by Ribera et al,Citation41 with the aim of developing a satisfaction questionnaire (Spanish Satisfaction with Treatment of Psoriasis Questionnaire) and assess its validity, reliability and sensitivity to change, patients with severe psoriasis scored higher [(0= highest satisfaction; 48= highest dissatisfaction), 27; SD: 2.6] than patients with moderate psoriasis (22.6; SD: 9.5). These authors described a weak correlation between reduction in PASI score during a 12-month study period and improvement in satisfaction.
In summary, satisfaction studies indicated that patients receiving biologic therapy were more satisfied and their satisfaction was correlated to improvements in clinical features (mainly measured by PASI score).
Patient preferences for therapies in psoriasis
Five publications examined patient preferences for treatment; four of them described the results of a conjoint analysis based on a discrete choice experiment that aimed to analyze the preferences of individuals with moderate or severe psoriasis for outcome and process attributesCitation42–Citation45 (). In a study published by Schaarschmidt et al,Citation42 the attribute regarded as most important was treatment location (where the treatment takes place) (relative importance score [RIS]: 26.76), followed by probability of benefit (RIS: 23.77) and method of delivery (RIS: 23.49). The RISs for all process attributes were higher than for adverse effect (AE)-related attributes, indicating that participants were willing to trade an increased risk of AEs for increased probability and magnitude of therapeutic benefit. Age, disease severity (PASI score) and household income were the only factors that affected preferences. Older participants (≥65 years) found the probability of benefit less important than younger participants (P=0.005); patients with intermediate incomes (€1,000–€2,000 per month) granted less importance to treatment delivery method compared with patients with lower income; patients with higher PASI score considered the probability of benefit as less important (P=0.02) but the frequency of treatment more important compared with participants with a lower PASI score (P=0.04). Schaarschmidt et alCitation43 described the impact of treatment experience (satisfaction with current treatment, number of prior visits, disease duration, number of preceding therapies and currently prescribed treatment modalities) on treatment preferences. With regard to disease and treatment duration, participants with longer disease duration attached greater importance to the duration of benefit (β=0.206, P=0.018), whereas participants on oral therapy were more concerned about magnitude of benefit by trend (β=0.218, P=0.058). Participants receiving injectable therapy not only set higher value to probability of benefit (RIS =32.80 vs 21.89, P=0.025) but also to treatment location (RIS =44.74 vs 23.03, P=0.011), delivery method and treatment frequency (RIS =31.24 vs 16.89, P=0.005) and duration (RIS =32.54 vs 16.57, P=0.003) compared to others.Citation43 These results suggest that treatment preferences change over the course of time and with treatment experience. Participants on injectable therapy attached great importance to the effectiveness and convenience of treatment and were highly satisfied with it. As reported by Umar et al,Citation44 prolonged treatments in the inpatient setting (Mean Preference Score [MPS]: −13.48) and those with a lower probability of benefit (MPS: −12.28) were the least preferred while treatments with a high probability of benefit (MPS: 10.51) were most preferred. Patients were more concerned about improvement of their skin condition than about the reversibility or the severity of treatment side effects. Using data from the conjoint analysis, Umar et alCitation45 published a prospective cohort study which assessed the extent to which matching physicians’ treatment recommendations to patients’ treatment preferences was associated with improvement in treatment. The results of the study suggested that a closer match between physicians’ recommendations and patients’ preferences was associated with greater improvement in treatment satisfaction over time in each of the four subscales: effectiveness (β=0.53, P<0.001), side effects (β=0.25, P=0.009), convenience (β=0.78, P<0.001) and global satisfaction (β=0.49, P<0.001).
Table 3 Characteristics of preferences related studies reviewed
Finally, Torbica et alCitation46 conducted a discrete choice experiment on 244 Italian psoriatic patients. Overall, patients preferred the subcutaneous or intravenous route of administration (vs oral administration) and treatments that took less time to show improvement, ensured a longer time free of symptoms, involved a lesser reduction in life expectancy and had lower costs. In general, older patients placed significantly greater importance on reduced life expectancy, whereas time free of symptoms was less important to them than to patients under 60 years of age. Patients with high DLQI scores placed higher value on time free of symptoms than those with lower DLQI scores.
Data from these studies offer a focus on patients’ preferences for psoriasis treatment and suggest that when making decisions about treatment, the heterogeneity of patient’s expectations and preferences should be considered in order to identify individualized treatments that would aid in optimizing patient satisfaction and well-being, as well as overall treatment effectiveness.
Discussion
Despite the heterogeneity of the articles selected in terms of patients, treatment and methodology features, the information obtained from the studies included in this review provides an assessment of the challenge of non-adherence in psoriasis, together with an identification of patients’ preferences and levels of satisfaction regarding the medications currently approved for the treatment of psoriasis in the EU.
According to the results reported, adherence rates in patients with psoriasis were generally low and were influenced by multiple factors, such as the characteristics of patients and the treatments, treatment effectiveness, patient–physician relationship or patient motivation. However, findings were inconsistent with regard to predictive factors of adherence.
In addition to treatment adherence, this review investigated current knowledge regarding patient preferences and satisfaction with available treatment options for psoriasis. The results highlight that patients receiving biologic treatment were consistently more satisfied compared to those receiving traditional systemic therapies, while patients receiving topical therapies were the least satisfied. Moreover, the positive association between clinical treatment success and satisfaction suggested that the use of effective drugs that provide greater reduction in disease severity (PASI score) may contribute to higher rates of satisfaction.
Several studies conducted outside the EU support these results. Overall satisfaction scores, as measured by the TSQM, obtained in a cross-sectional study of 1,182 moderate-to-severe psoriasis patients conducted by Callis Duffin et alCitation47 in the US, were highest for patients receiving biologic monotherapies, biologic combinations or photo-therapy (83.3), while scores were lowest for those receiving topical therapies only (66.7). Significant correlations were found between overall survival and both PASI (ρ=−0.36, P<0.001) and DLQI (ρ=−0.47, P<0.001). Similarly, Finch et alCitation48 reported that levels of satisfaction with phototherapy and systemic treatments were high; conversely, there were higher levels of dissatisfaction with topical treatments.
Regarding patients’ preferences, psoriasis patients attach greater importance to process attributes (treatment location, method of delivery, frequency, duration and cost) than to outcome attributes (probability, magnitude or duration of benefit and AE probability, reversibility or severity) when selecting treatment. Although the probability of benefit was also highly considered, psoriasis patients appear to be willing to accept treatment-related AEs if the process characteristics of psoriasis treatment provide a better fit with their personal and professional life. Treatment preferences may change over time and with treatment experience. Recently, in a study conducted by Kromer et al,Citation49 the most important attributes in relation to biologic agents for patients with moderate-to severe psoriasis were safety (probability of severe AE) and efficacy (probability of 90% improvement). With regard to efficacy, although a 75% improvement in PASI score (PASI 75) is generally considered the gold standard of treatment efficacy in the clinical setting in patients with psoriasis,Citation50 when the advances obtained with biologic therapy are considered, PASI 90 may represent the best meaningful clinical response, particularly in patients with very severe psoriasis.Citation51
Additionally, these authors have revealed that preferences vary with sociodemographic characteristics and working status. Of note, men were more concerned about the probability of symptom improvement than women, and women attached greater value to treatment frequency than men. Older participants judged the probability of improvement less important than younger patients but they worried more about severe side effects. Finally, patients with a full-time job gave more value to time until response, treatment location and treatment frequency than non-working patients.Citation49
In line with these data, a review that aimed to examine the published evidence regarding patient preferences and satisfaction in rheumatoid arthritis,Citation52 process attributes, such as vehicle, and treatment location attributes were also very important for patients with rheumatoid arthritis. In addition, when given a choice among various therapeutic options, these patients chose a biologic or combination therapy that included a biologic agent.
The overall results suggested that incorporating patient preferences into treatment decision-making may contribute to improve treatment satisfaction, adherence and thus, clinical outcome.
Possible limitations of this review included the small number of papers retrieved. This may be due to the exclusion of studies published before the introduction of biologic treatments. In addition, there may be relevant papers in languages other than English or Spanish or that are indexed in databases other than those searched, which we did not identify. Nevertheless, as all the studies included European populations, this review reflects the disease characteristics of homogeneous populations in industrialized countries.
Finally, it is important to point out that, although there were differences between study designs, populations, outcome parameters and the treatments compared among the publications included, the information with regard to adherence and PROs in psoriasis that was obtained from our comprehensive search was very robust and valuable in terms of facilitating shared decision-making during the clinical encounter.
Conclusion
The results of this review support the conclusion that adherence rates in patients with psoriasis are suboptimal, highlight the need to improve treatment compliance and add satisfaction with treatment to enhance the HRQoL for patients with psoriasis. To this end, a better understanding of the factors that motivate and discourage patient participation in treatment is necessary. Patient preferences should be taken into account in the treatment decision-making process in order to improve patients’ clinical outcomes by ensuring satisfaction and adherence.
Supplementary material
Table S1 Search terms and research strategies used in international and Spanish databases
Disclosure
The study was sponsored by Novartis Farmacéutica S.A. The authors report no other conflicts of interest in this work.
References
- SchönMPBoehnckeWHPsoriasisN Engl J Med2005352181899191215872205
- GelfandJMTroxelABLewisJDThe risk of mortality in patients with psoriasis: results from a population-based studyArch Dermatol2007143121493149918086997
- SternRSNijstenTFeldmanSRMargolisDJRolstadTPsoriasis is common, carries a substantial burden even when not extensive, and is associated with widespread treatment dissatisfactionJ Investig Dermatol Symp Proc200492136139
- AugustinMHollandBDartschDLangenbruchARadtkeMAAdherence in the treatment of psoriasis: a systematic reviewDermatology2011222436337421757881
- KurdSKGelfandJMThe prevalence of previously diagnosed and undiagnosed psoriasis in US adults: results from NHANES 2003–2004J Am Acad Dermatol200960221822419022533
- MenterAGottliebAFeldmanSRGuidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologicsJ Am Acad Dermatol200858582685018423260
- FerrándizCCarrascosaJMToroMPrevalencia de la psoriasis en España en la era de los agentes biológicos. [Prevalence of Psoriasis in Spain in the Age of Biologics]Actas Dermosifiliogr20141055504509 Spanish24569109
- LebwohlMGBachelezHBarkerJPatient perspectives in the management of psoriasis: results from the population-based Multinational Assessment of Psoriasis and Psoriatic Arthritis SurveyJ Am Acad Dermatol2014705871881e1e3024576585
- LangleyRGKruegerGGGriffithsCEPsoriasis: epidemiology, clinical features, and quality of lifeAnn Rheum Dis200564Supp 2ii18ii2315708928
- BhosleMJKulkarniAFeldmanSRBalkrishnanRQuality of life in patients with psoriasisHealth Qual Life Outcomes200643516756666
- ChalmersRJAssessing psoriasis severity and outcomes for clinical trials and routine clinical practiceDermatol Clin2015331577125412783
- RappSRFeldmanSRExumMLFleischerABJrReboussinDMPsoriasis causes as much disability as other major medical diseasesJ Am Acad Dermatol1999413 Pt 140140710459113
- MrowietzUReichKPsoriasis – new insights into pathogenesis and treatmentDtsch Arztebl Int20091061–21118 quiz 919564982
- FeldmanSRGartonRAverettWBalkrishnanRValleeJStrategy to manage the treatment of severe psoriasis: considerations of efficacy, safety and costExpert Opin Pharmacother2003491525153312943482
- MillerDWFeldmanSRCost-effectiveness of moderate-to-severe psoriasis treatmentExpert Opin Pharmacother20067215716716433581
- BrunassoAMPuntoniMSalviniCTolerability and safety of biological therapies for psoriasis in daily clinical practice: a study of 103 Italian patientsActa Derm Venereol2011911444921088813
- SaccomaniCPenzSGuerre-SchmidtRUtilisation des biothérapies dans le psoriasis modéré à sévère : expérience du service de dermatologie du CHU de Besançon (2004–2008). [Biological therapy for psoriasis: practical experience at a French dermatology unit]Ann Dermatol Venereol200913612877882 French20004312
- BerendsMADriessenRJLangewoutersAMBoezemanJBVan De KerkhofPCDe JongEMEtanercept and efalizumab treatment for high-need psoriasis. Effects and side effects in a prospective cohort study in outpatient clinical practiceJ Dermatolog Treat2007182768317520463
- de GrootMAppelmanMSpulsPIde RieMABosJDInitial experience with routine administration of etanercept in psoriasisBr J Dermatol2006155480881416965432
- MazzottaAEspositoMCostanzoAChimentiSEfficacy and safety of etanercept in psoriasis after switching from other treatments: an observational studyAm J Clin Dermatol200910531932419658444
- AntoniouCStefanakiIStratigosAInfliximab for the treatment of psoriasis in Greece: 4 years of clinical experience at a single centreBr J Dermatol201016251117112319906069
- WarrenRBBrownBCLaveryDAshcroftDMGriffithsCEBiologic therapies for psoriasis: practical experience in a U.K. tertiary referral centreBr J Dermatol2009160116216918808412
- CarrollCLFeldmanSRCamachoFTBalkrishnanRBetter medication adherence results in greater improvement in severity of psoriasisBr J Dermatol2004151489589715491434
- BewleyAPageBMaximizing patient adherence for optimal outcomes in psoriasisJ Eur Acad Dermatol Venereol201125Suppl 491421507078
- RichardsHLFortuneDGGriffithsCEAdherence to treatment in patients with psoriasisJ Eur Acad Dermatol Venereol200620437037916643132
- DubertretLMrowietzURankiAEUROPSO Patient Survey GroupEuropean patient perspectives on the impact of psoriasis: the EUROPSO patient membership surveyBr J Dermatol2006155472973616965422
- KruegerGKooJLebwohlMMenterASternRSRolstadTThe impact of psoriasis on quality of life: results of a 1998 National Psoriasis Foundation patient-membership surveyArch Dermatol2001137328028411255325
- NijstenTMargolisDJFeldmanSRRolstadTSternRSTraditional systemic treatments have not fully met the needs of psoriasis patients: results from a national surveyJ Am Acad Dermatol2005523 Pt 143444415761421
- LecluseLLTutein NoltheniusJLBosJDSpulsPIPatient preferences and satisfaction with systemic therapies for psoriasis: an area to be exploredBr J Dermatol200916061340134319416228
- Centre for Evidence-Based Medicine [homepage on the Internet]CEBMOxford, UKCentre for Evidence-Based Medicine2014 Available from: http://www.cebm.net/?o=1025Accessed April 22, 2015
- ObradorsMBlanchCComellasMFiguerasMLizanLHealth-related quality of life in patients with psoriasis: a systematic review of the European literatureQual Life Res Epub201663
- ThorneloeRJBundyCGriffithsCEAshcroftDMCordingleyLAdherence to medication in patients with psoriasis: a systematic literature reviewBr J Dermatol20131681203122963128
- ZschockeIMrowietzUKarakasiliEReichKNon-adherence and measures to improve adherence in the topical treatment of psoriasisJ Eur Acad Dermatol Venereol201428Suppl 24924684738
- PuigLCarrascosaJMBelinchónIPanel de Expertos del Consenso Delphi sobre Tratamiento tópico de la psoriasisGrupo de Psoriasis de la Academia Española de Dermatología y VenereologíaAdherence and patient satisfaction with topical treatment in psoriasis, and the use, and organoleptic properties of such treatments: a Delphi study with an expert panel and members of the Psoriasis Group of the Spanish Academy of Dermatology and VenereologyActas Dermosifiliogr2013104648849623395400
- SchaarschmidtMLKromerCHerrRSchmiederAGoerdtSPeitschWKTreatment satisfaction of patients with psoriasisActa Derm Venereol201595557257825394584
- van CranenburghODde KorteJSprangersMAde RieMASmetsEMSatisfaction with treatment among patients with psoriasis: a web-based survey studyBr J Dermatol2013169239840523565643
- Ragnarson TennvallGHjortsbergCBjarnasonATreatment patterns, treatment satisfaction, severity of disease problems, and quality of life in patients with psoriasis in three Nordic countriesActa Derm Venereol201393444244523138500
- van den ReekJMvan LüumingPPOteroMESatisfaction of treatment with biologics in high in psoriasis: results from the Bio-CAPTURE networkBr J Dermatol201417051158116524484403
- SchäferIHackerJRustenbachSJRadtkeMFranzkeNAugustinMConcordance of the Psoriasis Area and Severity Index (PASI) and patient-reported outcomes in psoriasis treatmentEur J Dermatol2010201626719822480
- ChristophersESegaertSMilliganGMoltaCTBoggsRClinical improvement and satisfaction with biologic therapy in patients with severe plaque psoriasis: results of a European cross-sectional observational studyJ Dermatolog Treat201324319319822620684
- RiberaMDaudénEPuigLDesign and validation of a questionnaire to measure treatment satisfaction in patients with moderate-to-severe psoriasis: the NEODERMA study. [Diseño y validación de un cuestionario para medir la satisfacción con el tratamiento del paciente con psoriasis moderada y grave: estudio NEODERMA]Actas Dermosifiliogr201110212838 Spanish21315859
- SchaarschmidtMLSchmiederAUmarNPatient preferences for psoriasis treatments: process characteristics can outweigh outcome attributesArch Dermatol2011147111285129422106115
- SchaarschmidtMLUmarNSchmiederAPatient preferences for psoriasis treatments: impact of treatment experienceJ Eur Acad Dermatol Venereol201327218719822225546
- UmarNSchöllgenITerrisDDIt is not always about gains: utilities and disutilities associated with treatment features in patients with moderate-to-severe psoriasisPatient Prefer Adherence2012618719422536054
- UmarNSchaarschmidtMSchmiederAPeitschWKSchöllgenITerrisDDMatching physicians’ treatment recommendations to patients’ treatment preferences is associated with improvement in treatment satisfactionJ Eur Acad Dermatol Venereol201327676377022631875
- TorbicaAFattoreGAyalaFEliciting preferences to inform patientcentred policies: the case of psoriasisPharmacoeconomics201432220922324446282
- Callis DuffinKYeungHTakeshitaJPatient satisfaction with treatments for moderate-to-severe plaque psoriasis in clinical practiceBr J Dermatol2014170367268024266717
- FinchTShimTNRobertsLJohnsonOTreatment satisfaction among patients with moderate-to-severe psoriasisJ Clin Aesthet Dermatol201584263026060515
- KromerCSchaarschmidtMLSchmiederAHerrRGoerdtSPeitshWKPatient preferences for treatment of psoriasis with biological: a discrete choice experimentPLoS One2015106e012912026058083
- MrowietzUKragballeKReichKDefinition of treatment goals for moderate to severe psoriasis: a European consensusArch Dermatol Res2011303111020857129
- TorresTPuigLTreatment goals for psoriasis: should PASI 90 become the standard of care?Actas Dermosifiiogr20151063155157
- BartonJLPatient preferences and satisfaction in the treatment of rheumatoid arthritis with biologic therapyPatient Prefer Adherence2009333534420016797