
Abstract
Background
Many placebo-controlled studies have demonstrated that allergen immunotherapy (AIT) is an effective therapy for treating allergies. Both commonly used routes, subcutaneous (SCIT) and sublingual immunotherapy (SLIT), require high patient adherence to be successful. In the literature, numbers describing adherence vary widely; this investigation compares these two routes of therapy directly.
Methods
All data were retrieved from the patient data management system of a center for dermatology, specific allergology, and environmental medicine in Germany. All 330 patients (aged 13–89 years) included in this study had commenced AIT between 2003 and 2011, thus allowing a full 3-year AIT cycle to be considered for each investigated patient.
Results
In this specific center, SCIT was prescribed to 62.7% and SLIT to 37.3% of all included patients. The total dropout rate of the whole patient cohort was 34.8%. Overall, SLIT patients showed a higher dropout rate (39.0%) than did SCIT patients (32.4%); however, the difference between these groups was not significant. Also, no significant difference between the overall dropout rates for men and for women was observed. A Kaplan–Meier curve of the patient collective showed a remarkably high dropout rate for the first year of therapy.
Conclusion
The analysis presented in this single-center study shows that most patients who discontinue AIT do so during the first year of therapy. Patients seem likely to finish the 3-year therapy cycle if they manage to adhere to treatment throughout the first year. Strategies for preventing nonadherence in AIT, therefore, need to be developed and standardized in future investigations.
Introduction
For more than a century, allergen immunotherapy (AIT) has been the only disease-modifying therapy to treat allergies. AIT targets freedom from symptoms and can be administered through subcutaneous (SCIT) or sublingual immunotherapy (SLIT) routes.Citation1,Citation2 Major studies have proven the efficiency of AIT,Citation3 although this treatment modality requires patients to be adherent for at least 3 yearsCitation4 for it to succeed. This requirement outlines the main challenge: patients are rarely adherent to long-term therapy of chronic diseases.Citation5 Adherence to the available forms of AIT–SCIT and SLIT–appears to be no exception. In the literature, figures on adherence to SCIT and to SLIT differ immensely. SLIT adherence rates are reported to be between 7% and 82%, whereas SCIT adherence rates range from 23% to 55%.Citation5–Citation8 Reasons for nonadherence vary with the most commonly cited reasons for nonadherence to SLIT being nonperception of efficacy, costs, and side effects.Citation9–Citation11
Four dimensions of causes for nonadherence are usually mentioned: patient-centered factors, health care delivery factors, disease-related factors, and treatment-related factors.Citation12 The complexity and variety of factors influencing adherence to AIT are extensive.Citation13
SCIT has been available in Germany for decades, whereas the first SLIT drops were registered in Germany in 2004 and the first SLIT grass tablet in 2006.Citation14 To gain a broader picture of the adherence to these two common routes of therapy, we decided to analyze the differences between adherence to SCIT and adherence to SLIT in patients at one private allergy center in Germany. By analyzing patient adherence in only one physician’s practice retrospectively, we were able to avoid bias resulting from different health care delivery procedures and to obtain data that were immediately comparable.
Materials and methods
Population
Data were retrieved from one German private allergy center providing care to patients who have statutory or private health insurance. Therefore, all health care expenses and medication costs were reimbursed 100%. Data of patients who had started AIT in 2003 or later had been saved in the center’s practice management system (MediSoftware, Kiel, Germany). The patient information was evaluated anonymously and retrospectively.
This study included patients who had begun AIT between 2003 and 2011, allowing a full 3-year cycle to be pictured for each patient. In all, 330 patients aged 13–89 years were involved in this analysis. Besides demographical data, the patients’ former and current diagnoses, medication as well as forms and duration of therapy were also documented. Furthermore, the personal allergy history and the allergen spectrum, that is, whether the patients were monosensitized or polysensitized, were also assessed.
The practice
Data were obtained in a private practice with two locations, both in Hamburg, Germany. The participating physicians were specialized in dermatology with a subspecialization in allergology. This specialization involves 2-year training, board certification, and further continuing medical education. In all, 1,825 patients were diagnosed with allergic rhinitis between 2003 and 2011, 330 (18.1%) of whom were eligible for immunotherapy according to the German guidelines.
Immunotherapy
In total, 83 different allergen extracts from 9 manufacturers were prescribed to the patients. The allergen extracts most often prescribed were for allergy to the pollen of grass, birch tree, alder tree, hazel tree, wheat, and rye, as well as for allergy to house dust mites and wasps. For a detailed summary of the SCIT and SLIT compounds used ().
Table 1 Allergen extracts used in the SCIT and SLIT patients studied
SCIT compounds were based either on native, nonmodified extracts that used unchanged conformation of allergens, or on polymerized allergoids. Semidepot allergen extracts were applied most often, which contain native or modified allergens that are based on calcium phosphate, tyrosine, or aluminum hydroxide.
SLIT compounds were prescribed as drops or tablets containing allergoids or native allergens. According to the manufacturer, some of the tablets or drops required storage in a refrigerator or at room temperature.
Following the German guidelines for AIT, SCIT patients were required to stay at the practice for at least 30 minutes after each injection so that any possible anaphylactic reactions could be treated immediately. SLIT patients received their first tablet or drops under observation and had to remain in the practice for 30 minutes. Thereafter, SLIT treatment was self-administered by the patients; the patients were able to renew their prescription by phone and continue their treatment at home.Citation15
Mode of therapy
The different modes of therapy were prescribed taking into consideration the patient’s preferred route of therapy, the allergy itself, the manufacturer’s recommendations, the patient’s allergy history, and the patient’s personal circumstances.
Preseasonal modes were usually administered for seasonal allergies, and allergens were only given for 4 months before each season. The dosage of allergens was increased to a maximum in a short amount of time just before the season and was discontinued for the duration of the season and the time immediately after (8 months). A complete treatment cycle (including interruptions) lasted at least 28 consecutive months ().
Figure 1 Preseasonal mode of immunotherapy.
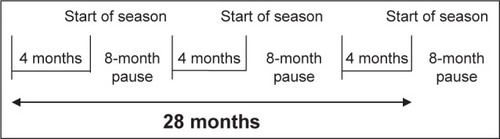
Pre-coseasonal modes started before each season and continued throughout the season but paused after the season. Treatment began again shortly before the next season. A complete treatment cycle (including pauses) comprised at least 28 consecutive months.
Perennial modes usually involved one injection every 4–6 weeks, totaling 8–12 injections per year, over a period of at least 36 months with the same constant dosage of allergens.
Perennial–seasonal mode means that the patients were polysensitized; different allergens were given according to their needed scheme, perennially and seasonally. This mode also consisted of at least 36 consecutive months of therapy.
Short-term immunotherapy comprised 4–8 injections before the season and also required a consecutive 36-month cycle.
Adherence data
Adherence was measured retrospectively and indirectly by analyzing patient data with respect to the starting date of therapy and the termination date. The perennial and the perennial–seasonal modes of therapy and the short-term immunotherapy were scheduled to consist of 36 months of treatment in total. The preseasonal and pre-coseasonal modes of therapy were scheduled to comprise at least 28 months of treatment (). Any patient who abandoned therapy before that set amount of time was considered a dropout.
Data management
Statistics were compiled and analyzed using IBM SPSS Statistics for Windows (version 22.0, IBM Corp., Armonk, NY, USA) and Microsoft Excel (Microsoft Corporation, Redmond, Washington, DC, USA). Quantitative parameters were expressed as means and in percentages with respect to the entire population. Any statistical conspicuity was validated with a Mann–Whitney U test or Fisher’s exact test to determine statistical significance, which was defined as P<0.05.
All patients had formerly consented to the treatment. A written informed consent for the study was not necessary because it was a retrospective anonymous analysis. Retrospect use of data by the treating physician for scientific purposes is allowed and desired. We did, however, consult the official ethics committee of the University of Cologne, which confirmed that the data came from the coauthor Kasche and may be used anonymously by her and our research institute. According to German law, there is no need for a consultation of the ethics committee.
Results
Patients’ demographic characteristics
The observed population of 330 patients consisted of 207 SCIT and 123 SLIT patients. shows the demographic and therapy-related characteristics of the population studied. An analysis of the patient data revealed a significant difference in age between SCIT and SLIT patients in the whole collective (P=0.01). SLIT patients were younger than SCIT patients. All other demographic characteristics showed no significant differences ().
Table 2 Demographic and therapy-related characteristics of the SLIT and SCIT patients studied
Dropouts
In total, 115 (34.8%) patients dropped out of AIT before completing their respective 3-year therapy cycle. The patients who terminated therapy prematurely were significantly younger than the entire group of patients evaluated (P<0.001). The average age of nonadherent patients was 38.6 years, whereas adherent patients had an average age of 44.5 years. The analysis of dropouts by sex and age showed no significant differences. The difference between men and women who terminated therapy prematurely was not statistically significant. Similarly, the difference between male and female dropouts within the SLIT or SCIT groups was not significant. The dropout numbers according to allergen extract are pictured in .
Table 3 Dropouts by allergen extract
Survival rate
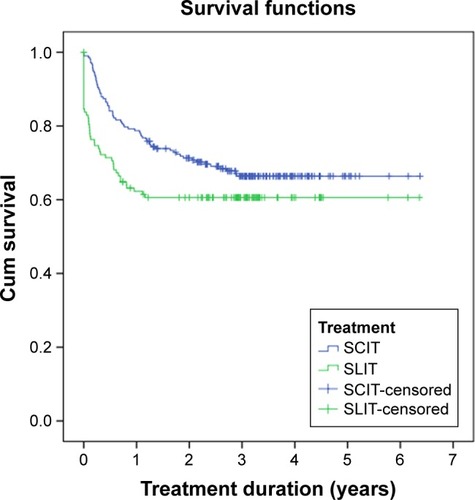
A Kaplan–Meier survival curve resulted in similar trends for both routes of therapy. shows that most patients who dropped out did so during the first year of therapy. Those patients who continued with the second year of therapy were more likely to accomplish the full 3 years of treatment. SCIT patients in this practice generally tended to be more adherent to their therapy than SLIT patients were to theirs.
Figure 2 Kaplan–Meier curve of SCIT and SLIT patients illustrating dropout from therapy over time.
Patients’ reasons for dropping out
The data on patients’ motives for dropping out of therapy were based on the physician–patient consultation and the corresponding physician’s records that were entered into the data management system. Only 32 (27.8%) of the 115 patients who dropped out were willing to state their reasons for doing so in a physician–patient conversation. The following reasons were documented: 10 patients (31%) stated move or travel, 7 (22%) noncompliance, 6 patients (19%) reported adverse effects, 4 patients (13%) stated pregnancy or the desire to have a child, 3 (9%) blamed long waiting hours at the practice, and 2 patients (6%) changed the route of therapy from SCIT to SLIT.
Reported adverse reactions
A retrospective analysis showed that 1.8% of the population (6 of 330) experienced an anaphylactic reaction. All 6 cases of anaphylaxis occurred in patients treated with SCIT. Two patients were treated with Clustoid® grass pollen SCIT, 1 with ALK-Scherax mite mix, 1 with ALK-Scherax early flowering tree mix, 1 with Allergovit® birch/alder/hazel mix, and 1 with ALK wasp. All of the adverse events were grade 1 or 2 reactions retrospectively rated according to the World Allergy Organization SCIT Systemic Reaction Grading system.Citation16 No case required an epinephrine injection.
In all, 58 patients (m=24, f=34) reported negative side effects (ie, mild swelling, redness, and temporary dizziness); 48 of these patients (23.2%) were treated with SCIT.
Discussion
The range of adherence to SLIT and SCIT in the literature
Our results suggest that adherence to SLIT is not as good as adherence to SCIT; however, a significant difference could not be verified. To evaluate our outcome, we searched the literature for similar observations. Four other studies have previously analyzed adherence to AIT with respect to a full 3-year therapy cycle. All of these studies were retrospective and aimed to compare the two AIT routes: SCIT and SLIT.Citation6–Citation8,Citation17 The dropout rate for SLIT patients ranged from 41% to 93% versus 40% to 77% for SCIT patients.
provides an overview of studies comparing SLIT and SCIT adherence with respect to the studies’ definitions of dropouts, sources of data, sample sizes, and dropout rates.
Table 4 Overview of studies comparing SLIT and SCIT adherence
The retrospective study from the Netherlands shows a high number of dropouts during the first year of therapy; in the second and third years, those numbers increased slowly and gradually. The observations of the time-dependent course of dropouts correlate with ours. The overall compliance rate for completing AIT was 18%. The compliance rate of 23% in SCIT patients was better than that in SLIT patients (7%). The median duration of therapy was 1.7 years in SCIT patients and 0.6 years in SLIT patients.Citation7 The Netherlands’ health care system is different than Germany’s, which may generally prevent the comparability of study results from these countries. In the Netherlands, often the patient’s first contact with immunotherapy is through a specialist, but due to scarcity of specialists, most patients are referred back to their general practitioner. That circumstance may influence and explain the high dropout rate in the first year. In conclusion, especially regarding the health care delivery factors to adherence, the data from this particular Dutch study have to be interpreted carefully.
A recent German study that examined the sales data from one manufacturer for 5 consecutive years confirms our results, indicating that adherence to SCIT is better than adherence to SLIT. SLIT patients showed a particularly poor adherence rate of 16% in total. It is worth particular mention that the investigated population of 85,241 SCIT patients and 706 SLIT patients was very large. Children and adolescents were found to be more compliant than adults.Citation8 Because the data were provided by only one manufacturer, the results from that study are hardly comparable to those from other studies.
Our retrospective analysis, however, did in fact uncover a significant difference between the age groups of patients who dropped out of therapy. Also, our analysis showed that the reasons stated for dropping out were mainly patient-related and not due to a lack of communication or information. A study published in 2012 also aimed to determine the reasons why patients discontinue AIT. The motives for discontinuing AIT differed between the treatment groups: SCIT patients most often stated inconvenience as the reason, whereas SLIT patients doubted the efficacy of this treatment. Overall, 45% of SCIT patients and 41% of SLIT patients did not fulfill the treatment requirement of 3 years, resulting in no significant difference in adherence. Concerning the duration of therapy, too, no significant difference between the groups could be recognized.Citation17 The health care setting in this study was similar to that of our study; likewise, the results of dropout rates were also similar.
One aspect of our results concurs with one of the observations Sieber et al made when they examined the medication persistence for AIT in 1,409 patients. Our common observations showed that younger patients tended to drop out of therapy before completing the 3-year treatment cycle. The study by Sieber et al evaluated prescription renewal and followed SCIT and SLIT patients for 3 consecutive years. The patients were grouped according to whether they had received natural extract SLIT, natural extract SCIT, or allergoid SCIT. There was no significant difference in adherence between the two SCIT groups (dropout rate of 66% in the SCIT extract group and 62% in the SCIT allergoid group); however, the SLIT patients were more adherent to treatment, having a lower dropout rate of 49%. Female patients and middle-aged patients were more likely to terminate treatment prematurely.Citation6
Leader et al have just published a retrospective review comparing the compliance to SLIT and to SCIT at one setting. They observed a significantly better compliance to SCIT (85%) than to SLIT (66%). One must consider that their results were obtained using a specific definition of compliance based on a rating scale of compliance from poor, fair, good to excellent. That circumstance makes it rather difficult to compare their results to those of the studies depicted in .Citation18
Due to different data sources, allergen extracts, populations, and different health care systems, an immediate comparison between our results and the aforementioned studies that targeted the same study goal is not reliable. It should be pointed out, however, that results obtained when comparing adherence continue to diverge widely.
SLIT and SCIT compounds are also not comparable due to their distinct and individual compositions. Moreover, the different methods used by manufacturers to measure the concentration of allergens preclude a comparison of the compounds at all.Citation15
Reasoning nonadherence to AIT
The study presented here offers clear evidence that the first year of therapy is a crucial turning point for patient adherence. It appears that once patients manage to be adherent in the first year, they are more likely to complete the rest of their respective AIT.
Only few patients were willing to explain to the physician why they had stopped therapy. Overall, 66% of the reasons for terminating therapy prematurely were based on patient-related factors. For example, 31% of dropouts did not finish their therapy because they had moved away from that practice. However, we cannot actually be sure that they did not continue therapy at another practice. Nonadherence was the cause of therapy discontinuation for 22% of dropouts. Also, 13% of dropouts who terminated therapy were women wishing to become pregnant. One must also consider this study’s setting in the German health care system, in which patients receive 100% reimbursement for allergy treatment expenses. This situation completely excludes costs as a factor influencing adherence.
So far, no studies have proposed an explanation as to why patients adhere more poorly to SLIT than to SCIT. One starting point for an explanation, however, could be the lack of standardized SLIT dosages. Pfaar et alCitation19 have just reported in a dose-finding study that the most efficient SLIT dose has not yet been established for birch tree pollen. They found that the higher the dosage of birch allergens, the better the symptom scores and improvement. The differences were statistically significant. This study outcome raises questions about the efficacy of SLIT itself.Citation19 Hence, nonperception of efficacy is strongly supported as a reason for nonadherence with this outcome. The lack of SLIT dosage recommendations has also been outlined by Leatherman et alCitation20 and its meaning cannot be neglected in reasoning nonadherence.
To improve patients’ long-term adherence, all dimensions of management strategies need to be taken into consideration and enhanced. The health care team in particular can strive toward agreement with the patient on a treatment strategy that puts the patient’s needs first. Fostering a solid, supportive physician–patient relationship may thus prevent patient-related factors for nonadherence. Antico stated that patient-related factors for nonadherence can be prevented with interventions in the physician–patient relationship. The first intervention he describes is to explain the allergy itself to the patient and then to explain the therapy itself to improve the patient’s knowledge and awareness.Citation13 A few studies have already identified the importance of suitable patient information. Interestingly, a German study emphasized that even when patients said they felt well informed, less than half of them could answer 5 questions about their therapy correctly.Citation21 The importance of being well-informed and its consequences for adherence were clearly demonstrated in a recent study that conducted an online patient survey in five countries (USA, France, Spain, Germany, and Russia) with 261 patients who had been treated with AIT. The outcome was alarming: 28% of all patients did not know which allergen was being administered to them during AIT. Another 27% claimed not knowing that allergies were chronic conditions. Patients who dropped out indicated that their reasons for therapy discontinuation were high costs and a lack of perceived efficacy (39%). This study shows quite bluntly that a lack of education in AIT patients impedes therapy success.Citation22 Bender and OppenheimerCitation5 recommend the adaptation of successful management tools used in other chronic diseases, such as effective communication, follow-up, and adequate information. AnticoCitation13 concentrates on management strategies which focus on provider-, health system-, and patient-related impact factors.
Conclusion
In conclusion, our investigation revealed a clear peak of dropouts in the first year of AIT. No significant difference was detected between the dropout rates based on the sex of the patients. Also, dropouts could not be allocated to a certain mode of therapy. However, patients who dropped out tended to be younger than the patients in the entire collective. A trusting physician–patient relationship seems to be a crucial component of good adherence to AIT. Our results strengthen this hypothesis. The adherence rates in this individual practice were remarkably better than those reported in other studies, which can be linked to the practice itself, health care delivery, and the practice’s emphasis on a positive physician–patient relationship. This study’s outcome, however, is limited by its single-center design.
This study provides clear evidence that the first year of therapy is pivotal for patient adherence to AIT. It appears that if patients adhere to their AIT schedule in the first year, they are more likely to complete the rest of their treatment. Our results can, therefore, be interpreted as support for the importance of patient education and for emphasizing the importance of close physician–patient communication during the first year of treatment as decisive factors contributing to the success of AIT.
Acknowledgments
We thank Gena Kittel for her valuable assistance in editing this manuscript and Dr Neuner for his statistical support.
Disclosure
The authors report no conflicts of interest in this work.
References
- LeeSNolteHBenningerMSClinical considerations in the use of sublingual immunotherapy for allergic rhinitisAm J Rhinol Allergy201529210611425785750
- AboshadyOAElghanamKMSublingual immunotherapy in allergic rhinitis: efficacy, safety, adherence and guidelinesClin Exp Otorhinolaryngol20147424124925436040
- CanonicaGWBousquetJCasaleTSub-lingual immunotherapy: World Allergy Organization Position Paper 2009World Allergy Organ J200921123328123268425
- CanonicaGWCoxLPawankarRSublingual immunotherapy: World Allergy Organization position paper 2013 updateWorld Allergy Organ J201471624679069
- BenderBGOppenheimerJThe special challenge of nonadherence with SLITJ Allergy Clin Immunol Pract20142215215524607041
- SieberJDe GeestSShah-HosseiniKMösgesRMedication persistence with long-term, specific grass-pollen immunotherapy measured by prescription renewalsCurr Med Res Opin201127485586121323505
- KielMARöderEGerth van WijkRAlMJHopWCRutten-van MölkenMPReal-life compliance and persistence among users of subcutaneous and sublingual allergen immunotherapyJ Allergy Clin Immunol2013132235336023651609
- Egert-SchmidtAKolbeJMMusslerSThum-OltmerSPatients’ compliance with different administration routes for allergen immunotherapy in GermanyPatient Prefer Adherence201481475148125368517
- ScuratiSFratiFPassalacquaGPuccinelliPHilaireCIncorvaiaCItalian Study Group on SLIT ComplianceAdherence issues related to sublingual immunotherapy as perceived by allergistsPatient Prefer Adherence2010414114520622914
- SaviEPeveriSSennaGPassalacquaGCauses of SLIT discontinuation and strategies to improve the adherence: a pragmatic approachAllergy20136891193119523915164
- SennaGRidoloECalderonMLombardiCCanonicaGWPassalacquaGEvidence of adherence to allergen-specific immunotherapyCurr Opin Allergy Clin Immunol20099654454819823080
- PassalacquaGBaiardiniISennaGCanonicaGWAdherence to pharmacological treatment and specific immunotherapy in allergic rhinitisClin Exp Allergy2013431222823278877
- AnticoALong-term adherence to sublingual therapy: literature review and suggestions for management strategies based on patients’ needs and preferencesClin Exp Allergy201444111314132624975231
- PEI.de [homepage on the Internet]Langen: Allergene zur sublingualen Immuntherapie, Paul-Ehrlich-Institut, Bundesinstitut für Impfstoffe und biomedizinische Arzneimittel, [updated 2016 September 12; cited 2013 December 12] Available from: http://www.pei.de/DE/arzneimit-tel/allergene/therapie-allergene/sublingual/sublinguale-therapie-node.html or http://www.pei.de/EN/medicinal-products/allergens/therapy-allergens/sublingual/sublingual-therapy-node.htmlAccessed July, 2016
- PfaarOBachertCBufeAGuideline on allergen-specific immunotherapy in IgE-mediated allergic diseases – S2k Guideline of the German Society for Allergology and Clinical Immunology (DGAKI), the Society for Pediatric Allergy and Environmental Medicine (GPA), the Medical Association of German Allergologists (AeDA), the Austrian Society for Allergy and Immunology (ÖGAI), the Swiss Society for Allergy and Immunology (SGAI), the German Society of Dermatology (DDG), the German Society of Oto-Rhino-Laryngology, Head and Neck Surgery (DGHNO-KHC), the German Society of Pediatrics and Adolescent Medicine (DGKJ), the Society for Pediatric Pneumology (GPP), the German Respiratory Society (DGP), the German Association of ENT Surgeons (BV-HNO), the Professional Federation of Paediatricians and Youth Doctors (BVKJ), the Federal Association of Pulmonologists (BDP) and the German Dermatologists Association (BVDD)Allergo J Int201423828231926120539
- CoxLLarenas-LinnemannDLockeyRFPassalacquaGSpeaking the same language: the World Allergy Organization subcutaneous immunotherapy systemic reaction grading systemJ Allergy Clin Immunol2010125356957420144472
- HsuNMReisacherWRA comparison of attrition rates in patients undergoing sublingual immunotherapy vs subcutaneous immunotherapyInt Forum Allergy Rhinol20122428028422434716
- LeaderBARotellaMStillmanLDelGaudioJMPatelZMWiseSKImmunotherapy compliance: comparison of subcutaneous versus sublingual immunotherapyInt Forum Allergy Rhinol20166546046426718480
- PfaarOvan TwuijverEBootJDA randomized DBPC trial to determine the optimal effective and safe dose of a SLIT-birch pollen extract for the treatment of allergic rhinitis: results of a phase II studyAllergy20167119910726417901
- LeathermanBDKhalidALeeSDosing of sublingual immunotherapy for allergic rhinitis: evidence-based review with recommendationsInt Forum Allergy Rhinol20155977378326097218
- SondermannNShah-HosseiniKHenkelKSchwalfenbergAMösgesRErfolgsfaktoren der Adherence bei Hyposensibilisierung [Success factors of adherence in hyposensitization]Allergologie2011349441446 German
- CalderonMCoxLCasaleTThe effect of a new communication template on anticipated willingness to initiate or resume allergen immunotherapy: an internet-based patient surveyAllergy Asthma Clin Immunol20151111726015786