
Abstract
Background
Overuse with antibiotics in the treatment of infectious diseases has become a central focus of public health over the years. The aim of this study was to provide an up-to-date evaluation of the blood test-guided antibiotic use on patients with acute diarrhea in primary hospitals of China.
Materials and methods
A cross-sectional survey was conducted on 330 patients with acute diarrhea in Shanghai, People’s Republic of China, from March 2013 to February 2016. These patients were treated with or without antibiotics based on the results of their blood tests, including examinations of C-reactive protein (CRP), white blood cells (WBC), and the percentage of neutrophils (Neu%). The infection types, which included bacterial, viral, and combination diarrhea, were determined by microbiological culture methods. Antibiotics used in non-bacterial diarrhea patients were considered misused and overused.
Results
There were significant overall differences in the clinical characteristics and blood tests between patients with diarrhea with a bacterial infection and patients with other types of infections. The patients were divided into four grading groups (0–3) according to the number of the positive results from three blood testes (CRP, WBC, and Neu%). The misuse rates of antibiotics in each group (0–3) were 81.3%, 71.1%, 72.4%, and 64.9%, respectively.
Conclusion
In this prospective study, the current diagnostic criteria (CRP, WBC, and Neu%) based on blood tests are not reliable in diagnosing bacterial diarrhea or guiding antibiotics use. To limit antibiotic overuse, a rapid and accurate differentiation of bacterial diarrhea from other types of diarrhea is pivotal.
Introduction
Acute diarrhea is defined as the presence of three or more abnormally loose or watery stools over a period of 24 h. The most common cause of acute diarrhea is infective microorganism, such as viruses, bacteria, fungi, or parasites.Citation1 Routine fecal cultures primarily for invasive bacterial pathogens are the major methods used to distinguish bacterial and viral infections in acute diarrhea diagnosis.Citation2 The well-known weaknesses of the stool culture method are that they are quite time-consuming, costly, and have low sensitivity. Moreover, trained technicians and appropriate equipment are required.Citation3 Therefore, in the primary hospitals in People’s Republic of China, the most common tests used for the quick diagnosis and treatment guide of acute diarrhea are blood examinations.Citation4,Citation5 The widely used diagnostic criteria include the number of white blood cells (WBC), the percentage of neutrophils (Neu%), and C-reactive protein (CRP).Citation6 Normally, the treatments will be selected directly depending on the results from these blood examinations.Citation7
The principal components of the acute diarrhea treatments include fluid and electrolyte replacement, dietary modifications, and antibiotics therapy. Like the other infectious diseases, the irrational use of antibiotics for acute diarrhea treatment has become an outstanding problem all over the world, especially in low- and middle-income countries.Citation8 In People’s Republic of China, for economical and historical reasons, antibiotics have been frequently overprescribed in clinical practice for patients with acute diarrhea.Citation9,Citation10 Actually, the extreme overuse of antibiotics is a very serious and longstanding health issue in People’s Republic of China.Citation11 More than 20 years ago, 88.9% of patients with acute diarrhea were prescribed antibiotics, with only 30.1% having clinically diagnosed bacillary dysentery.Citation10 The government has adopted approaches of both education and policy regulation to reduce the overuse of antibiotics.Citation12,Citation13 Five years ago, antibiotics use in People’s Republic of China was under control but still much higher than recommended.Citation14,Citation15
We aimed to study and update our knowledge about the blood examination-guided antibiotic use in emergency care of patients with acute diarrhea from the primary hospitals of People’s Republic of China. Over 300 patients were divided into four groups based on their blood test results. We measured the antibiotic consumption and the misuse rate based on the stool culture examinations. Profound antibiotic overuse was discovered in patients with acute diarrhea, especially for patients who have tested negative in at least one blood examination.
Materials and methods
Study population
This study was carried out in 330 patients (317 adults who were defined as $14 years of age and 13 children) with acute diarrhea at Gongli Hospital and Jinyang Community Health Service Center, Pudong New Area, Shanghai, People’s Republic of China, from March 2013 to February 2016. In this study, there was no immunosuppressed patients, no patients with sepsis or mortality associated with diarrhea and no population needed hospitalization. In this survey, acute diarrhea refers to acute infectious diarrhea. The symptoms lasted 2–24 h before first medical contact. Patients were considered to have acute diarrhea if they were passing at least three loose or watery stools in 24 h or passing at least one bloody stool (macroscopic observation revealed blood mixed with feces or inseparable from the stool), and with an illness duration of no longer than 14 days.
Data collection
An anonymous, paper-based, descriptive questionnaire was used for collecting data. The questionnaire required physicians to report the basic and clinical characteristics of patients (age, gender, etc.), as well as any tests and medications that they had ordered. All the patients with acute diarrhea during the study period, and who agreed to participate in the survey, were included. Four infectious disease specialists were participating in the study. They have been working with other hospital physicians to help direct care for infectious disease for 4–15 years.
Blood tests
Blood samples for three tests (WBC count, Neu%, and CRP) were obtained on admission. WBC and differential counts were measured via the Hematology Analyzer (XS-1000, Sysmex, Kobe, Japan). WBC counts above 10×109/L represent above normal (positive). The Neu% was considered positive when >75%. The CRP level was obtained by a Latex agglutination slide test (Humatex, Wiesbaden, Germany). CRP level above 10 mg/L was considered as elevated (positive) in our laboratory.
Microbiological culture
Fecal samples were selected in the study by the routine enteric laboratory at the hospital. All samples included were diarrheal (adopting the shape of the container), had been stored at 4°C <48 h, and had sufficient fecal material to allow testing with all the assays. For the stool microbiological culture, a drop of a stool sample was resuspended in selective media for Yersinia (Sigma, St. Louis, MO, USA) and then inoculated on a Karmali agar plate (Oxoid, Basingstoke, Hampshire, UK) and incubated at 37°C in a microaerobic atmosphere. Colonies were observed daily until the third day after culture. The suspected colonies were confirmed based on motility, Gram staining, and oxidase activity. The bacterial species were identified by polymerase chain reaction (PCR) using species-specific PCR primers ( and ).Citation16,Citation17 Cultures were considered negative if no bacterial or other pathogen growth was visible after 3 days of incubation. For detection of diarrhea virus, 200 μL of supernatant was taken and used MagNA Pure LC Total Nucleic Acid isolation Kit to extract RNA by the Roche MagNA Pure LC2.0 system, and the total RNA was kept in −8°C for storage. PCR methods were used to detect the target through One-Step real-time polymerase chain reaction kit (Qiagen, Hilden, Germany). The reaction condition is listed in .
Ethics
This study was approved by the ethics committee at Gongli Hospital and Jinyang Community Health Service Center, Pudong New Area, Shanghai, People’s Republic of China. Verbal informed consent was obtained from patients whose medical data were included in the study. Participation was voluntary and no financial incentives were given. Personal identifying information was not collected from practitioners or participating patients.
Data analysis
Data were analyzed using Statistical Package for the Social Sciences (SPSS) software (SPSS Inc., version 13.0; SPSS Inc., Chicago, IL, USA). Between-region differences were assessed for categorical variables with the Pearson’s chi-square test. Continuous variables are expressed as mean ± standard deviation (SD) with 95% confidence intervals; differences were considered statistically significant at P<0.05 or <0.01.
Results
Basic characteristics of the patients with diarrhea
All patients were divided into four groups, that is, negative group (no infection), bacteria group (bacterial infection), virus group (viral infection), and combination (bacterial and viral infection). Characteristics of patients in different infection groups were examined and compared as shown in . No difference in gender, age, symptom (vomit and stomachache), or number of times diarrhea was observed in these four groups. There was a significant increase in WBC, Neu%, and number of fever cases in the bacterial group, compared to the negative group and virus group (). Interestingly, the CRP level and the rate of fever symptom in the combination group are much lower than other groups. Together, these data indicate that patients in the bacterial group show significant signs of inflammation, compared with other patients.
Figure 1 Baseline laboratory results for the study cohort.
Abbreviations: CRP, C-reactive protein; Neu%, percentage of neutrophils; WBC, white blood cells.
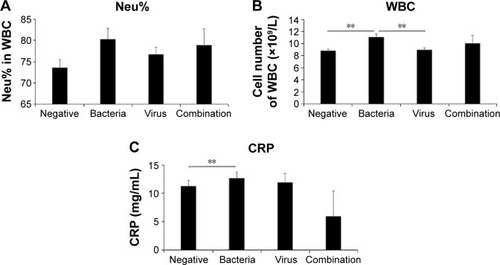
Table 1 Characteristics of patients in different infection groups
Blood tests of CRP, WBC, and Neu% in patients with diarrhea
To evaluate blood test-guided antibiotics use in the patients with diarrhea, the patients were stratified into four grading groups (from 0 to 3) based on the number of positive results (from 0 to 3) in the blood tests (CRP, WBC, and Neu%). As shown in , from grading group 0 to group 3, the percentage of no infection cases decreased from 66.3% to 35.1%, whereas the percentage of bacterial infection cases increased from 17.6% to 32.4%. Notably, the majority of these patients have either no infection or non-bacterial infection, which indicates that most of them are not qualified for antibiotics therapy. For example, even for patients with positive results from all blood tests (group 3), almost two of three of them (35.1% no infection and 29.7% viral infection) should not be treated with antibiotics. These data showed that the blood tests are not an accurate differentiation test for identifying bacterial infection in patients with diarrhea.
Table 2 Blood test results in different infection groups
Antibiotic use in patients with bacterial and non-bacterial diarrhea
To calculate the misuse rate of antibiotics, the negative group and virus group were combined into non-bacterial infection group, and bacterial group and combination group were combined into bacterial infection group in the following study. As shown in , the overall antibiotics use rates, as well as the use rates in each group, were calculated. The antibiotics use rate in non-bacterial infection groups was considered as a misuse of antibiotics. The overall misuse rate of antibiotics is 72.0%, and the misuse rate in individual grading groups (from 0 to 3) decreased from 81.3% to 64.9%. Even in group 3, the ratio of over-treated patients to properly treated patients (ratio of non-bacterial use to bacterial use) is nearly double (1.8). Hence, we concluded that this retrospective study showed a profound misuse of antibiotics in the patients with acute diarrhea, which was directly guided by the results from the blood tests of WBC, Neu%, and CRP.
Table 3 Antibiotic use rate in each infection group
Discussion
In this retrospective cohort study, we observed a profound misuse of antibiotics in patients with acute diarrhea who were treated based on blood testing (CRP, WBC, and Neu%). Although the results of the blood tests displayed a significant difference between patients with bacterial diarrhea and other groups of patients, these tests failed to prove their accuracy in differentiating between bacterial diarrhea and non- bacterial diarrhea.
As a common symptom faced by emergency doctors in People’s Republic of China, acute diarrhea and the intestinal secretory processes can be activated by infection from bacteria, viruses, or other pathogens. It was reported that the most common enteral infectious agents in People’s Republic of China from 2010 to 2015 include 7 bacteria, 5 viruses, and 3 protozoa. Diarrheagenic Escherichia coli was identified as the most predominant pathogen in diarrhea cases.Citation18,Citation19 In our study, the most frequent causes of infectious diarrhea were virus (Vibrio) and bacteria (Salmonella). In consistent with our findings, it seems that the epidemiology change during the several past years is virus becoming a more frequent cause than bacteria in Chinese as reported by citywide hospitals in big cities. For different infections, there were different treatments and the doctors in the primary hospitals and institutes determine the chance of bacterial infection using three criteria: elevated Neu%, WBC count, and CRP level. Doctors are more likely to prescribe antibiotics if more of these criteria are met as they are directly related to bacterial infection. However, in our current findings, these indicators showed low accuracy in identifying bacterial infectious diarrhea.
The Neu% and WBC count are two criteria used to diagnose bacterial infection. Neutrophils are responsible for the most rapid immune response and are the immune system’s first line of defense.Citation20 Upon bacterial infection, pathogen-associated molecular patterns of the bacteria, such as lipopolysaccharides and poly (I:C), may directly stimulate the infected tissue or local immune cells through toll-like receptors.Citation21 This strong inflammatory stimulation would directly induce the production of cytokines and chemokines, among them are several CXC chemokines.Citation22–Citation24 These two criteria seem to be specific for bacterial infection. However, recent discoveries showed that viral infection can also induce elevated peripheral neutrophil count and percentage through similar mobilization mechanisms. The neutrophils are also recruited to the virus-infected tissue.Citation25–Citation27 Thus, analyzing the neutrophil percentage and WBC count cannot clearly distinguish bacterial infection from viral infection. Moreover, the elevated WBC count is dependent on neutrophil mobilization. This makes these two criteria interdependent and should not be evaluated as two separated criteria.
Another criterion the Chinese clinical practitioners use to diagnose bacterial infection is the elevation of CRP. CRP is a typical acute-phase protein. CRP can directly bind to and opsonize bacteria. It also orchestrates the immune response.Citation28 Importantly, many studies showed that extremely high CRP is related to acute bacterial infection but not viral infection. This makes it a good candidate for a criterion that can distinguish between bacterial and viral infection.Citation29–Citation31 However, in our study, we did not find an extremely high average CRP concentration in the bacterial diarrhea infections (). This disappointing discovery may be due to the dynamic pattern of CRP expression. As we know, CRP was the acute-phase protein. Plasma CRP is produced by hepatocytes and study showed that in healthy adults the median concentration of CRP was 0.8 mg/L and the 99th centile is 10 mg/L and after an acute-phase stimulus, CRP values may increase to 10,000-fold.Citation32 We noticed that in acute bacterial diarrhea, drastically elevated CRP concentration can only be found within 20 h after the infection (data not shown), while in our clinical practice the blood testing is often conducted outside of this timeframe. This may explain that why CRP elevation may not be found in most of patients with bacterial diarrhea. Due to this fact, a moderate CRP concentration is an unreliable criterion for differentiating between viral diarrhea and bacterial diarrhea. Another cause that leads to misdiagnose is when the patients have both bacterial and viral infections, and the CRP level and other physical symptom are much lower, instead of higher, as we observed in this study. Actually, in most of the combined infection patients, the viral and bacterial infections usually occur simultaneously,Citation33 which make the typical features of the bacterial infection disappear.
In brief, the imprecise nature of these diagnostic criteria may have led to many misdiagnoses of bacterial diarrhea. This is reflected in our data, which shows that an extremely high percentage of antibiotics overuse occurred because the doctors relied solely on these tests. This is not the only contributing factor to antibiotics overuse, however.
Previous studies showed that Chinese health literacy has been low and antibiotics have been considered a stronger, faster, and higher quality medicine for treatment.Citation34 Pressure from patients and the financial concerns are two of major causes that conspire to encourage the dangerous overuse of antibiotics.Citation8 The antimicrobial resistance of antibiotics is commonly increasing in People’s Republic of China, whereas the rate varies on different infections. For instance, studies indicated that the antimicrobial resistance of levofloxacin is 53.4% in Shigella infections.Citation35 In the Campylobacter jejuni infection, the resistance to cefuroxime was increased to 93% in 2010 while it was 0% in the 1990s.Citation36 Actually, the preventive usage of antibiotics is beneficial in immunocompromised patients,Citation37,Citation38 which only counts for a small amount of patients with infectious diseases. For instance, only ~5%–8% of acute salmonellosis is in general population.Citation39 It is suggested that most patients should be prescribed with antibiotics only after confirmation of bacterial infection. However, confirmation of bacterial infection with culture analysis usually takes days, which is an unrealistic amount of time to wait to provide a treatment. Thus, Chinese medical practitioners utilized an inexact method to prescribe antibiotics, taking into account only the patients’ symptoms and quick lab tests. When information about antibiotics became available to the general public in People’s Republic of China, the elderly and parents of small children with limited health insurance preferred the use of antibiotics treatment because it was an inexpensive option. In addition, monetary incentives also contribute to clinicians prescribing antibiotics excessively. This is especially true of primary care clinicians as monetary incentives from drug prescriptions are a major source of income for them.Citation34
In summary, the higher rate of antibiotic prescription for patients with acute diarrhea by primary care clinicians may be explained by a combination of inaccurate criteria for diagnosis, lack of sufficient training, and stronger economic incentives. Practitioners should be cautious about overprescribing antibiotics and rely on other testing methods for treatment. Medical professionals, as well as government personnel working in the health sector, need to update their diagnostic and treatment guidelines based on the latest scientific evidence. The remedy of this situation requires that educational awareness programs be conducted on a regular basis to educate doctors and patients about the dangers of overuse and abuse of antibiotics.
Overall, we found that using these three blood tests to diagnose bacterial diarrhea and guide antibiotics treatment is not reliable. More accurate and efficient diagnostic criteria for identifying bacterial diarrhea are needed in People’s Republic of China to reduce antibiotic overuse and improve the efficiency of the clinical management of diarrhea.
Acknowledgments
This study was supported by Key Discipline Construction Project of Pudong Health Bureau of Shanghai (No: PWZx2014-03) and Shanghai Municipal Commission of Health and Family Planning Fund (No: 20134396). We thank SinoScript for proofreading this manuscript.
Supplementary materials
Table S1 Primer sequences for bacteria identification
Table S2 Primer sequences for virus identification
Table S3 The polymerase chain reaction condition of diarrhea pathogens
Disclosure
The authors report no conflicts of interest in this work.
References
- FarthingMSalamMALindbergGAcute diarrhea in adults and children: a global perspectiveJ Clin Gastroenterol2013471122023222211
- PawlowskiSWWarrenCAGuerrantRDiagnosis and treatment of acute or persistent diarrheaGastroenterology200913661874188619457416
- GuerrantRLShieldsDSThorsonSMSchorlingJBGroschelDHEvaluation and diagnosis of acute infectious diarrheaAm J Med1985786B91984014291
- WangDFangLXiaoSPorcine epidemic diarrhea in ChinaVirus Res201622671327261169
- ZhuMZhangJGaoYWangZPresent research on disease burden of diarrhea illnessWei Sheng Yan Jiu2008371126128 Chinese18421885
- GonzalezMDWilenCBBurnhamCAMarkers of intestinal inflammation for the diagnosis of infectious gastroenteritisClin Lab Med201535233334426004646
- RadlovicNLekovicZVuleticBRadlovicVSimicDAcute diarrhea in childrenSrp Arh Celok Lek201514311–12755762 Slovak26946776
- LiYChina’s misuse of antibiotics should be curbedBMJ2014348g108324523392
- HouFQWangYLiJWangGQLiuYManagement of acute diarrhea in adults in China: a cross-sectional surveyBMC Public Health2013134123324386
- KeBRanLWuSSurvey of physician diagnostic and treatment practices for patients with acute diarrhea in Guangdong province, ChinaFoodborne Pathog Dis201291475321988400
- MaoWVuHXieZChenWTangSSystematic review on irrational use of medicines in China and VietnamPLoS One2015103e011771025793497
- XiaoYZhangJZhengBZhaoLLiSLiLChanges in Chinese policies to promote the rational use of antibioticsPLoS Med20131011e100155624260030
- ZhangYHarveyKRational antibiotic use in China: lessons learnt through introducing surgeons to Australian guidelinesAustralia New Zealand Health Policy20063516732892
- DongLYanHWangDAntibiotic prescribing patterns in village health clinics across 10 provinces of Western ChinaJ Antimicrob Chemother200862241041518400805
- DongLYanHWangDDrug prescribing indicators in village health clinics across 10 provinces of Western ChinaFam Pract2011281636720876222
- YuXFPanJCMengDMWangHQZhangWZhengWMultiplex real-time PCR detecting Salmonella, Shigella and diarrheagenic Escherichia coliZhonghua yu fang yi xue za zhi2007416461465 Chinese18399125
- WangJXuZNiuPA two-tube multiplex reverse transcription PCR assay for simultaneous detection of viral and bacterial pathogens of infectious diarrheaBiomed Res Int2014201464852024711998
- ZhangSXYangCLGuWPCase-control study of diarrheal disease etiology in individuals over 5 years in southwest ChinaGut Pathog201685827891182
- WeiZQChangHLLiYFXuXBZengMClinical epidemiology and antimicrobial resistance of nontyphoidal Salmonella enteric infections in children: 2012–2014Zhonghua Er Ke Za Zhi2016547489495 Chinese27412737
- KolaczkowskaEKubesPNeutrophil recruitment and function in health and inflammationNat Rev Immunol201313315917523435331
- ZhengJMengJZhaoSSinghRSongWCampylobacter-induced interleukin-8 secretion in polarized human intestinal epithelial cells requires Campylobacter-secreted cytolethal distending toxin- and toll-like receptor-mediated activation of NF-kappaBInfect Immun200876104498450818644884
- AmulicBCazaletCHayesGLMetzlerKDZychlinskyANeutrophil function: from mechanisms to diseaseAnnu Rev Immunol20123045948922224774
- EashKJGreenbaumAMGopalanPKLinkDCCXCR2 and CXCR4 antagonistically regulate neutrophil trafficking from murine bone marrowJ Clin Invest201012072423243120516641
- ChangBXuMJZhouZShort- or long-term high-fat diet feeding plus acute ethanol binge synergistically induce acute liver injury in mice: an important role for CXCL1Hepatology20156241070108526033752
- GalaniIEAndreakosENeutrophils in viral infections: current concepts and caveatsJ Leukoc Biol201598455756426160849
- DrescherBBaiFNeutrophil in viral infections, friend or foe?Virus Res201317111723178588
- JenneCNWongCHZempFJNeutrophils recruited to sites of infection protect from virus challenge by releasing neutrophil extracellular trapsCell Host Microbe201313216918023414757
- ZhouZXuMJGaoBHepatocytes: a key cell type for innate immunityCell Mol Immunol201613330131526685902
- SasakiKFujitaIHamasakiYMiyazakiSDifferentiating between bacterial and viral infection by measuring both C-reactive protein and 2′-5′-oligoadenylate synthetase as inflammatory markersJ Infect Chemother200281768011957124
- HaranJPBeaudoinFLSunerSLuSC-reactive protein as predictor of bacterial infection among patients with an influenza-like illnessAm J Emerg Med201331113714422944552
- KorppiMKrogerLC-reactive protein in viral and bacterial respiratory infection in childrenScand J Infect Dis19932522072138511515
- PepysMBHirschfieldGMC-reactive protein: a critical updateJ Clin Invest2003111121805181212813013
- DuPontHLPersistent diarrhea: a clinical reviewJAMA2016315242712272327357241
- ReynoldsLMcKeeMFactors influencing antibiotic prescribing in China: an exploratory analysisHealth Policy2009901323618849089
- ZhangCLLiuQZWangJChuXShenLMGuoYYEpidemic and virulence characteristic of Shigella spp. with extended-spectrum cephalosporin resistance in Xiaoshan district, Hangzhou, ChinaBMC Infect Dis20141426024886028
- HouFQSunXTWangGQClinical manifestations of Campylobacter jejuni infection in adolescents and adults, and change in antibiotic resistance of the pathogen over the past 16 yearsScand J Infect Dis201244643944322339578
- KuruvillaMde la MorenaMTAntibiotic prophylaxis in primary immune deficiency disordersJ Allergy Clin Immunol Pract20131657358224565703
- MiaoRHuangSZhouZTargeted disruption of MCPIP1/Zc3h12a results in fatal inflammatory diseaseImmunol Cell Biol201391536837623567898
- OnwuezobeIAOshunPOOdigweCCAntimicrobials for treating symptomatic non-typhoidal Salmonella infectionCochrane Database Syst Rev201211CD00116723152205