
Abstract
Purpose
To evaluate the impact of several factors on the patient’s perception on quality of life in a group of patients with type 2 diabetes mellitus (T2DM).
Patients and methods
In this cross-sectional study, 198 patients with T2DM were enrolled according to a consecutive-case population-based study design. In all participants, the perception on the quality of life was measured using the quality of life index – diabetes version III proposed by Ferrans and Powers. We evaluated the impact of several anthropometric and diabetes-related (ie, diabetes history and quality of glycemic control) factors on the patient’s perception on the quality of life.
Results
The presence of diabetes complications was associated with a decreased quality of life: retinopathy (1 vs 5 points; P<0.001), chronic kidney disease (−1 vs 5 points; P<0.001), and neuropathy (−1 vs 5 points; P<0.001). A significant reverse correlation was found between the patient’s quality of life and depression’s severity (Spearman’s r=−0.345; P<0.001) and body mass index (Spearman’s r=−0.158; P=0.026). A positive association between the quality of life and the quality of diabetes-related self-care activities was found (Spearman’s r=0.338; P<0.001). No significant association was found between the patient’s quality of life and the quality of glycemic control, diabetes duration, age, gender, or smoking status.
Conclusion
To improve the patient’s quality of life, special care should be given to the modifiable diabetes-related factors: the prevention and treatment of diabetes complications, treatment of depression, and weight loss in obese and overweight patients.
Introduction
The marked increase in life expectancy has made it obvious that there is a need for other health-related measures other than life expectancy and cause of death, especially regarding the grade of lived years.Citation1 An individual’s existence in all its aspects can be summed up using the concept known as “quality of life” (QoL). Narrowing the specter and referring to the health domain of a person’s existence, the term “health-related quality of life (HRQoL)” is used as a subset, thus differentiating it from other QoL aspects. Since health embodies multidimensional domains such as physical, emotional, mental, and social functioning, they are also taken into account when speaking of HRQoL.Citation2,Citation3 In order to measure the differences in the patient’s QoL at a point in time or during a certain period of time, interviewer or self-administered questionnaires are a useful tool.Citation4
Diabetes mellitus (DM) is a group of metabolic diseases consisting of defects in what the secretion and/or action of insulin is regarded, leading to the main manifestation, hyperglycemia.Citation5 It represents a globally rising health issue, the number of people suffering from this chronic disease last being estimated in 2016 by the World Health Organization at 422 million.Citation6 The estimated number of affected individuals by the year 2030 is expected to double.Citation7
Chronic hyperglycemia as found in diabetes is associated with organ dysfunction, damage or even failure, and diabetes-specific complications.Citation8 Diabetic patients tend to exhibit signs of anxiety and poor emotional health due to negative diabetes perception, loss of control, and fear of complications.Citation9,Citation10 A “response shift”, which is an internal change of values, standards, and concepts regarding QoL must then take place in order for the patient to be able to confront the chronic disease and all that it entails.Citation11
In patients suffering from DM, particularities in QoL perception arise due to the strain of the chronic nature of the disease and to the multitude of complications that can derive from it. Cardiovascular complications such as atherosclerosis, hypertension, and cardiac autonomic neuropathy are also found in diabetes and represent a permanent stressor for the diabetic patient. Chronic kidney disease (CKD) has diabetes as a main cause in its final stages, leading to dialysis. Retinopathy is yet another complication present, one that can lead to visual impairment or even blindness. Diabetic neuropathy (DN) can affect the peripheral nerves, leading to foot ulcerations and even amputations, or autonomic ones, causing gastrointestinal, urinary and sexual dysfunctions. There are studies that confirm the link between depression and DN, even more, the link between the level of depression and the severity of the neuropathy. Depression is shown to appear shortly after the debut of diabetic complications, especially peripheral neuropathy.Citation5,Citation9,Citation10
Several studies, including here randomized clinical trials, described the influence of several factors that had an impact on the QoL in cohorts of patients diagnosed with both type 2 diabetes mellitus (T2DM)Citation12,Citation13 and type 1 diabetes mellitus (T1DM);Citation14 however, there were observed significant differences regarding the importance and impact on QoL of different factors, differences generated mainly by regional, geographical, and cultural differences between the studied cohorts. Emphasized by this fact and considering that the Romanian patients have a set of cultural and social particularities, we considered that studying these factors and their impact on Romanian patients’ QoL is of paramount importance.
Having taken all of the above into consideration, the aim of this study is to evaluate which factors may influence the perception on the QoL in Romanian patients with T2DM.
Patients and methods
Study design and patients
In this cross-sectional, noninterventional study, a cohort of 198 patients with T2DM was enrolled according to a consecutive-case population-based method. All patients were attending scheduled monitoring visits at the outpatient of the Diabetes Clinic from the Emergency Hospital in Timisoara and were previously diagnosed with T2DM. At the time of the screening, the following were considered exclusion criteria: the inability to provide informed consent, inability to provide accurate anamnestic medical history data, prior history of nondiabetic neuropathies, major cardiovascular events 3 months prior to screening, or any other condition that, in the investigators’ opinion, could lead to biases in the study results.
The studied group characteristics were representative of the Romanian T2DM population; the patients enrolled in the study had a median age of 61 years, a median diabetes duration of 7 years, and 55.1% of them (n=109) being females.
The study design, protocol, and informed consent form were reviewed and approved by the Ethics Committee of the Emergency Hospital Timisoara (no 328/2014); all patients provided written informed consent prior to any study procedure or activity.
QoL assessment
The QoL was investigated using the quality of life index – diabetes version III (QoL) proposed by Ferrans and Powers, which is a validated instrument for the diabetic population and which was validated for the Romanian population.Citation15 This instrument measures both satisfaction and importance of various aspects of life: health and functioning, social and economic, and psychological and family relationships. The instrument consists of two major parts: first in which satisfaction in previously mentioned items is measured and the second which measures the importance of these items for the questioned person. A higher score is associated with an increased QoL.Citation15
Diabetes complications and comorbidities assessment
DN was diagnosed using the Michigan Neuropathy Screening Instrument (MNSI). This is a validated score instrument for DN, being widely used for positive diagnosis and severity measurement of neuropathy. It consists of two distinct parts: a 15-item questionnaire that assesses the patient’s signs and symptoms regarding the neuropathy and a lower extremity examination performed by the health care professional in which pathological alterations are scored. The positive diagnosis of neuropathy was established if a questionnaire score higher than 7 or a clinical examination score higher than 2.5 was found. At the same time, a higher MNSI score was associated with a more severe neuropathy.
CKD was diagnosed according to Kidney Disease Improving Global Outcomes 2012 criteria and the diagnosis of retinopathy based on the funduscopic examination results performed by an ophthalmologist specialized in the eye’s diseases of diabetic patients.Citation16 The presence of cardiac autonomic neuropathy was investigated using the measurement of changes in postural blood pressure. A positive diagnosis for postural hypotension was defined by a drop in systolic blood pressure of 20 mmHg or diastolic blood pressure of 10 mmHg within 3 minutes after changing the body position from supine to standing.Citation17
Clinical, anthropometric, and laboratory data
Data on the patient’s age, diabetes duration, and smoking status were collected from the patient’s medical records. The HbA1c level was measured using an NGSP-standardized and DCCT-compliant immune-turbidimetric assay (Roche), having an intermeasurement coefficient of variation of 1.64% according to the manufacturer’s specifications. Body mass index (BMI) was calculated by dividing the patient’s weight (measured in kilograms) to the square of the patient’s height (measured in meters).
Depression and quality of diabetes-related self-care activities
To evaluate the presence and the severity of depression, we used the Patient’s Health Questionnaire-9 (PHQ-9). With its 9 items, the PHQ-9 test consists of the actual 9 criteria on which the diagnosis of DSM-IV depressive disorders is based. The PHO-9 is a dual-purpose instrument that can establish, with the same 9 items, depressive distress and grade depressive symptom severity. A higher PHQ-9 score is associated with more severe depression.Citation18
The quality of diabetes-related self-care activities was evaluated using the Summary of Diabetes-related Self-Care Activities questionnaire (SDSCA), which is a validated tool in the population of DM patients. A higher SDSCA score is associated with a better disease self-care in these patients. The SDSCA questionnaire includes items assessing the following aspects of diabetes care: general and specific diet measures, exercise, blood-glucose testing, foot care, and smoking.Citation19
Statistical analysis
Data were collected and analyzed using the Statistical Package for the Social Sciences (SPSS) v. 17 software suite (SPSS Inc., Chicago, IL, USA) and are presented as medians and interquartile range for continuous variables without Gaussian distribution, average ± standard deviation for continuous variables with Gaussian distribution or number of individuals and percentage from the subgroup total in case of nominal variables. The normality of the variable’s distribution was tested prior to analysis according to the following methods: Kolmogorov and Smirnov normality test used in parallel with Shapiro–Wilk and normality plot analysis (at these tests a P-value <0.05 was considered to be associated with a non-Gaussian values distribution).
To assess the significance of the differences between groups, Mann–Whitney U, Kruskal–Wallis (medians, non-Gaussian populations), and chi-square (percentages) tests were used. The correlation between studied variables was evaluated using Spearman’s rank sum correlation coefficient (non-Gaussian distributed variables), its statistical significance being assessed using the t-distribution score test.
The individual impact of several confounding factors on the variance of a continuous variable was assessed by building multivariate regression models. The predictors, in the final regression equations, were accepted according to a repeated backward-stepwise algorithm (inclusion criteria P<0.05 and exclusion criteria P>0.20) in order to obtain the most appropriate theoretical model to fit the collected data. The quality of the model was described using the accuracy of the prediction by adjusted R2 (multivariate linear regression). In this study, a P-value of <0.05 was considered as the threshold for statistical significance.
Results
Demographic, social, psychological, and anthropometric factors
In our study group, the perception on the QoL was associated with neither the patient’s age (Spearman’s r=0.016; P=0.820) nor the duration of DM (Spearman’s r=−0.004; P=0.957). There were no differences regarding the QoL’s perception with respect to gender (P=0.343), smoking status (P=0.595), or dangerous alcohol consumption habits, as evaluated with the AUDIT-C questionnaire (P=0.775).
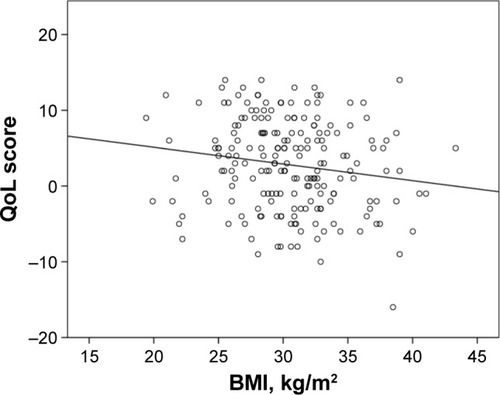
Our results are pointing to a significant negative correlation between the patients’ BMI and their perception on the QoL (Spearman’s r=−0.158; P=0.026), indicating thus that patients with a higher BMI tend to have a decreased QoL ().
Figure 1 The correlation between the BMI and the patient’s QoL.
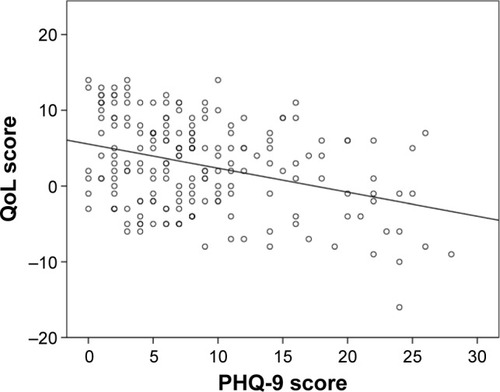
At the same time, the presence and severity of depression, assessed using the PHQ-9 score, was reverse and significantly correlated with the QoL (Spearman’s r=−0.345; P<0.001), denoting that patients with more severe depression symptomatology are having a decreased QoL ().
Figure 2 The association between depression and perception on the QOL.
The details regarding the impact of the demographic, social, psychological, and anthropometric factors on the patient’s QoL are summarized in .
Table 1 Association between demographic, social, psychological, and anthropometric factors and patient’s QoL
Diabetes-related factors influencing the QoL
Glycemic control and patient’s adherence to treatment
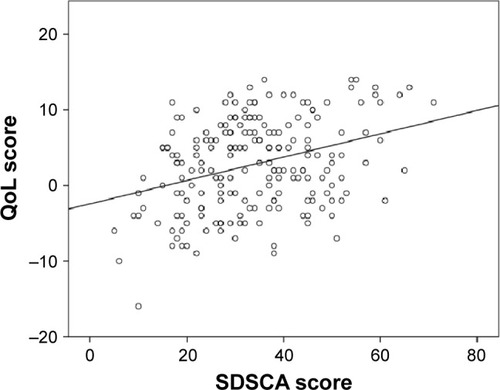
The QoL was not significantly correlated with the quality of the glycemic control measured using the HbA1c value (Spearman’s r=−0.114; P=0.110); in contrast, it was positively and significantly correlated with the patient’s adherence to diabetes-related self-care activities (Spearman’s r=0.338; P<0.001; ).
Figure 3 The correlation between the quality of diabetes-related self-care activities and patient’s QoL.
Diabetes complications and comorbidities
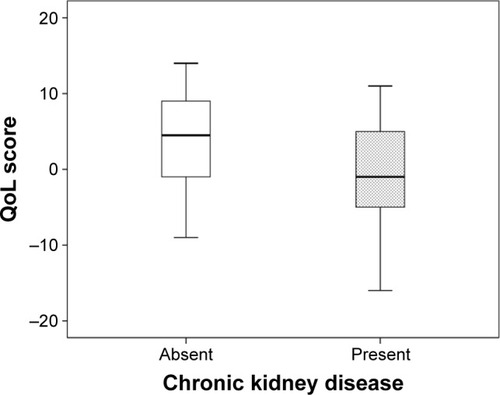
The study results are pointing to a decreased QoL in patients having diabetes complications. This decrease was observed for patients with neuropathy (−1 vs 5 points, P<0.001), CKD (−1 vs 4 points, P<0.001, ), retinopathy (1 vs 5 points, P<0.001), and cardiac autonomic neuropathy (−1 vs 4 points, P=0.001).
Figure 4 Comparison of QoL in patients with vs without neuropathy.
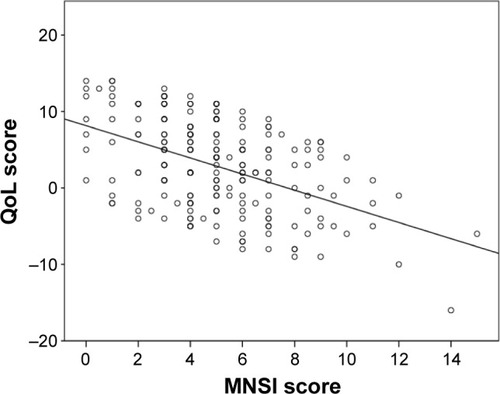
Moreover, the severity of neuropathy, assessed using the MNSI score was reversed and significantly correlated with the patient’s QoL (Spearman’s r=−0.483, P<0.001, ).
Figure 5 Correlation between the neuropathy’s severity and patient’s QoL.
The presence of hypertension as a comorbidity of diabetes seemed to not influence significantly the patient’s QoL.
An analysis of diabetes complications and comorbidities impact on the patient’s perception regarding the QoL is presented in .
Table 2 Diabetes complications and comorbidities impact on patient’s QoL
Multivariate regression analysis
Since the QoL in patients with DM may be influenced by multiple factors, factors between which and independent relation may exist, we aimed to evaluate which factors are possible independent predictors and which are only cofactors in influencing the perception on the QoL in this cohort of patients. To evaluate the independent impact for each evaluated factor we built, with the collected parameters, a multivariate regression model having as outcome variable the value of QoL. To obtain the best fit model, the initial collected parameters (patient’s age, diabetes duration, gender, HbA1c, MNSI score, smoking status, alcohol consumption, BMI, PHQ-9 score, SDSCA score, and the presence of complications and comorbidities: CKD, retinopathy, and hypertension) were added in the regression model according to a backward-stepwise criterion (inclusion criteria: P<0.05, exclusion criteria: P>0.20). On the basis of this inclusion algorithm, the following predictors were accepted in the final model: patient’s age, the value of HbA1c, MNSI score, depression’s severity (PHQ-9 score), the presence of retinopathy, and CKD.
According to our model, an independent significant impact on the patient’s QoL had the severity of neuropathy (MNSI score), the presence of CKD and retinopathy, and the severity of depression. Our results are pointing that for each increase with a standard deviation in the value of the MNSI score, the depression score decreased with 0.356 standard deviations (Exp(β)=−0.356, P<0.001). In parallel, significant independent predictors were the HbA1c value (Exp(β)=−0.103; P=0.010), the presence of CKD (Exp(β)=−0.120; P=0.009), and diabetic retinopathy (Exp(β)=−0.113; P=0.013). The other analyzed predictors had no significant independent impact on the patient’s QoL.
Discussion
The study results show a decreased QoL in patients suffering from diabetic complications, such as neuropathy, CKD, retinopathy, and cardiac autonomic neuropathy. The severity of neuropathy assessed using the MNSI score was reversed and significantly correlated with the patient’s QoL. In the case of diabetic foot ulcer (DFU) presence or history, physical impairment gravely affected QoL,Citation20 to such an extent that mobile amputees had a better psychological status than DFU patients.Citation21 The proliferative diabetic retinopathy diagnosis increases depression and negative life experiences for a period of 2 years after the diagnosis, as proven by several studies.Citation22,Citation23
Another factor that was positively and significantly correlated with QoL was the patient’s adherence to diabetes-related self-care activities, such as proper diet, exercise routine, and glycemic control. These elements play a crucial role in preventing the apparition of complications and in maintaining a healthy BMI, as patients with a higher BMI have been found to have a decreased QoL, underlining the significant negative correlation between the two. It has been found that if two or more diabetes-related complications were present, there was a significantly associated likelihood that patients with diabetes showed clinical symptoms of depression or anxiety.Citation24 Signs of depression and emotional distress should be closely monitored, as they influence self-care behaviors in a negative manner, studies have shown.Citation25,Citation26
When referring to the association between QoL in patients with diabetes and treatment regimen, it was found that the QoL decreases as the treatment regimen advances, being perceived as best when they only had a diet and exercise program, having less diabetes-related worries than patients taking oral medication, whereas those taking insulin reported more burden of illness and less treatment satisfaction than those controlling their glucose levels orally or by diet and exercise alone.Citation27
The strength of this study lies in the fact that it is the only one that addresses the QoL in diabetic patients in Romania. Although such studies exist elsewhere, we must keep in mind the particularities of the Romanian population in what culture, tradition, education, health, and socioeconomic status are regarded. The results of this study are based on a large patient cohort, one that very well comprises the characteristics of the diabetic population in Romania, thus being a very representative pool.
The limitative character of this study is rendered by the transversal manner in which the evaluation of glycemic control was made: altering of QoL in respect to glycemic control might necessitate a longer timespan than 3 months, which is the period comprised by our analyzing of HbA1c.
The number of complications has also been reported as a strong predictor of QoL in a population of diabetic patients by Trief et al,Citation28 while Jacobson et al noted that the greater the severity of complications, the lower scores on all QoL scales,Citation27 these results being in accord with our findings.
The authors’ findings are mixed regarding the relation between the QoL and duration of diabetes. While several studies have found that a decreased QoL was associated with an increased duration of diabetes,Citation29 others as ourselves have found no relevant association between the two. Peyrot and Rubin found no notable association between diabetes duration and depression in those with both T1DM and T2DM,Citation24 nor did a Swedish study on type 2 diabetes patients, whose evaluations were done using scores on Bradley’s well-being or treatment satisfaction questionnaires.Citation30
QoL is an extremely important component in the management of any disease, especially chronic ones such as diabetes. The diabetic patient’s QoL is influenced by a series of factors, such as neuropathy, CKD, retinopathy, cardiac autonomic neuropathy, and BMI. By identifying this series and by managing it, we could improve the QoL of our patients. Improvements in QoL should always be at the center of the patient’s treatment and global management.
Conclusion
In patients with T2DM, the perception on the QoL is significantly influenced by the presence and severity of associated complications (neuropathy, CKD, and retinopathy), by the BMI, and by the presence and severity of depression. Given the modifiable character of these factors, special care should be provided in order to improve QoL in patients with T2DM. Also of great importance are the study’s results that demonstrated that patients with decreased QoL simultaneously present a decrease in what the quality of diabetes-related self-care activities is concerned, thus leading to a decreased overall diabetes prognosis and an increase in the incidence of diabetes-associated complications.
Acknowledgments
This research was supported by an internal grant, funded by “Victor Babes” University of Medicine and Pharmacy, Timisoara, Romania (PLURINEURODIAB. PII-C4-TC- 2016-16441-01).
Disclosure
The authors report no conflicts of interest in this work.
References
- World Health OrganizationThe World Health Organization Quality of Life Assessment (WHOQOL): position paper from the World Health OrganizationSoc Sci Med2005411014031409
- GeorgeWTorrance Utility approach to measuring health-related quality of lifeJ Chronic Dis19874065936033298297
- FerransCEDefinitions and conceptual models of quality of lifeLipscombJGotayCCSnyderCOutcomes Assessment in CancerCambridge, EnglandCambridge University20051430
- GuyattGFeenyDHPatrickDMeasuring health-related quality of lifeAnn Intern Med199311886226298452328
- American Diabetes AssociationDiagnosis and classification of diabetes mellitusDiabetes Care200427Suppl 1s5s1014693921
- World Health OrganizationGlobal Report on DiabetesGeneva, SwitzerlandWHO2016 Available from: http://apps.who.int/iris/bitstream/10665/204871/1/9789241565257_eng.pdfAccessed August 30, 2016
- WildSRoglicGGreenASicreeRKingHGlobal prevalence of diabetes: estimates for the year 2000 and projections for 2030Diabetes Care20042751047105315111519
- American Diabetes AssociationDiagnosis and classification of diabetes mellitusDiabetes Care201235Suppl 1S64S7122187472
- BalcıoğluASMüderrisoğluHDiabetes and cardiac autonomic neuropathy: clinical manifestations, cardiovascular consequences, diagnosis and treatmentWorld J Diabetes201561809125685280
- RekleitiMSarafisPSaridiMInvestigation of depression in Greek patients with diabetic peripheral neuropathyGlob J Health Sci20135510711423985112
- SprangersMASchwartzCEIntegrating response shift into health-related quality of life research: a theoretical modelSoc Sci Med199948111507151510400253
- JohariNManafZAIbrahimNShaharSMustafaNPredictors of quality of life among hospitalized geriatric patients with diabetes mellitus upon dischargeClin Interv Aging2016111455146127799751
- BannierKLichtenauerMFranzMImpact of diabetes mellitus and its complications: survival and quality-of-life in critically ill patientsJ Diabetes Complications20152981130113526361811
- BakkerSFPouwerFTushuizenMEHoogmaRPMulderCJSimsekSCompromised quality of life in patients with both Type 1 diabetes mellitus and coeliac diseaseDiabet Med201330783583923534496
- FerransCEPowersMJQuality of life index: development and psychometric propertiesANS Adv Nurs Sci19858115243933411
- AndrassyKMCKD Work GroupKidney disease: improving global outcomes (KDIGO). KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney diseaseKidney Int201386Suppl 31150
- HermanWHPop-BusuiRBraffettBHUse of the Michigan neuropathy screening instrument as a measure of distal symmetrical peripheral neuropathy in type 1 diabetes: results from the diabetes control and complications trial/epidemiology of diabetes interventions and complicationsDiabet Med201229793794422417277
- KroenkeKSpitzerRLWilliamsJBWThe PHQ-9: validity of a brief depression severity measureJ Gen Intern Med200116960661311556941
- ToobertDJHampsonSEGlasgowREThe summary of diabetes self-care activities measureDiabetes Care200023794395010895844
- MeijerJWTripJJaegersSMQuality of life in patients with diabetic foot ulcersDisabil Rehabil200123833634011374523
- McNeelyMJBoykoEJAhroniJHThe independent contributions of diabetic neuropathy and vasculopathy in foot ulcerationDiabetes Care19951822162197729300
- WuslinLRJacobsonAMRandLIPsychosocial aspects of diabetic retinopathyDiabetes Care19871033673733297581
- WuslinLRJacobsonAMVisual and psychological function in PDR (Abstract)Diabetes198938Suppl 1242A
- PeyrotMRubinRRLevels and risks of depression and anxiety symptomatology among diabetic adultsDiabetes Care19972045855909096984
- PietteJDRichardsonCValensteinMAddressing the needs of patients with multiple chronic illnesses: the case of diabetes and depressionAm J Manag Care2004102 Pt 215216215005508
- PeyrotMMcMurryJFJrKrugerDFA biopsychosocial model of glycemic control in diabetes: stress, coping and regimen adherenceJ Health Soc Behav199940214115810467761
- JacobsonAMde GrootMSamsonJAThe evaluation of two measures of quality of life in patients with type I and type II diabetesDiabetes Care19941742672748026281
- TriefPMGrantWElbertKWeinstockRSFamily environment, glycemic control, and the psychosocial adaptation of adults with diabetesDiabetes Care19982122412459539989
- AaltoAMUutelaAAroARHealth related quality of life among insulin-dependent diabetics: disease-related and psychosocial correlatesPatient Educ Couns19973032152259104378
- WredlingRStalhammarJAdamsonUBerneCLarssonYOestmanJWell-being and treatment satisfaction in adults with diabetes: a Swedish population-based studyQual Life Res1995465155228556011