
Abstract
The concept of patient engagement in health care is gaining more and more attention not only in the scientific literature, but also as a requirement in the everyday practices of health care organizations. In general terms, the growing body of literature devoted to patient engagement is mainly inspired by the sociological and public health perspectives, which have generated various theories and models trying to explain how people become active agents in their health and care management. However, theories focusing on the psychosocial dimensions intervening in the patient engagement experience are still limited. This paper proposes a psychosocial perspective on patient engagement and discusses the Patient Health Engagement model, which is an evidence-based psychological theory built on extensive qualitative narrative research and literature analysis aimed at explaining patient engagement and its development in the patients’ perspective. The model has been applied to orient patient and professional educational interventions and has contributed to the generation of the first scientific measure of the psychological experience of patients’ engagement in their own care (Patient Health Engagement scale). According to this theory, patient engagement is a developmental process that involves the recovered patients’ ability to have a life projectuality and goal directedness – even if living with a disease. The paper will also discuss the theoretical origins of this model and will conduct a critical comparison of the theory with the Transtheoretical Model of Change developed by Prochaska and the five-stage grief theory by Kubler-Ross.
Video abstract
Point your SmartPhone at the code above. If you have a QR code reader the video abstract will appear. Or use:
Clinical and organizational implications of patient engagement
Patient engagement in health care is gaining more and more attention not only in the scientific literature but also as a requirement for the everyday practices of health care organizations.Citation1–Citation4 In a situation of resource paucity despite the greater demand for health services provision, health care systems are required to “do more with less”.Citation5,Citation6 In this complex situation, the idea of patient engagement has been advanced as a potential solution to make the health care system more effective and efficient.Citation7 First formulated about 10 years ago in the USA, the concept of patient engagement was initially well received by policy makers and health care managers, given the idea that the “individual recipient of care” should be conceived as a crucial actor also in the phases of planning and delivery of the health care services themselves.Citation8,Citation9 In other words, according to a patient engagement oriented view of health care, patients should be considered one of the crucial human resources in the health care organization and as part of the care team.Citation10 Patients not only need to be “put at the center” of the medical action in terms of consideration of their needs and expectations of care, but should also be seen as one of the actors who contribute to the successful accomplishment of the health care organization’s mission and actions.Citation11,Citation12
The proposal of establishing a true partnership between patients and health care organizations and their professionals in the health care journey is magnified by the concept of patient engagement, which defines the individual not only as a passive recipient of care interventions but also as an actor who should orient such a course of action in a co-creative and participative approach to the management of his/her health and care.Citation13 The paradigm of Participatory Medicine is the context in which the concept of engagement grew and assumed concrete meaning.Citation14 This approach stresses the importance of sustaining collaborative spaces not only among health care professionals and patients, but also within the overall health care system and the social communities in which patients are embedded: this approach advocates more closely integrated and synergic approaches to patients’ care.Citation12 This is not to support unregulated self-care without agreement with the responsible health care professional, but – on the contrary – to foster the reciprocal acknowledgment of roles and responsibilities between patients and health care professionals. This mutual awareness and acknowledgment, together with targeted patient education, should be the basis for collaboration and the co-creation of more sustainable and satisfactory health care trajectories.
Factors impacting on patient engagement
The growing body of literature focused on patients’ engagement in their own care is mainly inspired by the sociological and public health perspectives. The most established definitions and models of engagementCitation1,Citation15–Citation18 point to the following factors as impacting on the ability of people to be engaged in their health care. reports the most established definitions of patient engagement in the current scientific literature.
Table 1 Main definitions of patient engagement currently available in the scientific literature
Patient-related factors
Some authorsCitation17–Citation20 have mainly focused on individual-related characteristics of the patient; according to their research, factors such as age,Citation21 ethnicity,Citation22 level of education,Citation20,Citation23 level of income,Citation24,Citation25 and also personal dispositions and beliefs about the patient’s role in managing health careCitation1,Citation20,Citation26,Citation27 may affect individuals’ ability to engage with their health care providers along the medical pathway. Moreover, these studies underline the importance of clinical (ie, the gravity of the disease), cultural (ie, patients’ cultural-related orientations toward their role in the health care consultation), and social (ie, demographic) characteristics of the patient, along with the characteristics of the prescribed therapeutic regimen (ie, frequency, modes of administering the therapy) as key factors that could potentially impede patients from gaining the skills necessary to play an active role in the medical journey.
Health professional-related factors
Other authorsCitation12,Citation27–Citation33 have highlighted the role of health care professionals and the care team’s characteristics in affecting patients’ willingness and disposition to become more active in their health care journey. In particular, factors such as the role identity of the health professionals,Citation7,Citation34 their set of communicative and relational skills,Citation20,Citation35,Citation36 and their attitude toward the concept of patients’ centricity and active engagement in shared decisions about their care processCitation37–Citation41 are all indicated as potential factors fostering or impeding the process of patients’ engagement in their own care. These authors have indicated the role of professionals’ practices and cultures,Citation42–Citation44 together with the level of professionals’ work motivation, work engagement, and organizational commitmentCitation45,Citation46 as crucial elements in sustaining their patients’ choice to engage actively in their own health management. On the contrary, individual or organizational resistances related to the organizational culture of the health and social services can hinder the process of patients’ engagement in their own care. The sensitization and education of health and social practitioners in regard to the concept of engagement is considered a crucial prerequisite for any program promoting the active involvement of patients and their informal/family caregivers.
Organization-related factors
Other authors have discussed the role of enabling factors connected to the organizational structure, and processes featuring the health care system as an unavoidable requirement for the promotion of patients’ engagement in their own care. Specific organizational models, together with the infrastructural features, technological resources available, human resources characteristics, and services’ routines and practices are demonstrated as being crucial factors which may sustain or hinder patients’ engagement in their own care. Particularly crucial is organizational preparedness (in terms of organizational climate and available resources) and organizational processes: for instance, an institutional vision open to new clinical approaches aimed at fostering the patient’s active role and human resources education in this regard.Citation1,Citation12,Citation47–Citation49
Lay community-related factors
Social and community-related factors such as the characteristics of family, informal caregivers, peer networks, and the society as a whole are found to be further facilitators of or obstacles to patient engagement.Citation1,Citation20,Citation50–Citation53 The role of communities in sustaining patients’ motivation to engage in their own health management is much debated, with particular reference to the role of social media and online communities of peers with the same illness.Citation54–Citation57
A health psychology perspective on patient engagement
In regard to the growing debate on patient engagement in health care, it is interesting that the analyses and evidence related to the psychological dimensions involved in such experience are still limited.Citation16
Studies on individual-related factors impacting on patient engagement mainly refer to cultural and sociological determinants, while analysis of the psychological components is mainly focused on cognitive and/or behavioral variables related to such engagement. Based on our research and perspective, only focusing on the behavioral componentCitation17,Citation58,Citation59 of the patient engagement experience might propose again a passivizing approach to patients’ care, as well as it is based on the assumption that a patient has to be “activated” (by someone else) to be effective in self-care.Citation60 For instance, Hibbard et al,Citation19 in their theory of patient activation, describe engagement as a function of patients’ skills, knowledge, and self-efficacy concerning their health and care management. Surprisingly, despite the increasing interest in patient engagement and the growing debate on strategies to foster it, the patients’ psychological and emotional experience related to becoming actively engaged in the health care process has been neglected by the scientific community. Scant attention has been paid to the meaning and lived experience of patients when they become engaged in their health care, the extent to which they want (or not) to be engaged, and the drivers of/barriers against its delivery. This lack of an experience-based modeling of patient engagement may be a missed opportunity to promote the sustainability and effectiveness of services: exploring patients’ perspectives on engagement is crucial for supporting care strategies really able to improve engagement in the real world.Citation61,Citation62
The discipline of health psychologyCitation63,Citation64 may support the analysis of engagement in the “patients’ eyes”. This discipline conducts systematic investigation on how individuals, groups, or organizations enact (or obstruct) health care behaviors and choices. It can offer valuable insights into engagement as a psychosocial and subjective experience, and thus add significantly to the knowledge about engagement and the factors which may sustain or hinder it.
The Patient Health Engagement model
The “Patient Health Engagement” (PHE) model was developed by embracing the notions and paradigms of consumer health psychology. It is an experience-based psychological theory based on the systematic and in-depth study of patients’ illness experiences by means of narrative qualitative research.Citation16,Citation60 According to this theory, patient engagement is a developmental process involving a recovered patient’s capacity to plan realistic life projects (ie, meaningful life aims that the patient might generate unless living with the disease condition) and to be goal oriented – even if living with a disease. The process of patient engagement as described by the PHE model involves four developmental phases, namely, blackout, arousal, adhesion, and eudaimonic project.Citation65 The model points to the role of the emotional component as the main driver of patients’ ability to adjust and adapt to the change of self-role identity involved in the engagement experience. In other words, the concept of engagement implies the patients’ personal choice to change their attitude toward the health care system, from passive, to a partner and co-pilot with the health provider of the health care journey. This change in the personal role identity is a function of patients’ evolving adjustment and resilience to their health condition.
As said above, the PHE model theorizes a developmental view of patient engagement. It suggests that a fully engaged patient results from a continuous emotional and motivational reframing of his/her health status and his/her role identity. According to the PHE model, becoming engaged in health and care management means being more resilient at the emotional level and effectively adjusting to the health condition and its medical requirements. The final phase of the patient engagement process (eudaimonic project) features an individual with a goal-oriented and more positive approach to health management that is – at this stage – more integrated in the patient’s life course. The PHE model theorizes possible trajectories of engagement which are not necessarily linear (a patient may move backward and forward according to critical events in his/her life and disease course). This process also features distinctive ways of interacting and engaging in decisional negotiation between the patient and the health care system that depend closely on the phase of the process through which the patient is passing.
In the following sections, the specific features of each phase of the PHE model will be discussed in depth. These phases are also more deeply explained in some seminal articles by the authorsCitation16,Citation34,Citation38,Citation66,Citation67 ().
Figure 1 Description of the phases featuring the PHE model.
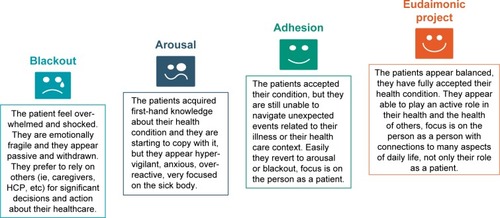
Blackout
This phase of the PHE model mainly occurs when patients experience feelings of psychological vulnerability connected to a critical event, such as a disease diagnosis, a new symptomatology, a disease relapse, and the need to assume new lifestyles in order to manage the health condition. In this phase, patients seem psychologically frozen and feel paralyzed.
In this stage of the PHE model, patients perceive the diagnosis and the requirements for managing the disease as distressing and conflicting with their life habits; for this reason, patients in blackout frequently experience feelings of deep sadness and anger. Consequently, these patients tend to be passive toward their health care providers. To overcome the blackout phase, patients primarily need emotional and psychological support in order to adjust to their new health condition and develop a new sense of agency and control and sense of effectiveness concerning their health management.
Arousal
Patients in arousal have acquired an initial awareness of their health condition, but still have superficial knowledge about how to manage it in an effective way. They are not able to adapt to it and to consider their new health status as part of their daily lives. These patients often report that they are hypervigilant over their body and body signals. Every unexpected change in their body status causes emotional alarm and overwhelming emotional responses. In this position, health care providers are crucial points of reference for patients. They must also support them in managing their illnesses and coping with illness, thus preventing care dropouts (that are particularly frequent in this phase).
Adhesion
When patients succeed in the process of emotional regulation and coping with the illness condition, they experience the third phase of the PHE model: adhesion. In this phase, patients have developed a good acceptance of their disease and have overcome the major psychological stress connected to the disease onset. Moreover, they report being more and more aware of their health status and of its impact on their lives and life habits. In this phase, moreover, patients are increasingly knowledgeable about how to effectively manage their disease and treatment.
However, patients undergoing the adhesion phase are not fully autonomous in their disease management in terms of medical prescription (both life habits and therapeutic regimens), and they frequently experience trouble when something in their life context changes (ie, going on holiday, working life changes, and so on). This happens because patients in this phase are not totally aware of the reasons behind the medical prescriptions; they appear to be formally compliant with their health providers’ requirements, but risk failing when some variables in their life change. As a consequence, patients in this phase need to be assisted by an expert figure who can help them maintain correct health behavior even in stressful or atypical situations. Although patients in this phase still tend to rely frequently on their health care professionals’ advice and support, they also start to perceive the importance of playing an active part in their health care journey. This initial awareness about their role identity, not only as patients but also as persons who are active partners in the medical course, is a crucial antecedent of the last phase of the PHE model: the eudaimonic project phase.
Eudaimonic project
When patients become totally aware of their disease and its implications in terms of changed life habits and therapeutic requirements, they are able to become active agents in reaching a positive and satisfying quality of life, unless living with a disease condition. Patients experiencing the eudaimonic project phase – the last one described by the PHE Model – have elaborated and accepted “patient identity” as one of the many features in a person’s life. In the “eudaimonic project” phase, patients are able to integrate – in a more synergic manner – their health and disease management into their life goals. This reframed perspective of patients toward their health condition makes them able to embrace a more positive and satisfactory approach to their life.
Patients experiencing this phase of the PHE model are also more effective in health information-seeking processes and understanding the rationale behind the medical prescription (differently from the previous phases). Finally, in this phase, patients are able to “activate” the health care professionals when needed, in order fully to respond to their needs and well-being expectations. Health care practitioners are thus considered as reliable allies, and patients see themselves as active members of the care team. Finally, patients in the eudaimonic project phase are also able to become advocates of patients’ rights and to play the role of peer experts in patient associations and advocacy groups, or in co-producing services at a policy level.
The PHE model and its links with other health psychology models
The PHE model discussed in this article has its theoretical roots in both behavioral change and adaptation to change theories and their related constructs in the discipline of health psychology. Inspired by these epistemological roots, the PHE model seeks to furnish a psychosocial processual theory aimed at explaining how people adjust emotionally to their health status and reframe their self-conception, shifting from playing a passive role (asking for a paternalistic approach to care) to considering themselves as authors and owners of their own health and care, ready to act as partners in the health care system in terms of playing an active role in managing their own health. Thus, the PHE model emphasizes the role of the emotional and dynamic components of the engagement process in affecting patients’ cognitions and behaviors related to their health management. Changes imposed by the new health condition on patients’ daily lives may cause emotional upheavals, which often determine the loss of meaning in life, self-confidence, and motivation to go on and adapt to the change. Thus, the dynamic process of psychological adaptation to such a crucial event requires not only a new cognitive mindset and new behavioral skills, but also a complex process of emotional adjustment and self-identity elaboration able to sustain the patient in the reconfiguration of a self-image that does not overlap with the diagnosis but includes it. These emotional and psychodynamic components of the PHE model are – from our perspective – its distinctive features which differentiate and make this psychological approach complementary to other theoretical frameworks of patient engagement rooted in other disciplinary traditions (ie, sociology, public health, health policy) which mainly focus on patients’ behavioral activationCitation1,Citation17,Citation19,Citation59 or cognitive or emotional reframing processes.Citation41,Citation68 The dynamic nature of the emotional adjustment to the disease onset has been well described by the adaptation models developed in the field of health psychology. The term “adaptation theories” is used to denote a group of theories and models that try to explain the psychological process of adjustment that takes place whenever people are faced with situations that require them to undertake a major revision of their assumptions about the world and adapt to those situations (eg, the onset of a disease). One of the most established among these models is the one developed by Kubler-Ross,Citation69 who propounded a five-stage theory describing the psychological reactions of terminally ill individuals to their disease: that is, denial–dissociation–isolation, anger, bargaining, depression, and acceptance. The stage theory of grief has been generalized to a wide variety of adaptation processes, including patient reactions to chronic diseases. The scientific definition of recurrent patterns of individuals’ adaptation to change is undoubtedly of great applied importance because it augments the comprehension of how individuals psychologically react to the life changes with which they are coping. The above-outlined five stages of emotional change theory feature a process that ranges from the astonishment and emotional chaos caused by the critical event to a phase of emotional integration which allows the patient to adapt to the situation and the required changes. The processual model proposed by Kubler-Ross well describes the emotional elaboration and meaning-making process that patients experience when coping with disease. The Kubler-Ross model was a fundamental root for the PHE model. Particularly, some connections can be found with the emotional reactions described in the different phases of PHE model (ie, denial, alert, acceptance, elaboration). However, the PHE model does not only describe the emotional adjustment to the disease and the diagnosis, but also tries to describe how the self-concept reconfiguration (ie, from a healthy individual to an ill patient, to an engaged individual through-out the health care course) happens, so that the patient can embrace a more proactive role in his/her health care journey. However, this implies that the patient autonomously takes the decision to change his/her attitude toward the health care journey by opting for a more proactive role in not only the determination of his/her health outcomes, but also the definition and planning of health care services and pathways. Thus, besides an emotional process of adjustment to the health condition, the PHE model also implies patients’ motivation to change attitudes and behaviors related to health management.
In the domain of health psychology, social cognition models have been widely applied to explain patients’ behavioral change. The Transtheoretical Model of change is certainly the one that has best theorized the evolution of individuals’ motivation and decision making in regard to health behaviors, and it is thus, to some extent, aligned with the PHE model, at least in its theoretical goals. The Transtheoretical Model – by embracing theoretical contributions from various disciplinary domains of psychology – was the first to stress the complexity and the stage process of change in health behavior. In particular, the Transtheoretical Model maintains that individuals change their health behaviors in different stages. They pass from not being concerned to change their behaviors (pre-contemplation stage) to starting to think about them (contemplation) to finally enacting them (action stage) and fully engaging in those behaviors in the long run (maintenance).Citation70 The model furnishes strategies to guide the individual through five stages to long-term maintenance, and it includes self-efficacy as a key construct. This model unveiled the complexity of the patients’ decisional dynamics when changing their health-related behaviors and described 10 cognitive processes which play a role in sustaining patients’ behavioral change toward a more active and aware role in managing health. However, the main focus on self-confidence, on the locus of control, and the decisional balance to nurture the decision for a behavioral change leave less prominence to the emotional and motivational components of that decision. Although Prochaska’s model mentions the role of patients’ (cognitive) awareness about the need to change behaviors, it does not refer to the role of illness emotional elaboration and psychological adaptation to the change (aspects widely addressed, as said above, by the PHE model). Furthermore, this model is not directly linked to the concept of patients’ engagement and participation in health care, but rather on the decision making for health prevention and self-management.
The PHE application to clinical practice
The PHE scale (PHE-s)
There is increasing debate on the importance of giving voice to patients regarding their health and care experience and the importance of collecting patient-reported experience measures.Citation62 Among the patients’ experiences to be recounted and reported, the level of patient engagement is regarded as a key indicator of the quality of patients’ experience, and in particular, as a predictor of how patients will be able to maximize their care pathway. Adopting a scientific measurement of engagement, thus being sensitive to this experience variation among individuals and clinical situations, is key for improving clinical practice. The PHE-sCitation71 has been developed to advance theory in this field (). The scale, developed according to the PHE model theoretical framework, is the first international tool devoted to assess the psychological experience of engagement, and it has robust psychometric proprieties. This quantitative scale only comprises five items and has the peculiarity (in che senso? [in English “peculiar” = “unusual/strange/eccentric”]) of adopting an ordinal structure, so that the patient can describe his/her experience along a continuum of engagement featuring four main positions (see the PHE model). The items were developed based on both systematic analysis of the literature and wide-ranging qualitative studies on chronic patients’ engagement in their health care management.Citation33,Citation38,Citation65 The phrasing of each item was formulated according to the language and terms used by patients in the qualitative phase that oriented the scale development and was then cognitively tested in the pilot phase of the scale generation. This ensured that the items featuring the PHE-s were well understood by the general population. The scale was designed to be self-administered by the patient, who was required to select one response option for each item (line). For more details on administration and scoring, see the previous papers by the authors of this study.Citation71,Citation72
Figure 2 Description of the PHE-s: introduction and items.
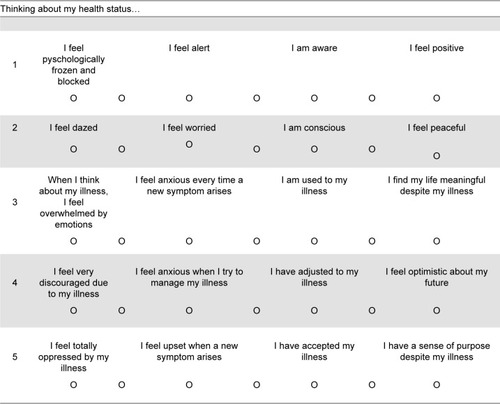
Although the PHE model described four engagement positions, the PHE-s features a seven-point scale to facilitate the patients’ responses and to avoid social desirability biases. To make a patient free to rate himself, positioning in an intermediate position between two stages of engagement might facilitate a more accurate patient response. According to the ordinal nature of the PHE-s, the median score is considered the more reliable index to calculate the final patients’ scoring.Citation72 To obtain the final PHE-s position, the median of the row PHE-s scores should be calculated. According to the score obtained, each respondent can be allocated to one of the four engagement positions as described in the PHE model. The scale is based on the assumption that the score obtained by the patients should reflect the actual patient engagement level.
With its brevity and simplicity, the scale was developed to be easily used in “real-world” clinical contexts in order to give voice to patients about their engagement experience and to offer a structured and reliable measurement for clinicians to tailor their communication strategies with the characteristic of the single patient.Citation72 shows the PHE-s items. PHE-s is at present validated in various languages and cultural contexts. Validations in Italian,Citation71 Chinese,Citation73 and SpanishCitation74 have already been published.
The PHE model in action
As mentioned earlier, the PHE model may be used as a psychological framework not only to assess the engagement of patients, but also to detect their needs and expectations to improve along the engagement journey. In particular, corresponding to each engagement position featured by the PHE model are specific needs of support and psychological counseling. The PHEinACTION intervention protocol has been developed specifically to support patients in their psychological journey of engagement.Citation75 The PHEinACTION intervention protocol is an individual coaching intervention. It consists of two face-to-face consultations with the clinician (eg, nurse, physician, general practitioner, psychologist) sustained by a set of home-based assignments and exercises personalized according to the fours phases of engagement.
The key features of the PHEinACTION intervention are the following:
It is a personalized engagement counseling based on assessment of the level of engagement performed with the PHE-s. The assessment of the level of engagement is considered crucial not only because it personalizes the counseling, but also because it is a first occasion of self-awareness where the patient comes to terms with his/her engagement experience and also an occasion of goal set-ting in terms of the level of engagement to be achieved.
The home-based assignments and exercises proposed are personalized according to the level of patient engagement. Moreover, they are multi-componential, targeting not only the cognitive (health literacy) and behavioral (self-management), but also the emotional resilience of patients.
The protocol is quite simple and structured, and it may be adopted in autonomy by the patient, albeit with the support and supervision of a dedicated health care professional.
For further details, the authors of this study refer to previously published papers.Citation76
Conclusion
To sum up, the psychological adaptation and elaboration have an essential role in how patients can (or cannot) cope with their illness, thus influencing their possibility and choice to become effectively engaged in their health care. The transition from a passive approach to active behaviors in managing health and care is based on a complex process of meaning-making and self-identity elaboration, which is primarily emotional and psychodynamic. The subjective, and sometimes irrational, perceptions that individuals have about themselves and the subjective viewpoint through which individuals define the criteria to evaluate their quality of life are – in our opinion – fundamental for enabling the process of engagement and should be included in real-life health engagement models. The value of a psychosocial theory – like the one proposed by the PHE model – is judged not only by its explanatory and predictive power, but also by its applied potential to guide psychosocial changes. In this regard, the PHE model has demonstrated quite an interesting predictive power on the level of patients’ adherence to medical prescriptionsCitation16 and on the level of patients’ empowerment in self-management.Citation66 These features of the PHE model make this theory particularly interesting also for both service delivery and policy making, because it may function as a “compass” to orient and personalize clinical actions and policy making initiatives based on the patient or population level of patient engagement (and, on the contrary, risks of disengagement). The PHE model has the strength of offering a processual explanation of the psychosocial dynamics occurring when a patient becomes engaged in his/her own health care and recognizes that being fully engaged strongly depends on individuals’ choice and disposition to play an active role in the care team. For these reasons, the model – according to the current literature – does not maintain that more engagement is always the best. On the contrary, effective patient engagement occurs when the health care system recognizes and addresses the patient’s unique needs specific of each patient engagement phase. However, the shortcoming of the model is that it does not measure actual patient engagement behaviors. Future research should, therefore, illuminate the heuristic and applicative power of the PHE model, above all, in predicting patient engagement behaviors. Nevertheless, adoption of a psychosocial approach for defining and measuring patient engagement promises to greatly enhance our understanding of how people can decide to change their role in the health care journey in favor of engagement.
Disclosure
The authors report no conflicts of interest in this work.
References
- CarmanKLDardessPMaurerMPatient and family engagement: a framework for understanding the elements and developing interventions and policiesHealth Aff (Millwood)20133222323123381514
- DentzerSRx for the “Blockbuster Drug” of patient engagementHealth Aff2013322202
- BlantonKThe patient engagement prescriptionN C Med J201576315716026510218
- PelletierLRStichlerJFAction brief: patient engagement and activation: a health reform imperative and improvement opportunity for nursingNurs Outlook2013611515423527404
- SuhrckeMNugentRAStucklerDRoccoLChronic Disease: An Economic PerspectiveLondonOxford Health Alliance2006
- GordonJELeimanJMDelandELPardesHDelivering value: provider efforts to improve the quality and reduce the cost of health careAnnu Rev Med20146544745824111890
- CoulterALeadership for patient engagementKing’s Fund201220
- BarelloSGraffignaGSavareseMBosioACEngaging patients in health management: towards a preliminary theoretical conceptualizationPsicologia della Salute2014331133
- GraffignaGBarelloSTribertiSPatient engagement: A consumer-centered model to innovate healthcareBerlinWalter de Gruyter GmbH & Co KG2016
- VahdatSHamzehgardeshiLHessamSHamzehgardeshiZPatient involvement in health care decision making: a reviewIran Red Crescent Med J2014161e1245424719703
- GraffignaGBarelloSRivaGPromozione del patient engagement in ambito clinico-assistenziale per le malattie croniche: raccomandazioni dalla prima conferenza di consenso italiana [Promotion of patient engagement in the clinical-care setting for chronic diseases: recommendations from the first Italian consensus conference]Recenti Prog Med2017108455475 Italian29149163
- GraffignaGBarelloSRivaGFertilizing a patient engagement ecosystem to innovate healthcare: toward the first Italian Consensus conference on patient engagementFront Psychol201781628197108
- HardymanWDauntKLKitchenerMValue co-creation through patient engagement in health care: a micro-level approach and research agendaPublic Manag Rev201517190107
- DysonEWhy Participatory medicine?J Particip Med2009115
- HibbardJHStockardJMahoneyERTuslerMDevelopment of the patient activation measure (PAM): conceptualizing and measuring activation in patients and consumersHealth Serv Res2004394I1005102615230939
- GraffignaGBarelloSBonanomiAThe role of Patient Health Engagement model (PHE-model) in affecting patient activation and medication adherence: a structural equation modelPLoS One2017126e017986528654686
- GrumanJRovnerMHFrenchMEFrom patient education to patient engagement: implications for the field of patient educationPatient Educ Couns201078335035620202780
- ForbatLCaylessSKnightingKCornwellJKearneyNEngaging patients in health care: an empirical study of the role of engagement on attitudes and actionPatient Educ Couns2009741849018790594
- HibbardJHMahoneyEToward a theory of patient and consumer activationPatient Educ Couns201078337738120188505
- RodriguezKMIntrinsic and extrinsic factors affecting patient engagement in diabetes self-management: perspectives of a certified diabetes educatorClin Ther20133517017823411000
- ParkerJLReganJFPetroskiJBeneficiary activation in the Medicare populationMedicare Medicaid Res Rev201444E14
- RyvickerMFeldmanPHChiuY-LGerberLMThe role of patient activation in improving blood pressure outcomes in Black patients receiving home careMed Care Res Rev201370663665223864112
- RademakersJNijmanJBrabersAEMde JongJDHendriksMThe relative effect of health literacy and patient activation on provider choice in the NetherlandsHealth Policy20141142–320020623972373
- NijmanJHendriksMBrabersAde JongJRademakersJPatient activation and health literacy as predictors of health information use in a general sample of Dutch health care consumersJ Health Commun201419895596924397280
- LubetkinEIZaborECBrennesselDKemenyMMHayJLBeyond demographics: differences in patient activation across new immigrant, diverse language subgroupsJ Community Health2014391404923918645
- SimmonsLAWoleverRQBechardEMSnydermanRPatient engagement as a risk factor in personalized health care: a systematic review of the literature on chronic diseaseGenome Med201461624571651
- GagliardiARLemieux-CharlesLBrownADSullivanTGoelVBarriers to patient involvement in health service planning and evaluation: an exploratory studyPatient Educ Couns200870223424118023129
- ThompsonAGHThe meaning of patient involvement and participation in health care consultations: a taxonomySoc Sci Med20076461297131017174016
- KennedyAGaskLRogersATraining professionals to engage with and promote self-managementHealth Educ Res200520556757815741189
- The King’s FundLeadership and engagement for improvement in the NHS: together we canLeadersh Rev2012148
- BarelloSGuendalinaGGiulianaPMailaMMaurizioCLivioPAn educational intervention to Train professional nurses in promoting patient engagement: a pilot feasibility studyFront Psychol20172020
- CoulterAPatient engagement – what works?J Ambul Care Manage201235808922415281
- BarelloSGraffignaGVegniESavareseMLombardiFBosioAC“Engage me in taking care of my heart”: a grounded theory study on patient-cardiologist relationship in the hospital management of heart failureBMJ Open201553e005582
- GraffignaGBarelloSBonanomiAMenichettiJThe motivating function of healthcare professional in eHealth and mHealth interventions for type 2 diabetes patients and the mediating role of patient engagementJ Diabetes Res20162016297452126881243
- ZolnierekKBHDimatteoMRPhysician communication and patient adherence to treatment: a meta-analysisMed Care20094782683419584762
- BigiSCommunication skills for patient engagement: argumentation competencies as means to prevent or limit reactance arousal, with an example from the italian healthcare systemFront Psychol20167147227729890
- GreeneJHibbardJHAlvarezCOvertonVSupporting patient behavior change: approaches used by primary care clinicians whose patients have an increase in activation levelsAnn Fam Med201614214815426951590
- BarelloSGraffignaGEngaging patients to recover life projectuality: an Italian cross-disease frameworkQual Life Res20152451087109625373927
- LamianiGBarelloSBrowningDMVegniEMeyerECUncovering and validating clinicians’ experiential knowledge when facing difficult conversations: a cross-cultural perspectivePatient Educ Couns201287330731222196987
- CouëtNDesrochesSRobitailleHAssessments of the extent to which health-care providers involve patients in decision making: a systematic review of studies using the OPTION instrumentHealth Expect201314542561
- KohHKBrachCHarrisLMParchmanMLA proposed “health literate care model” would constitute a systems approach to improving patients’ engagement in careHealth Aff (Millwood)201332235736723381529
- GrantBColelloSHCulture change through patient engagementNurs Manage201041104446
- AppelboomGLoPrestiMReginsterJ-YSander ConnollyEDumontEPLThe quantified patient: a patient participatory cultureCurr Med Res Opin201413
- ZeunerRFroschDLKuzemchakMDPolitiMCPhysicians’ perceptions of shared decision-making behaviours: a qualitative study demonstrating the continued chasm between aspirations and clinical practiceHealth Expect20141862465247624938120
- AbdelhadiNDrach-ZahavyAPromoting patient care: work engagement as a mediator between ward service climate and patient-centred careJ Adv Nurs2012681276128721913960
- GillPSPatient engagement: an investigation at a primary care clinicInt J Gen Med20136859823515133
- PiñaILCohenPDLarsonDBA framework for describing health care delivery organizations and systemsAm J Public Health2015105467067924922130
- SafranDGMillerWBeckmanHOrganizational dimensions of relationship-centered care. Theory, evidence, and practiceJ Gen Intern Med200621Suppl 1S9S15
- LuxfordKSafranDGDelbancoTPromoting patient-centered care: a qualitative study of facilitators and barriers in healthcare organizations with a reputation for improving the patient experienceInt J Qual Health Care201123551051521586433
- HibbardJHCommunity-based participation approaches and individual health activationJ Ambul Care Manage200932427527719887999
- BertoniADonatoSGraffignaGBarelloSPariseMEngaged patients, engaged partnerships: singles and partners dealing with an acute cardiac eventPsychology, health & medicine2015205505517
- GrandeSWFaberMJDurandMAThompsonRElwynGA classification model of patient engagement methods and assessment of their feasibility in real-world settingsPatient Educ Couns201495228128724582473
- NgC-JLeeP-YLeeY-KAn overview of patient involvement in healthcare decision-making: a situational analysis of the Malaysian contextBMC Health Serv Res20131340824119237
- FisherJClaytonMWho gives a tweet: assessing patients’ interest in the use of social media for health careWorldviews Evid Based Nurs20129210010822432730
- GraffignaGBarelloSTribertiSWiederholdBKBosioACRivaGEnabling ehealth as a pathway for patient engagement: a toolkit for medical practiceStud Health Technol Inform2014199132124875682
- IrizarryTDeVito DabbsACurranCRPatient portals and patient engagement: a state of the science reviewJ Med Internet Res2015176e14826104044
- FranklinVLGreeneAWallerAGreeneSAPagliariCPatients’ engagement with “Sweet Talk” – a text messaging support system for young people with diabetesJ Med Internet Res2008102e2018653444
- HibbardJHelenGSupporting people to manage their health: an introduction to patient activationKing’s Fund201451151
- DukeCCLynchWDSmithBWinstanleyJValidity of a new patient engagement measure: the altarum consumer engagement (ACE) measure™Patient20158655956826097010
- GraffignaGBarelloSTribertiSGiving (back) a role to patients in the delivery of healthcare services: Theoretical roots of patient engagement Patient Engagement: A Consumer-Centered Model to Innovate HealthcareGraffignaGBarelloSTribertiSWarsawDe Gruyter Open20151326
- CoulterACollinsAMaking decision making a reality. No decision about me, without meKings Fund2011156 Available from: http://www.kingsfund.org.uk/publications/nhs_decisionmaking.htmlAccessed March 23, 2018
- CoulterAMeasuring what matters to patientsBMJ2017j81628219884
- AlbaJWHutchinsonJWConsumer psychologyHandbook of Applied CognitionSecond EditionNew YorkWiley2008683711
- TwedtDWConsumer psychologyAnnu Rev Psychol196516126529414268888
- GraffignaGBarelloSLibreriCBosioCAHow to engage type-2 diabetic patients in their own health management: implications for clinical practiceBMC Public Heal2014141648
- GraffignaGBarelloSBonanomiARivaGFactors affecting patients’ online health information-seeking behaviours: the role of the Patient Health Engagement (PHE) ModelPatient Educ Couns2017100101918192728583722
- GraffignaGBarelloSModelling patient engagement in healthcare: Insight for research and pratice Patient Engagement: A Consumer-Centered Model to Innovate HealthcareGraffignaGBarelloSTribertiSWarsawDe Gruyter Open20152743
- McCormackLThomasVLewisMARuddRImproving low health literacy and patient engagement: a social ecological approachPatient Educ Couns2017100181327475265
- Kubler-RossEOn Death and Dying1New YorkThe Macmillan Company1969
- ProchaskaJOVelicerWFThe transtheoretical model of health behavior changeAm J Heal Promot AJHP19971213848
- GraffignaGBarelloSBonanomiALozzaEMeasuring patient engagement: development and psychometric properties of the patient health engagement (PHE) scaleFront Psychol2015627425870566
- GraffignaGBarelloSThe Value of Measuring Patient Engagement in Healthcare: New Frontiers for Healthcare QualityGraffignaGPromoting Patient Engagement and Participation for Effective Healthcare Reform, Medical Information Science ReferenceHershey PA, USA2016192214
- ZhangYGraffignaGBonanomiAAdaptation and validation of a Chinese version of patient health engagement scale for patients with chronic diseaseFront Psychol201781928197108
- MagallaresAGraffignaGBarelloSBonanomiALozzaESpanish adaptation of the Patient Health Engagement scale (S.PHE-s) in patients with chronic diseasesPsicothema201729340841328693715
- MenichettiJGraffignaG“PHE in action”: development and modeling of an intervention to improve patient engagement among older adultsFront Psychol20167140527695435
- MenichettiJGraffignaG“PHE in Action”: development and modeling of an intervention to improve patient engagement among older adultsFront Psychol20167140527695435
- LégaréFWittemanHOShared decision making: examining key elements and barriers to adoption into routine clinical practiceHealth affairs201332227628423381520
- MittlerJNMartsolfGRTelenkoSJScanlonDPMaking sense of “consumer engagement” initiatives to improve health and health care: a conceptual framework to guide policy and practiceThe Milbank Quarterly2013911377723488711