Abstract
Nearly 15 million people in the United States suffer from either aortic or mitral valvular disease. For patients with severe and symptomatic valvular heart disease, valve replacement surgery improves morbidity and mortality outcomes. In 2009, 90,000 valve replacement surgeries were performed in the United States. This review evaluates the advantages and disadvantages of mechanical and bioprosthetic prosthetic heart valves as well as the factors for consideration in deciding the appropriate valve type for an individual patient. Although many caveats exist, the general recommendation is for patients younger than 60 to 65 years to receive mechanical valves due to the valve’s longer durability and for patients older than 60 to 65 years to receive a bioprosthetic valve to avoid complications with anticoagulants. Situations that warrant special consideration include patient co-morbidities, the need for anticoagulation, and the potential for pregnancy. Once these characteristics have been considered, patients’ values, anxieties, and expectations for their lifestyle and quality of life should be incorporated into final valve selection. Decision aids can be useful in integrating preferences in the valve decision. Finally, future directions in valve technology, anticoagulation, and medical decision-making are discussed.
Overview
Nearly 15 million people in the United States suffer from either aortic or mitral valvular disease.Citation1,Citation2 For patients with severe and symptomatic valvular heart disease, valve replacement surgery improves morbidity and mortality outcomes. In 2009, 90,000 valve replacement surgeries were performed in the United States.Citation3 In general, 2 options exist for replacement valves – mechanical and bioprosthetic valves. The decision on which valve replacement to use requires careful consideration of the specific advantages and disadvantages of the valve types and integration of this knowledge into the clinical characteristics and personal preferences of the individual patient. This article outlines advantages and disadvantages of each valve type, as well as outcomes and factors for consideration in deciding the appropriate valve type for an individual patient.
Mechanical valves
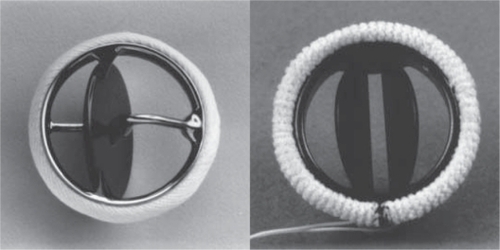
The two common types of mechanical valves, tilting-disc and bileaflet valves (),Citation4 have comparable durability and both require life-long anticoagulation therapy due to their associated thrombotic risk.Citation5
Figure 1 Photographs of commonly used prosthetic valves. Left: single-tilting-disk (Medtronic-Hall, Medtronic, Minneapolis, MN) valve; Right: bileaflet-tilting-disk (St Jude Medical, Little Canada, MN) valve.
Mechanical valve advantages
Mechanical valves have advantages and disadvantages, the most important of which is their greater durability (20–30 years) than tissue bioprosthetic valves (10–15 years).Citation6–Citation9 Their greater durability translates into lower reoperation rates among these patients, compared with patients with bioprosthetic valves.Citation9,Citation10
The excellent durability of mechanical valves was illustrated most definitively by a trial that randomized 575 patients between 1977 and 1982 at 13 different US Department of Veterans Affairs centers to receive either a mechanical or bioprosthetic valve replacement. The investigators found that patients younger than 65 years who received a bioprosthetic valve had a greater rate of primary valve failure for both aortic valve replacements (AVR) and mitral valve replacements (MVR) 15 years after implantation compared with similarly aged patients with mechanical valve replacements (bioprosthetic vs mechanical 26% vs 0%, P < 0.001 for AVR and 44% vs 4%, P < 0.001 for MVR). However, in patients older than 65, there was no significant difference in primary valve failure between the two valve types, presumably due to the shorter lifespans of the older patients.Citation11 This large randomized control study demonstrates the excellent durability of mechanical heart valves compared with bioprosthetic heart valves.
Mechanical valve disadvantages
Although mechanical valves are more durable than bioprosthetic valves, mechanical valves also have several disadvantages that a provider and patient must consider. Blood flow around the mechanical valve results in high sheer stresses, which can result in platelet activation and a higher risk for thrombosis on the valve surface and a subsequent risk for embolism. Given this risk, all patients with mechanical heart valves require lifelong anticoagulation, most commonly with a vitamin K antagonist such as warfarin. Although warfarin use is efficacious in reducing thrombosis risk, it heightens hemorrhagic risk.Citation9,Citation10,Citation12,Citation13 For example, a 60-year-old male with a mechanical valve replacement has a lifetime risk of bleeding of 41% compared with a 12% risk in a similar patient with a bioprosthetic valve replacement.Citation14
Anticoagulation and bleeding
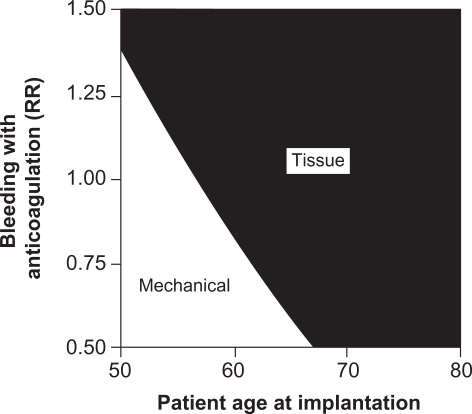
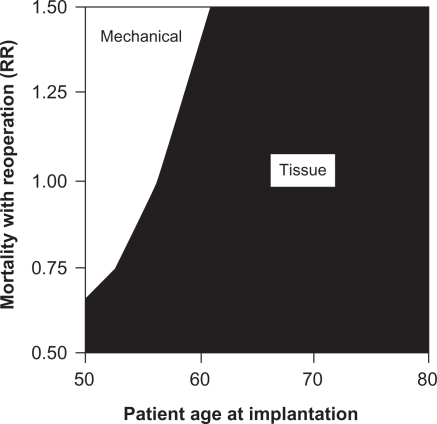
Furthermore, the risk of bleeding from anticoagulant therapy increases as patients age.Citation15–Citation25 Patients with mechanical valves on anticoagulation therapy who are older than 60 years are nearly 7 times more likely to bleed than patients younger than 60.Citation15 The increased risk of bleeding with a mechanical valve replacement in older patients further supports avoiding mechanical valves in this population. illustrates this concept in a 2-way sensitivity analysis that studies the interaction between age and bleeding risk in deciding on valve type. As the age of the patient increases and/or the relative risk of bleeding on anticoagulation increases, tissue valve implantation becomes more favorable than mechanical valve implantation.Citation26
Figure 2 Two-way sensitivity analysis of the effects of anticoagulant-related bleeding and patient age at implantation on the recommended valve type.
The need for anticoagulation therapy, usually with warfarin, introduces a variety of additional considerations for both providers and patients. Therapeutic levels of warfarin are difficult to achieve and maintain, due to both barriers to adherence and the variety of interactions that warfarin has with other medications and diet. A recent study underscored this difficulty by demonstrating that only 62% of those patients with a mechanical valve on anticoagulation medication are found within the appropriate international normalized ratio (INR) range, even in the setting of adequate medication adherence.Citation15 In order to maximize the benefits and minimize the risks of warfarin therapy, patients are required to make significant and lifelong lifestyle adjustments, including frequent office visits to monitor INR levels, monitoring of their diet to maintain consistent levels of vitamin K, and avoidance of contact sports and other potentially traumatic situations.Citation26
Anticoagulation and co-morbidities
Individual patient co-morbidities also affect the decision for mechanical valve replacement and its attendant need for anticoagulation. For example, a mechanical valve is recommended when the patient is already on anticoagulants for another medical condition, such as atrial fibrillation or a thrombotic disorder.Citation3,Citation27 Patients and providers also need to consider future scenarios where discontinuation of anticoagulation with warfarin would be necessary, such as surgical procedures or pregnancy.Citation28 Warfarin is contraindicated with pregnancy. As such, the provider and patient need to consider the implantation of a bioprosthetic valve in a woman with the potential to become pregnant. Careful discussion of these possibilities and ongoing communication between provider and patient are essential to anticipate these events and adjust therapies accordingly.
In summary, mechanical valves offer greater durability at the expense of lifelong anticoagulation, higher bleeding risks, and the attendant lifestyle modifications and considerations to minimize these risks.Citation3,Citation29,Citation30 Accordingly, mechanical valves are generally recommended for younger patients since a patient with a longer life expectancy is more likely to outlive a bioprosthetic valve and require a reoperation.Citation13,Citation26,Citation31 However, valve type selection should be a shared decision-making process in choosing the optimal prosthetic heart valve for a specific patient in order to minimize the valve’s associated risks.Citation3,Citation13,Citation26,Citation29–Citation31
Bioprosthetic valves
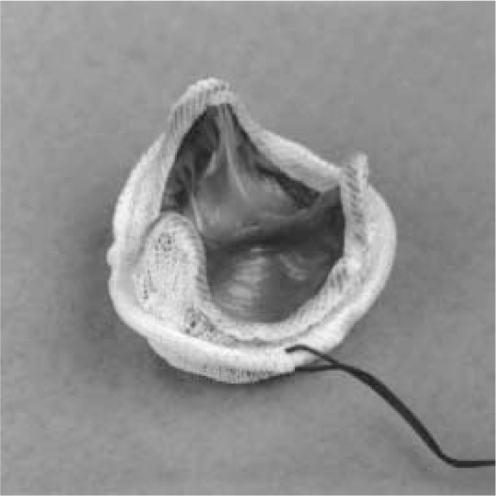
Bioprosthetic valves commonly used in clinical practice are called heterografts, which are usually stented or stentless porcine or bovine tissue valvesCitation3 (see ).Citation4 Heterografts have similar advantages and limitations relative to mechanical valve replacements.Citation32
Figure 3 Photograph of Porcine (Carpentier–Edwards) Bioprosthesis.
Bioprosthetic valve advantages
The main advantage with bioprosthetic valves is that they do not require lifelong warfarin therapy, due to their lower thrombotic risk compared with mechanical valves (0.87% and 1.4%, per year respectively).Citation13,Citation14 Accordingly, patients with bioprosthetic valves have a significantly decreased risk of bleeding.Citation10,Citation14
Bioprosthetic valve disadvantages
The bioprosthetic valve also has disadvantages. Whereas the mechanical valve has an increased risk of thromboembolism but is more durable, the prosthetic valve has a decreased risk of thromboembolism but is less durable. This process of structural valve deterioration is poorly understood but is thought to result from the accumulation of calcium and lipids on the valve surface.Citation33 An incomplete saline rinse of the valve both prior to and during surgery can also exacerbate structural valve deterioration leading to an increased risk of valve thickening and calcification.Citation34 Improvements in second-generation bioprosthetic valves have reduced the rapidity of deterioration compared with first-generation valves, but structural valve deterioration remains a major disadvantage for bioprosthetic valves.Citation10 For most patients with a bioprosthetic valve, structural valve deterioration begins around 5 years post-implantation and rapidly increases. For example, one study demonstrated that at 5 years post-implantation of a bioprosthetic valve, structural valve deterioration occurred in 1.0% ± 0.3% of patients. At 10 and 15 years post-implantation, rates of structural valve deterioration increased to 17.2% ± 2.2% and 37.2% ± 5.8% of patients, respectively.Citation13
Bioprosthetic valves and reoperation
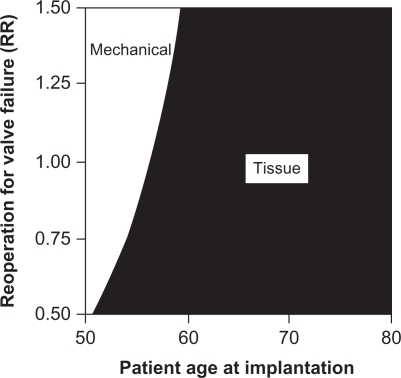
This increased risk of deterioration translates to an increased risk of reoperation for these patients. One study compared the durability of the bioprosthetic valve and mechanical valve and concluded that the lifetime risk of reoperation is 25% for a bioprosthetic valve compared with 3% for a mechanical valve.Citation10,Citation14 This risk of reoperation is a major driver in the decision to select a mechanical or tissue valve. illustrates this concept with a 2-way sensitivity analysis comparing the relative risk for reoperation to the patient’s age at initial valve implantation. As the relative risk of reoperation increases, the optimal decision favors mechanical valve implantation for more patients. However, at age 60 years and higher, tissue valves appear to be the dominant strategy even with a 50% higher risk of reoperation, since the expected lifespan of the patient is not likely to exceed the lifespan of the tissue valve.Citation26
Figure 4 Two-way sensitivity analysis of the effects of reoperation for tissue valve failure and patient age at implantation on the recommended valve type.
Reoperation to replace a failed prosthetic valve has risks. A 2009 analysis from a Vancouver dataset demonstrated that the mortality risk of reoperation to replace a bioprosthetic valve that has deteriorated is 7.3% (average patient age was 54 years old).Citation14 Interestingly, old age does not excessively increase mortality in valve replacement surgeries.Citation35 Nonetheless, proper decision-making around valve replacement requires consideration of the risks of reoperation and its associated mortality. demonstrates this trade-off in a 2-way sensitivity analysis comparing the relative risk of reoperation-associated mortality and patient age at valve implantation.Citation26 At younger ages, higher relative risks of surgical mortality favor implantation of a mechanical valve. However, for patients aged 60 years or more, the likelihood of reoperation is low enough to justify tissue valve implantation, even in patients with a 50% higher relative risk of reoperative mortality.
Figure 5 Two-way sensitivity analysis of the effects of mortality with reoperation and patient age at implantation on the recommended valve type.
Given these relative risks of structural valve deterioration and subsequent reoperation, the current general recommendation for patients older than 60 to 65 years is a bioprosthetic valve and for patients less than 60 to 65 years is a mechanical valve.Citation10,Citation26 For a 65-year-old patient, structural valve deterioration of a tissue valve will occur, on average, 10 to 15 years after implantation while the patient’s life expectancy is only 11.3 years.Citation10,Citation36 Thus, a patient choosing to undergo a prosthetic valve replacement at 65 years will have a 28% chance of needing a reoperation.Citation10 As tissue valves continue to improve in durability and rates of reoperation decrease, lowering of the recommended age for tissue valve implantation may occur.Citation11,Citation15,Citation36,Citation37 Conversely, as life expectancy continues to increase, more elderly patients may face the need for a tissue valve replacement. Thus, decision-making about valve type will need to keep these changes in mind.
Bioprosthetic valves and co-morbidities
Certain subpopulations of patients require special consideration in the decision to implant a tissue valve. Co-morbidities that confer a shortened life expectancy, such as renal failure requiring dialysis or cancer, may favor tissue valve implantation.Citation3,Citation15 Other co-morbidities, such as hyperparathyroidism, appear to accelerate tissue valve deterioration and thus may favor mechanical valve implantation.Citation3 Accordingly, the general recommendations for valve selection need to be considered in light of the patient’s co-morbidities and individual circumstances.
Factors affecting valve selection
The process of deciding which prosthetic valve type is best for an individual patient is complex. Consideration of the general advantages and disadvantages of the valve types, as outlined above, is only the first step. These general recommendations need to be then tailored to the individual patient’s clinical condition and, equally importantly, personal preferences. Once the specific advantages and disadvantages are considered in the context of the individual patient, then the information needs to be communicated in an effective way for the provider and patient to fully comprehend the consequences of valve selection. Finally, frameworks to allow for incorporation of the myriad factors to aid decision-making are necessary.
Age
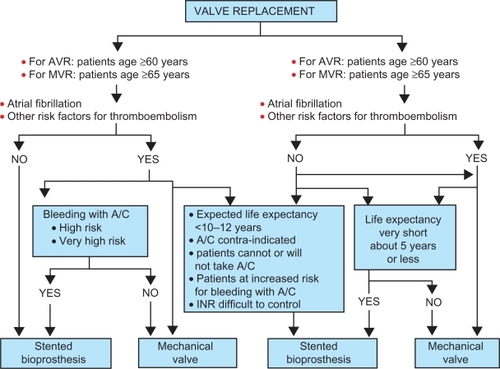
The general recommendations around valve choice center on age, taking into consideration the life expectancy of the patient in relation to the valve. Patients older than 65 years typically do not outlive the life expectancy of a tissue valve.Citation11,Citation15 In light of the higher bleeding event rates relative to reoperation rates, implanting a tissue valve in an elderly patients can avoid anticoagulation and its attendant bleeding risks.Citation3,Citation10 Thus, the current recommendation for patients older than 60 to 65 years is a bioprosthetic valve. Patients younger than 50 years are more likely to experience structural valve deterioration and a need for reoperation; so mechanical valves are generally recommended for younger patients. is an example of an algorithm that integrates general recommendations with patient co-morbidities, valve risk assessment, life expectancy, and patient preference.Citation15
Figure 6 Algorithm for choice of prosthetic heart valve.
Abbreviations: A/C, anticoagulants; AVR, aortic valve replacements; INR, international normalized ratio; MVR, mitral valve replacements.
In support of current recommendations, studies have compared the lifetime rates of reoperation after bioprosthetic valve implantation to the rates of bleeding events after mechanical valve implantation and concurrent anticoagulation.Citation10 Among 35-year-old patients, the lifetime risks are 63% for reoperation and 83% for bleeding events. For 65-year-old patients, these risks are 28% and 47%, respectively. For 75-year-old patients, these risks are 11% and 24%, respectively. In addition, a separate study found that the mortality risk of reoperation is 3 times less than the mortality risk of a bleeding event.Citation14 These results reflect the greater reoperation risk of implanting a bioprosthetic valve in individuals younger than 60 to 65 years, but illustrate how these reoperation risks may be less significant than bleeding risks associated with anticoagulation.
Surgical factors and co-morbidities
Once the relative advantages and disadvantages of valve type are properly appreciated, then providers need to consider individual patient factors that can influence valve selection. Surgical factors, such as concurrent need for aortic root replacement, may favor one valve type over the other.Citation27 Other co-morbidities, such as atrial fibrillation, renal failure, and other conditions refererred to above, will also affect the valve selection. Other significant medical history of the patient, contraindications, and the potential of pregnancy are other issues that the provider and patient need to consider.
Patient preferences
Once the individual patient characteristics have been considered, discussion should then turn to the patient’s values, anxieties and expectations for their lifestyle and quality of life and how these affect the valve selection. Ultimately, assuming no contraindication to anticoagulants, the patient’s choice will largely depend on which potential outcome, reoperation with a tissue valve or lifelong anticoagulation with a mechanical valve, he or she wishes to keep at a minimum.Citation15 If the patient refuses to be on warfarin therapy regardless of reoperation risk, then the valve type selection process is relatively straightforward. Similarly, if the patient is strongly opposed to reoperation and would rather take life-long warfarin, then the valve type selection process is also relatively straightforward. However, when the patient’s preferences are not strongly associated with one valve type over another, the provider and patient must together evaluate the complex issues of valve selection and make a decision.
Evaluation of competing risks is a complex task, due to the uncertainty surrounding various outcomes, the difficulty in valuing future events, and the relative unfamiliarity patients have with the medical consequences of their decisions. It is essential to communicate these risks in an understandable form to patients and to provide frameworks for decision-making.
Decision aids
Decision aids are a promising approach in effective communication of risks to patients. One such example of their effectiveness has been illustrated among patients with early stage breast cancer and their need to choose between mastectomy and lumpectomy. Decision aids have been constructed to illustrate the options in an understandable format, using pie graphs and other illustrative diagrams. Investigators have studied the effectiveness of decision aids on knowledge in decision-making about breast cancer surgery. They found that decision aids enable the patient to be more knowledgeable about the treatment options, reduce decisional conflict, and ultimately bring the patient more satisfaction of the decision.Citation38 These tools improve the decision-making process by placing an emphasis on patient knowledge and therefore ultimately patient preference. This shared decision-making process offers the patient ownership of their decision, which can lead to better medication and therapeutic regimen adherence. Employing decision aids in prosthetic valve selection may offer similarly beneficial outcomes.
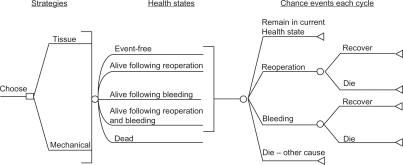
Once risks have been properly specified and communicated, they need to be incorporated into an overall decision-making framework to assist providers and patients in making an optimal choice. Two decision-making models are potentially useful. One option is the utilization of decision trees. Decision trees model current and future choices and calculate the probability of various outcomes. The decision tree is a useful decision-making tool that simplifies complex issues into a more understandable format. In addition, decision trees can incorporate patient preferences in the decision-making process. For example, is a decision tree that associates chance events with each valve selection in a framework that allows for more effective decision-making.Citation26
Figure 7 Schematic of decision model structure. All patients are initially in the event-free state. With each 1-year cycle of the model, they can move to a different state or remain in the same state according to chance events specified under “Chance events each cycle”.
Another potential tool is a microsimulation model. A microsimulation model calculates probabilities of events, similar to decision models, but then performs thousands of simulations of patients making various decisions and experiencing outcomes within the model. This analysis allows for these simulated patients to reflect similar ages, medical histories, and values of the patient facing the decision, and thus allows the patient and his or her provider to predict more accurately the likely outcome of their decision.Citation10,Citation39 Both microsimulation models and decision trees are potentially helpful options in the valve type selection process.
Costs
Finally, costs associated with valve selection should be part of the decision-making process. From the patient’s perspective, costs include money spent on co-pays, medication, and other medical care; money spent on lifestyle adaptations; and economic costs such as lost income and missed days at work secondary to medical care and/or complications. Costs incurred by family members or other support and their assistance with transportation and emotional support should also be incorporated into the overall valve selection considerations.
Selection of the ideal valve type for a given patient involves a dizzying array of variables. However, by carefully considering the medical circumstances of the individual patient and incorporating their preferences, ideally with the assistance of decision aids and frameworks such as decision or microsimulation models, the likelihood of making a satisfactory choice increases. A patient’s satisfaction with his or her decision can significantly affect their quality of life and highlights the importance of the prosthetic heart valve choice being a shared decision between the provider’s expertise and the patient’s expectations.Citation40
Future directions
Innovations in prosthetic valve construction, anticoagulation, and medical decision-making will all affect future valve selection. For patients considering mechanical valve replacement, improvements in valve structure may lower thrombotic risk and require lower intensity of anticoagulation.Citation14 New oral anticoagulants, such as dabigatran and rivaroxaban, have a fixed dosing regimen that delivers a more consistent anticoagulant effect that may eliminate the need for frequent monitoring. This improved pharmacokinetic profile also has potential to significantly reduce the associated bleeding risks of anticoagulation with mechanical valves.Citation41 Improvements in tissue valves and implantation technique may reduce structural valve deterioration, thus improving valve durability and reducing reoperation rates. Any or all of these innovations would substantially affect the current considerations in prosthetic valve selection.
Improvements in decision aids and medical decision-making need to accompany technical improvements in prosthetic valves and anticoagulation. Further refinement of risk quantification and communication of risk to patients is essential to improve patient comprehension and the quality of decision-making. An integral part of refinements in risk quantification is ongoing research in the actual outcomes of contemporary patients receiving valve replacements. Many studies that form the foundation of our understanding of valve outcomes are derived from studies occurring decades ago and primarily in Caucasian males. Updating this information with outcomes from a more diverse patient population using modern surgical techniques, valve technology, and anticoagulation strategies will allow for more precise characterization of the risks and benefits that current patients face in valve selection.
Conclusion
Optimal valve selection results when the patient and provider carefully consider the advantages and disadvantages of each valve type in the context of the individual patient’s age, clinical conditions, values, and lifestyle desires. The provider needs to communicate clearly the medical considerations, and both provider and patient need to appropriately weigh medical and individual considerations in the final decision, ideally employing validated decision aids and models to assist with their deliberation. This calculated and thorough approach provides the best opportunity for achieving optimal outcomes in prosthetic valve selection and subsequent replacement.
Acknowledgements
We would like to acknowledge Dr Daniel Matlock for his advice on the use of decision-making aids in the selection of prosthetic heart valves.
Disclosure
The authors report no conflicts of interest in this work.
References
- JonesECDevereuxRBRomanMJPrevalence and correlates of mitral regurgitation in a population-based sample (the Strong Heart study)Am J Cardiol20018729830411165964
- BachDSRadevaJIBirnbaumHGFournierAATuttleEGPrevalence, referral patterns, testing, and surgery in aortic valve disease: leaving women and elderly patients behindJ Heart Valve Dis20071636236917702360
- PibarotPDumesnilJGProsthetic heart valves: selection of the optimal prosthesis and long-term managementCirculation20091191034104819237674
- VongpatanasinWHillisLDLangeRAMedical progress prosthetic heart valvesN Engl J Med19963354074168676934
- MastersRGHelouJPipeALKeonWJComparative clinical outcomes with St. Jude Medical, Medtronic Hall and CarboMedics mechanical heart valvesJ Heart Valve Dis20011040340911380109
- VongpatanasinWHillisLDLangeRAProsthetic heart valvesN Engl J Med19963354074168676934
- YacoubMRasmiNRHSundtTMFourteen-year experience with homovital homografts for aortic valve replacementJ Thorac Cardiovasc Surg199560110186
- O’BrienMFStaffordEGGardnerMAAllograft aortic valve replacement: long-term follow-upAnn Thorac Surg199560S657646213
- HammermeisterKESethiGKHendersonWGA comparison of outcomes in men 11 years after heart-valve replacement with a mechanical valve or bioprosthesis. Veterans Affairs Cooperative Study on Valvular Heart DiseaseN Engl J Med1993328128912968469251
- PuvimanasingheJPASteyerbergEWTakkenbergJJMEijkemansEJvan HerwerdenLAPrognosis after aortic valve replacement with a bioprosthesis: predictions based on meta-analysis and microsimulationCirculation20011031535154111257081
- HammermeisterKSethiGKHendersonWGOprianCRahimtoolaSHOutcomes 15 years after valve replacement with a mechanical versus a bioprosthetic valve: final report of the Veterans Affairs randomized trialJ Am Coll Cardiol2000361152115811028464
- OxenhamHBloomfieldPWheatleyDJTwenty year comparison of a Bjork-Shiley mechanical heart valve with porcine bioprosthesesHeart20038971572112807838
- RahimtoolaSHChoice of prosthetic heart valve for adult patientsJ Am Coll Cardiol20034189390412651032
- Van GeldorpMJamiesonEKappeteinAPPatient outcome after aortic valve replacement with a mechanical or biological prosthesis: weighing lifetime anticoagulant-related event risk against reoperation riskJ Thorac Cardiovasc Surg200913788188619327512
- RahimtoolaSHChoice of prosthetic heart valve in adults: an updateJ Am Coll Cardiol2010552413242620510209
- The Stroke Prevention in Atrial Fibrillation InvestigatorsBleeding during antithrombotic therapy in patients with atrial fibrillationArch Intern Med19961564094168607726
- ByethRQuinnLLandefeldCProspective evaluation of an index for predicting the risk of major bleeding in outpatients treated with warfarinAm J Med199810591999727814
- FihnSCallahanCMartinDMcDonellMHenikoffJWhiteRThe risk for and severity of bleeding complications in elderly patients treated with warfarinAnn Intern Med19961249709798624064
- LandefeldCGoldmanLMajor bleeding in outpatients treated with warfarin: incidence and prediction by factors known at the start of outpatient therapyAm J Med1989871441522787958
- LandefeldCBeythRAnticoagulant-related bleeding. Clinical epidemiology, prediction, and preventionAm J Med1993953153288368229
- LaunbjergJEgebladHHeafJNielsenNFuglehomALadefogedKBleeding complications to oral anticoagulant therapy: multivariate analysis of 1010 treatment years in 551outpatientsJ Intern Med19912293513552026988
- PalaretiGLealiNCoccheriSBleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative studyLancet19963484234288709780
- PalaretiGManottiCD’AngeloAThrombotic events during oral anticoagulant treatment: results of the inception cohort, prospective, collaborative ISCOAT studyThromb Haemost199778143814439423791
- SteffensenFKristensenKEjlersenEDahlerupJSorensenHMajor haemorrhagic complications during oral anticoagulant therapy in a Danish population-based cohortJ Intern Med19972424975039437411
- Van der MeerFRosendaalFVandenbrouckeJBrietEAssessment of a bleeding risk index in two cohorts of patients treated with oral anticoagulantsThromb Haesmost1996761216
- BirkmeyerNJBirkmeyerJDTostesonANProsthetic valve type for patients undergoing aortic valve replacement: a decision analysisAnn Thorac Surg2000701946195211156100
- De VincentiisCKunklABTrimarchiSAortic valve replacement in octogenarians: is biologic valve the unique solutionAnn Thorac Surg2008851296130118355513
- HungLRahimtoolaSHProsthetic heart valves and pregnancyCirculation20031071240124612628941
- BonowROCarabelloBAKanuCACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 Guidelines for the Management of Patients With Valvular Heart Disease): developed in collaboration with the Society of Cardiovascular Anesthesiologists: endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic SurgeonsCirculation200681114e84e23116880336
- VahanianABaumgartnerHBaxJGuidelines on the management of valvular heart disease: The Task Force on the Management of Valvular Heart Disease of the European Society of CardiologyEur Heart J20072823026817259184
- ChanVJamiesonWRGermannEPerformance of bioprostheses and mechanical prostheses assessed by composites of valve-related complications to 15 years after aortic valve replacementJ Thorac Cardiovasc Surg20061311267127316733156
- KappeteinAPTakkenbergJPuvimanasingheJJamiesonWREijkemansMBogersADoes the type of biological valve affect patient outcomeInteract Cardiovasc Thorac Surg2006539840217670601
- KulikAMastersRGBédardPPostoperative lipid-lowering therapy and bioprosthesis structural valve deterioration: justification for a randomised trialEur J Cardiothorac Surg20103713914419674916
- CarpentierAHemodynamic factors affecting the fate of valvular bioprosthesisCirculation20101212083208420439782
- KvidalPBergstromRHorteLGStableEObserved and relative survival after aortic valve replacementJ Am Coll Cardiol20003574775610716479
- PuvimanasingheJPATakkenbergJJMEdwardsMComparison of outcomes after aortic valve replacement with a mechanical valve or a bioprosthesis using microsimulationHeart2004901172117815367517
- GrunkemeierGJamiesonWMillerDStarrAActuarial versus actual risk of porcine structural valve deteriorationJ Thorac Cardiovasc Surg19941087097187934107
- WhelanTLevineMWillanAEffect of a decision aid on knowledge and treatment decision making for breast cancer surgery: a randomized trialJAMA200429243544115280341
- TakkenbergJJMPuvimanasingheJPAvan HerwerdenLADecision-making in aortic valve replacement: bileaflet mechanical valves versus stented bioprosthesesNeth Heart J200311510
- CherDMiyamotoJLenertLIncorporating risk attitude into Markov-process decision models: importance for individual decision makingMed Decis Making1997173403509219195
- BorrisLCRivaroxaban and dabigatran etexilate: two new oral anticoagulants for extended postoperative prevention of venous thromboembolism after elective total hip arthroplastyArch Orthop Trauma Surg201013058358919565250