
Abstract
Objective
Dietary habits are an important etiological factor in the development of dental caries. Several tools, such as 24-h dietary recall (retrospective) and diet-diaries (prospective), have been recommended for dietary assessment in dental practice. Diet-diaries are commonly advocated as a tool for oral health education; however, low adherence is found to be a recognized downside of their use in dental settings, as well as nutritional research more widely. However, the reasons for poor adherence to diet-diaries remain unclear. This study aimed to explore the reasons for poor adherence to diet-diaries issued to children in a dental hospital setting.
Methods
A qualitative collective case study design was employed to explore the use of diet-diaries as a health education tool. Twenty-eight data sources across 11 appointments included: observation of dentist–patient interactions, semi-structured interviews with child–parent dyads and dentists, in addition to documentary analysis of returned diet-diaries (this included 11 observations of dentist–patient interactions, 14 interviews with the child/parent dyads and dentists, and documentary analysis of three completed diet-diaries). Data from these multiple sources were integrated in a thematic analysis to identify themes and sub-themes.
Results
Two overarching themes were identified: 1) the diet-diary is perceived as a test which carries a potential for embarrassment and blame, which in turn generates defensive behavior from parents; and 2) parents’ values, priorities, and circumstances affect the level of commitment to completing a diet-diary.
Conclusion
Low adherence to diet-diary completion in clinical dentistry results from interacting factors related to the diet-diary itself, the patient, and the clinician. This study identifies a need for a more appropriate tool for dietary assessment that is patient-centered and compatible with modern lifestyles.
Supplementary materials
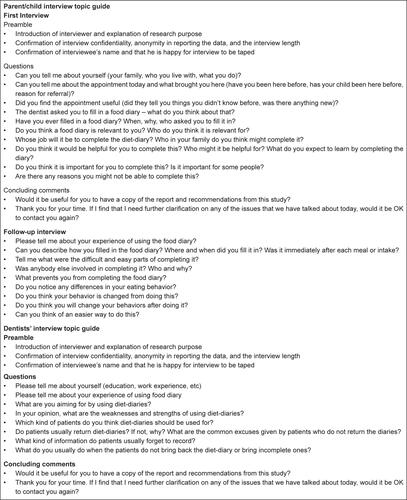
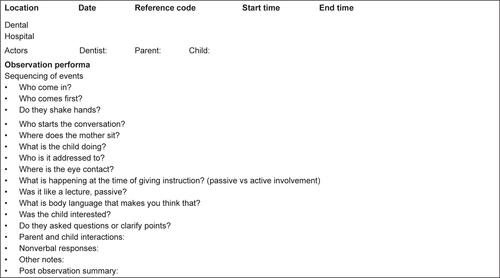
Figure S1 Topic guide for interviews and observation performa.
Acknowledgments
The authors wish to thank all study participants.
Author contributions
All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.