
Abstract
Background
Patients with heart failure (HF) can suffer from increased thirst intensity and distress. Trajectories of thirst intensity and distress from hospital to home are unclear. The aim of this study was to describe thirst intensity and distress trajectories in patients from the time of hospital admission to 4 weeks after discharge, and describe trajectories of thirst intensity and distress by patients’ characteristics (gender, age, body mass index [BMI], plasma urea, anxiety, and depression).
Patients and methods
In this observational study, data were collected from patients with HF (n=30) at hospital admission, discharge, and at 2 and 4 weeks after discharge. Thirst intensity (visual analog scale, 100 mm) and distress (Thirst Distress Scale-HF, score 9–45) were used. Trajectories were examined using growth modeling.
Results
Trajectory of the thirst intensity was significantly different, for patients with low and high thirst intensity levels (median cut-off 39 mm), from admission to 4 weeks follow up (thirst increased and decreased, respectively). Patients with high level of thirst distress (median score >22) at admission, having fluid restriction and women continued to have higher thirst distress over time. Patients feeling depressed had higher thirst intensity over time. There were no differences in the trajectories of thirst intensity and distress by age, BMI, plasma urea, and anxiety.
Conclusion
Intensity and distress of thirst, having fluid restriction, and feeling depressed at the admission were critical in predicting the trajectory of thirst intensity and distress after discharge to home in patients with HF. Effective intervention relieving thirst should be provided before their discharge to home.
Introduction
Thirst can be a troublesome symptom in patients with heart failure (HF).Citation1–Citation9 Nineteen percent of HF patients have persistent thirst.Citation8 Patients with HF are most likely to have thirst that comes and goes, but once thirst occurs, there is a risk that it will emerge again at a later time.Citation8 Thirst is the subjective sensation of a desire to drink water that cannot be ignored, and it can be measured as intensity and distress.Citation1,Citation10 Thirst intensity is defined as the severity or the strength of thirst, and thirst distress is the degree to which the patient is bothered by thirst or its associated discomfort.Citation1,Citation11 Given thê26 million patients with HF worldwide,Citation12 thirst can be seen as an important health issue that can adversely affect patients’ quality of life.Citation1,Citation2,Citation13,Citation14
Research shows that having a fluid restriction, higher body mass index (BMI), higher plasma urea, being younger and feeling anxiety, and depressive symptoms are associated with increased thirst in patients with HF.Citation1,Citation8,Citation9,Citation13–Citation16 In a previous cross-sectional study, it was found that very intensive thirst was experienced in patients with worsening HF admitted to an emergency hospital.Citation7 However, there is limited knowledge about whether thirst experience changes from admission to after hospital discharge, and whether their thirst experience is associated with patient characteristics. Therefore, the aim of this study was to describe trajectories of thirst intensity and distress in patients with HF, from the time of hospital admission to 4 weeks after discharge. The specific objectives were as follows: (a) examine whether trajectories of thirst intensity and distress differ between patients who experienced high and low levels of thirst intensity and distress at the time of hospital admission, and (b) examine whether trajectories of thirst intensity and distress are different by patients’ characteristic factors, such as gender, fluid restriction, age, BMI, plasma urea, anxiety, and depression. These potential demographic, clinical, and psychological factors were selected based on previous studies that reported significant associations with thirst experience.Citation1,Citation8,Citation9,Citation13–Citation16
Methods
A prospective observational study was conducted between January 2012 and August 2014. The Regional Ethics Committee Stockholm approved the study (2011/232-31/1), and all patients provided written informed consent before participation. The study complied with the Declaration of Helsinki.
Sample and setting
Patients >60 years of age who were admitted to the hospital due to worsening HF, with a left ventricular ejection fraction (LVEF) of ≤50%, were included. Patients were excluded if they had either of the following conditions or other diseases that carry a risk of increased thirst (eg, pulmonary disease with oxygen treatment and insulin-treated diabetes). They were also excluded if they had difficulty understanding or reading the Swedish language, a hospital stay <24 hours, or patients who could not communicate due to severe HF and thus, could not answer any questions. The study was performed at the Department of Internal Medicine at a midsized hospital in Sweden.
Procedure
A research nurse recruited patients from the Department of Internal Medicine during the daytime, within 24 hours after admission to the hospital. Data were collected at the time of hospital admission, at the time of hospital discharge, and 2 and 4 weeks after discharge to the patients’ home, by the research nurse. The time point of data collection at admission was included based on previous results about increased thirst in patients with HF at hospital admission.Citation7 Participants completed questionnaires, including thirst intensity and distress, feelings of anxiety and depression, and demographics. The research nurse collected clinical characteristics by medical chart review. Patients were also asked to provide blood samples immediately after responding to the questionnaires.
Measurements
A visual analog scale (VAS) was used to assess the sensation of thirst intensity at the moment of questioning. This scale has been previously validated and used to assess thirst intensity in patients with HF.Citation7–Citation9,Citation14–Citation17 The patients were asked to place a cross-mark on a line (100 mm) to grade their thirst intensity from none (0 mm) on the left side, to the worst possible level (100 mm) on the right side.
The Thirst Distress Scale for patients with HF (total score 9–45) was used to measure the thirst distress perceived by the patients during the preceding 3 days.Citation18 This scale consists of 9 items, rated from 1 (strongly disagree) to 5 (strongly agree). The scale is a valid and reliable tool for evaluating thirst distress in patients with HF.Citation9,Citation18,Citation19 In this study, the Cronbach’s α was 0.85.
In this study, patient factors associated with thirst included gender, age, fluid restriction, BMI, plasma urea, anxiety, and depression. Data on age and gender were collected using a structured sociodemographic questionnaire. Information about prescribed fluid restriction was collected by asking the patients whether or not they restricted their fluids, and the volume of the prescribed restriction was recorded. BMI was calculated by weight (kg)/length (m2). Blood samples were analyzed for plasma urea (coefficient of variation 6%; DXC800, Beckman-Coulter, Brea, CA, USA) at the Study Center, Karolinska University Laboratory, Stockholm, Sweden. We also collected the symptom severity of HF, the New York Heart Association (NYHA) functional classification, the LVEF, plasma N-terminal prohormone brain natriuretic peptide (NT-proBNP, ng/L), plasma creatinine (μmol/L), serum osmolality (mosmol/kg), and duration of hospitalization to describe patients’ characteristics.
We assessed being anxious (experiencing worry or nervousness) and depressed (a state of unhappiness or despondence) using a 5-point Likert scale (1= strongly disagree to 5= strongly agree) in past 3 days. Although many standardized instruments for assessing anxiety and depression are available, most instruments assess experience of such psychological distress in past 2 weeks to 4 weeks that may be not sensitive to capture the association with their thirst experience in past 3 days in this study. We assessed face validity of the 2 questions of being anxious and being depressed in patients with HF before we used the items in this study. Internal consistency of the items was satisfactory (Cronbach’s α 0.79). In this study, patients who scored ≥3 on a 5-point Likert scale were considered to be experiencing moderate-to-severe anxiety or depression.
Data analysis
Descriptive statistics (mean [SD], median [interquartile range, IQR], or frequency [%]) were used to describe the study samples’ demographic and clinical characteristics. Before we conducted growth modeling analysis, we dichotomized patients into low and high thirst intensity groups at the time of admission using the median VAS of 39 mm as a cutpoint. Patients with a score of ≤39 were the low thirst intensity group, and >39 were the high thirst intensity group. Patients were also dichotomized into low and high thirst distress groups by using the median score of 22 from the Thirst Distress Scale at admission.
We grouped patients into 2 groups at hospital admission based on patient factors using mean (SD) or median (IQR) based on their distribution. For example, patients were grouped into young and old age groups, and high and low BMI groups using mean values of age (81±7 years) and BMI (26±6 kg/m2), and high and low plasma urea groups using median (IQR) value (9, 8–12 mmol/L). Patients were categorized into being anxious and depressed using the score ≥3, and into absence or presence of fluid restriction groups using their self-report.
For this study, we were interested in evaluating thirst intensity and distress during hospitalization and after discharge to home. Growth modeling was used to identify trajectories of thirst intensity and distress over time.Citation20,Citation21 Growth modeling is a way of analyzing repeated-measures data that have a hierarchical structure in regression.Citation20 The advantages with growth modeling are that it measures growth throughout, not just at the end of the study, and provides intercept and estimate to calculate the rate of growth.Citation20–Citation22 The intercept is thirst (intensity or distress) of each participant at the initial point, which was the admission time in this study, and the estimate (ie, unstandardized B) indicates slope. If the P-value of interaction between time and group is <0.05, it indicates a significant trajectory of thirst intensity and distress between 2 groups over time (ie, from admission to 4 weeks after discharge). Estimates with 95% CIs were calculated for each growth model. A P-value of <0.05 was considered significant. All data were analyzed with the Statistical Package for Social Sciences version 22 (SPSS, Chicago, IL, USA).
Results
Sample characteristics
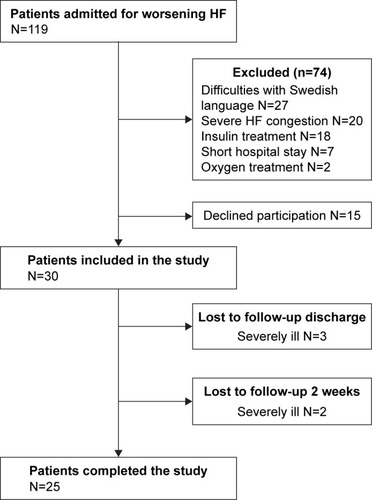
Of the 119 patients with worsening HF who were screened at the time of hospital admission, the majority were excluded because of difficulty with the Swedish language (n=27) or due to severe HF congestion (n=20). Another 27 patients were excluded due to other exclusion criteria (). Fifteen patients declined to participate. A total of 30 patients were included in this study and 3 were lost to follow-up due to severe illness at discharge, while 2 were lost after 2 weeks of follow-up (). Patients who were lost to follow-up (n=5, 2 men and 3 women) had lower LVEF (mean 23%), longer hospital stay (median [IQR], days 8 [3–17]), and higher median NT-proBNP (11,000 [5,365–21,300] ng/L) than patients who completed the study. Their mean age (years 79±8), median thirst intensity (VAS 43 [8–65] mm), and thirst distress (scores 22 [17–42]) were similar to those who completed the study.
Figure 1 Flowchart of patients in the study.
At admission to hospital, the included patients (n=30) had a mean (SD) age of 81 (7) years, and 14 (47%) were women (). The mean LVEF of the patients was 37% (12%). All patients were prescribed diuretics (dose 30–250 mg/day/patient; mean dose 77 mg/day) and 23 (77%) were prescribed beta blockers. Most patients (n=28, 93%) were NYHA functional class III at the time of admission, and 2 (7%) were class IV. At the admission, 12 patients (40%) reported being depressed and 15 (50%) reported being anxious. Nine (30%) patients were on fluid restriction (). The median thirst intensity was 39 (14–59) mm and thirst distress scores 22 (17–28) ().
Table 1 Characteristics of the study sample at time of hospital admission
Table 2 Thirst intensity and distress from hospital admission to 4 weeks follow-up after hospital discharge in patients with heart failure
Trajectories of thirst intensity and distress by the high and low intensity and distress groups
The mean of thirst intensity was significantly different between the high intensity and the low intensity groups at the admission (59 mm vs 16 mm, P<0.001). Trajectory of the thirst intensity was significantly different for the two groups from admission to 4-weeks follow up (Time*Group interaction =−8.9, P=0.005) (). As time passed, thirst intensity was decreased for the high intensity group, whereas thirst intensity was increased for the low intensity group ().
Figure 2 Trajectories of thirst intensity and distress in HF patients admitted to hospital with low and high thirst intensity and distress.
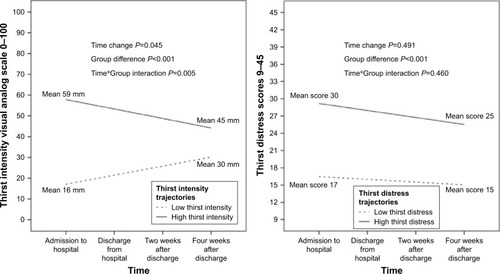
Table 3 Trajectories of thirst intensity and distress for patients with low and high levels of thirst groups at hospital admission
Although there was a mean difference between the high and low thirst distress groups at admission, the trajectory of thirst distress was not significantly different between groups over time from admission to 4 weeks after discharge. (Time*Group interaction =−0.7, P= 0.460) ().
Trajectories of thirst intensity and distress by patients’ factors
At the admission, the depressed group reported higher level of thirst intensity than those who were not depressed (, ). The trajectories of thirst intensity and distress for both groups were not significantly different from the admission to 4 weeks after discharge but the group difference in intensity and distress remained over time. Women reported significantly higher level of thirst distress than men at the admission and the group difference in thirst distress remained over time (). However, there was no difference in trajectory of thirst intensity or distress between men and women over time (). The fluid restriction group had higher level of thirst distress than the no-fluid restriction group at the admission (P=0.013) (). However, the trajectory of thirst distress was not significantly different between 2 groups. For thirst intensity, there was no group or trajectory difference.
Figure 3 Trajectories of thirst intensity and distress by the patient factors of feeling depressed, gender, and fluid restriction in HF patients.
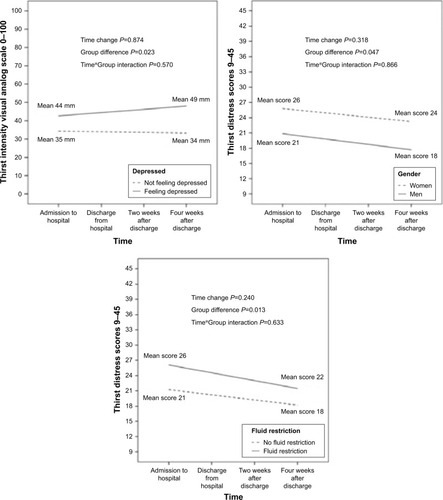
Table 4 Trajectories of thirst intensity and distress by patients’ factors
There was no group difference, time effect, or difference in the trajectory of thirst intensity and distress between the high and low anxiety groups, between the young and old age groups, between the high and low BMI groups, and between the high and low urea groups ().
Discussion
To our knowledge this is the first study examining trajectories of thirst intensity and distress in patients with HF in a longitudinal observation study from hospital admission to 4 weeks follow-up at home. First of all, we found that HF patients with initially high thirst intensity at admission to hospital decreased their thirst over time, in contrast, patients with initially low thirst intensity increased their thirst over time. We also found that patients who were admitted to the hospital with high thirst distress continued to have high thirst distress over time. Patients with fluid restriction and patients who were feeling depressed, had higher level of thirst distress over time than those who did not have fluid restriction or feeling depressed.
Thirst intensity changed over time in patients who were admitted to hospital with high and low thirst intensity levels. From a physiological view, the thirst sensation is to ensure behavior to drink water, and it is primarily regulated by the body fluid osmolality and changes in plasma volume.Citation23 Patients who do not drink enough, for example, if they have fluid restriction, may be dehydrated and therefore, experience higher thirst intensity. The different changes of thirst intensity as seen in patients in the 2 groups in this study, may be related to different body hydration states from hospital admission to 4 weeks after discharge. Diuretics are also one possible cause for increased thirst.Citation1 Tolvaptan, a selective vasopressin V2 receptor blocker antagonist,Citation1 has been reported to increase thirst in patients with HF, but none of the patients in our study were prescribed this drug. All patients in this study were prescribed diuretics with different doses at admission and for the majority, the dose remained the same during the follow-up. Similar thirst intensity changes, as in our study, were seen in a study in hospitalized decompensated HF patients who were followed up 1 month after hospital discharge in a randomized controlled study investigating the effects of fluid restriction.Citation16 The results of our study could also be explained by the regression to the mean.
Patients who reported high thirst distress on admission to the hospital continued to have high thirst distress over time in this study. This confirms our previous findings, in which a majority of patients with HF had temporary thirst, but the likelihood of experiencing thirst over time was dependent on whether thirst was reported at the first measurement.Citation8 Patients with persistent thirst need to be identified and might be in need of greater involvement by clinicians.Citation1,Citation2,Citation13
Having a fluid restriction was associated with higher level of thirst distress trajectory in this study. Restricting fluid in patients with HF is based on logical reasoning, to relieve congestion and HF symptoms, such as dyspnea and edema.Citation24,Citation25 However, no convincing evidence is found for the standard prescription of fluid restriction for all patients with HF.Citation26 The negative effect of fluid restriction on thirst distress is supported in a study in which patients with HF had increased thirst distress over time while having prescribed a fluid restriction, even though the patients received education and behavioral strategies to manage the restriction.Citation13 Suffering from thirst caused by fluid restriction should be seriously considered, and such a restriction should only be prescribed in patients who can truly benefit from it.Citation26 According to guidelines, fluid restriction is not recommended for all patients with HF.Citation24–Citation27 A temporary fluid restriction can be beneficial for patients with HF who have fluid overload, severe edema and/or ascites and/or with hyponatremia, in order to relieve congestion and symptoms.Citation24–Citation27 A tailored fluid restriction based on body weight (30 mL/kg per day) seems to be most reasonable and has the least effect on thirst.Citation14,Citation15,Citation26
For patients who need a fluid restriction, clinicians should help to manage thirst distress. There are no evidence-based interventions to relieve thirst distress, but in practice, concrete advice has been given, such as distributing fluid intake evenly throughout the dayCitation28 and sucking on ice cubes or peppermint.Citation5
We also found that psychological distress, such as being depressed, was associated with trajectory of thirst intensity. Patients who were feeling depressed had high thirst intensity over time, compared with those who were not feeling depressed. Antidepressant medication, which is associated with thirst,Citation29 was prescribed to only 1 patient in the present study. About 30% of all HF patients are estimated to have depressive symptoms.Citation30 Previous studies have shown that stress, measured with the stress-related biomarker cortisol, is increased in patients with high thirst.Citation9 HF patients with high thirst have also reported feeling more depressed and anxious.Citation7–Citation9 The mechanism between psychological distress and thirst can be the high level of sympathetic activity that is seen in patients with HF, as well as the stressful life situations HF patients are coping with. Patients with HF have various symptoms, which often do not occur alone. Clinicians need to follow a patient-centered approach and should consider thirst as part of the patient’s overall troublesome symptoms.
Finally, we found that women had a higher level of thirst distress over time than men. This is not consistent with a previous finding, in which men had been identified to have a higher potential risk for persistent thirst.Citation8 In healthy persons, no difference has been reported in thirst between men and women.Citation31 However, previous research has shown that women tend to have more symptoms related to HF, and they experience higher distress levels of fatigue, anxiety, and feeling depressed, compared with men.Citation32–Citation36
The strength of this study was the use of growth modeling, as it has advantages over the more traditional data analytic approach with repeated-measures ANOVA; for example, missing data values do not cause a given subject to be dropped.Citation20,Citation22,Citation37 Moreover, the linear mixed analysis has sufficient power to detect group differences in a moderate or small sample size.Citation37 Other strengths of this study are that it includes longitudinal data collected at 4 time points. This study has several limitations. We assessed patients feeling depressed and anxious using a 2-item question, not standardized or valid questionnaires that may capture a more comprehensive phenomenon of depression or anxiety. Thus, the findings should be generalized with caution and should not be interpreted as clinical depression or anxiety. Another limitation in the study is that we did not collect individual information of the patients’ habitual drinking behaviors. In fact, if all individuals have habitual drinking behavior from admission to 4 weeks after discharge, our study finding may be more significant because having habitual drinking behavior may minimize changes of drinking amounts within subject (individuals) over time. Due to a small sample size of this study, there is limited generalizability in the HF population.
Implications for practice at hospital admission, nurses are recommended to: (a) screen for and identify patients with HF with increased thirst intensity and distress, with fluid restriction, and feeling depressed. Although women were more likely to have increased thirst in this study, both men and women should be asked about thirst. Before patient’s discharge: (b) educate patients about thirst, what can cause thirst, how to monitor thirst, and give solutions how to relieve thirst (eg, sucking ice cubes), (c) evaluate the usefulness of a fluid restriction with a cardiologist, (d) consult a cardiologist if the patient feels depressed, and (e) schedule a follow-up visit for patients with troublesome thirst to an outpatient HF clinic. A randomized controlled trial is needed to test if an educational program for nurses, using the recommendations, is effective to decrease thirst intensity and distress in patients with HF.
Conclusion
Levels of thirst intensity and distress (high and low) in patients with HF at the admission were critical in predicting the trajectory of thirst intensity and distress after discharge to their home. Being depressed, having fluid restriction and gender were also associated with trajectories of thirst intensity or distress. Engaging clinicians in regular thirst-monitoring is the first step to recognizing increased thirst intensity and distress and prompting the process toward management strategies to alleviate thirst in HF patients.
Acknowledgments
The authors are grateful to the patients who participated in this study. They also acknowledge Pia Jonsson for her help with data collection, and the cardiologists at the Department of Internal Medicine for performing the echocardiography.
Disclosure
The authors report no conflicts of interest in this work.
References
- WaldréusNHahnRGJaarsmaTThirst in heart failure: a systematic literature reviewEur J Heart Fail201315214114923180606
- ReillyCMMeadowsKDunbarSCullerSSmithAThirst and QOL in persons with heart failureHeart & Lung: The Journal of Acute and Critical Care2010394353
- NordgrenLSörensenSSymptoms experienced in the last six months of life in patients with end-stage heart failureEur J Cardiovasc Nurs20032321321714622629
- BrännströmMEkmanINorbergABomanKStrandbergGLiving with severe chronic heart failure in palliative advanced home careEur J Cardiovasc Nurs20065429530216546447
- van der WalMHJaarsmaTMoserDKvan GilstWHvan VeldhuisenDJQualitative examination of compliance in heart failure patients in The NetherlandsHeart Lung201039212113020207272
- FalkSWahnAKLidellEKeeping the maintenance of daily life in spite of chronic heart failure. A qualitative studyEur J Cardiovasc Nurs20076319219917141572
- WaldréusNSjöstrandFHahnRGThirst in the elderly with and without heart failureArch Gerontol Geriatr201153217417821035203
- WaldréusNvan der WalMHHahnRGvan VeldhuisenDJJaarsmaTThirst trajectory and factors associated with persistent thirst in patients with heart failureJ Card Fail201420968969524951934
- WaldréusNHahnRGLyngåPvan der WalMHHägglundEJaarsmaTChanges in Thirst Intensity During Optimization of Heart Failure Medical Therapy by Nurses at the Outpatient ClinicJ Cardiovasc Nurs2016315E17E2426696035
- TotoKHRegulation of plasma osmolality: thirst and vasopressinCrit Care Nurs Clin North Am1994646616747766344
- WelchJLDevelopment of the thirst distress scaleNephrol Nurs J200229433734212224366
- AmbrosyAPFonarowGCButlerJThe global health and economic burden of hospitalizations for heart failure: lessons learned from hospitalized heart failure registriesJ Am Coll Cardiol201463121123113324491689
- ReillyCMHigginsMSmithACullerSDDunbarSBIsolating the benefits of fluid restriction in patients with heart failure: A pilot studyEur J Cardiovasc Nurs201514649550524990176
- HolstMStrömbergALindholmMWillenheimerRLiberal versus restricted fluid prescription in stabilised patients with chronic heart failure: result of a randomised cross-over study of the effects on health-related quality of life, physical capacity, thirst and morbidityScand Cardiovasc J200842531632218609051
- HolstMStrömbergALindholmMWillenheimerRDescription of self-reported fluid intake and its effects on body weight, symptoms, quality of life and physical capacity in patients with stable chronic heart failureJ Clin Nurs200817172318232618705707
- AlitiGBRabeloERClausellNRohdeLEBioloABeck-da-SilvaLAggressive fluid and sodium restriction in acute decompensated heart failure: a randomized clinical trialJAMA Intern Med2013173121058106423689381
- HolstMStrömbergALindholmMUdenGWillenheimerRFluid restriction in heart failure patients: is it useful? The design of a prospective, randomised studyEur J Cardiovasc Nurs20032323724214622632
- JaarsmaTWaldréusNvan der WalMKato PerkiöNMeasuring thirst in patients with heart failure: The Thirst Distress Scale for patients with HF is ready to useCirculation2016134Suppl 1A16876
- WaldréusNJaarsmaTvan der WalMHKato PerkiöNDevelopment and psychometric evaluation of the Thirst Distress Scale for patients with heart failureEur J Cardiovasc Nurs201817322623428838260
- HesserHModeling individual differences in randomized experiments using growth models: Recommendations for design, statistical analysis and reporting of results of internet interventionsInternet Interv201522110120
- FieldAPDiscovering statistics using IBM SPSS statistics4thLondonSage publications2013
- EndersCKTofighiDCentering predictor variables in cross-sectional multilevel models: a new look at an old issuePsychol Methods200712212113817563168
- ThorntonSNThirst and hydration: physiology and consequences of dysfunctionPhysiol Behav20101001152120211637
- PonikowskiPVoorsAAAnkerSDESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESCEur J Heart Fail201618889197527207191
- YancyCWJessupMBozkurtB2013 ACCF/AHA Guideline for the Management of Heart Failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice GuidelinesJ Am Coll Cardiol20136216e147e23923747642
- JohanssonPvan der WalMHStrömbergAWaldréusNJaarsmaTFluid restriction in patients with heart failure: how should we think?Eur J Cardiovasc Nurs201615530130427169459
- LainscakMBlueLClarkALSelf-care management of heart failure: practical recommendations from the Patient Care Committee of the Heart Failure Association of the European Society of CardiologyEur J Heart Fail201113211512621148593
- PhilipsonHEkmanIForslundHBSwedbergKSchaufelbergerMSalt and fluid restriction is effective in patients with chronic heart failureEur J Heart Fail201315111304131023787719
- GuptaAEpsteinJBSroussiHHyposalivation in elderly patientsJ Can Dent Assoc200672984184617109806
- HareDLToukhsatiSRJohanssonPJaarsmaTDepression and cardiovascular disease: a clinical reviewEur Heart J201435211365137224282187
- ArmstrongLEJohnsonECMckenzieALEllisLAWilliamsonKHEndurance Cyclist Fluid Intake, Hydration Status, Thirst, and Thermal Sensations: Gender DifferencesInt J Sport Nutr Exerc Metab201626216116726479401
- LeeKSSongEKLennieTASymptom clusters in men and women with heart failure and their impact on cardiac event-free survivalJ Cardiovasc Nurs201025426327220539161
- BarnesSGottMPayneSPrevalence of symptoms in a community-based sample of heart failure patientsJ Pain Symptom Manage200632320821616939845
- GottliebSSKhattaMFriedmannEThe influence of age, gender, and race on the prevalence of depression in heart failure patientsJ Am Coll Cardiol20044391542154915120809
- EkmanIEhrenbergAFatigue in chronic heart failure – does gender make a difference?Eur J Cardiovasc Nurs200211778214622871
- HägglundLBomanKOlofssonMBrulinCFatigue and health-related quality of life in elderly patients with and without heart failure in primary healthcareEur J Cardiovasc Nurs20076320821517092775
- FanXPower of Latent Growth Modeling for Detecting Group Differences in Linear Growth Trajectory ParametersStructural Equation Modeling: A Multidisciplinary Journal2003103380400