Abstract
Background: Approximately 60% of the patients with type 2 diabetes mellitus (T2DM) on basal insulin have an HbA1c ≥7%. This analysis of the US Perceptions of Control (POC-US) study aimed to understand US patient and health care professional (HCP) views of diabetes “control,” which may play a role in whether patients reduce their HbA1c or achieve HbA1c <7%.
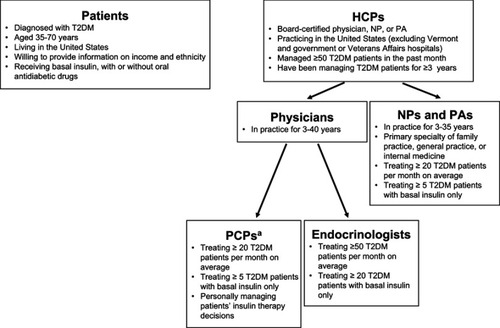
Methods: A cross-sectional, Web-based survey of 500 US HCPs (primary care physicians, endocrinologists, nurse practitioners/physician assistants) and 618 US adults with T2DM using basal insulin was conducted to assess perceptions, attitudes, and behaviors associated with T2DM management. The survey was developed from previous research examples and qualitative exploratory research and was pretested. Patients self-reported their most recent HbA1c level and confirmed this value with their HCP, if necessary.
Results: Patients and HCPs differed on some definitions of “in control.” HbA1c value was used most often by both populations, but more frequently by HCPs (91% vs 69%). Patients also often used behavioral criteria (eg, adherence to lifestyle changes and/or treatment regimens), and HCPs often used clinical criteria (eg, hypoglycemia). Most HCPs focused on the last 3 months to define control (67% vs 34% patients; P<0.05), whereas patients more frequently reported focusing on “the current moment” or “the past week.” Patients were more likely to agree that controlling their condition is “completely the patients’ responsibility” (patients, 67%; HCPs, 34%; P<0.05); HCPs were more likely to agree that they have “a responsibility to actively contribute to the control of their patients’ T2DM” (90% vs 60%; P<0.05).
Conclusion: US patients with T2DM have differing views from HCPs on key aspects of diabetes control and management and are less likely to consider HbA1c value as a criterion for determining control. Recognizing and addressing these differences may improve patient-HCP communication and may potentially improve patient outcomes.
Acknowledgments
Writing assistance was provided by Jessica Monteith, PhD, of ETHOS Health Communications in Yardley, PA, USA, and was supported financially by Novo Nordisk Inc., Plainsboro, NJ, USA, in compliance with international Good Publication Practice guidelines. An abstract of this study was presented at the American Diabetes Association’s 78th Scientific Sessions as a poster presentation and is available at https://ada.scientificposters.com/epsAbstractADA.cfm?id=1. This research was sponsored by Novo Nordisk Inc.
Disclosure
KJ Tomaszewski is an employee of KJT Group, which provides paid research services to Novo Nordisk. A Allen is an employee of KJT Group, which provides paid research services to Novo Nordisk. M Mocarski is an employee of Novo Nordisk Inc. and a stockholder of Novo Nordisk A/S. A Schiffman is an employee of Novo Nordisk Inc. and a stockholder of Novo Nordisk A/S. D Kruger is a consultant and speaker for Novo Nordisk, and her institution receives research funding from Novo Nordisk. Y Handelsman has received research grants and consultant and speaker honoraria from Aegerion, Amarin, Amgen, AstraZeneca, Bristol-Myers Squibb, Boehringer Ingelheim, Boehringer Ingelheim-Lilly, Gan & Lee Pharmaceutical, Gilead, Hanmi, Janssen, Lexicon, Lilly, Merck, Merck-Pfizer, Mylan, Novo Nordisk, Regeneron, and Sanofi. M Heile is an advisor for Bigfoot Biomedical Company, Janssen Pharmaceutical, Novo Nordisk, and Roche Diagnostics and a speaker for Insulet Corporation, Janssen Pharmaceutical, and Novo Nordisk. M Brod is a paid consultant for Novo Nordisk. A Allen reports professional fees for design and execution of supporting research from Novo Nordisk, during the conduct of the study. D Kruger reports grants and personal fees from Novo Nordisk, outside the submitted work. Y Handelsman reports grants and personal fees from Amgen, AstraZeneca, Merck, Janssen, Novo Nordisk, and Sanofi; and grants from BMS, BI, Gan & Lee, Hamni, Lexicon, and Mylan, personal fees from Aegerion, Amarin, Gilead, Intarcia, and Regeneron, outside the submitted work. M Heile served as an advisor and member of the speakers bureau for Novo Nordisk, outside the submitted work. The authors report no other conflicts of interest in this work.
Supplementary material