Abstract
Purpose
Social anxiety disorder (SAD) is a disabling condition that affects almost 5% of the general population. Many types of drugs have shown their efficacy in the treatment of SAD. There are also some data regarding psychotherapies, but no data are available today about the efficacy of brain stimulation techniques. The aim of the study is to compare the efficacy of noninvasive brain stimulation neuro psycho physical optimization (NPPO) protocol performed by radio electric asymmetric conveyor (REAC) with that of sertraline in adults with SAD.
Patients and methods
Twenty SAD patients on sertraline were compared with 23 SAD patients who refused any drug treatment and who chose to be treated with NPPO-REAC brain stimulation. This was a 6-month, open-label, naturalistic study. Patients on sertraline received flexible doses, whereas NPPO-REAC patients received two 18-session cycles of treatment. Clinical Global Improvement scale items “much improved” or “very much improved” and Liebowitz Social Anxiety Scale total score variation on fear and avoidance components were used to detect the results. The statistical analysis was performed with t-test. All measures <0.05 have been considered statistically significant.
Results
Ten of 23 subjects on NPPO-REAC and six of the 20 taking sertraline were much improved or very much improved 1 month after the first NPPO-REAC cycle (t1). Sixteen of the subjects on NPPO-REAC and ten of the subjects taking sertraline were much improved or very much improved 1 month after the second NPPO-REAC cycle (t2). In respect of the Liebowitz Social Anxiety Scale, at t1 NPPO-REAC resulted in statistically more efficacy for sertraline on both fear and avoidance total scores. At t2, NPPO-REAC resulted in statistically more efficacy for sertraline on fear but not on avoidance.
Conclusion
NPPO-REAC is an effective treatment for SAD, allowing substantial and clinically meaningful reductions in symptoms and disability in comparison with sertraline.
Introduction
Social anxiety disorder (SAD), also known as social phobia, is characterized by the marked fear of being observed or evaluated by others,Citation1–Citation3 in particular nonrelatives. In such situations, patients with SAD fear that they will say or do something to embarrass or humiliate themselves or that others will notice that they are anxious. Consequently, subjects with SAD often avoid situationsCitation2,Citation4,Citation5 where such scrutiny might take place, or they endure them with intense distress.Citation6 This can result in impaired functioning and disrupted quality of life.Citation7,Citation8 Patients affected from SAD may have few social relationships, experience trouble dating, drop out of schoolCitation9,Citation10 or work,Citation11 reject promotions at work, become demoralized, abuse alcohol,Citation12–Citation16 and develop other psychiatric disordersCitation17–Citation19 like major depression.Citation20–Citation22 SAD is more frequent in the primary care setting,Citation23–Citation27 but it is often undiagnosedCitation28 and, consequently, untreated. This low rate of recognition and appropriate treatment reflects the fact that social phobia remains a largely neglected anxiety disorder.Citation29.Citation30 However, the available epidemiological studiesCitation31–Citation33 show a prevalence of at least 5% in the general population.
Most clinicians associate the term “social phobia” with a fear of public speaking. Indeed, social phobia often involves public speaking and, in some cases, does so exclusively. However, there is a variant of SAD that is more pervasive and usually more disabling: generalized SADCitation7, Citation34–Citation37 (gSAD). Subjects with gSAD typically fear and avoid a broad array of situations that most people take for granted, such as speaking in small groups, attending social gatherings, talking to people in authority, and interacting with peers in an informal setting.
The neglect of gSAD obviously extends into the area of treatment. Treatment options for gSAD include monoamine oxidase inhibitors,Citation38 reversible inhibitors of monoamine oxidase A (moclobemide),Citation39,Citation40 and, in particular, selective serotonin reuptake inhibitors.Citation41–Citation43 Based on their success in the treatment of many mood and other anxiety disorders, selective serotonin reuptake inhibitors have been investigated in the treatment of social phobia, and they are considered as first-choice drugs for the treatment of gSAD. Excluding some psychotherapies,Citation44–Citation47 at the moment, no data are available about other therapeutical approaches such as noninvasive brain stimulation techniques like radio electric asymmetric conveyor (REAC) treatments. Neuro psycho physical optimization (NPPO)-REAC has demonstrated efficacy in improving certain psychiatric disorders such as stress-related disorders,Citation48–Citation53 anxiety,Citation53,Citation54 depression,Citation53–Citation55 bipolar disorder,Citation56 and behavioral and psychiatric symptoms in Alzheimer disease. Citation57 The main goal of the present study was to investigate the efficacy of NPPO-REAC in the treatment of gSAD in patients who refuse drug treatment.
Materials and methods
This was an open-label, naturalistic study. Patients with gSAD came spontaneously to our medical centers and were observed in the normal clinical practice. gSAD was diagnosed with structured clinical interviewCitation58,Citation59 according to the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revised.
The data for the current study were collected from the Psychic Studies Center, Cagliari, Italy, for 20 patients () treated with flexible doses of sertralineCitation60–Citation62 (mean dose 125.0 ± 15.5 mg/day once a day) and from the Rinaldi Fontani Institute, Florence, Italy, for 23 patients () who refused drug treatment and were treated with two cycles of 18 NPPO-REAC sessions. The time between the two treatment cycles was about 3 months. None of the patients enrolled in the study had been previously treated for gSAD, and none took psychotropic drugs during the study, except for sertraline. Patients were evaluated for safety and efficacy about 1 month after the end of the first NPPO-REAC treatment cycle (t1) and about 1 month after the end of the second NPPO-REAC treatment cycle (t2). According to the Rinaldi- Fontani protocol, this time period lasted about 6 months and determined the duration of the comparison study. The main efficacy variables were the percentage of responders at t1 and t2, defined as those rated on the Clinical Global Improvement (CGI)Citation63,Citation64 scale as 1 (very much improved) or 2 (much improved), and the mean change from baseline at t1 and t2 on the Liebowitz Social Anxiety ScaleCitation65–Citation67 (LSAS) total score. The LSAS is a 24-item assessment of fear and avoidance of several public-social situations. Statistical analysis of the obtained data was performed using t-test, and P < 0.05 was considered statistically significant.
Table 1 Demographics
Radio electric asymmetric conveyer
The REACCitation68,Citation69 is a medical device that is based on an innovative technology for biostimulation and/or bioenhancement techniques. The model used in this study (Convogliatore di Radianza Modulante, ASMED, Florence, Italy) is specific for noninvasive brain stimulation techniques.
The NPPO-REAC treatment protocol consisted of seven radiofrequency bursts of 500 ms each at a frequency of 10.5 GHz and a specific absorption rate of 7 μW/kg, applied by touching the metallic tip of the REAC probe to the ear pavilion.
Results
Both treatments were well tolerated, and no patients suspended the study because of any side effects. At baseline, in both the NPPO-REAC and sertraline groups, for fear and avoidance, a marked clinical picture was detected ( and ).
Figure 1 Liebowitz Social Anxiety Scale (LSAS) score decreasing for fear.
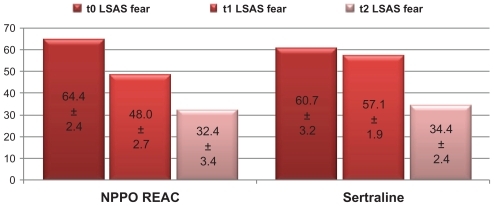
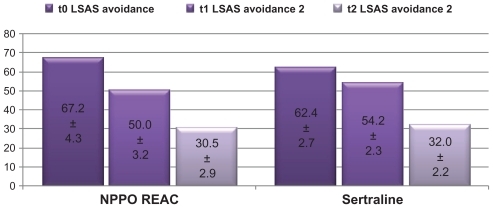
Figure 2 Liebowitz Social Anxiety Scale (LSAS) score decreasing for avoidance.
Ten (43.5%) of 23 subjects on NPPO-REAC and six (30.0%) of the 20 taking sertraline were much improved or very much improved 1 month after the first NPPO-REAC cycle (t1) (). Sixteen (69.6%) of the subjects on NPPO-REAC and ten (50.0%) of the subjects taking sertraline were much improved or very much improved 1 month after the second NPPO-REAC cycle (t2) (). The proportion of NPPO-REAC responders (ie, a CGI score of 1 or 2) was significantly greater than for sertraline ().
Table 2 Clinical Global Improvement (CGI)
At t1, for NPPO-REAC, LSAS total fear score decreased from 64.4 ± 2.4 to 48.0 ± 2.7 () and for sertraline from 60.7 ± 3.2 to 57.1 ± 1.9 (t-test t = −12.595, DF = 41, P = 0.000) (); for NPPO-REAC, LSAS total avoidance score decreased from 67.2 ± 4.3 to 50.0 ± 3.2 and for sertraline from 62.4 ± 2.7 to 54.2 ± 2.3 (t-test t = −4.873, DF = 41, P = 0.000) ().
From baseline to t1, gSAD improved from marked to moderate both for fear () and for avoidance () in the NPPO-REAC treatment group, and only for avoidance in the sertraline group.
At t2, for NPPO-REAC, LSAS total fear score decreased from 48.0 ± 2.7 to 32.4 ± 3.4 () and for sertraline from 57.1 ± 1.9 to 34.4 ± 2.4 (t-test t = −2.196, DF = 41, P < 0.05) (); for NPPO-REAC, LSAS total avoidance score decreased from 50.0 ± 3.2 to 30.5 ± 2.9 () and for sertraline from 54.2 ± 2.3 to 32.0 ± 2.2 (t-test t = −1.888, DF = 41, P = NS) ().
From baseline to t2, in both the NPPO-REAC and the sertraline groups, for fear () and avoidance (), gSAD improved from marked to subthreshold for both fear and avoidance for NPPO-REAC.
Discussion and conclusion
This is probably the first study that compares the efficacy of a brain stimulation technique with a targeted drug, sertraline, in the treatment of gSAD. The results clearly demonstrate that NPPO-REAC treatment effectively and quickly reduces the core symptoms and the avoidance associated with this disorder. In this research, NPPO-REAC was globally statistically superior to standard dosages of sertraline on selected primary efficacy criteria, CGI improvement, and LSAS total score for fear and avoidance. Considering the early age at onset and chronic course of this disorder, detecting a reduction in disability after only a 6-month follow-up is noteworthy. It is hoped, but remains to be shown in future studies, that longer duration and more cycles of NPPO-REAC treatment might result in even further structuration of results and, consequently, in the reduction of functional impairment.
As previously demonstrated in the treatment of agoraphobia, also in this study a sort of cognitive restructuration performed by NPPO-REAC has been highlighted, in order to guarantee the patient a more rational control of emotions when exposed to social and performance situations and, consequently, better management of the pattern of avoidance behaviors.
In respect of the CGI scale, the greater percentage of patients who felt themselves to be much improved or very much improved with NPPO-REAC than with sertraline highlights the deeper action of the gentle NPPO-REAC brain stimulation compared with the drug.
Another aspect of particular interest is the feeling of natural and no artificial improvement of gSAD symptomatology. This is very important, because typical of anxiety disorders, and probably one of the main reasons of the premature discontinuation of the drug treatment, is the feeling of the artificiality of the results. Therefore, from this point of view, the NPPO-REAC provides greater adherence to the treatment of these patients.
Obviously, there are a number of limitations to this study. SAD is a chronic and disabling disease that in any cases may require long-term therapy. Because of its design, this study did not accurately assess NPPO-REAC efficacy beyond the short, 6-month treatment period. It is possible, although not yet proven, that a longer course of therapy could result in sustained and even greater reductions in impairment and in improvement in quality of life.
Indeed, further studies of long-term treatment with NPPO-REAC are needed to determine the optimal duration of therapy, the number of NPPO-REAC cycles needed, and the efficacy in sustaining remission.
Because NPPO-REAC is also effective in the treatment of depressive symptoms, another limitation of this study is its inability to definitively demonstrate that reductions in social anxiety symptoms were not simply a secondary manifestation of this antidepressant effect.
Conclusion
NPPO-REAC is an effective treatment for SAD, allowing substantial and clinically meaningful reductions in symptoms and disability, in comparison with sertraline.
Disclosure
Salvatore Rinaldi and Vania Fontani are the inventors of the radio electric asymmetric conveyor.
References
- WeeksJWHeimbergRGRodebaughTLPsychometric evaluation of the fear of positive evaluation scale in patients with social anxiety disorderPsychol Assess1032011
- SchneierFRRodebaughTLBlancoCFear and avoidance of eye contact in social anxiety disorderCompr Psychiatry2011521818721220069
- ZimmermanMDalrympleKChelminskiIRecognition of irrationality of fear and the diagnosis of social anxiety disorder and specific phobia in adults: implications for criteria revision in DSM-5Depress Anxiety201027111044104920577989
- MoitraEHerbertJDFormanEMBehavioral avoidance mediates the relationship between anxiety and depressive symptoms among social anxiety disorder patientsJ Anxiety Disord20082271205121318282686
- HofmannSGBitranSSensory-processing sensitivity in social anxiety disorder: relationship to harm avoidance and diagnostic subtypesJ Anxiety Disord200721794495417241764
- KashdanTBMorinaNPriebeSPost-traumatic stress disorder, social anxiety disorder, and depression in survivors of the Kosovo War: experiential avoidance as a contributor to distress and quality of lifeJ Anxiety Disord200923218519618676121
- BarreraTLNortonPJQuality of life impairment in generalized anxiety disorder, social phobia, and panic disorderJ Anxiety Disord20092381086109019640675
- HambrickJPTurkCLHeimbergRGThe experience of disability and quality of life in social anxiety disorderDepress Anxiety2003181465012900952
- Masia-WarnerCKleinRGDentHCSchool-based intervention for adolescents with social anxiety disorder: results of a controlled studyJ Abnorm Child Psychol200533670772216328746
- FisherPHMasia-WarnerCKleinRGSkills for social and academic success: a school-based intervention for social anxiety disorder in adolescentsClin Child Fam Psychol Rev20047424124915648278
- FurukawaTAChenJWatanabeNVideotaped experiments to drop safety behaviors and self-focused attention for patients with social anxiety disorder: do they change subjective and objective evaluations of anxiety and performance?J Behav Ther Exp Psychiatry200940220221018930452
- XuYSchneierFHeimbergRGGender differences in social anxiety disorder: Results from the national epidemiologic sample on alcohol and related conditionsJ Anxiety Disord8172011
- BaconAKHamLSAttention to social threat as a vulnerability to the development of comorbid social anxiety disorder and alcohol use disorders: an avoidance-coping cognitive modelAddict Behav2010351192593920605074
- SchneierFRFooseTEHasinDSSocial anxiety disorder and alcohol use disorder co-morbidity in the National Epidemiologic Survey on Alcohol and Related ConditionsPsychol Med201040697798820441690
- ChouKLSocial anxiety disorder in older adults: evidence from the National Epidemiologic Survey on alcohol and related conditionsJ Affect Disord20091191–3768319394088
- BucknerJDTurnerRJSocial anxiety disorder as a risk factor for alcohol use disorders: a prospective examination of parental and peer influencesDrug Alcohol Depend20091001–212813719022589
- AkechiTOkuyamaTSagawaRSocial anxiety disorder as a hidden psychiatric comorbidity among cancer patientsPalliat Support Care20119110310521352622
- DalrympleKLZimmermanMScreening for social fears and social anxiety disorder in psychiatric outpatientsCompr Psychiatry200849439940618555062
- BruceSEYonkersKAOttoMWInfluence of psychiatric comorbidity on recovery and recurrence in generalized anxiety disorder, social phobia, and panic disorder: a 12-year prospective studyAm J Psychiatry200516261179118715930067
- LinCCDuloxetine treatment of social anxiety disorder with comorbid major depressionJ Clin Psychopharmacol2008285591592 author reply 592–59318794669
- SchneierFRBlancoCCampeasRCitalopram treatment of social anxiety disorder with comorbid major depressionDepress Anxiety200317419119612820174
- BronischTHechtHMajor depression with and without a coexisting anxiety disorder: social dysfunction, social integration, and personality featuresJ Affect Disord19902031511572148334
- MoitraEBeardCWeisbergRBKellerMBOccupational impairment and social anxiety disorder in a sample of primary care patientsJ Affect Disord20111301–220921220934220
- CulpepperLSocial anxiety disorder in the primary care settingJ Clin Psychiatry200667Suppl 12313717092194
- KashdanTBFruehBCKnappRGSocial anxiety disorder in veterans affairs primary care clinicsBehav Res Ther200644223324716389063
- GrossROlfsonMGameroffMJSocial anxiety disorder in primary careGen Hosp Psychiatry200527316116815882762
- ElliottHWReiflerBSocial anxiety disorder. A guide for primary care physiciansN C Med J200061317617810832377
- KatzelnickDJGreistJHSocial anxiety disorder: an unrecognized problem in primary careJ Clin Psychiatry200162Suppl 11115 discussion 15–1611206029
- SheeranTZimmermanMSocial phobia: still a neglected anxiety disorder?J Nerv Ment Dis20021901178678812436021
- LiebowitzMRGormanJMFyerAJKleinDFSocial phobia. Review of a neglected anxiety disorderArch Gen Psychiatry19854277297362861796
- FinkMAkimovaESpindeleggerCSocial anxiety disorder: epidemiology, biology and treatmentPsychiatr Danub200921453354219935490
- Khalid-KhanSSantibanezMPMcMickenCRynnMASocial anxiety disorder in children and adolescents: epidemiology, diagnosis, and treatmentPaediatr Drugs20079422723717705562
- GrantBFHasinDSBlancoCThe epidemiology of social anxiety disorder in the United States: results from the National Epidemiologic Survey on Alcohol and Related ConditionsJ Clin Psychiatry200566111351136116420070
- HaJLimSWShinYCOhKSComparison of anxiety-related traits between generalized and nongeneralized subtypes of social anxiety disorderJ Nerv Ment Dis2011199639039321629017
- CoxBJTurnbullDLRobinsonJAThe effect of avoidant personality disorder on the persistence of generalized social anxiety disorder in the general population: results from a longitudinal, nationally representative mental health surveyDepress Anxiety201128325025521308885
- MoscovitchDASuvakMKHofmannSGEmotional response patterns during social threat in individuals with generalized social anxiety disorder and non-anxious controlsJ Anxiety Disord201024778579120708493
- ShahSGKlumppHAngstadtMAmygdala and insula response to emotional images in patients with generalized social anxiety disorderJ Psychiatry Neurosci200934429630219568481
- BlancoCAntiaSXLiebowitzMRPharmacotherapy of social anxiety disorderBiological Psychiatry200251110912011801236
- WarwickJMCareyPVan der LindenGA comparison of the effects of citalopram and moclobemide on resting brain perfusion in social anxiety disorderMetab Brain Dis2006212–324125216850261
- SteinDJCameronAAmreinRMontgomerySAMoclobemide is effective and well tolerated in the long-term pharmacotherapy of social anxiety disorder with or without comorbid anxiety disorderInt Clin Psychopharmacol200217416117012131599
- SteinMBSeedatSGelernterJSerotonin transporter gene promoter polymorphism predicts SSRI response in generalized social anxiety disorderPsychopharmacology (Berl)20061871687216525856
- VasileRGBruceSEGoismanRMResults of a naturalistic longitudinal study of benzodiazepine and SSRI use in the treatment of generalized anxiety disorder and social phobiaDepress Anxiety2005222596716094662
- Van AmeringenMManciniCFarvoldenPOakmanJDrugs in development for social anxiety disorder: more to social anxiety than meets the SSRIExpert Opin Investig Drugs200091022152231
- StangierUSchrammEHeidenreichTCognitive therapy vs interpersonal psychotherapy in social anxiety disorder: a randomized controlled trialArch Gen Psychiatry201168769270021727253
- SteinDJIpserJCCombined pharmacotherapy and psychotherapy for social anxiety disorderCurr Psychiatry Rep201012427327520568024
- HolmbergNKahkonenSCognitive psychotherapy of social phobia and generalized anxiety disorderDuodecim2009125181949195619860079
- LipsitzJDMarshallRDAlternative psychotherapy approaches for social anxiety disorderPsychiatr Clin North Am200124481782911723635
- CastagnaARinaldiSFontaniVDoes osteoarthritis of the knee also have a psychogenic component? Psycho-emotional treatment with a radio-electric device vs intra-articular injection of sodium hyaluronate: an open-label, naturalistic studyAcupunct Electrother Res2010351–211620578643
- CollodelGMorettiEFontaniVEffect of emotional stress on sperm qualityIndian J Med Res2008128325426119052335
- RinaldiSFontaniVAravagliLMannuPPsychometric evaluation of a radio electric auricular treatment for stress related disorders: a double-blinded, placebo-controlled controlled pilot studyHealth Qual Life Outcomes201083120302662
- RinaldiSFontaniVAravagliLStress-related psycho-physiological disorders: randomized single blind placebo controlled naturalistic study of psychometric evaluation using a radio electric asymmetric treatmentHealth Qual Life Outcomes2011915421771304
- RinaldiSFontaniVAravagliLMargottiMLPsychological and symptomatic stress-related disorders with radio-electric treatment: psychometric evaluationStress and Health2010265350358
- RinaldiSFontaniVMorettiEA new approach on stress-related depression and anxiety: neuro-psycho-physical-optimization with radio electric asymmetric conveyerIndian J Med Res201013218919420716819
- OlivieriEBVecchiatoCIgnaccoloNRadioelectric brain stimulation in the treatment of generalized anxiety disorder with comorbid major depression in a psychiatric hospital: a pilot studyNeuropsychiatr Dis Treat2011744945521857785
- MannuPRinaldiSFontaniVRadio electric treatment vs Es-citalopram in the treatment of panic disorders associated with major depression: an open-label, naturalistic studyAcupunct Electrother Res2009343–413514920344882
- MannuPRinaldiSFontaniVCastagnaALong-term treatment of bipolar disorder with a radioelectric asymmetric conveyorNeuropsychiatr Dis Treat2011737337921822388
- MannuPRinaldiSFontaniVCastagnaARadio electric asymmetric brain stimulation in the treatment of behavioral and psychiatric symptoms in Alzheimer diseaseClin Interv Aging2011620721121822377
- GermansSVan HeckGLMasthoffEDDiagnostic efficiency among psychiatric outpatients of a self-report version of a subset of screen items of the Structured Clinical Interview for DSM-IV-TR Personality Disorders (SCID-II)Psychol Assess201022494595221038969
- HajebiAMotevalianAAmin-EsmaeiliMTelephone versus face-to-face administration of the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, for diagnosis of psychotic disordersCompr Psychiatry852011
- ConnorKMDavidsonJRChungHMultidimensional effects of sertraline in social anxiety disorderDepress Anxiety200623161016216019
- SokolenkoMKutcherSSertraline for social anxiety disorderExpert Rev Neurother20033678779519810881
- LiebowitzMRDeMartinisNAWeihsKEfficacy of sertraline in severe generalized social anxiety disorder: results of a double-blind, placebo-controlled studyJ Clin Psychiatry200364778579212934979
- BusnerJTargumSDMillerDSThe Clinical Global Impressions scale: errors in understanding and useCompr Psychiatry200950325726219374971
- BusnerJTargumSDThe clinical global impressions scale: applying a research tool in clinical practicePsychiatry (Edgmont)200747283720526405
- RytwinskiNKFrescoDMHeimbergRGScreening for social anxiety disorder with the self-report version of the Liebowitz Social Anxiety ScaleDepress Anxiety2009261343818781659
- KummerACardosoFTeixeiraALFrequency of social phobia and psychometric properties of the Liebowitz social anxiety scale in Parkinson’s diseaseMov Disord200823121739174318661550
- MenninDSFrescoDMHeimbergRGScreening for social anxiety disorder in the clinical setting: using the Liebowitz Social Anxiety ScaleJ Anxiety Disord200216666167312405524
- RinaldiSFontaniVRadioelectric asymmetric conveyer for therapeutic useUS patentEP1301241(B1)10112006 2000
- RinaldiSFontaniVRadioelectric asymmetric conveyer for therapeutic useUS patent7,333,8592192008 2001