
Abstract
Purpose
Community-acquired urinary tract infection (CA-UTI) is a common and costly condition in females. Currently, there are no data on CA-UTI and quality of life (QoL) in Saudi Arabia. The aim of this study was to evaluate the impact of UTI and related socio-demographic characteristics on health-related quality of life (HRQoL) of Saudi females using the EuroQol 5-Dimension, 3-Level (EQ-5D-3L) instrument before and after treatment.
Patients and Methods
This was a cross-sectional questionnaire study conducted in the emergency department (ED) of a tertiary hospital over a three-month period.
Results
A total of 339 out of 524 females with a mean age of 36.2 years (SD: 9.57 years; range 19–59 years) completed both the baseline and follow-up questionnaires of the EQ-5D-3L for a response rate of 64.7%. The baseline utility index for the worst health state “33333” was −0.495 representing 1.18% of the patients, and the full health state “11111” was 1 corresponding to 30.68% of the patients. The utility index after treatment for the moderate health state “22222” was 0.524 corresponding to 0.88% of the total patients, and the full health state “11111” was 1 corresponding to 80.24% of the patients. The mean EuroQol Visual Analogue Scale (EQ-VAS) was 73 ± 26 before treatment and 87.46 ± 18.55 after treatment. The frequency of patients reporting problems in the EQ-5D dimensions of mobility, self-care, usual activities, pain/discomfort and anxiety/depression decreased following treatment (27.43% vs 0.88%, 4.42% vs 0.88%, 25.96% vs 6.78%, 61.95% vs 13.27%, 39.52% vs 15.63%, respectively; all P < 0.001). There were statistically significant associations between HRQoL and socio-demographic characteristics, chronic diseases, and herbal supplements.
Conclusion
Community-acquired tract infections (CA-UTIs) have a significant negative impact on the HRQoL of Saudi females with a varying effect depending on the socio-demographic characteristics and chronic diseases.
Introduction
Urinary tract infections (UTIs) are a common and costly condition worldwide, affecting all ages and gender, with the highest prevalence among women.Citation1–Citation3 The prevalence of community-acquired urinary tract infections (CA-UTIs) accounts for 14.6% of emergency visits among adults in Saudi Arabia and recurrent episodes among females accounts for 20.6%.Citation1
Urinary tract infections represent 22% of infections in the emergency department (ED) of hospitals in Saudi Arabia.Citation4 CA-UTIs are most often treated with antibiotics, and overuse and inappropriate practices involving antibiotics can result in the development of antimicrobial resistance and increased costs.Citation4–Citation6 The mean cost for CA-UTI treatment in EDs in Saudi Arabia has been estimated as $134.56±$31.34.Citation1
Despite the fact that UTIs are a common health problem in EDs and primary care with clinical and economic impact,Citation1–Citation3 there are limited data available regarding how UTIs affect the quality of life (QoL) of patients throughout the world. In Saudi Arabia, no information is available on the effects of CA-UTIs on health-related QoL in Saudis females. QoL indicators are strong predictors of a patient’s general ability to preserve long-term health and productivity.Citation1,Citation7 In this regard, health-related quality of life (HRQoL) is crucial for measuring the burden of illness and assisting physicians and policy makers to improve patient care and policy decisions.Citation8
Several instruments have been implemented to measure HRQoL such as the EuroQol 5-Dimension, 3-Level questionnaire (EQ-5D-3L). The EQ-5D instrument was designed by the EuroQol Group to assess health for clinical and economic appraisal by utilizing a simple, generic and standardized HRQoL questionnaire.Citation9,Citation10 The EQ-5D is a valid and reliable measure in many disease areas and is the most commonly used tool for assessing cost-utility analyses in order to appraise healthcare interventions.Citation10–Citation16
Utility scores are used to quantify the severity of a patient’s condition and the burden of disease state, allowing for comparisons across a wide range of disease states, people, and different treatment modalities. In addition, the utility scores can be combined with life expectancy estimates to calculate quality-adjusted life years, which is a unit of measurement for quantifying the benefits of an intervention.Citation15 Utility scores range from 0 to 1 on a scale with high utility (1) indicating a full health outcome, low utility demonstrating a worse health outcome, and zero representing death.Citation15,Citation17,Citation18
Therefore, it is necessary to know the level of HRQoL of CA-UTI patients and identify factors that result in decreased or impaired HRQoL as this will help policy makers to prioritize funding and implement interventions to improve QoL. The aim of this research was to evaluate the impact of CA-UTIs and related socio-demographics on the HRQoL using the EQ-5D-3L instrument in Saudis females before and after treatment for the CA-UTIs.
Methods
Design/Setting
This was a cross-sectional questionnaire-based study performed in the ED of King Abdulaziz Medical City (KAMC) over a three-month period. KAMC is a 1505-bed university affiliated major tertiary care center in Riyadh, Saudi Arabia.
Participants
The participants of interest were females aged 18 to 59 years and had their condition diagnosed by a physician based on a history of symptoms as well as urinalysis results consistent with CA-UTIs and having at least one antibiotic prescription from the ED. Participants were excluded from the study if they were younger than 18 or older than 59 years, were pregnant, had catheter acquired urinary tract infection, vesicoureteral reflux disease, acute pyelonephritis, kidney failure, or an immunodeficiency disorder.
Data Collection
The questionnaires for the Saudi females were demonstrated in Arabic and the statement of confidentiality issues was explained on the cover page. The completion of the questionnaire was considered consent to participate in the study. Each questionnaire was completed by the participants.
The questionnaire composed of two parts as follows:
Socio-Demographic Characteristics
Socio-demographic data including age, medical history, current use of herbal supplements, education status (higher education, middle education, low education), marital status (single, married, other), employment status (employed, unemployed, student), and the patient’s monthly income in Saudi Arabian Riyal (SAR).
Assessment of HRQoL
The validity and reliability of an Arabic version of the EQ-5D-3L questionnaire was determined after obtaining prior approval from the EuroQol Research Foundation.Citation16 The EQ-5D instrument questionnaire is comprised of two components: a description of health state (EQ-5D descriptive system) and an evaluation of health state (EQ-5D visual analogue scale (EQ-VAS)). The health state description, EuroQol 5-Dimension, 3-Level (EQ-5D-3L) consists of five dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension has three levels of severity scale: 1) no problems, 2) moderate problems, 3) severe or extreme problems and the participants were asked to select the statement that best describes their health status. The responses are combined to produce a five-digit number describing the respondent’s health status (ranging from 11111 to 33333): 11111 (having no problems in all dimensions or full health) and 33333 (having extreme problems in all dimensions or worst health). The EQ-5D-3L health states were converted based on the crosswalk methodology to obtain a standardized utility index (UI) score ranging from 0 (representing death) to 1 (representing full health), with negative values representing states worse than death.Citation14,Citation17 The second part of the instrument is an evaluation of health state, EQ-VAS, which is a visual vertical scale ranging from “0” to “100”. The participant records her health status on a vertical VAS ranging from “Best imaginable health state” (100) to “Worst imaginable health state” (0).
Statistical Analysis
Analyses were performed using SPSS statistical software (version 22; IBM, Armonk, NY, USA). Descriptive statistics such as frequency, percentage, mean ± SD, or median (range) were used for socio-demographic, illness variables, and problems at each level for each dimension of the EQ-5D-3L. Bivariate analysis using Pearson’s χ2 test was used for categorical variables. For all statistical tests, P<0.05 was considered statistically significant.
Ethical Issues
The study was approved by the Institutional Review Board and the Ethical Committee at King Abdullah International Medical Research Center (KAIMRC), King Saud Bin-Abdulaziz University for Health Sciences, Riyadh (RR20/551/R). Oral informed consent and completion of the questionnaire were considered consent to participate in the study.
Patient confidentiality and privacy of information were secured by the principal investigator.
Results
A total of 339 out of 524 females completed both baseline and follow-up questionnaires for a response rate of 64.7%.
Social Demographic Characteristics
The respondents had a mean age of 36.2 years (SD: 9.57 years; range 19–59 years). Most patients were aged 40–49 years (35.69%) followed by the age groups 30–39 years (33.63%), 19–29 years (24.19%) and then 50–59 years (6.46%). The healthy respondents represented 52.21% of patients whereas 47.79% of respondents had at least one medical illness. The most common medical illnesses were gynaecological (fibroid/ovarian cysts) representing 17.07% of the patients and diabetes mellitus representing 14.02% of patients. The use of herbal supplements during the CA-UTI episode occurred in 30.68% of patients. The majority of the female patients had a high level of educational (59%) and were employed 49.56%; 35.10% were unemployed and 15.34% were students and most of the respondents were married (71.09%), .
Table 1 Socio-Demographic Characteristics of Patients
Assessment of HRQoL
Description of Health State (EQ-5D)
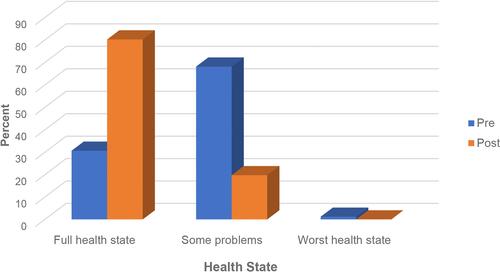
illustrates that there was an improvement in the health state among respondents after treatment. The percentage of respondents that did not have a problem in any dimensions of the EQ-5D (perfect or full health state) increased from (30.68%) to (80.24%). The percentage of respondents that reported having problems in some dimensions of the EQ-5D decreased from (68.14%) to (19.76%). The number of respondents that reported having problems in all dimensions of the EQ-5D (worse or extreme health state) decreased from (1.18%) to none of the respondents following treatment.
Figure 1 Health state pre- and post-treatment.
As shown in , at baseline, the percentage of respondents who reported having no problems in terms of mobility, self-care, usual activities, pain or discomfort and anxiety or depression were 72.57%, 94.40%, 74.04%, 38.05%, and 60.47%, respectively.
Table 2 Numbers and Proportions Reporting Levels Within EQ-5D Dimensions: Pre- and Post-Treatment
Treatment of UTI led to a decrease in the percentage of patients reporting some problems in the dimensions of mobility (27.43% to 0.88%; P < 0.001), self-care (4.42% to 0.88%; P < 0.001), usual activities (25.96% to 6.78%; P < 0.001), pain/discomfort (61.95% to 13.27%; P < 0.0001), and anxiety/depression (39.52% to15.63%; P < 0.001). No severe problems were reported after the treatment.
As shown in , the baseline for the health state ranged from “11111” to “33333”. The full health state “11111” was represented in 30.68% of the patients and the worst health state “33333” was represented in 1.18% of the patients. After treatment, the health state ranged from “11111” to “22222”. The full health state “11111” was represented in 80.24% of patients and the moderate health state “22222” was represented in 0.88% of patients. Treatment of CA-UTI increased the percentage of patients reporting health states “11111” (30.68% to 80.24%; P < 0.001) and “11222” (1.77% to 5.31%%; P < 0.001). There was a decrease in the percentage of patients who reported health states “11121” (14.75% to 4.13%; P < 0.001), “11122” (12.68% to 2.95%, P < 0.001), and “11221” (1.77% to 0%, P < 0.001).
Figure 2 Health-related quality of life measured using the EQ-5D-3L scale.
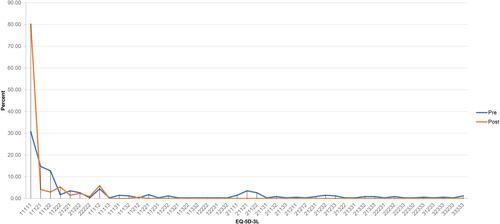
The baseline utility index for the worst health state “33333” was - 0.495 representing 1.18% of the total patients and 1 for the full health state “11111” corresponding to 30.68% of the total patients. The utility index after treatment for the moderate health state “22222” was 0.524 corresponding to 0.88% of the total patients and 1 for the full health state “11111” corresponding to 80.24% of the total patients.
Evaluation of Health State (EQ-VAS)
Health was assessed using the EQ-VAS at two times: baseline VAS (first time was before treatment) and second VAS (after treatment). This assessment showed that, in general, the respondents tended towards a gain in quality of life after treatment. The baseline mean EQ-VAS was 73 ± 26 and after treatment the mean EQ-VAS was 87.46 ± 18.55.
Relationship Between HRQoL and Socio-Demographic Characteristics
presents the association between HRQoL and socio-demographic characteristics before and after treatment based on univariate analyses. The baseline frequencies of the moderate to severe health state were significantly higher in older females (86.4%), females with a history of medical disease (85%), females who reported having a gynaecological disease (96.4%), and diabetic females (95.7%) (all P < 0.001). A significantly higher frequency was also reported among herbal supplement users compared to those who did not receive herbal supplements (87.5% vs 61.3%; P = 0.001). After treatment, the moderate to severe health state was significantly higher in females with a history of medical disease (28.4%), females who reported having a gynaecological disease (39.3%), diabetes mellitus (34.8%), or older females (31.8%) (all P <0.001).
Table 3 Association Between Overall Health-Related Quality of Life Pre- and Post-Treatment and Other Sample Characteristics
Discussion
This was the first study to measure HRQoL among Saudi females in the kingdom of Saudi Arabia with CA-UTI utilizing the EuroQol instrument (EQ-5D-3L). In the present study, the implementation of the EQ-5D was straightforward, and the response rate over the three-month interval was 64.7%. The results of the questionnaire provide a descriptive view of the patients’ HRQoL and allow for a direct calculation of Health Utility Values (HUVs). HUVs are key variables in economic decision models and are used in cost–utility analyses for the direct calculation of quality-adjusted life years (QALYs) and the costs associated with medical treatment of CA-UTI.Citation15,Citation18
The values of health states differ from equivalent values depending on the measure and method of valuation.Citation19 Quality of life is a broad concept that is affected by multiple parameters other than the patient’s health status. These parameters include the level of independence, social setting, psychological state, and medical history.Citation19,Citation20 In the current study, the baseline health status of females with CA-UTI ranged from “33333” to “11111” for values −0.495 to 1 and ranged from “22222” to “11111” for values 0.524 to 1 after treatment. The mean EQ-VAS was 73 ± 26 at baseline and 87.46 ± 18.55 after treatment.
There is no direct comparison between the current study and previous studies due to the differences in the methodology and instrument. There were several studies that estimated utilities of CA-UTI among females using different instruments to measure HRQoL and in the previous studies the baseline utilities were significantly low with scores ranging from 0.3 to 0.65 with improvements after treatment ranging from 0.8 to 0.99.Citation19,Citation21,Citation22 The overall improvement of QoL ranged from 78% to 95%, which was similar to the current study.Citation19,Citation23–Citation25
In the current study, the overall general health status of the majority of females showed clinically significant improvements in HRQoL, as measured by the EQ-5D-3L instrument, may be due to the fact that most of the CA-UTIs were mild and easily resolved with appropriate antibiotic treatment. The current study indicates that UTIs severely affect HRQoL and contributes to depression, decreased mobility activity, report pain, restriction of work and school, and bed rest, which affects quality of life and has economic impacts.
Pain/discomfort was the most frequently reported complaint followed by anxiety/depression, whereas self-care problems were the least frequently reported, which is similar to other studies.Citation7,Citation19 In the current study, the quality of life was affected by socio-demographic characteristics such as older age, employment status, and marital status. These findings were consistent with previous studies.Citation26 Older age was associated with poor HRQoL, similar to previous studies in other countries.Citation19,Citation26 However, some studies have reported that most diseases have an equally strong impact on HRQoL and all age groups suffer from some chronic conditions having the same impact on QoL.Citation27 Employed females had significantly higher health state than unemployed females, which may be due to the work environment. Some studies reported that employment impacts patients’ HRQoL.Citation26,Citation27 The association between HRQoL and chronic diseases has been confirmed by many previous studies measured by different instruments and consistent with a QoL study of diabetic patients conducted in Saudi Arabia.Citation7,Citation26,Citation27
Gynaecology diseases had a high impact on the health state probably due to anatomical and functional characteristics of females resulting in female patients having a relatively high percentage of UTIs compared to male patients.Citation1
In the current study, approximately 30.68% of the females used herbal supplements to treat UTIs during the study. Several strategies have used different prophylactic or treatment strategies for the treatment of UTI, such as altered diets, increased water intake, in taurine acidification using ascorbic acid, and dietary or supplemental cranberry; however, the evidence base for the efficacy of many of these strategies is weak or entirely lacking.Citation28,Citation29 The European Association of Urology recommends OM-89 as a prophylactic strategy in urology infections with the highest evidence level and recommendation grade.Citation28
This study indicates that in this female patient population, QoL is mainly influenced by CA-UTI with QoL showing a decrease in the results analysis of EQ-5D and EQ-VAS with age, employment, chronic disease, and marriage. The EQ-5D instrument is a tool used to measure general health status and is a sensitive and valid approach for monitoring changes in QoL and patient outcomes in Saudi females with CA-UTI.
Limitations
The current study has some limitations. First, it was conducted in only the ED setting of KAMC, which does not represent all hospital settings; thus, the findings cannot be generalized. Second, only females between the ages of 18 to 59 years were investigated in the study, which might produce some bias, especially when participants over 50 years of age had a lower response than the other age groups. Third, this was a short cross-sectional study over a three-month period with a response rate of 64.7%that did not represent all of the population. Finally, the measurement of health status using the EQ-5D instrument may have resulted in over- or underestimation of QoL of females with UTIs because the patients self-assessed their quality of health and may have selected a high level. Multicentre prospective studies are recommended for the accurate measurement of HRQoL of CA-UTIs among the Saudi population.
Conclusion
CA-UTIs have a significant negative impact on females’ HRQoL with a varying effect based on socio-demographic characteristics and chronic diseases. Identifying the health status of Saudi females with CA-UTIs and recognizing the factors that are significantly associated with HRQoL could support and help clinicians and health policymakers make effective and efficient strategies for the improvement and monitoring of patient outcomes in the future.
Acknowledgments
The author would like to thank the King Abdullah International Medical Research Center (KAIMRC) for their help and cooperation. Special thanks to Dr. Ahmed Alaskar for his support and to Dr. Fulwah Y Alqahtani for consultation, and thanks to the emergency department.
Disclosure
The author reports no conflicts of interest in this work.
References
- Alanazi MQ. An evaluation of community-acquired urinary tract infection and appropriateness of treatment in an emergency department in Saudi Arabia. Ther Clin Risk Manag. 2018;14:2363–2373. doi:10.2147/TCRM.S178855
- François M, Hanslik T, Dervaux B, et al. The economic burden of urinary tract infections in women visiting general practices in France: a cross-sectional survey. BMC Health Serv Res. 2016;16(a):365. doi:10.1186/s12913-016-1620-2
- Kalyanaraman R, Demtchouk V, Iyer V, Patterson D. Determining the health state utility value of urinary tract infection in Women. Female Pelvic Med Reconstr Surg. 2019;25(2):185–187. doi:10.1097/SPV.0000000000000696
- Alanazi MQ, Al-Jeraisy MI, Salam M. Prevalence and predictors of antibiotic prescription errors in an emergency department, Central Saudi Arabia. Drug Healthc Patient Saf. 2015;7:103–111.
- Alanazi MQ, Alqahtani FY, Aleanizy FS. An evaluation of E. coli in urinary tract infection in emergency department at KAMC in Riyadh, Saudi Arabia: retrospective study. Ann Clin Microbiol Antimicrob. 2018;17(1):3. doi:10.1186/s12941-018-0255-z
- Alanazi MQ, Salam M, Alqahtani FY, et al. An evaluation of antibiotics prescribing patterns in the emergency department of a tertiary care hospital in Saudi Arabia. Infect Drug Resist. 2019;12:3241–3247. doi:10.2147/IDR.S211673
- Alshayban D, Joseph R. Health-related quality of life among patients with type 2 diabetes mellitus in Eastern Province, Saudi Arabia: a cross-sectional study. PLoS One. 2020;15(1):e0227573.
- Guyatt GH, Feeny DH, Patrick DL. Measuring health-related quality of life. Ann Intern Med. 1993;118(8):622–629. doi:10.7326/0003-4819-118-8-199304150-00009
- The EuroQol Group. EuroQol–a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199–208. doi:10.1016/0168-8510(90)90421-9
- Cabasés J, In: RR. Introduction. In: Szende A, Janssen B, Cabases J, editors. Self-Reported Population Health: An International Perspective Based on EQ-5D. Dordrecht: Springer; 2014:1–6.
- Devlin NJ, Shah KK, Feng Y, Mulhern B, van Hout B. Valuing health‐related quality of life: an EQ‐5D‐5L value set for England. Health Econ. 2018;27:7–22. doi:10.1002/hec.3564
- Wisloff T, Hagen G, Hamidi V, Movik E, Klemp M, Olsen JA. Estimating QALY gains in applied studies: a review of cost-utility analyses published in 2010. Pharmacoeconomics. 2014;32:367–375. doi:10.1007/s40273-014-0136-z
- Devlin NJ, Brooks R. EQ-5D and the EuroQol group: past, present and future. Appl Health Econ Health Policy. 2017;15(2):127–137. doi:10.1007/s40258-017-0310-5
- Rupel VP, Crosswalk OM. EQ-5D-5L value set for Slovenia. Slovenian J Public Health. 2020;59(3):189–194. doi:10.2478/sjph-2020-0024
- Harvie HS, Shea JA, Andy UU, Propert K, Schwartz JS, Arya LA. Validity of utility measures for women with urge, stress, and mixed urinary incontinence. Am J Obstet Gynecol. 2014;210(1):85–e1. doi:10.1016/j.ajog.2013.09.025
- EuroQol Research foundation. EQ-5D-3L user Guide. Available from: https://euroqol.org. Accessed November 24, 2020.
- Van Hout B, Janssen MF, Feng YS, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708–715. doi:10.1016/j.jval.2012.02.008
- Sanyal C, Husereau DR, Beahm NP, Smyth D, Tsuyuki RT. Cost-effectiveness and budget impact of the management of uncomplicated urinary tract infection by community pharmacists. BMC Health Serv Res. 2019;19(1):499. doi:10.1186/s12913-019-4303-y
- Bermingham SL, Ashe JF. Systematic review of the impact of urinary tract infections on health‐related quality of life. BJU Int. 2012;110(11c):E830–6. doi:10.1111/j.1464-410X.2012.11337.x
- Gerlinger C, Bamber L, Leverkus F, et al. Comparing the EQ-5D-5L utility index based on value sets of different countries: impact on the interpretation of clinical study results. BMC Res Notes. 2019;12(1):1–6.
- Sonnenberg FA, Burkman RT, Hagerty CG, Speroff L, Speroff T. Costs and net health effects of contraceptive methods. Contraception. 2004;69:447–459. doi:10.1016/j.contraception.2004.03.008
- Ernst EJ, Ernst ME, Hoehns JD, Bergus GR. Women’s quality of life is decreased by acute cystitis and antibiotic adverse effects associated with treatment. Health Qual Life Outcomes. 2005;3:45. doi:10.1186/1477-7525-3-45
- Ellis AK, Verma S. Quality of life in women with urinary tract infections: is benign disease a misnomer? J Am Board Fam Pract. 2000;13:392–397. doi:10.3122/15572625-13-6-392
- Abrahamian FM, Krishnadasan A, Mower WR, Moran GJ, Coker JR, Talan DA. The association of antimicrobial resistance with cure and quality of life among women with acute uncomplicated cystitis. Infection. 2011;39:507–514. doi:10.1007/s15010-011-0163-z
- Plowman R, Graves N, Esquivel J, Roberts JA. An economic model to assess the cost and benefits of the routine use of silver alloy coated urinary catheters to reduce the risk of urinary tract infections in catheterized patients. J Hosp Infect. 2001;48:33–42. doi:10.1053/jhin.2001.0938
- Wagenlehner F, Wullt B, Ballarini S, Zingg D, Naber KG. Social and economic burden of recurrent urinary tract infections and quality of life: a patient web-based study (GESPRIT). Expert Rev Pharmacoecon Outcomes Res. 2018;18(1):107–117. doi:10.1080/14737167.2017.1359543
- Xu RH, Cheung AW, Wong EL. Examining the health-related quality of life using EQ-5D-5L in patients with four kinds of chronic diseases from specialist outpatient clinics in Hong Kong SAR, China. Patient Prefer Adherence. 2017;11:1565. doi:10.2147/PPA.S143944
- Bonkat G, Pickard R, Bartoletti R, et al. EAU guidelines on urological infections; 2017 [ cited April 27, 2017]. Available from: http://uroweb.org/wp-content/uploads/EAU-Guidelines-Urological-Infections-v2.pdf. Accessed November 24, 2020.
- Ochoa-Brust GJ, Fernández AR, Villanueva-Ruiz GJ, et al. Daily intake of 100 mg ascorbic acid as urinary tract infection prophylactic agent during pregnancy. Acta Obstet Gynecol Scand. 2007;86:783–787. doi:10.1080/00016340701273189