
Abstract
Purpose
Pregnant women witness many changes in the body as well as in the oral cavity with many factors influencing these changes. This study evaluated the relationship between oral health status, perceptions, and pregnancy outcomes.
Methods
A cross sectional study design was implemented to recruit a convenience sample of women attending Obstetrics and gynecology department in public hospitals in East and capital city of Saudi Arabia. To collect data, a validated self-administered questionnaire in English and Arabic was used. The questionnaire covered background information, perceived oral health status, and dental visits.
Results
About 64.4% of the 481 women recruited had dental problems, 49.7% reported deterioration in their oral health during pregnancy, and 17.5% reported adverse pregnancy outcomes. Only 40.7% of pregnant women rated their oral health as good, and only 22% visited a dentist during their pregnancy. Dentists were the most common source of oral health information (44.1%), followed by social media (38.9%). Dental problems during pregnancy were significantly associated with adverse outcomes (P=0.007). Oral health perceptions of pregnant women, not visiting the dentist during pregnancy, and gingival problems were also significantly associated with adverse pregnancy outcomes (P=0.001). Those with fair to poor oral health were twice as likely to experience adverse pregnancy outcome. Those who intended to visit the dentist during their pregnancy but did not do so, as well as those who did not visit the dentist at all were 12 and 9 times more likely to experience adverse pregnancy outcomes respectively.
Conclusion
Dental complaints during pregnancy, oral health perceptions, and a lack of dental visits were all linked to increased likelihood of adverse pregnancy outcomes. There is a need for interprofessional collaboration to dispel myths and encourage oral health care and regular dental visits during pregnancy.
Introduction
Pregnancy-induced changes in the woman’s endocrine and immune systems increase her susceptibility to a variety of infections, including those of the oral cavity.Citation1 The reduction in pH, which in turn leads to a decrease in salivary buffering capacity may explain the shift in the microbial composition.Citation2 These combined with changes in dietary and oral hygiene habits, contribute to bacterial growth and raise the risk of dental caries during pregnancy.Citation3,Citation4 Pregnant women are usually at greater risk of developing gingival inflammation and periodontal diseases due to hormonal changes.Citation1,Citation5 Altered host inflammatory response, increased vascular permeability and the shift in supra and sub microbiota are some proposed factors that explain periodontal changes during pregnancy.Citation2,Citation6
Adverse pregnancy outcome has been linked to periodontal diseases; the compromised immunity, inflammatory mediators and toxic products were some of the reasons that explained the link between periodontal disease and adverse pregnancy outcomes.Citation2,Citation6 The most common adverse pregnancy outcomes include preterm delivery, low birth weight and pre-eclampsia. Children born with preterm low birth weight (which is a combination of preterm delivery and low birth weight) are at greater risk of newborn death and lifelong disabilities.Citation7 Pre-eclampsia is a multisystem progressive disorder characterized by hypertension and proteinuria leading to postpartum risks to women and also to the offspring who may be exposed to preterm low birth weight and increased disease risk in their postnatal lives.Citation8
Correct knowledge and perception were identified as key predictors to the adoption of good oral health practices as well as maintaining regular dental visits among pregnant women.Citation9 However, studies conducted among pregnant women have always reported lack of proper oral health knowledge as well as wrong perceptions about the importance of oral health and its effects on their pregnancy and their offsprings oral and general health.Citation9–11 It was also reported that pregnant women lack the knowledge about the importance of regular dental visits and tend to avoid dental care even if they suffer from dental problemsCitation11 mainly due to lack of knowledge and misconceptions that dental care/treatment will harm the fetus.Citation12
In Saudi Arabia there is a continuum increase in the prevalence of adverse pregnancy outcomesCitation13 as well as high prevalence of periodontal diseases.Citation14 Dental care for pregnant women is recommended and appropriate, either as a preventive measure for oral diseases and their potential consequences or as a means of treating existing problems and is completely safe when followed by certain precautions.Citation15–17 Avoidance of dental care during pregnancy was linked to personal, psychosocial, financial, behavioral, and perceptions about general and oral health needs.Citation18,Citation19 Self-assessment or self-perception of health is the individual ability to evaluate or to assess disease risks as well as severity, and it has been used as a subjective predictive indicator of long-term morbidity and mortality.Citation20 Although many studies investigated oral health knowledge, attitudes and practices among pregnant women in Saudi Arabia as well as in other Arab countries, nevertheless these studies were either from a single site or did not investigate women’s perceptions and its link to adverse pregnancy outcomes. As such evaluating the oral changes that occur during pregnancy is critical for early detection and intervention to prevent adverse pregnancy outcomes and promoting oral health of the newly born. This study investigated oral health changes, perceptions, and pregnancy outcomes among women in Saudi Arabia.
Materials and Methods
Study Design and Setting
This cross-sectional survey-based study was carried in the Eastern province and Riyadh (the capital city of Saudi Arabia) over a period of one month from November to December 2022 (for both the recruitment period and data collection period).
Study Participants
The study enlisted female participants (pregnant or not) from the eastern province and the Riyadh region. The survey targeted female patients that were or were not pregnant. Participants were included if they agreed to participate and answered all of the survey questions. Female dentists were barred from participating in the study.
Sample Size and Sampling Technique
The research team members visited selected healthcare facilities during the study period, and recruited women attending Obstetrics and gynecology department using convenience sampling. The sample size was calculated using an online calculator with a 95% confidence level, and 5% accuracy resulting in a minimum and a population of 16,000 and considering pregnant women’s population attending pre-natal facilities for 2 months to be as such: 500 pregnant women/week leading to a total of 16,000 women (500×4 (weeks) × 2 (months) × 4 (sites: Dammam, Khobar, Dhahran and Riyadh). The computed sample size was 375 pregnant women, which was increased to 400 to compensate for any missing data.
Data Collection Tool
The data was collected in reception areas or lounges while participants were waiting for their turn in the Obstetrics and gynecology department. The research team shared the link with the participants and just requested them to notify the team when they complete it.
Participants responded to the questionnaire using their own mobile phones. The participant could not respond to the questionnaire more than once using the same device. A closed-ended, self-administered questionnaire was used. The questionnaire was developed on Google forms and a QR code was generated to be scanned and shared online and was administered in both English and Arabic languages. Before beginning the study, the questionnaire was pilot tested on 30 pregnant women (who were not part of the actual study) and Cronbach’s α coefficient was calculated (0.85). We also requested feedback from the piloted participants regarding the clarity and simplicity of the questions. No questions required modifications or deletion. The questionnaire included the following sections:
Demographics
This section consisted of nine questions and included 1) age with possible response of younger than 25 years old, between 25 and 40 years, or older than 40 years. 2) nationality and participants can choose either Saudi or not Saudi. The categorization of age was purposely selected by the authors to include a range from >25 to < than 40 years as the childbearing age with an average of 26.6 years as per the Statista GCC report of 2017. 3) marital status with two options either married or not married. 4) educational level with three options no formal education, school education or university degree and above. 5) occupation and participants can choose either being a housewife, employed or employed in the health sector. For occupation, the categorization was purposively selected as housewife i.e unemployed Vs employed however we added a third category as employed in health sector as those working in health sector would have better knowledge and practices as such controlling this confounder. 6) family income per month categorized into less than 5000 Saudi Riyal (SR), between 5000 and 20,000 SR, more than 20,000SR or not sure. The income categorization was based on Statista Research Department data of 2021. 7) history of pregnancy answered as yes, no, currently pregnant. 8) participants were asked if they suffer from any of the following medical conditions hypertension, diabetes, obesity, high cholesterol, or others or none if they do not suffer from any medical condition. 9) participants were also asked if they are currently taking any medications and can respond with yes or no.
Oral Problems and Changes in Oral Health
Participants were asked if they had suffered from any oral problems or changes in their oral health during the last year answered as yes, no, or I do not recall. Participants who are currently pregnant, were asked if they had any dental complaints in the last year with possible answers of dental decay, tooth pain, gingivitis, gum bleeding, or no complaint. Participants were also asked to report what kind of oral changes during pregnancy have they encountered and they can choose one or more of the following options tooth pain, gum bleeding, bad oral odor, swelling in the oral cavity, gingival swelling, no changes. Responses for oral changes which was based on the common dental/oral problems during pregnancy that are thought to be linked to adverse pregnancy outcomes.
Perceptions of Oral Health
Participants were asked about how they perceive their oral health status with possible answers of good, fair, poor, or not sure.
Dental Visits and Sources of Health Information
Participants were asked about their patterns of dental visits before and during pregnancy (answered as yes, no, I planned to but did not go, yes, due to dental problem/complaint). They were also asked if they had been advised against dental care by a nurse or health-care professional (no, I did not receive, yes, from a nurse, yes, from an obstetrician, I was not pregnant before). Regarding dental visits, the selection of responses was based on previous reports that pregnant women either avoid dental visits (no) or visit the dentist (yes) or hesitant due to misconceptions about dental treatment (planned but did not go) or visit the dentist due to emergency (Yes, due to dental problem/complaint). We also asked if any of the participants have a close family member who is a dentist answered with yes or no.
Oral Health Knowledge
Participants were asked if they think that pregnancy increases the possibility of gingival inflammation and they can answer with yes, no, or I do not know. They were asked about the possible cause of oral changes during pregnancy, and they can answer hormonal changes, improper teeth brushing, poor oral hygiene, malnutrition, medications, or do not know. Participants were asked if they are aware about the treatment of gingival inflammation during pregnancy and they can choose surgical removal of swollen gum, no treatment needed, professional scaling, extract the affected tooth, medications, or do not know. We also asked the participants if they are aware about the consequences of gingival inflammation and they can choose one or more from the following options overgrowth of gum tissue, spontaneous gum bleeding, inflammation of supporting tooth structure, tooth sensitivity, tooth decay, affects oral health of the newborn, abscess, tooth mobility, loss of teeth, cause preterm labor and/or deliveries with low birth weight, do not know, no effect.
Adverse Pregnancy Outcomes
Participants were asked to report if they suffered from any complications during or after birth with possible answers of: no, I did not have any; no, I was not pregnant before; yes, low birth weight; yes, I did, had a preterm birth; yes, I had septicemia.
Ethical Considerations
The study protocol was developed in accordance with the principles of ethics of Helsinki declaration and was reviewed and approved by Deanship of Scientific Research at Imam Abdulrahman bin Faisal University (IRB-2022—02-085). A written introduction explaining the study objectives, the survey details and the time required to complete it was provided to all participants. Participants were assured of the confidentiality and anonymity of their responses, as well as the freedom to quit the survey at any time by choosing not to submit or exit button with no risks at all to the participants. Reading the survey introduction and agreeing to participate was considered as a consent to participate in the study.
Statistical Analysis
The dependent variable was adverse pregnancy outcomes. Two models were implemented. In the first model, we investigated oral health factors (oral health changes during pregnancy, dental complaints during pregnancy, and dental visits) as the independent variables and adverse pregnancy outcomes as a dependent variable. In the second model, we investigated perceptions of oral health as independent variable and adverse pregnancy outcomes as a dependent variable. Descriptive statistics were used to calculate the frequency and percentage of demographic characteristics. The association between factors and oral health knowledge and habits was examined using the Chi-Square Test. Additionally, multiple logistic regression was conducted, with adverse pregnancy outcomes as the dependent variable and oral health factors (such as changes during pregnancy, dental complaints, and dental visits) as the independent variables. Data were downloaded as Excel sheet, coded, and analysis was performed using the Statistical Package for the Social Sciences (SPSS version 22, IBM USA), with statistical significance defined as a p-value below 0.05.
Results
A total of 481 women participated in the survey, with presenting their demographic details. The largest age group was between 25 and 45 years old, comprising 53% of respondents. Almost all participants (95.6%) were Saudi nationals, 83% were married, 76.7% had higher education, and 46.4% identified as housewives. The majority (74.8%) had a history of pregnancy.
Table 1 Background Information of the Study Participants (N=481)
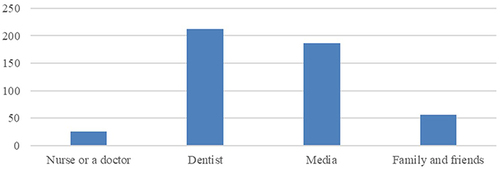
Among the participants, 17.5% reported complications during or after birth, 64.4% faced dental issues in the past year, and 46.2% rated their oral health as fair. illustrates that over 250 women noticed oral health deterioration during pregnancy, but only 22.5% visited the dentist during pregnancy. The majority (74.4%) did not receive oral health education during pregnancy, with dentists being the primary source of oral health information followed by media ().
Figure 1 Number of women who noticed deterioration in their oral health during pregnancy.
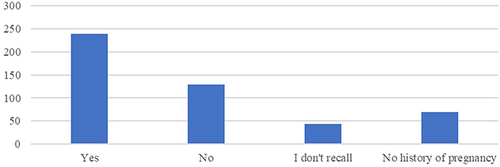
Figure 2 Source of oral health information among study participants.
outlines factors associated with adverse pregnancy outcomes. Experiencing dental problems in the past year, perceiving poor oral health, noticing oral health deterioration during pregnancy, and lacking dental visits or oral health education during pregnancy were all linked to adverse outcomes (p<0.05). Gingival bleeding, dental pain, or halitosis were also significantly associated with adverse outcomes (p<0.05). Those rating their oral health as fair or poor were twice as likely to experience adverse outcomes.
Table 2 Factors Associated with Adverse Pregnancy Outcomes
delves into the association between perception/knowledge of oral health and adverse pregnancy outcomes. Believing that pregnancy exacerbates gingival inflammation (p-0.002) or increases the risk of tooth loss was significantly linked to adverse outcomes (p-0.04).
Table 3 Oral Health Knowledge and Its Association with Adverse Pregnancy Outcomes
Poor oral health was associated with a 2.562-fold increase in adverse pregnancy outcomes (p=0.02) (). While obtaining oral health information from family and friends seemed to increase the likelihood of adverse outcomes by 3.27 times, this association was not statistically significant (p>0.05). Planning to visit the dentist during pregnancy but not doing so increased the likelihood of adverse outcomes by 1.82 times. Conversely, those who did not visit the dentist at all were less likely to experience adverse outcomes, a statistically significant finding (p=0.002).
Table 4 Multiple Logistics Regression
Discussion
This study investigated oral health status, perceptions, and adverse pregnancy outcomes among a sample of women in two Saudi cities. Although almost half of the women witnessed deterioration in their oral health and less than half perceived their oral health as good, yet less than a quarter visited the dentist during pregnancy. Dental complaints, lower perception of oral health and lack of dental visits during pregnancy were all associated with increased likelihood of adverse pregnancy outcomes.
Complications during pregnancy and childbirth are among the leading causes of disease and death among women in reproductive age worldwide.Citation21 In the current study, less than a quarter (17.5%) reported adverse pregnancy outcomes, a recent study in Qassim also reported a similar prevalence of 17.9%Citation22 which was significantly associated with higher prevalence and severity of periodontal diseases in both studies. The evidence for such an association is increasing with the prevalence reported worldwide to be between 15% and 100%.Citation23–25 A recent study has linked adverse pregnancy outcomes to increased risk of ischemic heart disease.Citation26 Premature infant health issues can have an impact on both their general and oral health. Due to enamel defects and poor dietary and oral hygiene habits, these children may be at greater risk of developing dental caries as well.Citation27 Adverse pregnancy outcomes are the most important indicators used to evaluate the efficiency of maternal and child health programs; they are also a measure of the quality of maternal and child health care services such as antenatal care, intrapartum care, and medical care. As a result, collaborative efforts are required to raise awareness about the risk factors and consequences of adverse pregnancy outcomes, as well as to identify potential risk factors through prenatal dental checkups.
According to the current study, more than half of the participants possessed adequate knowledge about the oral health changes they might experience during pregnancy. These findings are at odds with those of other studies.Citation28–31 On the other hand, our results are in line with those of a prior study that was carried out in Saudi Arabia.Citation32 Women educational level may be one of the factors that contribute to increased level of overall oral health knowledge. In the current sample, almost seventy-five percent of the women had a bachelor’s degree or higher which is a key factor in oral health knowledge and awareness.
Slightly more than half (52%) of women who participated in this study noticed deterioration in their dental health during pregnancy, contraindicating to what was reported by Swiss women as the majority (71%) did not experience any changes in their oral health during pregnancy.Citation33 Oral health status is affected by many factors such as personal factors (socioeconomic status and educational level), proper oral hygiene practices as well as relevant oral health knowledge.Citation34 Western societies have always reported better oral hygiene measures as well as access to correct oral health information,Citation35 all these factors collectively might explain the observed differences in oral health status during pregnancy. Inadequate oral health care during pregnancy has been linked to negative outcomes for both mothers and their newborns, according to previous studies.Citation1,Citation3,Citation6 It is critical to provide pregnant and conceiving women with accurate oral health information and care. A combination of personal and professional care is essential during pregnancy, as it plays a significant role in improving oral health.
The majority of women in the current study suffered from gingival bleeding, dental discomfort, bad breath, or gingival swelling which are all signs of periodontal diseases. Periodontitis can cause the loss of connective tissue and alveolar bone, which can lead to tooth loss. Preterm birth, fetal growth restriction, low birth weight, pre-eclampsia, and gestational diabetes are all linked to periodontal disease.Citation25 Periodontal diseases’ potential effect could be explained by two mechanisms: periodontal pathogen translocation to the fetoplacental unit or the effect of inflammatory mediators.Citation36 Although periodontal diseases start with objective signs that women can easily detect but misconceptions about dental treatments during pregnancy may prevent them from seeking dental care.Citation37 Less than half of the women surveyed rated their oral health as fair, and a quarter visited the dentist during their pregnancy, which is consistent with previous research that pregnant women are less likely to visit the dentist.Citation31,Citation38,Citation39 Many pregnant women do not seek or receive oral care, even if they have signs or symptoms of oral disease.Citation40 Financial barriers, a lack of awareness of the importance of oral health, perceived quality of care, access to technical aids, and the information provided have all been reported as barriers to dental visits during pregnancy.Citation12 Although some recommend that no treatment can be delivered during the first trimester,Citation41 there is a consensus agreement that it is safe to perform tooth extractions as well as preventive, emergency dental, restorative, and periodontal procedures during pregnancy, including the use of local anesthetics and radiographs given that the appropriate protection and precautionary measures are implemented.Citation42
It is crucial to be aware of the oral changes that occur during pregnancy in order to alleviate the psychological burden or concerns that women may experience. In the current study, half of the participants were aware that hormonal changes during pregnancy cause gingival inflammation. Consuming more refined carbohydrates will provide a suitable substrate for carcinogenic bacteria and may predispose some people to tooth decay. Frequent vomiting in some women during pregnancy has also been linked to the development of dental erosion.Citation40 However, reports on the knowledge of pregnant women about the causes and consequences of oral problems from elsewhere were controversial.Citation31,Citation33,Citation38,Citation43,Citation44 This might be due to differences across countries in prenatal care and maternal education provided.
More than two-thirds of pregnant women (74.4%) in the current study did not receive any oral health education during pregnancy, and the dentist was the primary source of oral health information, followed by the media. Pregnancy and postpartum period are ideal times for health education because women are concerned about the well-being of their newborns.Citation42 According to the American Dental Association (ADA) and the American College of Obstetricians and Gynecologists (ACOG), both obstetricians and dentists should advise pregnant women on the importance of good oral hygiene throughout their pregnancy.Citation45–47 There is a need for the inclusion of oral health within prenatal care and the collaboration of health professionals who are part of the prenatal care in oral health education and in correcting the misconceptions regarding dental treatment during pregnancy. In addition, there is a need to plan and evaluate multi-disciplinary interventions that can promote maternal health and wellbeing.Citation48
There are certain limitations in the current study that we would like to acknowledge, first its cross-sectional design can only identify the associated risk factors but does not prove causation. The self-reporting nature of the study might have led to a social desirability bias as well as over or under-reporting of the variables investigated. The sample was recruited from only two cities, samples from other cities might lead to different findings. Additionally, the “adverse pregnancy outcomes” measure combined three undesirable pregnancy outcomes many women might have had more than one of the listed complications so, women having one, two or the three undesirable pregnancy outcomes were included in the same group with women having only one complication. Future studies should analyze these outcomes separately. Despite the limitations, the use of a validated questionnaire and the representative sample allow for generalizing of the study findings by policymakers and different stakeholders to develop policy and plans to address the highlighted gaps.
Conclusion
Dental complaints during pregnancy, oral health perceptions, lack of dental visits, and gingival inflammation were significantly associated with adverse pregnancy outcomes. This study sheds the light on the low level of oral health awareness among pregnant women and the high prevalence of oral problems they experience during pregnancy. It also highlights the need for combined efforts of dentists and obstetricians in correcting the misconceptions with regard to dental treatments and oral health care. Cohort studies using both surveys and clinical examinations may allow for a better understanding of the key factors associated with adverse pregnancy outcomes. Oral health educational campaigns are also needed to clarify misconceptions among pregnant women and encourage regular dental visits during pregnancy.
Disclosure
The authors declare no conflicts of interest in this work.
References
- Silva de Araujo Figueiredo C, Gonçalves Carvalho Rosalem C, Costa Cantanhede AL, et al. Systemic alterations and their oral manifestations in pregnant women. J Obstet Gynaecol Res. 2017;43(1):16–22. doi:10.1111/jog.13150
- Zi MY, Longo PL, Bueno-Silva B, et al. Mechanisms involved in the association between periodontitis and complications in pregnancy. Front Public Health. 2015;2:290. doi:10.3389/fpubh.2014.00290
- Gonzalez-Jaranay M, Téllez L, Roa-López A, et al. Periodontal status during pregnancy and postpartum. PLoS One. 2017;12(5):e0178234. doi:10.1371/journal.pone.0178234
- Martínez-Pabón MC, Martínez Delgado CM, López-Palacio AM, et al. Características fisicoquímicas y microbiológicas de la saliva durante y después del embarazo [The physicochemical and microbiological characteristics of saliva during and after pregnancy]. Rev Salud Publica. 2014;16(1):128–138. doi:10.15446/rsap.v16n1.35767
- Saadaoui M, Singh P, Al Khodor S. Oral microbiome and pregnancy: a bidirectional relationship. J Reprod Immunol. 2021;145:103293. doi:10.1016/j.jri.2021.103293
- Figueiredo MGOP, Takita SY, Dourado BMR, et al. Periodontal disease: repercussions in pregnant woman and newborn health-A cohort study. PLoS One. 2019;14(11):e0225036. doi:10.1371/journal.pone.0225036
- Daalderop LA, Wieland BV, Tomsin K, et al. Periodontal disease and pregnancy outcomes: overview of systematic reviews. JDR Clin Trans Res. 2018;3(1):10–27. doi:10.1177/2380084417731097
- Turbeville HR, Sasser JM. Preeclampsia beyond pregnancy: long-term consequences for mother and child. Am J Physiol Renal Physiol. 2020;318(6):F1315–F1326. doi:10.1152/ajprenal.00071.2020
- Velosa‐Porras J, Rodríguez Malagón N. Perceptions, knowledge, and practices related to oral health in a group of pregnant women: a qualitative study. Clin Experiment Dent Res. 2024;10(1):e823. doi:10.1002/cre2.823
- Cagetti MG, Salerno C, Ionescu AC, et al. Knowledge and attitudes on oral health of women during pregnancy and their children: an online survey. BMC Oral Health. 2024;24(1):85. doi:10.1186/s12903-023-03732-2
- Keirse MJNC, Plutzer K. Women’s attitudes to and perceptions of oral health and dental care during pregnancy. J Perinat Med. 2010;38(1):3–8. doi:10.1515/jpm.2010.007
- Barman D, Ranjan R, Kundu A. Factors associated with dental visit and barriers to the utilization of dental services among tribal pregnant women in Khurda district, Bhubaneswar: a cross-sectional study. J Indian Soc Periodontol. 2019;23(6):562–568. doi:10.4103/jisp.jisp_704_18
- Fayed AA, Wahabi H, Mamdouh H, et al. Demographic profile and pregnancy outcomes of adolescents and older mothers in Saudi Arabia: analysis from Riyadh Mother (RAHMA) and Baby cohort study. BMJ Open. 2017;7(9):e016501. doi:10.1136/bmjopen-2017-016501
- Alshammari AK, Wahi MM. A narrative review of the prevalence of periodontitis in Saudi Arabia: a proposal for a national oral health research agenda for vision 2030. Open Dent J. 2019;13(1):171–176. doi:10.2174/1874210601913010171
- Steinberg BJ, Hilton IV, Iida H, et al. Oral health and dental care during pregnancy. Dent Clin North Am. 2013;57(2):195–210. doi:10.1016/j.cden.2013.01.002
- Kurien S, Kattimani VS, Sriram RR, et al. Management of pregnant patient in dentistry. J Int Oral Health. 2013;5(1):88–97.
- Ressler-Maerlender J, Krishna R, Robison V. Oral health during pregnancy: current research. J Womens Health. 2005;14(10):880–882. doi:10.1089/jwh.2005.14.880
- Rocha JS, Arima LY, Werneck RI, et al. Determinants of dental care attendance during pregnancy: a systematic review. Caries Res. 2018;52(1–2):139–152. doi:10.1159/000481407
- Albasry Z, Alhaddad B, Benrashed MA, et al. A cross-sectional analysis of dental care utilization among pregnant women in Saudi Arabia. Open Access Maced J Med Sci. 2019;7(23):4131–4136. doi:10.3889/oamjms.2019.870
- Adeyemi OJ, Gill TL, Paul R, et al. Evaluating the association of self-reported psychological distress and self-rated health on survival times among women with breast cancer in the U.S. PLoS One. 2021;16(12):e0260481. doi:10.1371/journal.pone.0260481
- World Health Organization. Trends in maternal mortality 2000 to 2017: estimates by WHO, UNICEF, UNFPA, world bank group and the united nations population division; 2019. Available from: https://www.unfpa.org/sites/default/files/pub-pdf/Maternal_mortality_report.pdf. Accessed May 25, 2024.
- Alrumayh A, Alfuhaid F, Sayed AJ, et al. Maternal periodontal disease: a possible risk factor for adverse pregnancy outcomes in the Qassim region of Saudi Arabia. J Pharm Bioallied Sci. 2021;13(Suppl 2):1723. doi:10.4103/jpbs.JPBS_838_20
- Laine MA. Effect of pregnancy on periodontal and dental health. Acta Odontol Scand. 2002;60(5):257–264. doi:10.1080/00016350260248210
- Bobetsis YA, Graziani F, Gürsoy M, et al. Periodontal disease and adverse pregnancy outcomes. Periodontol. 2000;83(1):154–174. doi:10.1111/prd.12294
- Komine-Aizawa S, Aizawa S, Hayakawa S. Periodontal diseases and adverse pregnancy outcomes. J Obstet Gynaecol Res. 2019;45(1):5–12. doi:10.1111/jog.13782
- Crump C, Sundquist J, McLaughlin MA, et al. Adverse pregnancy outcomes and long term risk of ischemic heart disease in mothers: national cohort and co-sibling study. BMJ. 2023;380:e072112. doi:10.1136/bmj-2022-072112
- Koberova R, Radochova V, Zemankova J, et al. Evaluation of the risk factors of dental caries in children with very low birth weight and normal birth weight. BMC Oral Health. 2021;21(1):11. doi:10.1186/s12903-020-01372-4
- Boggess KA, Urlaub DM, Moos MK, et al. Knowledge and beliefs regarding oral health among pregnant women. J Am Dent Assoc. 2011;142(11):1275–1282. doi:10.14219/jada.archive.2011.0113
- Penmetsa GS, Meghana K, Bhavana P, et al. Awareness, attitude and knowledge regarding oral health among pregnant women: a comparative study. Niger Med J. 2018;59(6):70–73. doi:10.4103/nmj.NMJ_151_18
- Sukkarwalla A, Tanwir F, Khan S. Assessment of knowledge, attitude and behavior of pregnant women in Pakistan towards oral hygiene-A cross-sectional study. SMU Med J. 2015;1604(2):50–66.
- Togoo RA, Al-Almai B, Al-Hamdi F, et al. Knowledge of pregnant women about pregnancy gingivitis and children oral health. Eur J Dent. 2019;13(2):261–270. doi:10.1055/s-0039-1693236
- Gaffar BO, El Tantawi M, Al-Ansari A, et al. Association between oral health knowledge and practices of Saudi pregnant women in Dammam, Saudi Arabia. East Mediterr Health J. 2016;22(6):411–416. doi:10.26719/2016.22.6.411
- Lazaridi I, Zekeridou A, Schaub L, et al. A survey on oral health knowledge, attitudes and practices of pregnant women attending four general health hospitals in Switzerland. Oral Health Prev Dent. 2022;20(1):33–40. doi:10.3290/j.ohpd.b2573007
- Farmer J, Phillips RC, Singhal S, et al. Inequalities in oral health: understanding the contributions of education and income. Can J Public Health. 2017;108(3):e240–e245. doi:10.17269/CJPH.108.5929
- Bernabe E, Marcenes W, Hernandez CR, et al.; GBD 2017 Oral Disorders Collaborators. Global, regional, and national levels and trends in burden of oral conditions from 1990 to 2017: a systematic analysis for the global burden of disease 2017 study. J Dent Res. 2020;99(4):362–373. doi:10.1177/0022034520908533
- Madianos PN, Bobetsis YA, Offenbacher S. Adverse pregnancy outcomes (APOs) and periodontal disease: pathogenic mechanisms. J Periodontol. 2013;84(4 Suppl):S170–S180. doi:10.1902/jop.2013.1340015
- Graner S, Klingberg-Allvin M, Duong le Q, et al. Pregnant women’s perception on signs and symptoms during pregnancy and maternal health care in a rural low-resource setting. Acta Obstet Gynecol Scand. 2013;92(9):1094–1100. doi:10.1111/aogs.12170
- Khalaf SA, Osman SR, Abbas AM, et al. Knowledge, attitude and practice of oral healthcare among pregnant women in Assiut, Egypt. Int J Community Med Public Health. 2018;5(3):890–900. doi:10.18203/2394-6040.ijcmph20180743
- Swathi K, Koothati RK, Motor RR, et al. Knowledge and experience of women about dental services utilization during pregnancy: a cross-sectional questionnaire study. J Pharm Bioallied Sci. 2021;13(Suppl 2):2.
- Marla V, Srii R, Roy DK, et al. The Importance of oral health during pregnancy: a review. Méd Express. 2018;5:1–6.
- Vt H, Nisha AV. Dental considerations in pregnancy-a critical review on the oral care. J Clin Diagn Res. 2013;7(5):948–953. doi:10.7860/JCDR/2013/5405.2986
- Bao J, Huang X, Wang L, et al. Clinical practice guidelines for oral health care during pregnancy: a systematic evaluation and summary recommendations for general dental practitioners. Quintessence Int. 2022;53(4):362–373. doi:10.3290/j.qi.b2644863
- Zhong C, Ma KN, Wong YS, et al. Oral health knowledge of pregnant women on pregnancy gingivitis and children’s oral health. J Clin Pediatr Dent. 2015;39(2):105–108. doi:10.17796/jcpd.39.2.n66w635638w643n7
- Ekiz D, Ekiz A, Özköse B, et al. Questionnaire on mouth and dental health during pregnancy: myths and facts. Perinat J. 2015;23(4):180–185. doi:10.2399/prn.15.0233010
- American Dental Association Oral Health topics: pregnancy: key points: ADA policies related to pregnancy: dental treatment during pregnancy [Trans.2014:508]; 2014. Available from: https://www.ada.org/en/member-center/oral-health-topics/pregnancy. Accessed March 8, 2021.
- American College of Obstetricians and Gynecologists. Committee on health care for underserved women committee opinion 569: oral health care during pregnancy and through the lifespan. Obstet Gynecol. 2013;122(2):417–422. doi:10.1097/01.AOG.0000433007.16843.10
- National Maternal and Child Oral Health Resource Center. Promoting Oral Health During Pregnancy: Update on Activities—May 2020. Washington, DC, USA: National Maternal and Child Oral Health Resource Center; 2020.
- Abuhaloob L, MacGillivray S, Mossey P, et al. Maternal and child oral health interventions in Middle East and North Africa regions: a rapid review. Int Dent J. 2019;69(6):409–418. doi:10.1111/idj.12506