
Abstract
Objective
The objective of this review was to summarize evidence for the effectiveness of music therapy (MT) and to assess the quality of systematic reviews (SRs) based on randomized controlled trials (RCTs).
Study design
An SR of SRs based on RCTs.
Methods
Studies were eligible if they were RCTs. Studies included were those with at least one treatment group in which MT was applied. We searched the following databases from 1995 to October 1, 2012: MEDLINE via PubMed, CINAHL (Cumulative Index of Nursing and Allied Health Literature), Web of Science, Global Health Library, and Ichushi-Web. We also searched all Cochrane Database and Campbell Systematic Reviews up to October 1, 2012. Based on the International Classification of Diseases, 10th revision, we identified a disease targeted for each article.
Results
Twenty-one studies met all inclusion criteria. This study included 16 Cochrane reviews. As a whole, the quality of the articles was very good. Eight studies were about “Mental and behavioural disorders (F00-99)”; there were two studies on “Diseases of the nervous system (G00-99)” and “Diseases of the respiratory system (J00-99)”; and there was one study each for “Endocrine, nutritional and metabolic diseases (E00-90)”, “Diseases of the circulatory system (I00-99)”, and “Pregnancy, childbirth and the puerperium (O60)”. MT treatment improved the following: global and social functioning in schizophrenia and/or serious mental disorders, gait and related activities in Parkinson’s disease, depressive symptoms, and sleep quality.
Conclusion
This comprehensive summary of SRs demonstrated that MT treatment improved the following: global and social functioning in schizophrenia and/or serious mental disorders, gait and related activities in Parkinson’s disease, depressive symptoms, and sleep quality. MT may have the potential for improving other diseases, but there is not enough evidence at present. Most importantly, no specific adverse effect or harmful phenomenon occurred in any of the studies, and MT was well tolerated by almost all patients.
Article focus
Although many studies have reported the effects of music therapy (MT), there is no review of systematic reviews (SRs) based on randomized controlled trials (RCTs).
Key messages
The key messages of this paper are as follows.
This is the first SR of SRs of the effectiveness of cure based on music interventions in studies with RCT designs.
Our study is unique because it summarizes the evidence for each target disease according to the International Classification of Diseases, revision 10 (ICD-10).
We propose the future research agenda for studies on the treatment effect of MT.
Strength and limitation of this study
The strengths of this study are as follows: 1) the methods and implementation registered high on the PROSPERO database; 2) it was a comprehensive search strategy across multiple databases with no data restrictions; and 3) there were high agreement levels for quality assessment of articles.
This study has three limitations. Firstly, some selection criteria were common across studies; however, the bias remained due to differences in eligibility for participation in each original RCT. Secondly, publication bias was a limitation. Lastly, since this review focused on summarizing the effects of MT for each disease, we did not describe all details on quality and quantity, such as type of MT, frequency of MT, and time on MT.
Introduction
MT is widely utilized for treatment of and assistance in various diseases. In one literature review, the authors found seven case reports/series and seven studies on MT for multiple sclerosis patients. The results of these studies as well as the case reports demonstrated patients’ improvements in the domains of self-acceptance, anxiety, and depression.Citation1 Another review examined the overall efficacy of MT in children and adolescents with psychopathology, and examined how the size of the effect of MT is influenced by the type of pathology, the subject’s age, the MT approach, and the type of outcome.Citation2 The analysis revealed that MT had a medium to large positive effect (effect size =0.61) on clinically relevant outcomes that was statistically highly significant (P<0.001) and statistically homogeneous. A more recent SR assessed the effects of musical elements in the treatment of individuals with acquired neurological disorder.Citation3 The results showed that mechanisms of recovery remained unclear: two of the three studies that examined mechanisms of recovery via neuro-imaging techniques supported the role of the right hemisphere, but reports were contradictory, and exact mechanisms of recovery remained indefinable. An interesting meta-analysis described results that justified strong consideration for the inclusion of neonatal intensive care unit (NICU) MT protocols in best practice standards for NICU treatment of preterm infants: examples of these therapies were listening to music for pacification, music reinforcement of sucking/feeding ability, and music as a basis for pacification during multilayered, multimodal stimulation.Citation4
Examining the curative effects of MT has unique challenges. A review article by NilssonCitation5 described how nurses face many challenges as they care for the needs of hospitalized patients, and that they often have to prioritize physical care over the patient’s emotional, spiritual, and psychological needs. In clinical practice, music intervention can be a tool to support these needs by creating an environment that stimulates and maintains relaxation, wellbeing, and comfort. Furthermore, the Nilsson articleCitation5 presented a concrete recommendation for music interventions in clinical practice, such as “slow and flowing music, approximately 60 to 80 beats per minute”, “nonlyrical”, “maximum volume level at 60 dB”, “patient’s own choice, with guidance”, “suitable equipment chosen for the specific situation”, “a minimum duration of 30 minutes in length”, and “measurement, follow up, and documentation of the effects”. In addition, MT has been variably applied as both a primary and accessory treatment for persons with addictions to alcohol, tobacco, and other drugs of abuse. However, an SRCitation6 described that no consensus exists regarding the efficacy of MT as treatment for patients with addictions.
On the other hand, music may be considered an adjunctive therapy in clinical situations. Music is effective in reducing anxiety and pain in children undergoing medical and dental procedures.Citation7 A meta-analysis confirmed that patients listening to music during colonoscopy, which is now the recommended method for screening colon cancer, was an effective method for reducing procedure time, anxiety, and the amount of sedation. More importantly, no harmful effects were observed for all the target studies.Citation8 The usual practice following a cervical cancer abnormal cervical smear is to perform a colposcopy. However, women experience high levels of anxiety and negative emotional responses at all stages of cervical screening. An SR of RCTs evaluated interventions designed to reduce anxiety levels during colposcopic examination. Psychosexual dysfunction (ie, anxiety) was reduced by playing music during colposcopy.Citation9
The definition of musical intervention is complex, but the literature describes two broad categories of music interventions: music medicine and MT.Citation10 Music medicine is the use of passive listening (usually involving prerecorded music) as implemented by medical personnel. In music medicine studies, the subject’s preference for the music used may be considered by having him or her select from a variety of tapes. Alternately, some studies use predefined music stimuli that do not take the subject’s preferences into account. Furthermore, there is generally no attempt by the researcher to form a therapeutic relationship with the subject, and there is no process involved in the music treatment. In essence, music medicine studies usually allow one to assess the effects of music alone as a therapeutic intervention. In contrast, MT interventions most often involve a relationship between the therapist and the subject, the use of live music (performed or created by the therapist and/or patient), and a process that includes assessment, treatment, and evaluation. Patient preference for the music is usually a consideration in MT studies.
We were interested in evaluating the curative effect of MT according to diseases because many of the primary studies and review articles of much MT have reported results in this way. In particular, we wanted to focus on all cure and rehabilitation effects using the ICD-10. It is well known in research design that evidence grading is highest for an SR with meta-analysis of RCTs. Although many studies have reported the effects of MT, there is no review of SRs based on RCTs. The objective of this review was to summarize evidence for the effectiveness of MT and to assess the quality of SRs based on RCTs of these therapies.
Methods
Criteria for considering studies included in this review
Types of studies
Studies were eligible if they were SRs (with or without a meta-analysis) based on RCTs.
Types of participants
There was no restriction on patients.
Types of intervention and language
Studies included were those with at least one treatment group in which MT was applied. The definition of MT is complex, but in this study, any kind of MT (not only music appreciation but also musical instrument performance and singing, for example) was permitted and defined as an intervention. Studies had to include information on the use of medication, alternative therapies, and lifestyle changes, and these had to be comparable among groups. There was no restriction on the basis of language.
Types of outcome measures
We focused on all cure and rehabilitation effects using the ICD-10.
Search methods for studies identification
Bibliographic database
We searched the following databases from 1995 to October 1, 2012: MEDLINE via PubMed, Cumulative Index of Nursing and Allied Health Literature (CINAHL), Web of Science, Ichushi Web (in Japanese), the Global Health Library (GHL), and the Western Pacific Region Index Medicus (WPRIM). The International Committee of Medical Journal Editors (ICMJE) recommended uniform requirements for manuscripts submitted to biomedical journals in 1993. We selected articles published (that included a protocol) since 1995, because it appeared that the ICMJE recommendation had been adopted by the relevant researchers and had strengthened the quality of the reports.
We also searched the Cochrane Database of Systematic Reviews (Cochrane Reviews), the Database of Abstracts of Reviews of Effects (Other Reviews), the Cochrane Central Register of Controlled Trials (Clinical Trials or CENTRAL), the Cochrane Methodology Register (Methods Studies), the Health Technology Assessment Database (Technology Assessments), the NHS Economic Evaluation Database (Economic Evaluations), About The Cochrane Collaboration databases (Cochrane Groups), the Campbell Systematic Reviews (the Campbell Collaboration), and the All Cochrane, up to October 1, 2012.
All searches were performed by two specific searchers (hospital librarians) who were qualified in medical information handling, and who were experienced in searches of clinical trials.
Search strategies
The special search strategies contained the elements and terms for MEDLINE, CINAHL, Web of Science, Ichushi Web, GHL, WPRIM, and All Cochrane databases ( and ). Only keywords about intervention were used for the searches. First, titles and abstracts of identified published articles were reviewed in order to determine the relevance of the articles. Next, references in relevant studies and identified SRs were screened.
Figure 1 Flowchart of trial process.
Abbreviations: CINAHL, Cumulative Index of Nursing and Allied Health Literature; CENTRAL, Cochrane Central Register of Controlled Trials; RCT, randomized controlled trial; SR, systematic review.
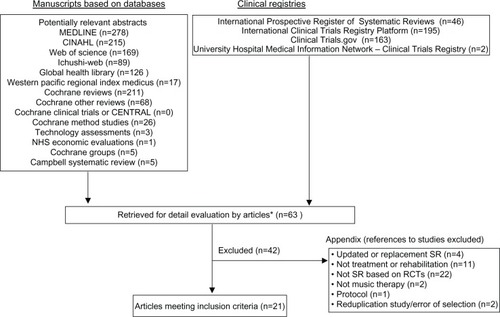
Table 1 The special search strategies
Registry checking
We searched the International Clinical Trials Registry Platform (ICTRP), ClinicalTrials.gov, and the University Hospital Medical Information Network – Clinical Trials Registry (UMIN-CTR), up to October 1, 2012.
ICTRP in the WHO Registry Network meet specific criteria for content, quality and validity, accessibility, unique identification, technical capacity, and administration. Primary registries meet the requirements of the ICMJE. Clinical ClinicalTrials.gov is a registry of federally and privately supported clinical trials conducted in the US and around the world. UMIN-CTR is a registry of clinical trials conducted in Japan and around the world.
Handsearching and reference checking
We handsearched abstracts published on MT in relevant journals in Japan. We checked the references of included studies for further relevant literature.
Review methods
Selection of trials
To make the final selection of studies for the review, all criteria were applied independently by four authors (ie, TH, JK, SJP, and TA) to the full text of articles that had passed the first eligibility screening (). Disagreements and uncertainties were resolved by discussion with other authors (ie, HK, KT, and YM).
Studies were selected when 1) the design was an SR based on RCTs and 2) one of the interventions was a form of MT. Protocols without results were excluded, and we included only completed studies. Cure and rehabilitation effects were used as a primary outcome measure. Trials that were excluded are presented with reasons for exclusion ().
Quality assessment of included studies
To ensure that variation was not caused by systematic errors in the study design or execution, eleven review authors (HP, MY, HO, SO, SJP, TO, KT, TH, SH, JK, and HK) independently assessed the quality of the articles. A full quality appraisal of these papers was made using the combined tool based on the AMSTAR checklistCitation11 developed to assess the methodological quality of SRs.
Each item was scored as “present” (Yes), “absent” (No), “unclear or inadequately described” (Can not answer), or “not applicable” (n/a). Depending on the study design, some items were not applicable. The “n/a” was excluded from calculation for quality assessment. We displayed the percentage of descriptions that were present on all items for the quality assessment of articles. Then, based on the percentage of risk of poor methodology and/or bias, each item was assigned to one of the following categories: good description (80%–100%), poor description (50%–79%), or very poor description (0%–49%).
Disagreements and uncertainties were resolved by discussion with other authors (ie, KT and HK). Inter-rater reliability was calculated on a dichotomous scale using percentage agreement and Cohen’s kappa coefficient (κ).
Summary of studies and data extraction
Eleven review authors (HP, MY, HO, SO, SJP, TH, TO, SH, JK, KT, and HK) described the summary from each article based on the structured abstracts.Citation12,Citation13
Benefit and harm
The GRADE Working GroupCitation14 reported that the balance between benefit and harm, quality of evidence, applicability, and the certainty of the baseline risk were all considered in judgments about the strength of recommendations. Adverse events for intervention were especially important information for researchers and users of clinical practice guidelines, and we presented this information with the description of each article.
Research protocol registration
We submitted and registered our research protocol to the PROSPERO (no 42012002950). PROSPERO is an international database of prospectively registered SRs in health and social care.Citation15 Key features from the review protocol are recorded and maintained as a permanent record in PROSPERO. This provides a comprehensive listing of SRs registered at inception, and enables comparison of reported review findings with what was planned in the protocol. PROSPERO is managed by UK Centre for Reviews and Dissemination (CRD) and funded by the UK National Institute for Health Research. Registration was recommended because it encourage full publication of the review’s findings and transparency in changes to methods that could bias findings.Citation16
Results
Study selection
The literature searches included potentially relevant articles (). Abstracts from those articles were assessed, and 63 papers were retrieved for further evaluation (checks for relevant literature). Forty-two publications were excluded because they did not meet the eligibility criteria (). A total of 21 studiesCitation17–Citation37 met all inclusion criteria (). The language of all eligible publications was English.
Study characteristics
The contents of all articles were summarized as structured abstracts (). Sinha et alCitation17 reported that there was no evidence that auditory integration therapy or other sound therapies are effective as treatments for autism spectrum disorders. Mossler et alCitation18 concluded that MT as an addition to standard care helps people with schizophrenia to improve their global state, mental state (including negative symptoms), and social functioning if a sufficient number of MT sessions are provided by qualified music therapists. Bradt et alCitation19 indicated that music interventions may have beneficial effects on anxiety, pain, mood, and quality of life (QoL) in people with cancer. Bradt and DileoCitation20 reported that there may be a benefit of MT on QoL of people in end-of-life care. Vink et alCitation21 reported that the methodological quality and the reporting of the included studies on dementia were too poor to draw any useful conclusions. Bradt et alCitation22 indicated that listening to music may have a beneficial effect on heart rate, respiratory rate, and anxiety in mechanically ventilated patients. Cepeda et alCitation23 reported that listening to music reduces pain intensity levels and opioid requirements on patients with chronic, acute, neuropathic, and cancer pain or experimental pain, but the magnitude of these benefits is small and therefore its clinical importance unclear. Bradt et alCitation24 reported that rhythmic auditory stimulation might be beneficial for gait improvement in people with stroke. Gold et alCitation25 indicated that MT may help children with autistic spectrum disorder to improve their communicative skills. Laopaiboon et alCitation26 indicated that music during planned cesarean section under regional anesthesia may improve pulse rate and birth satisfaction score. Bradt and DileoCitation27 reported that listening to music may have a beneficial effect on blood pressure, heart rate, respiratory rate, anxiety, and pain in persons with coronary heart disease. Maratos et alCitation28 suggested that MT is accepted by people with depression and is associated with improvements in mood, but the small number and low methodological quality of studies meant that it is not possible to be confident about its effectiveness. de Dreu et alCitation29 reported that music-based movement therapy appeared promising for the improvement of gait and gait-related activities in Parkinson’s disease. Cogo-Moreira et alCitation30 concluded that there is no evidence available on which to base a judgment about the effectiveness of music education for the improvement of reading skills in children and adolescents with dyslexia. Drahota et alCitation31 reported that music may improve patient-reported outcomes in certain circumstances such as anxiety for hospital patients. Chan et alCitation32 concluded that listening to music over a period of time helps to reduce depressive symptoms in the adult population. Naylor et alCitation33 reported that there is limited qualitative evidence to support the effectiveness of music on health-related outcomes for children and adolescents with clinical diagnoses. Irons et alCitation34 concluded that because no studies that met the criteria were found, their review was unable to support or refute the benefits of singing as a therapy for people with cystic fibrosis. Irons et alCitation35 reported that they could not draw any conclusion to support or refute the adoption of singing as an intervention for people with bronchiectasis because of the absence of data. de Niet et alCitation36 concluded that music-assisted relaxation could be without intensive investment in training and materials and is therefore cheap, easily available and can be used by nurses to promote music-assisted relaxation to improve sleep quality. Gold et alCitation37 reported that MT is an effective treatment which helps people with psychotic and nonpsychotic severe mental disorders to improve global state, symptoms, and functioning.
Table 2 A structured abstract of 21 systematic reviews
Based on ICD-10, we identified a disease targeted in each article (). Among 21 studies, eight studies were about “Mental and behavioural disorders (F00-99)”. There were two studies in “Diseases of the nervous system (G00-99)” and “Diseases of the respiratory system (J00-99)”, and one study in “Endocrine, nutritional and metabolic diseases (E00-90)”, “Diseases of the circulatory system (I00-99)”, and “Pregnancy, childbirth and the puerperium (O60)”. Because there were a variety of target diseases, there were six articles in which we could not identify a single disease.
Table 3 International classification of target diseases in each article
Evidence of effectiveness
presents a brief summary of 21 SRs. Five studies (ie, schizophrenia for global and mental state and social functioning,Citation18 Parkinson’s disease for gait and related activities,Citation29 depressive symptoms,Citation32 sleep quality,Citation36 and serious mental disorders for global and social functioningCitation37) concluded that there are effects of the intervention.
Table 4 Brief summary of 21 systematic reviews
Ten studies with a meta-analysis (ie, cancer for anxiety, pain, mood, and QoL,Citation19 advanced life-limiting illness for QoL,Citation20 mechanically ventilated patients for heart rate, respiratory rate, and anxiety,Citation22 multiple pain for intensity level and opioid requirement,Citation23 acquired brain injury for gait parameters,Citation24 autistic spectrum disorders for communicative skills,Citation25 cesarean section for heart rate and birth satisfaction,Citation26 coronary heart disease for blood pressure, heart rate, respiratory rate, anxiety, and pain,Citation27 hospital patients for self-reported outcomes such as anxiety,Citation31 and various clinical conditions for health outcomes in children with learning and developmental disorderCitation33) concluded that there might be an effect of the intervention. An SR without a meta-analysis of depression reported that there might be an effect of the intervention.Citation28
Two studies (ie, autism spectrum17 and dementiaCitation21) described that the effect of intervention is unclear. There was no evidence for three studies (ie, dyslexia,Citation30 cystic fibrosis,Citation34 and bronchiectasisCitation35) because they were not RCTs.
Adverse events
There were no specific adverse events in any of the studies.
Quality assessment
We evaluated eleven items from the AMSTAR checklist in more detail (). Inter-rater reliability metrics for the quality assessment indicated substantial agreement for all 231 items (percentage agreement 95.3% and κ=0.825). As a whole, the quality of the articles was very good.
Table 5 AMSTAR is a measurement tool created to assess the methodological quality of systematic reviews
Discussion
This is the first SR of SRs of the effectiveness of cure based on music interventions in studies with RCT designs. Our study is unique because it summarized the evidence for each target disease according to ICD-10 classification. We assume that this study will be helpful to researchers who want to grasp an effect of MT comprehensively and could provide information that is indispensable for the organization that is going to make the guidelines according to each disease.
Twenty-one SRs based on RCTs were identified, and music intervention was clearly effective for five diseases (ie, schizophrenia for global and mental state and social functioning, Parkinson’s disease for gait and related activities, depressive symptoms, sleep quality, and serious mental disorders for global and social functioning).
A review of all SRs showed that there was no special adverse effect or harm associated with MT.
Tendency of target disease and outcome
The most commonly reported target diseases were “Mental and behavioural disorders (F00-99)”,Citation17,Citation18,Citation21,Citation25,Citation28,Citation30,Citation32,Citation36 and the effect of MT on these diseases was improved mental health (eg, anxiety and mood), pain, QoL, and communication skills. The main reason given in these articles for improved mental health was that the beauty and rhythm of the music tone allowed the patient to be comfortable. In studies about the effects of MT on anxiety, discomfort, fear, and pain, MT has been variably applied as an accessory treatment for persons with addictions,Citation6 and as evasion of direct discomfort for undergoing medical device procedures such as colonoscopy,Citation8 colposcopyCitation9 and dental procedures.Citation7
The second most frequently reported target diseases were “Diseases of the nervous system (G00-99)”,Citation24,Citation29 and the effects of MT on these diseases showed commonly gait parameters. MT is expected to improve gait and related activities such as rehabilitation in diseases of the central nervous system. There were also several studies that identified “Diseases of the respiratory system (J00-99).”Citation22,Citation35 Improvements seen in these studies were mainly due to effects of singing on breathing function, such as respiratory rate, and on the circulation function, such as heart rate.
Validity of overall evidence based on quality assessment
We performed an evaluation of all SRs by the AMSTAR checklist developed to assess the methodological quality of SRs. There were no serious problems with the conduct and reporting of all target studies. This study included 16 Cochrane Reviews.Citation17–Citation28,Citation30,Citation31,Citation34,Citation35 In the Cochrane Reviews, the eligibility criteria for a meta-analysis are strict, and for each article, heterogeneity and low quality of reporting are to first be excluded. Therefore, we assumed that the conclusion of each SR had enough validity.
Overall evidence
Most importantly, a specific adverse effect or harmful phenomenon did not occur in any study, and MT was well tolerated by almost all patients. MT treatment has positive effects for the following: schizophrenia and/or serious mental disorders for global and social functioning, Parkinson’s disease for gait and related activities, depressive symptoms, and sleep quality. We assume that the direct effects of MT are generally improvement of mental health and sense of rhythm, and reduction of pain. In addition, we assume that communication with other people improves through music, the sense of isolation disappears, and QoL rises.
Although further accumulation of RCT data is necessary, MT may be effective treatment for the following diseases and symptoms: cancer and/or advanced life-limiting illnesses affecting mental state and QoL, mechanically ventilated patients with impaired respiratory function and mental state, chronic pain requiring opioid treatment, acquired brain injury affecting gait parameters, autistic spectrum disorders involving communicative skills, cesarean section effects on heart rate and birth satisfaction, coronary heart disease effects on circulatory, respiratory function, and mental state, and self-reported outcomes for hospitalized patients and other patients with various clinical conditions. These SRs describe the need for additional high quality RCTs to assess the effect of MT.
Future research agenda to build evidence
shows the future research agenda for studies on the treatment effect of MT. Because only SRs of RCTs were included in this study, their characteristic study designs limited our results to the assessment of short-term effects. Even if a study is not an RCT design, it is necessary to evaluate the long-term effects.
Table 6 Future research agenda to build evidence of music therapy
Because studies of intervention using music vary in design, a consensus of the framework is necessary.Citation10 In this study, examination according to a detailed intervention method was not possible, but it would be important for future studies to define MT. Furthermore, studies to assess dose–response relationships according to each disease are clearly necessary.Citation18
Bowen et alCitation38 suggested that public health is moving toward the goal of implementing evidence-based intervention. However, the feasibility of possible interventions and whether comprehensive and multilevel evaluations are needed to justify them must be determined. It is at least necessary to show the cost of such interventions. We must introduce an interventional method based on its cost-benefit, cost-effectiveness, and cost-utility.
In addition, MT as an intervention is unique and completely different than pharmacological or traditional rehabilitation methods. Therefore, it may be necessary to add some original items like herbal intervention,Citation39 aquatic exercise,Citation40 and balneotherapyCitation41 to the CONSORT 2010 checklist as alternative or complementary medicines.
Strength and limitations
This review has several strengths: 1) the methods and implementation registered high on the PROSPERO database; 2) it was a comprehensive search strategy across multiple databases with no data restrictions; 3) there were high agreement levels for quality assessment of articles; and 4) it involved detailed data extraction to allow for collecting all articles’ content into a recommended structured abstract.
This review also had several limitations that should be acknowledged. Firstly, some selection criteria were common across studies, as described above; however, bias remained due to differences in eligibility for participation in each original RCT. Secondly, publication bias was a limitation. Although there was no linguistic restriction in the eligibility criteria, we searched studies with only English and Japanese keywords. Thirdly, in order to be specific to SRs based on RCTs, it ignores some excellent results of primary research by other research designs. Fourthly, as a point of terminology for MT, because we applied a broad definition to the use of music in medicine, it may be more confusing or a bit misleading in the cultural context of Western health care.
In addition, since this review focused on summaries of effects of MT for each disease, we did not describe all details on quality and quantity such as type of MT, frequency of MT, and time on MT. Moreover, we could not follow standard procedures as estimates of the effects of moderating variables. Finally, because we broadly defined MT as music appreciation, musical instrument performance, and singing, we could not assess a specific intervention.
Conclusion
This comprehensive summary of SRs demonstrates that MT treatment improved the following: global and social functioning in schizophrenia and/or serious mental disorders, gait and related activities in Parkinson’s disease, depressive symptoms, and sleep quality. MT may have the potential for improving other diseases, but there is not enough evidence at present. Most importantly, a specific adverse effect or harmful phenomenon did not occur in any of the studies, and MT was well tolerated by almost all patients.
To most effectively assess the potential benefits of MT, it will be important for future research to explore 1) long-term effects, 2) a consensus of the framework of music intervention, 3) dose–response relationships, 4) the cost of the intervention, and 5) development of the original check item in MT.
Author contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data. All authors took part in drafting the article or revising it critically for important intellectual content.
Ethical approval
No ethical approval was required.
Data sharing
No additional data are available.
Acknowledgments
We would like to express our appreciation to Ms Aya Maruyama (methodology of MT), Ms Rie Higashino, Ms Yoko Ikezaki, Ms Rinako Kai (paperwork), and Ms Satoko Sayama and Ms Mari Makishi (all searches of studies) for their assistance in this study.
Supplementary material
Table S1 References to studies excluded in this review
Funding
This study was supported by the Health and Labour Sciences Research Grants (Research on Health Security Control ID No H24-021; representative Dr K Tsutani) from the Japanese Ministry of Health, Labour and Welfare of Japan in 2012.
Disclosure
The authors report no conflicts of interest in this work.
References
- OstermannTSchmidWMusic therapy in the treatment of multiple sclerosis: a comprehensive literature reviewExpert Rev Neurother2006646947716623646
- GoldCVoracekMWigramTEffects of music therapy for children and adolescents with psychopathology: a meta-analysisJ Child Psychol Psychiatry2004451054106315257662
- HurkmansJde BruijnMBoonstraAMMusic in the treatment of neurological language and speech disorder: a systematic reviewAphasiology201226119
- StandleyJMusic therapy research in the NICU: an updated meta-analysisNeonatal Network20123131131622908052
- NilssonUThe anxiety- and pain-reducing effects of music interventions: a systematic reviewAORN J20088778080718395022
- MaysKLClarkDLGordonAJTreating addiction with tunes: a systematic review of music therapy for the treatment of patients with addictionsSubstance Abuse200829515919042198
- KlassenJALiangYTjosvoldLKlassenTPHartlingLMusic for pain and anxiety in children undergoing medical procedures: a systematic review of randomized controlled trialsAmbul Pediatr2008811712818355741
- TamWWSWongELYTwinnSFEffect of music on procedure time and sedation during colonoscopy: a meta-analysisWorld J Gastroenterol2008145336534318785289
- GalaalKBryantADeaneKHAl-KhaduriMLopesADInterventions for reducing anxiety in women undergoing colposcopyCochrane Database Syst Rev201112CD00601322161395
- DileoCEffects of music and music therapy on medical patients: a meta-analysis of the research and implications for the futureJ Soc Integr Oncol20064677019442338
- SheaBJGrimshawJMWellsGADevelopment of AMSTAR: a measurement tool to assess the methodological quality of systematic reviewsBMC Med Res Methodol200771017302989
- HopewellSClarkeMMoherDCONSORT for reporting randomized trials in journal and conference abstractsLancet200837128128318221781
- HopewellSRavaudPBaronGEffect of editors’ implementation of CONSORT guidelines on the reporting of abstracts in high impact medical journals: interrupted time series analysisBMJ2012344e417822730543
- AtkinsDBestDBrissPAGrading quality of evidence and strength of recommendationsBMJ20043281490149715205295
- International Prospective Register of Systematic Reviews [database on the Internet]York, UKUniversity of York Available from: http://www.crd.york.ac.uk/prosperoAccessed June 20, 2012
- BoothAClarkeMGhersiDAn international registry of systematic review protocolsLancet201137710810920630580
- SinhaYSiloveNHayenAWilliamsKAuditory integration training and other sound therapies for autism spectrum disorders (ASD)Cochrane Database Syst Rev201112CD00368122161380
- MosslerKChenXHeldalTOMusic therapy for people with schizophrenia and schizophrenia-like disordersCochrane Database Syst Rev201112CD00402522161383
- BradtJDileoCGrockeDMusic interventions for autistic spectrum disorderCochrane Database Syst Rev20118CD00691121833957
- BradtJDileoCMusic therapy for end-of-life careCochrane Database Syst Rev20101CD00716920091619
- VinkACBirksJSBruinsmaMSScholtenRJMusic therapy for people with dementiaCochrane Database Syst Rev20034CD003477
- BradtJDileoCGrockeDMusic interventions for mechanically ventilated patientsCochrane Database Syst Rev201012CD00690221154376
- CepedaMSCarrDBLauJMusic for pain reliefCochrane Database Syst Rev20062CD00484316625614
- BradtJMageeWLDileoCMusic interventions for acquired brain injuryCochrane Database Syst Rev20107CD00678720614449
- GoldCWigramTElefantCMusic therapy for autistic spectrum disorderCochrane Database Syst Rev20062CD00438116625601
- LaopaiboonMLumbiganonPMartisRMusic during caesarean section under regional anaesthesia for improving maternal and infant outcomesCochrane Database Syst Rev20092CD00691419370660
- BradtJDileoCMusic for stress and anxiety reduction in coronary heart disease patientsCochrane Database Syst Rev20092CD00657719370642
- MaratosAGoldCWangXMusic therapy for depressionCochrane Database Syst Rev20081CD00451718254052
- de DreuMJvan der WilkASPoppeEKwakkelGvan WegenEERehabilitation, exercise therapy and music in patients with Parkinson’s diseases: a meta-analysis of the effects of music-based movement therapy on walking ability, balance and quality of lifeParkinsonism Relat Disord201218Suppl 1S114S11922166406
- Cogo-MoreiraHAndrioloRBYazigiLMusic education for improving reading skills in children and adolescents with dyslexiaCochrane Database Syst Rev20128CD00913322895983
- DrahotaAWardDMackenzieHSensory environment on health-related outcomes of hospital patientsCochrane Database Syst Rev20123CD00531522419308
- ChanMFWongZYThayalaNVThe effectiveness of music listening in reducing depressive symptoms in adults: a systematic reviewComplement Ther Med20111933234822036525
- NaylorKTKingsnorthSLamontAThe effectiveness of music in pediatric healthcare: a systematic review of randomized controlled trialsEvid Based Complement Alternat Med2011201146475920976017
- IronsJYKennyDTChangABSinging for children and adults with cystic fibrosisCochrane Database Syst Rev20105CD00803620464761
- IronsJYKennyDTChangABSinging for children and adults with bronchiectasisCochrane Database Syst Rev20102CD00772920166097
- de NietGTiemensBLendemeijerBHutschemaekersGMusic-assisted relaxation to improve sleep quality: meta-analysisJ Adv Nurs2009651356136419456998
- GoldCSolliHPKrugerVDose-response relationship in music therapy for people with serious mental disorders: systematic review and meta-analysisClin Psychol Rev20092919320719269725
- BowenDJKreuterMSpringBHow we design feasibility studiesAm J Prev Med20093645245719362699
- GragnierJJBoonHRochonPReporting randomized, controlled trials of herbal interventions: an elaborated CONSORT statementAnn Intern Med200614436436716520478
- KamiokaHTsutaniKOkuizumiHEffectiveness of aquatic exercise and balneotherapy: a summary of systematic reviews based on randomized controlled trials of water immersion therapiesJ Epidemiol20102021219881230
- KamiokaKKawamuraYTsutaniKA checklist to assess the quality of reports on spa therapy and balneotherapy trials was developed using the Delphi consensus method: the SPAC checklistComplement Ther Med201321432433223876563