
Abstract
Multiple sclerosis (MS), a chronic demyelinating neuroinflammatory disease of the central nervous system, is the most common neurological disorder leading to disability in young adulthood. In the last 2 decades, numerous treatments for relapsing–remitting MS have been approved with eleven treatment options available worldwide. One of the determinants in treatment selection is disease activity in the individual patient. However, patient preferences play an increasingly major role in treatment decision making. With teriflunomide, a reversible inhibitor of the enzyme dihydroorotate dehydrogenase, a new oral therapeutic option, given once daily, has been approved within the last 2 years by the regulatory agencies. The current review focuses on characteristics of the drug relevant for patients’ preferences in the treatment decision process in the light of the available medications. Perceiving and considering patients’ preferences will have an effect on treatment adherence, which is known to be often low in MS patients. Teriflunomide-related adherence issues will also be discussed regarding mode of application, dosing, and potential side effects.
Introduction
Multiple sclerosis (MS) is a chronic demyelinating neuroinflammatory disease of the central nervous system, affecting approximately 2 million people worldwide. The etiology is assumed to be multifactorial involving, for example, environment and genetic predisposition, affecting disease development. MS is the most common neurological disorder leading to disability in young adulthood. Clinical disease starts with recurrent and often reversible neurological deficits in early adulthood in the majority of patients. MS can follow three different clinical courses: relapsing–remitting (RR), secondary progressive, and primary progressive MS.
In the past 2 decades, numerous immunoprophylactic and, to a much lesser extent, symptomatic treatments have been approved for MS, especially for RR MS. The disease cannot be cured by the available treatments so far, but a reduction of relapse rate, disease progression and other clinical activity markers, eg, magnetic resonance imaging (MRI) lesions and brain atrophy, could be achieved.
Treatment options in MS
Treatment of relapses as well as immunoprophylactic and symptomatic treatment are the mainstays of modern MS therapy.
For many years, interferon beta preparations and glatiramer acetate () have belonged to the well-established group of injectable immunoprophylactic therapeutics, with a well-known safety profile for use in RR and (interferon beta-1b subcutaneously [sc], interferon beta-1a sc three times per week [tiw]), secondary progressive MS with inflammatory disease activity, which is characterized by relapses. Interferon beta-1b was licensed as the first beta interferon in the US in 1993, and glatiramer acetate in 1996. For MS patients with highly active disease, natalizumab and mitoxantrone have been introduced as further treatment options. In 2010, fingolimod, a sphingosine phosphate receptor agonist, was licensed by the US Food and Drug Administration (FDA) as the first modern oral immunoprophylactic treatment. In most European countries, fingolimod is restricted to patients with high clinical and MRI disease activity.
Table 1 Treatment options for RR MS (in alphabetical order)
Within the last 2 years in the US and European Union, two further oral drugs have been approved: dimethyl fumarate (DMF), given as capsules twice daily (bid); and teriflunomide with a once-daily application. Alemtuzumab was licensed by the European Medicines Agency in 2013 for RR MS, and the FDA approved alemtuzumab in autumn 2014.
In the growing field of currently available disease modifying treatments (DMTs), it is crucial to identify factors for patients’ treatment decisions. The current review focuses on teriflunomide as a new treatment option in RR MS, in particular considering patients’ preference and adherence.
PubMed was searched using the terms “teriflunomide AND multiple sclerosis”, “teriflunomide AND adherence”, “teriflunomide AND preference”, “multiple sclerosis AND adherence”, and “multiple sclerosis AND preference” without time-period restriction. The references of the resulting studies were used to identify additional articles to be included in the review. Additionally, congress abstracts presented in 2014 have been selected.
Teriflunomide – efficacy and safety
Teriflunomide is an immunomodulatory drug with anti-inflammatory properties. In 2012, the FDA approved Teriflunomide 7 mg and 14 mg once daily for the treatment of adult patients with RR MS. In 2013, the 14 mg dose was approved for the treatment of RR MS patients by the European Medicines Agency.
Teriflunomide reversibly inhibits the enzyme dihydroorotate dehydrogenase – a key enzyme for the de novo synthesis of pyrimidine – thus leading to a reduced proliferation of autoreactive T- and B-cell clones. Resting and slowly proliferating cells can fulfil their demand from the existing pyrimidine pool and remain unaffected.Citation1
After oral intake, teriflunomide is rapidly absorbed; the bioavailability is almost 100%. More than 99% of the active substance is bound to plasma proteins. There is almost no involvement of the CYP450 system, which may decrease potentially clinically relevant drug–drug interactions. Nevertheless, some interactions have to be kept in mind (eg, with warfarin; for details see summary of product characteristicsCitation2). Teriflunomide is almost exclusively excreted via the feces and undergoes extensive enterohepatic recycling. The half-life is approximately 19 days. To achieve a rapid decrease in the plasma level, the oral administration of cholestyramine is required (dosage: 8 g three times daily (tid) for 11 days, or 4 g tid when cholestyramine 8 mg is not tolerated). Alternatively, the administration of activated charcoal is possible (50 g charcoal powder, administered every 12 hours over a period of 11 days).Citation3
Teriflunomide has been studied in an extensive clinical development program including two placebo-controlled Phase III studies: TEMSO (Teriflunomide Multiple Sclerosis Oral) and TOWER (Teriflunomide Oral in people With relapsing multiplE scleRosis).
TEMSO is a placebo-controlled, double-blind trial that included 1,086 patients with RR MS from 126 centers in 21 countries.Citation4 The patients were between 18 and 55 years old and had a mean Expanded Disability Status Scale of 2.7. They were required to have an active disease defined by at least one exacerbation in the previous 12 months or two relapses in the previous 24 months. About one-quarter of the patients were pretreated with immunomodulatory agents.
During the 2-year study period, patients received either placebo, teriflunomide 7 mg or 14 mg once daily. The primary endpoint was the annualized relapse rate. Secondary endpoints included disability progression and several MRI parameters (number of T1 gadolinium-enhanced lesions, T2 lesion load defined by new and enlarging T2 lesions). Teriflunomide 14 mg significantly reduced the annualized relapse rate by 31% compared to placebo (P<0.001). In addition, 14 mg teriflunomide resulted in a significant risk reduction of disability progression of 30% (P=0.02) compared to placebo. The analysis of the MRI data showed a significantly reduced number of gadolinium-enhancing T1 lesions and of new and enlarging T2 lesions (69%) for the 14 mg dose. A significant reduction of the annualized relapse rate was also observed for the 7 mg dose; however, the response of the other parameters (in particular MRI) was clearly dose dependent with superiority of the 14 mg dose.
The international, multicenter, double-blind, placebo-controlled Phase III study TOWER included 1,169 patients with RR MS from 26 nations. Patients were 18–55 years old and had experienced at least one exacerbation in the past year, or two relapses in the last 2 years. The minimum duration of treatment was 48 weeks; the average time on treatment was 18 months.Citation5
The study participants received either placebo or teriflunomide 7 mg or 14 mg once daily. Again, the primary endpoint was the annualized relapse rate. Progression of disability confirmed after 12 weeks was one of the secondary endpoints. The significant reduction of the annualized relapse rate in patients treated with 14 mg teriflunomide could be reproduced in the TOWER study. Administration of 14 mg teriflunomide resulted in a relative risk reduction of 36.3% (P<0.0001) compared to placebo. In addition, more patients remained relapse-free during the entire study period (P<0.0001). Finally, the risk of disability progression was reduced significantly by 31.5% (P=0.0442). Thus, teriflunomide is the only oral treatment option that has shown a significant reduction in disability progression in two pivotal studies.
In TEMSO, an overall good tolerability of teriflunomide could be observed. The incidence of adverse events was comparable in all study groups, including the placebo group. An increase in liver enzymes, diarrhea, nausea, and decreased hair density was more frequently observed in patients treated with teriflunomide compared with placebo. Discontinuation rates showed also no significant differences between the treatment arms. There was no increased risk for opportunistic infections and no increased risk for serious infections in patients treated with teriflunomide. Furthermore, no increased risk of malignancy was observed. Fortunately, no deaths occurred during the study. This good tolerability and favorable side effect profile was also observed in the TEMSO extension study.
In the TOWER study, the favorable safety profile was reproduced; no unexpected safety signals were observed. The infection rate was similar between the treatment arms, and there was also no evidence of an increased rate of malignant tumors. The most common side effects were mild elevation of liver enzymes, a slight increase in blood pressure, and a decreased hair density. In the TOWER study, three deaths (one traffic accident, one suicide, and one case of sepsis) occurred in the teriflunomide arms. All death were unrelated to the study treatment. In the placebo arm, a death occurred as a result of a respiratory infection.
In order to evaluate the clinical efficacy of teriflunomide in comparison to well-established immunomodulatory drugs, the efficacy of 48–115 (median 63.6) weeks’ treatment with oral teriflunomide 7 and 14 mg/day versus subcutaneous interferon beta-1a 44 tiw was investigated in a randomized, single-blind, multicenter, Phase III study (TENERE; n=324) in patients with RR MS. The participants were aged 18 years or older and had an Expanded Disability Status Scale ≤5.5.Citation6
The core treatment period lasted until 48 weeks after randomization of the last patient. Teriflunomide recipients were blinded as to dosage; interferon beta-1a treatment was open-label. The primary endpoint was the time to treatment failure in the intent-to-treat population during the core treatment period. Treatment failure was defined as the occurrence of a disease relapse or study discontinuation for any reason. The secondary outcome measures included annualized relapse rate, patient-reported fatigue using the Fatigue Impact Scale, and patient satisfaction assessed with the Treatment Satisfaction Questionnaire for Medication.
In patients receiving 14 mg teriflunomide (n=111), 37.8% reached the primary endpoint, while treatment failure was observed in 42.3% of patients treated with interferon beta-1a (n=104). This difference was statistically not significant. There was also no statistically significant difference between teriflunomide 14 mg and interferon beta in the adjusted annualized relapse rate.
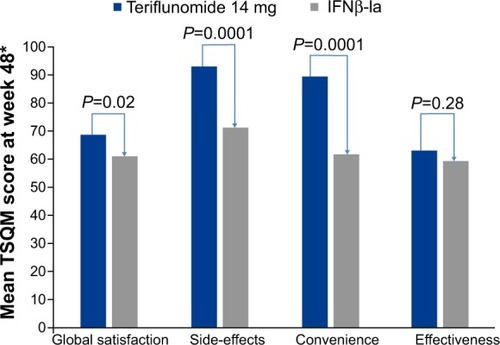
However, treatment satisfaction of patients treated with teriflunomide was significantly higher than in patients treated with interferon beta-1a. This result was based on the clearly superior ranking in the subscales “side effects” and “ease of therapy”, while no differences were observed in the subscale “clinical efficacy” ().
Figure 1 Treatment satisfaction at week 48 was significantly improved with teriflunomide 14 mg compared with sc IFNβ-1a in the TSQM domains of global satisfaction, side-effects, and convenience.
Abbreviations: IFN, interferon; TSQM, Treatment Satisfaction Questionnaire for Medication.
Finally the efficacy and safety of teriflunomide in patients with a first clinical episode suggestive of MS were evaluated (TOPIC study). Six hundred and eighteen patients were enrolled and randomly assigned to teriflunomide 14 mg (n=216), teriflunomide 7 mg (n=205), or placebo (n=197). Compared with placebo, teriflunomide significantly reduced the risk of relapse defining clinically definite MS (new neurological abnormality separated by at least 30 days from the onset of a preceding clinical event, present for at least 24 hours, and occurring in the absence of fever or known infection) at the 14 mg dose (42.6%, P=0.0087) and at the 7 mg dose (37.2%, P=0.0271).Citation7 Interpretation of the findings was limited because of early cessation of the study, reducing its statistical power. Nevertheless, the findings from the Phase III TOPIC study in clinically isolated syndrome, together with those from the TEMSO and TOWER studies in relapsing MS, support the beneficial effect of teriflunomide across a broad range of patients.
Teriflunomide – guidelines for clinical practice
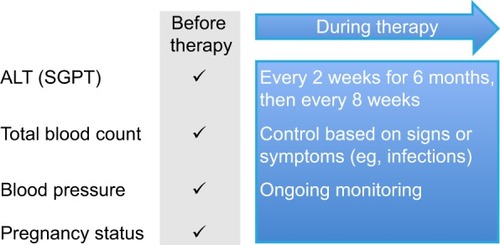
Due to the reported side effects in clinical studies, safety monitoring guidelines for teriflunomide include regular monitoring of blood pressure and liver function tests (). In addition, a complete blood count is required before initiation, and then if signs/symptoms of severe infection or hematologic toxicity occur.
Figure 2 Safety monitoring guidelines for teriflunomide.
The teratogenic potential of leflunomide and teriflunomide has been demonstrated in animals.Citation8 The FDA categorizes teriflunomide into pregnancy risk category X. Therefore, strict contraception is recommended for all females of reproductive age. To date, there is no evidence that teriflunomide has an effect on fertility or reproductive performance. In the pivotal clinical trials, women who became pregnant while on teriflunomide were required to perform the washout procedure. A teriflunomide plasma level <0.02 mg/L is considered as acceptable regarding safety during pregnancy. A recent analysis of the pregnancies (70 patients exposed with teriflunomide) reported in all clinical trials found no structural or functional deficits in any newborns with prenatal teriflunomide exposure. Furthermore, the proportion of spontaneous abortions was within population-based norms.Citation9
Vaccination with inactivated vaccines is possible during treatment with teriflunomide. This was documented in a study including 128 MS patients receiving influenza vaccine (against H1N1, H3N2, and B) while being treated with teriflunomide (TERIVA study). More than 90% of the patients showed an adequate immune response to vaccination with development of sufficiently high antibody titers.Citation10
If a patient would like to switch from interferon beta or glatiramer acetate to teriflunomide, no washout period is required. Add-on studies combining interferon beta or glatiramer acetate with teriflunomide have raised no safety concerns. In contrast, when a switch to an escalation treatment with natalizumab, fingolimod, or alemtuzumab is necessary, a washout procedure with cholestyramine or activated charcoal is highly recommended.
Patient preference for disease-modifying MS treatments – factors affecting treatment decision
With the increasing number of available DMTs for RR MS, the decision of how to treat the individual patient has become more complex within recent years. Nowadays, there are eleven agents (one given intramuscularly, four given sc, three given intravenously, and three given orally) licensed for RR MS in the US and Europe (). For patients with a clinically isolated syndrome, when the diagnosis of MS cannot yet be established according to the revised McDonald criteria,Citation11 only beta interferons and glatiramer acetate are approved by the regulatory agencies.
Patient counseling in the treatment decision process should focus on different aspects: disease type and activity, the benefit–risk assessment, individual contraindications, and patients’ preferences.
Disease activity and benefit–risk assessment
The currently licensed treatments for RR MS differ not only by the route of administration, but also by the spectrum of risks and possible side effects. The use of natalizumab is limited due to the risk of progressive multifocal leukoencephalopathy (PML). In mitoxantrone cardiotoxicity, limiting the treatment duration, and acute myelogenous leukemia are potential side effects. For this reason, both agents are mainly reserved for patients with breakthrough disease under other DMTs. However, there is evidence to suggest the use of natalizumab or mitoxantrone as induction therapy for patients with an early aggressive disease course, characterized by frequent relapses with incomplete remission and accumulation of MRI lesions.Citation12 Fingolimod can be used in the US without restriction regarding disease activity, whereas in most European countries it is licensed only for highly active RR MS patients. Alemtuzumab is approved for patients with active disease, defined by clinical or imaging features, in Europe, but national recommendations may restrict its use for patients with higher disease activity, relating to the inclusion criteria in the phase 3 studies.Citation13 Beta interferons, glatiramer acetate, teriflunomide, and DMF are approved irrespective of disease activity, but are mainly used as first-line agents. When treatment decisions are made against the backdrop of the benefit–risk assessment, patients’ decisions will depend on the estimate of the disease activity by the treating neurologist, but their preferences will influence the choice of treatment. It is worthwhile noting that the risk estimation of a given treatment may differ between the neurologist and the patient. Regarding the risk of PML in natalizumab treated patients, in one study, patients were willing to accept a higher risk of PML than their neurologists.Citation14
Contraindications
The choice of treatment will also be determined by contraindications for the potential medication. According to the summary of product characteristics, they include (but are not limited to): hypersensitivity to the drugs and/or the excipients and components for all medications; certain cardiac conditions and treatment with some antiarrhythmic drugs are contraindications for the use of fingolimod; current or history of PML precludes the use of natalizumab; HIV infection precludes the use of alemtuzumab; and severe hepatic impairment contraindicates the use of fingolimod, beta interferons, and natalizumab.Citation15–Citation23
A contraindication for teriflunomide is severe hepatic impairment. Furthermore, it may not be given in pregnant patients or women of childbearing potential who are not using reliable contraception, since it may cause fetal harm when administered in pregnancy. Coadministration of teriflunomide with leflunomide is not allowed. DMF is not recommended in pregnancy or in women of childbearing potential who are not using appropriate contraception.
Patients’ preferences
The prerequisites for a profound treatment decision by the patient (and the neurologist) are knowledge of the disease, the treatment options, the efficacy of treatments, potential sides effects, and risks of the planned intervention. MS affects mainly young, often well informed adults, but there are numerous patients who have little insight into the disease and the available therapeutic armamentarium. Obtaining information regarding the patient’s knowledge of the disease is therefore important for counseling. Patients and/or their caregivers have to be informed to a point at which decision making is possible. Treatment decisions in MS are becoming increasingly complex. Nowadays, assuring that patients understand the complex disease and the therapeutic field is challenging and also time consuming.
A shared decision-making process is increasingly advocated as an ideal model of treatment decisions in medical encounters.Citation24 In these situations, it is important to notice that patients and clinicians differ in their assessments of the relative importance of different elements of health-related quality of life.Citation25
The question of how patient education might influence treatment decisions has been addressed in a 12-month, multicenter, double-blind, randomized, controlled clinical trial in Germany with 192 patients with a diagnosis of RR MS or clinically isolated syndrome. A 4-hour interactive evidence-based educational program was compared with a 4-hours MS-specific stress management program. The primary endpoint was the proportion of participants displaying “informed choice” after 6 months of follow-up, comprising risk knowledge and congruency between attitude towards immunotherapy and actual immunotherapy uptake. Fifty of 85 (59%) participants in the intervention group achieved informed choice after 6 months compared with 18 of 89 (20%) in the control group (P<0.001). The intervention group showed good risk knowledge (significant difference between groups, P<0.001). There were trends towards increased autonomy preference after the intervention and increased adherence to immunotherapies.Citation26
Factors influencing the choice of treatment in clinical practice arise from the neurologist’s and the patient’s perspective. In a survey of 102 neurologists, the most important attributes of DMT selection were, in order of importance, efficacy, safety, tolerability, patient preference, and convenience,Citation27 indicating that patient preference was regarded as a less-important factor. According to Heesen et al however, 80% of MS patients demand autonomous roles in treatment decisions, with a higher risk knowledge correlating with a preference for higher autonomy.Citation28
A study by Mendel et al investigated whether physicians’ recommendations can pull patients away from their preferred treatment options. Inpatients, among them 101 with MS, were presented with a hypothetical scenario: the choice between two drugs. They were first asked about their preferences concerning the two drugs and then they received a (fictitious) clinician’s recommendation that was contrary to their preferences. Subsequently, they made a final choice between the two drugs. In the decision scenario, 26% of the patients with MS followed the advice of their physician and thus chose the treatment option that went against their initial preferences. Patients who followed their physician’s advice were less satisfied with their decision than patients not following their physician’s advice (for MS, P=0.009).Citation29 Since the waiver of the initial preference may have an impact on adherence, this study highlights the importance of patients being encouraged to establish their preference and decide on a treatment most suitable to them.
With regards to patients, factors influencing treatment decisions have been investigated in few studies. Concerning the question of whether to start or not to start a DMT, the patient’s risk attitude could be shown to be of relevance. More risk-seeking patients were less likely to choose a treatment compared with more risk-averse patients (P<0.01).Citation30 In a survey on the use of disease-modifying drugs in a group of 1,572 patients with MS in the Netherlands, the most important reasons not to start a treatment for MS were the severity and phase of the disease, possible side effects, the advice of the neurologist, and uncertainty about the effect of DMTs. According to the opinion of the patients, the neurologist had the most decisive role in starting or changing DMTs, whilst the patient was primarily responsible in deciding to stop the DMT.Citation31
To better understand patients’ preferences on DMTs, a choice-based conjoint analysis has been used to estimate the maximum acceptable risk trade-offs for various (hypothetical) DMT benefits. Severe side effect risks had the biggest impact on patient preference, with a 1% risk decreasing patient preference fivefold compared to no risk (odds ratio [OR]=0.22, P<0.001). Symptom improvement was the most preferred benefit (OR=3.68, P<0.001), followed by prevention of progression within 10 years (OR=2.4, P<0.001). In this study, daily oral administration had the third highest DMT preference rating (OR=2.08, P<0.001).Citation32 In the study by Utz et al an oral medication was preferred over injections by 93% of patients, when treatment frequency and frequency of side effects were held constant. However, patients preferred injections when pills had to be taken tid and injections only once per week. Injections were also preferred when pills were associated with frequent side effects.Citation33
Patient preferences and teriflunomide
Teriflunomide is an oral treatment given once daily. Different factors may influence patients’ preference (). The oral application is preferable for patients with injection anxiety refusing an injectable DMT, or who have stopped treatment for injection-related reasons. Compared to a bid or tid medication, patients may prefer the once-daily application of teriflunomide; although, according to our experience, this is crucial only in the minority of patients. Frequent liver enzyme controls within the first half year may be undesired by the patient, but are generally feasible in daily practice. Teriflunomide may cause gastrointestinal side effects, but in contrast to DMF (which has gastrointestinal side effects that are much more prevalent when taken while fasting), the tolerability of teriflunomide is generally not dependent on the fasting status, resulting in more flexibility of the patient. This is favorable for patients with an irregular routine of the day. Potential side effects of DMTs are a major issue in patient counseling before treatment initiation. In the TENERE trial, the only head-to-head Phase III trial, teriflunomide 7 and 14 mg were compared with interferon beta-1a sc tiw.Citation6 Based on the findings of this trial, potential patient preferences in clinical practice between teriflunomide and beta interferons may be discussed. Common adverse events (≥10% in any group) reported more frequently with teriflunomide included nasopharyngitis, diarrhea, hair thinning, paresthesia, and back pain. Influenza-like symptoms, Alanine Aminotransferase (ALT) increases, and headache occurred more frequently with interferon beta-1a. Influenza-like symptoms occurred in <5% of teriflunomide-treated patients, but in >50% of interferon beta-1a treated patients. These data favor teriflunomide for patients who fear flu-like symptoms, have experienced increasing fatigue or spasticity, or have experienced worsening of other MS symptoms associated with flu-like symptoms while injecting beta interferons. Since the incidence of infections was similar in the IFNβ-1a and teriflunomide 14 mg group, a higher incidence could be observed in the teriflunomide 7 mg group, the fear of infections may have no influence on the patient’s treatment decision. Gastrointestinal events, especially nausea and diarrhea, occurred more often (for diarrhea approximately threefold) in teriflunomide- than interferon beta-1a-treated patients. Patients with known gastrointestinal disorders may therefore not prefer teriflunomide. Remarkably, a history of gastrointestinal side effects did not have an impact on gastrointestinal tolerability in DMF-treated patients.Citation34 Whether this is also true for teriflunomide has yet to be determined. Patients wishing to avoid gastrointestinal side effects at best will decide for a parenteral therapy. Hair thinning (5.5% in the 7 mg and 20% in the 14 mg teriflunomide group) was much more common with teriflunomide, with the majority of cases occuring during the first 6 months. However only 2.7% of patients in the teriflunomide 14 mg group discontinued due to hair thinning (no patients in the 7 mg group discontinued due to hair thinning), with most patients recovering while continuing treatment. Since hair thinning is an undesirable side effect for many patients, counseling on the temporary nature before and also during treatment is important. Nevertheless, according to our experience, this potential side effects prompts some (more female than male patients) to decide against teriflunomide.
Table 2 Teriflunomide: factors potentially influencing patient preference in MS
Since teriflunomide can cause an increase of the systolic and diastolic blood pressure, patients with uncontrolled hypertension will decide against teriflunomide. Although rarely, teriflunomide may induce neuropathies;Citation35 a preexisting peripheral neuropathy may therefore be an argument against its use and if used in such cases, regular controls will be necessary.
Mean scores in the Treatment Satisfaction Questionnaire for Medication domains of global satisfaction, side-effects, and convenience were significantly improved with both doses of teriflunomide compared with interferon beta-1a in the TENERE trial. Scores in the effectiveness domain did not significantly differ between teriflunomide 14 mg and interferon beta-1a, but were lower with teriflunomide 7 mg.Citation6 These findings, however, may be more relevant for patients’ adherence than preference.
In animal studies, teriflunomide has been shown to be selectively teratogenic and embryolethal when administered during pregnancy, even at doses less than those used clinically. Therefore, women planning to become pregnant have to stop teriflunomide; due to the long half-life, the washout procedure described above is necessary. Women with a foreseeable plan to become pregnant should therefore, in our opinion, decide on an alternative therapeutic option, if available.
MS and adherence
The World Health Organization defines adherence as “the extent to which a person’s behavior corresponds with agreed recommendations from a healthcare provider” and stresses the importance of good adherence in achieving the full beneficial effects of long-term treatments.Citation36 It has been reported that 13%–72% of patients do not adhere to disease-modifying MS treatments,Citation37–Citation41 and poor adherence or treatment gaps are associated with a higher rate of relapse.Citation41–Citation46
Poor adherence is often caused by side effects resulting in a negative impact on quality of life.Citation47 It is therefore imperative to inform patients in detail about the planned therapeutic intervention, its risks, and side effects. Inquiry regarding potential side effects should be made at each visit, especially in active disease, when poor adherence may be suspected.
For oral DMTs, there is only very limited data comparing adherence with injectable DMTs. In a retrospective US study using pharmacy claims of patients who initiated DMTs between October 2010 and February 2011, patients initiating fingolimod (n=248) had the highest average proportion of days covered and medication possession ratio in both experienced and naive DMT patients compared to patients using injectable DMTs (n=1,643). The proportion of patients discontinuing their treatment within 12 months was significantly lower for fingolimod. Adjusted results found that patients self-injecting DMTs discontinued their treatment significantly sooner than fingolimod users.Citation48 Another retrospective study based on the PharMetrics Plus™ US administrative claims database (between October 2010 and September 2011) included patients naive to the index DMT. In this analysis, 3,750 patients (fingolimod n=889; glatiramer acetate n=1,233; any interferon beta n=1,341; natalizumab n=287) were included. Discontinuation rates (fingolimod 27.9%; glatiramer acetate 39.5%; interferon beta 43.7%; natalizumab 39.5%) and risk of discontinuation were significantly higher for patients receiving other DMTs compared with fingolimod. Adherence with fingolimod was higher than with the other treatment groups.Citation49
It could be shown that in injectable DMTs, only one-third of the reasons found to be responsible for poor adherence are dependent on the application form.Citation39 This means that non-injection related factors of nonadherence play a major role, as is known from other chronic disorders like epilepsy or hypertension.
Teriflunomide and adherence
Teriflunomide is distributed in a blister package, divided in 4 weeks’ doses, and labeled with the days of the week, which improves the control over the tablets already taken. The fact that teriflunomide is given once daily may favor adherence since compliance is inversely related to the number of daily doses.Citation50,Citation51 Due to the long half-life of teriflunomide, it may be speculated that incomplete adherence does not affect treatment efficacy. However, firstly, there are no data on the effect of poor adherence on teriflunomide efficacy; and secondly, the lower dosage of 7 mg daily has been shown to be less effective than 14 mg, indicating that dosage matters. Therefore, patients should, as with other DMTs, be advised to take the medication regularly.
In the TEMSO trial,Citation4 29% in the placebo, 25% in the 7 mg, and 27% in the 14 mg group discontinued treatment. The most common reason was side effects in 28%, 41%, and 40% of discontinuing patients, respectively.
Comparably, in the DEFINE trialCitation52 on DMF in RR MS, treatment discontinuation was observed in 35% of placebo-and 31% of DMF-bid-treated patients. Fifteen percent of placebo-treated patients and 48% of patients in the DMF cohort stopped medication for side effects.
Although data on treatment discontinuation in clinical trials may not be transferred to adherence in daily clinical practice and robust real-world data are lacking, it is important that patients have realistic expectations of potential side effects and that strategies to monitor and, if possible, manage them are discussed in detail.
Conclusion
The armamentarium of DMTs in MS is increasingly growing. Treatment decisions are made based upon several factors like disease activity, contraindications to the drugs, and, last but not least, physicians’ and patients’ preferences. Overall, teriflunomide has demonstrated efficacy and safety in a number of Phase III trials in the treatment of relapsing MS. The convenience of administration, the easy safety monitoring in the long-term course, and the tolerability of teriflunomide make it an attractive agent to add to the currently available treatment of relapsing MS. Characteristics of the drug have an impact on patients’ preferences. Due to its oral formulation, patients with fear of injections will decide for teriflunomide or the other approved oral options: DMF or fingolimod (if indicated according to the national label). Among oral treatments, factors favoring teriflunomide compared to DMF may be the once-daily dosing frequency and the lack of necessity to take the drug while nonfasting, which provides more flexibility to the patient’s everyday life. The long half-life of teriflunomide, however, may dissuade patients, especially women with a foreseeable wish to become pregnant, from taking teriflunomide. Adherence data in clinical daily practice are lacking for teriflunomide, but based on the experiences with other oral treatments in chronic disorders, it will be a challenging topic. In the currently growing field of MS therapeutics, patient counseling and perceiving patients’ attitudes will be of tremendous importance for treatment selection and adherence aiming at clinical stability and optimal quality of life.
Disclosure
Antonios Bayas has received honoraria for serving on advisory boards and as a speaker from Merck Serono, Biogen Idec, Bayer Vital, Novartis and Sanofi/Genzyme; for advisory board activities from TEVA; for trial activities from Biogen Idec, Merck Serono and Novartis; and received grants for congress trips and participation from Sanofi/Genzyme, Biogen Idec and Merck Serono.
Mathias Mäurer recieved honoraria for lectures from Biogen Idec, Novartis, Genzyme, Merck Serono, Bayer Vital, Böhringer Ingelheim, TEVA.
References
- GoldRWolinskyJSPathophysiology of multiple sclerosis and the place of teriflunomideActa Neurologica Scandinavica20111242758420880295
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002514/WC500148682.pdfAubagio, Summary of Product CharacteristicsAccessed 26.12.2014
- TallantyreEEvangelouNConstantinescuCSSpotlight on teriflunomideInternational MS Journal/MS Forum2008152626818782502
- O’ConnorPWolinskyJSConfavreuxCRandomized trial of oral teriflunomide for relapsing multiple sclerosisThe New England Journal of Medicine2011365141293130321991951
- ConfavreuxCO’ConnorPComiGOral teriflunomide for patients with relapsing multiple sclerosis (TOWER): a randomised, double-blind, placebo-controlled, phase 3 trialThe Lancet Neurology201413324725624461574
- VermerschPCzlonkowskaAGrimaldiLMTeriflunomide versus subcutaneous interferon beta-1a in patients with relapsing multiple sclerosis: a randomised, controlled phase 3 trialMultiple Sclerosis201420670571624126064
- MillerAEWolinskyJSKapposLOral teriflunomide for patients with a first clinical episode suggestive of multiple sclerosis (TOPIC): a randomised, double-blind, placebo-controlled, phase 3 trialThe Lancet Neurology2014131097798625192851
- FukushimaRKanamoriSHirashibaMTeratogenicity study of the dihydroorotate-dehydrogenase inhibitor and protein tyrosine kinase inhibitor Leflunomide in miceReproductive Toxicology2007243–431031617604599
- KieseierBBenamorMPregnancy Outcomes Following Maternal and Paternal Exposure to Teriflunomide During Treatment for Relapsing–Remitting Multiple SclerosisNeurology and Therapy20143133138
- Bar-OrAFreedmanMSKremenchutzkyMTeriflunomide effect on immune response to influenza vaccine in patients with multiple sclerosisNeurology201381655255823851964
- PolmanCHReingoldSCBanwellBDiagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteriaAnnals of Neurology201169229230221387374
- National Multiple Sclerosis Society NYMedications [webpage on the Internet]: Consensus on Disease-Modifying Therapies http://www.nationalmssociety.org/Treating-MS/Medications2014133Accessed 18.10.2014
- GoldRDiagnosis and treatment in multiple sclerosis. Guidelines of the German Society for Neurology (German)2014Accessed 26.12.2014
- HeesenCKleiterINguyenFRisk perception in natalizumab-treated multiple sclerosis patients and their neurologistsMultiple Sclerosis201016121507151220826527
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/003718/WC500150521.pdfLemtrada, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000102/WC500029425.pdfAvonex, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000136/WC500048681.pdfRebif, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000081/WC500053225.pdfBetaferon, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000933/WC500034701.pdfExtavia, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Public_assessment_report/human/002827/WC500170303.pdfPlegridy, Assessment reportAccessed 26.12.2014
- https://http://www.copaxone.com/Resources/pdfs/PrescribingInformation.pdfCopaxone, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002202/WC500104528.pdfGilenya, Summary of Product CharacteristicsAccessed 26.12.2014
- http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/000603/WC500044686.pdfTysabri, Summary of Product CharacteristicsAccessed 26.12.2014
- CharlesCGafniAWhelanTShared decision-making in the medical encounter: what does it mean? (or it takes at least two to tango)Social Science and Medicine19974456816929032835
- RothwellPMMcDowellZWongCKDormanPJDoctors and patients don’t agree: cross sectional study of patients’ and doctors’ perceptions and assessments of disability in multiple sclerosisBMJ19973147094158015839169401
- KopkeSKernSZiemssenTEvidence-based patient information programme in early multiple sclerosis: a randomised controlled trialJournal of Nneurology, Neurosurgery, and Psychiatry2014854411418
- HansonKAAgashivalaNWyrwichKWRaimundoKKimEBrandesDWTreatment selection and experience in multiple sclerosis: survey of neurologistsPatient Preference and Adherence2014841542224729689
- HeesenCKopkeSRichterTKasperJShared decision making and self-management in multiple sclerosis – a consequence of evidenceJournal of Neurology2007254Suppl 2II116II12117503119
- MendelRTraut-MattauschEFreyDDo physicians’ recommendations pull patients away from their preferred treatment options?Health Expectations: An International Journal of Public Participation in Health care and Health policy2012151233121323824
- ProsserLAKuntzKMBar-OrAWeinsteinMCThe relationship between risk attitude and treatment choice in patients with relapsing-remitting multiple sclerosisMedical Decision Making: An International Journal of the Society for Medical Decision Making200222650651312458981
- VisserLHvan der ZandeAReasons patients give to use or not to use immunomodulating agents for multiple sclerosisEuropean Journal of Neurology: the Official Journal of the European Federation of Neurological Societies201118111343134921496180
- WilsonLLoucksABuiCPatient centered decision making: Use of conjoint analysis to determine risk-benefit trade-offs for preference sensitive treatment choicesJournal of the Neurological Sciences20143441–2808725037284
- UtzKSHoogJWentrupAPatient preferences for disease-modifying drugs in multiple sclerosis therapy: a choice-based conjoint analysisTherapeutic Advances in Neurological Disorders20147626327525371708
- FoxEJVasquezAGraingerWGastrointestinal Tolerability of Delayed-Release Dimethyl Fumarate in a Multicenter, Open-Label Study of Patients with Relapsing Multiple SclerosisMultiple Sclerosis Journal201420S1205
- LeistTPFreedmanSMKapposLPooled Safety Analyses From the Teriflunomide Clinical Development ProgramMultiple Sclerosis Journal201420S1110
- SabatéEAdherence to Long-Term Therapies: Evidence for ActionWorld Health OrganizationGeneva, Switzerland2003
- BrandesDWCallenderTLathiEO’LearySA review of disease-modifying therapies for MS: maximizing adherence and minimizing adverse eventsCurrent Medical Research and Opinion2009251779219210141
- ReynoldsMWStephenRSeamanCRajagopalanKPersistence and adherence to disease modifying drugs among patients with multiple sclerosisCurrent Medical Research and Opinion201026366367420070144
- TreadawayKCutterGSalterAFactors that influence adherence with disease-modifying therapy in MSJournal of Neurology2009256456857619444532
- TremlettHLOgerJInterrupted therapy: stopping and switching of the beta-interferons prescribed for MSNeurology200361455155412939437
- MenzinJCaonCNicholsCWhiteLAFriedmanMPillMWNarrative review of the literature on adherence to disease-modifying therapies among patients with multiple sclerosisJournal of Managed Care Pharmacy: JMCP2013191 Suppl AS24S4023383731
- UitdehaagBConstantinescuCCornelissePImpact of exposure to interferon beta-1a on outcomes in patients with relapsing-remitting multiple sclerosis: exploratory analyses from the PRISMS long-term follow-up studyTherapeutic Advances in Neurological Disorders20114131421339904
- Al-SabbaghABennetRKozmaCDicksonMMeleticheDMedication gaps in disease-modifying therapy for multiple sclerosis are associated with an increased risk of relapse: findings from a national managed care databaseJournal of Neurology2008255Suppl 2S79
- SteinbergSCFarisRJChangCFChanATankersleyMAImpact of adherence to interferons in the treatment of multiple sclerosis: a non-experimental, retrospective, cohort studyClinical Drug Investigation20103028910020067327
- IvanovaJIBergmanREBirnbaumHGPhillipsALStewartMMeleticheDMImpact of medication adherence to disease-modifying drugs on severe relapse, and direct and indirect costs among employees with multiple sclerosis in the USJournal of Medical Economics201215360160922376190
- TanHCaiQAgarwalSStephensonJJKamatSImpact of adherence to disease-modifying therapies on clinical and economic outcomes among patients with multiple sclerosisAdvances in Therapy2011281516121153000
- O’RourkeKEHutchinsonMStopping beta-interferon therapy in multiple sclerosis: an analysis of stopping patternsMultiple Sclerosis2005111465015732266
- AgashivalaNWuNAbouzaidSCompliance to fingolimod and other disease modifying treatments in multiple sclerosis patients, a retrospective cohort studyBMC Neurology20131313824093542
- BergvallNPetrillaAAKarkareSUPersistence with and adherence to fingolimod compared with other disease-modifying therapies for the treatment of multiple sclerosis: a retrospective US claims database analysisJournal of Medical Economics2014171069670725019581
- SainiSDSchoenfeldPKaulbackKDubinskyMCEffect of medication dosing frequency on adherence in chronic diseasesThe American Journal of Managed Care2009156e22e3319514806
- ClaxtonAJCramerJPierceCA systematic review of the associations between dose regimens and medication complianceClinical Therapeutics20012381296131011558866
- GoldRKapposLArnoldDLPlacebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosisThe New England Journal of Medicine2012367121098110722992073