
 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Background
Episodic memory encoding and working memory (WM) deficits are among the first cognitive signs and symptoms in the course of schizophrenia spectrum disorders. However, it is not clear whether the deficit pattern is generalized or specific in nature. We hypothesized that encoding deficits at an early stage of the disease might be due to the more fundamental WM deficits.
Methods
We examined episodic memory encoding and WM by administering the California Verbal Learning Test, a 2-back task, and the Wisconsin Card Sorting Test in 90 first-episode psychosis (FE) patients and 116 individuals with an at-risk mental state for psychosis (ARMS) compared to 57 healthy subjects.
Results
Learning progress, but not span of apprehension, was diminished to a similar extent in both the ARMS and the FE. We showed that this was due to WM impairment by applying a structural equation approach.
Conclusion
Thus, we conclude that verbal memory encoding deficits are secondary to primary WM impairment in emerging psychosis.
Introduction
Current treatment strategies for schizophrenia aim at developing drugs specifically designed to enhance cognition and/or adopting an early detection and intervention approach in order to minimize symptom load and preserve functional capabilities.Citation1–Citation3
Both strategies depend on an accurate specification and a detailed description of the structure of cognitive deficits in the prodromal phase of the disease,Citation4 to provide either valid and reliable outcome measures for clinical trials or predictors for early detection approaches.
Structural and functional brain abnormalities are evident as early as in the prodromal phase of the disease.Citation5,Citation6 The same is true with cognitive deficits, where evidence indicates that the performance of patients in a prodromal phase of the disease lies between that of healthy controls and inferior performing patients in a first episode of psychosis.Citation7–Citation10
It is still debated, however, whether subjects at clinical high risk for psychosis or, interchangeably, with an at-risk mental state (ARMS), as well as first-episode psychosis (FE) patients, might display a deficit pattern of a specific or generalized nature, ie, whether a specifically circumscribed core deficit might explain the whole observable deficit pattern or not.Citation11–Citation14
It has been repeatedly reported that, among other domains, both working memory (WM) and verbal episodic memory are impaired in ARMS and FE patients.Citation7,Citation8,Citation14–Citation16
Unlike other cognitive domains affected, WM impairment is suggested to constitute a core feature of psychotic disorders.Citation17–Citation19 And because of its intermediate role between genotype and phenotype, it is generally regarded as an endophenotype in schizophrenia spectrum disorders.Citation20,Citation21 Even if the endophenotype concept has not been without criticism,Citation22 it once again emphasizes the significance of WM impairment in schizophrenia spectrum disorders.
Impairment in verbal episodic memory has been interpreted in terms of an encoding deficit.Citation23
In the present study, we adopted an approach which parsed the verbal memory encoding processes into smaller units, in order to shed some light on the kind of interdependence between both the episodic memory encoding deficit and the WM deficit in ARMS and FE patients. This is in line with recommendations regarding evidence on specific vulnerability markers for the prediction of psychosis.Citation11
Objectives
The current study sought to elucidate the influence of WM on verbal episodic memory encoding by means of the serial position effect of free recallCitation24 and the semantic cluster ratio (SCR) in ARMS and FE individuals. The SCR might reflect to what extent a subject engages in deep semantic encoding,Citation25 which is much more demanding on WM than the shallow encoding of physical properties (eg, small/large letters, male/female voice, etc.).
Serial position effects express nonuniform recall probabilities of memory items as a function of list position. The recency (rec) recall probability from the serial position curve is used as a surrogate measure of WM capacityCitation24,Citation26–Citation28 and is related to learning curves derived from the California Verbal Learning Test (CVLT).Citation29
Specific hypotheses are:
Compared to healthy control (HC) subjects, FE and ARMS individuals show an impaired encoding, as reflected by a reduced rate of learning and span of apprehension (recall performance regarding the first encoding trial).
Since WM performance in ARMS and FE patients is known to be impaired, we hypothesize that the rec effect of free recall (WM capacity component) and the SCR (central executive component of WM) is attenuated.
Moreover, we hypothesize a decreased impairment in episodic memory encoding after adjustment for WM deficiency. For that purpose, we additionally refer to explicit measures of WM, ie, response latency and omission errors from the N-back task and concept failures from the Wisconsin Card Sorting Test (WCST).
Methods
Participants
The study sample comprised 90 FE and 116 ARMS subjects (Supplementary materials) who completed a neuropsychological assessment at baseline. All participants were recruited between March 2000 and May 2015 from the specialized Early Detection of Psychosis (FEPSY) Clinic, which is an Outpatient Department of the University of Basel Psychiatric Hospital, Basel, Switzerland (Riecher-Rössler et al,Citation7,Citation30 for details of study design and screening procedure). The severity of psychopathology was assessed using the Brief Psychiatric Rating ScaleCitation31 and the Scale for the Assessment of Negative Symptoms.Citation32 Moreover, four selected Brief Psychiatric Rating Scale items served as decision criteria for the presence of manifest psychosis in the FEPSY project. Drug use was assessed with the Basel lnterview for Psychosis.Citation33
In total, 57 HCs were recruited by approaching students of a trade school, from hospital staff, and through advertisements. These subjects had no current psychiatric disorder, as assessed by a clinical interview, and no history of psychiatric illness, head trauma, neurological disease, serious medical or surgical illness, substance abuse, or family history of psychiatric disorders.
Exclusion criteria for patients were age younger than 18 years, insufficient knowledge of German language, IQ <70, previous episode of schizophrenic psychosis (treated with antipsychotics for >3 weeks), psychosis due to organic reasons or substance abuse, or psychotic symptoms within a clearly diagnosed affective psychosis or borderline personality disorder. The local ethics committee of the University of Basel approved all aspects of the study, and written informed consent was obtained from each participant.
Memory assessment
Episodic memory in ARMS, FE, and HC was assessed with a German version of the CVLT.Citation29 This assessment requires immediate recall of an auditory presentation of a 16-item word list, made up of four semantic categories (drinks, clothes, fruits, and tools), across five trials.
The following variables were extracted: number of words correctly recalled during trial one through five and the SCR, defined as the number of consecutive recalls of word pairs in a same-category list, divided by what would be randomly expected, if the participant would not have used a category-related recall strategy. Thus, an SCR of 1 reflects a semantic clustering completely at random, while an SCR >1 reflects a semantic clustering above random, ie, the adoption of a memory organization strategy based on the central executive component of the WM.
Encoding efficiency was derived by both the intercept (span of apprehension) and the learning curves’ slope, as function of the learning trials. The recall probabilities were computed item by item across the five trials. Each individual’s serial position curve was represented as a series of four averaged recall probabilities (primacy, middle 1, middle 2, and rec – Supplementary materials).
WM was assessed with the Test Battery for Attentional Performance (TAP) WM taskCitation34 and a computerized German version of the WCST.Citation35 The TAP WM task is a 2-back task requiring the participant to indicate whether a given stimulus (single-digit number appearing on the computer screen) matches a predecessor, two trials back. Task performance is reflected by number of omission errors and reaction time during correct responses.
Statistical analysis
Statistical and numerical analyses were performed using the R environment for statistical computing.Citation36 In order to test for simple group differences, analysis of variance (ANOVA) or Kruskal–Wallis rank sum test was adopted. Frequency balance across two or more groups was inspected with Fisher’s exact or χ2 tests. Missing values were subjected to imputation, such that the variance–covariance matrix of the data set remained unchanged (Supplementary materials). All subsequent analyses were performed based on the imputed data.
Learning performance of the CVLT was estimated using a log-linear limited growth mixed-effect model (Supplementary materials) that included an intrasubject random slope (for trial) and intercept. An ANOVA was performed on the linear mixed-effect model, based on marginal sums of squares (Type III Sum of Squares). Whenever necessary, log and trigonometric transforms were applied (Supplementary materials).
A structural equation modeling (using the package Lavaan 0.5-23.1097) approach, using maximum-likelihood estimation, was conducted in order to determine whether relevant factors, such as the TAP 2-back task, WCST concept failures, SCR, and rec effect, might contribute to word list encoding. Goodness of fit was assessed by calculating the root mean square error of approximation (RMSEA), where values of RMSEA <0.08 indicate appropriate fit. We, additionally, provided the comparative fit index (where >0.93 is generally considered a good fit) and the standardized root mean square residual (<0.08).
Wherever multiple comparisons of mean were required, a multivariate ANOVA was performed, followed by multiple univariate ANOVA. Finally, Tukey’s honest significant difference was computed.
Results
Demographic characteristics and descriptive statistics
The groups did not differ with respect to gender and education (). Unlike with cannabis use, the analyses of medication influences were limited to FE and ARMS, since HC did not use drugs. A significant proportion of FE (35.6%), but only 6 (5.2%) ARMS subjects, were treated with antipsychotics for less than 3 weeks at a maximum dose of below 125 mg chlorpromazine equivalent per day. ARMS patients received significantly more frequently antidepressants as compared to FE. Finally, there was a significant difference with regard to cannabis use. The highest proportion of cannabis users was observed in FE patients (34%), followed by ARMS patients (27%), and, finally, HC (8%). The most intense use was likewise observed in FE ().
Table 1 Demographic characteristics and psychopathology of ARMS subjects, FE patients, and HC
FE and ARMS patients did not differ in negative symptoms, but general psychopathology was somewhat more pronounced in FE as compared to ARMS patients (U=2076.5, p<0.001).
shows aggregated raw memory and WCST scores of ARMS, FE, and HC. Except for SCR, HC always outperformed ARMS and FE significantly. There were no statistical effects of age, gender, education, or of any medical compounds listed in on the WM performance measures.
Table 2 Mean, SD, and MD of the neuropsychological variables (raw values)
Encoding in word list learning
A log-linear limited growth mixed-effect model was fit in order to estimate the recall-by-trial function and by taking into account trial and subject as random factors. To model the inflating intertrial variance, a power variance function was additionally fit, using trial as covariate. For confounder selection, a sequential variable introduction and step-down approach was adopted, considering medication, cannabis use, and demographic variables as potential confounders.
An ANOVA indicated a main effect of log(trial) (F(1,1048)=2275.9; p<0.001) and a significant interaction log(trial) × group (F(2,1048)=10.1; p<0.001), but no main effect of group (F(2,258)=1.5; p=0.216). Additionally, we found a main effect of tranquillizer (F(1,258)=5.2; p=0.023) and sex (F(1,258)=13.3; p<0.001), and an interaction log(trial) × cannabis use (F(1,1048)=6.4; p=0.012), with cannabis use coded dichotomously, frequent (several times per week or daily) or less frequent use.
As the contrast analysis indicated, both ARMS (t=2.5; df=1,048; p=0.012) and FE (t=4.5; df=1,048; p<0.001) showed a smaller rate of learning (slope) than HC (). The rate of learning was also reduced by the use of cannabis (t=2.5; df=1048; p=0.012). Male gender was associated with a smaller intercept (span of apprehension) (t=3.6; df=258; p<0.001), as was the use of tranquillizers (t=2.3; df=258; p=0.023).
Table 3 Estimated intercept and slope of the learning curves of female ARMS individuals, FE patients, and HC adjusted for tranquilizer and cannabis use
The serial position effect of free recall
shows the recall probability of the memory items as a function of their serial position. Marked elevations at both ends indicate a strong primacy and a somewhat weaker rec effect. In contrast, the intermediate memory items yielded lower recall probabilities. However, in FE, there appears to be a region of exceptionally low recall probability at the level of mid2 (memory items 9–12).
Figure 1 The serial position effects of the CVLT learning trials according to ARMS subjects, FE patients, and HC.
Abbreviations: ARMS, at-risk mental state for psychosis; FE, first-episode psychosis; HC, healthy control; mid, middle; prim, primacy; rec, recency.
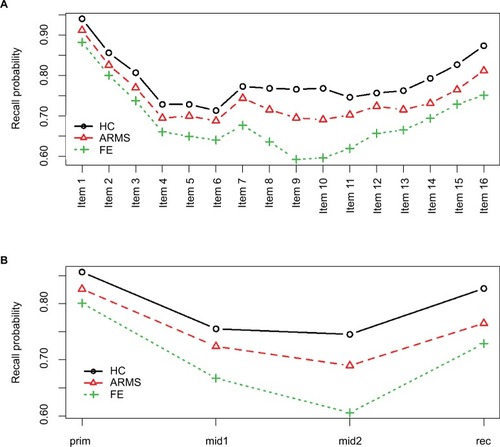
Positional recall probabilities were arcsine transformed and modeled by a multivariate ANOVA. Group, gender, age, education, neuroleptics, antidepressants, and cannabis use were modeled as independent variables. The multivariate ANOVA indicated a highly significant group effect (Wilks-λ=0.89; F(8,512)=3.9; p<0.001) and a trend for a gender effect (Wilks-λ=0.96; F(4,256)=2.4; p=0.052). Since none of the remaining variables showed a statistically significant relationship with the positional recall probabilities, they were excluded from further analyses.
A series of univariate ANOVAs indicated significant group differences at all serial positions, with effect sizes coarsely in increasing order (prim (F(2,259)=3.3; p<0.040), mid1 (F(2,259)=6.4; p=0.002), mid2 (F(2,259)=13.2; p<0.001), and rec (F(2,259)=7.4, p<0.001). Similarly, gender effects increased steadily from prim (F((1, 259)=3.2, p=0.072), mid1 (F(1,259)=4.1, p=0.044), mid2 (F(1,259)=4.5, p=0.035), to rec (F(1,259)=7.0, p=0.009).
Post hoc honest significant difference indicated a significantly lower primacy recall probability in FE compared to HC (p=0.035). At the level of mid1 and mid2, both ARMS and HC performed significantly superior compared to FE. At the level of the rec region, HC showed a significantly higher recall probability compared to both the FE (p<0.001) and the ARMS (p=0.031) patients. There was no significant difference between ARMS and FE patients. Thus, contrary to the pre-recency portion of the word list, the rec region exclusively showed an HC superiority effect.
Compromised learning as result of WM deficit
According to the hypothesis that a primary WM deficit accounts for deficits observed in verbal learning of FE and ARMS patients, we constructed a confirmatory structural equation model with an exogenous latent variable “WM”. This latent variable was constructed from maintenance WM (rec effect) and the central executive component of WM (SCR and WCST concept failure). To assure construct validity, the TAP 2-back tasks omission errors and response latency were fixed to the latent variable as composite measure central executive component of the WM (WMc). Where appropriate, variables were adjusted for confounders and z-transformed (Supplementary materials).
In order to explain the learning disabilities in FE and ARMS patients, it was sufficient to explain the difference between the group’s specific rates of learning (explained in the “Encoding in word list learning” section). Therefore, an individual regression-based rate of learning (slope) adjusted for cannabis use was determined according to each participant. The result is shown as a path diagram using standardized coefficients ().
Figure 2 Relationship between ARMS subjects, FE patients, rate of learning (slope), and WM as modeled by means of structural equations (N=263).
Abbreviations: ARMS, at-risk mental state for psychosis; FE, first-episode psychosis; HC, healthy control; rec, recency; SCR, semantic cluster ratio; cfail, Wisconsin Card Sorting Test concept failure; WM, working memory; WMc, central executive component of the WM.
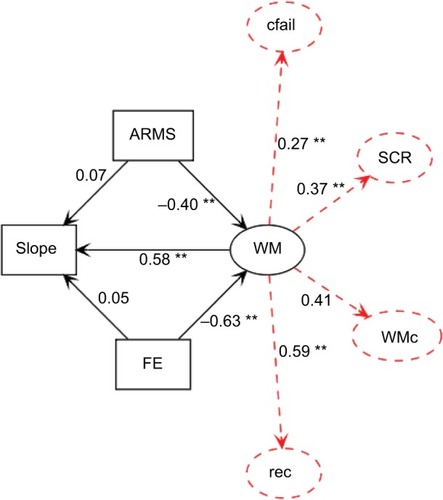
The χ2 test of model fit (χ2(11)=18.0; p=0.081) suggested the model’s appropriateness. This was further supported by its RMSEA =0.049 CI90 (0.0, 0.9), its CFI =0.94, and its SRMR =0.037. As a result of the WM’s mediator role, the direct association between both the FE (γ=0.05, z=0.5; p=0.649) and the ARMS patients (γ=0.07, z=0.8; p=0.447), with regard to the rate of learning, was no longer statistically significant.
Discussion
We provide evidence that verbal learning is moderately compromised in FE and ARMS patients. The same held true with regard to WM performance in explicit tests of WM (n-back, WCST). However, the impairment in episodic memory encoding affected only the rate of learning and did not influence the span of apprehension (Hypothesis I). As the analysis of the serial position recall probabilities revealed, for both FE and ARMS patients, the source of this reduced performance was mainly traced back to the rec proportion of the word list (Hypothesis II), while in FE patients it was additionally due to the pre-recency proportion. Apart from gender, the rate of learning was not dependent on potential confounders like age, medication, or cannabis use.Citation37 Thus, the rec region was the only source for the reduced rate of learning in ARMS patients.
According to the view that the rec effect reflects maintenance WM,Citation24,Citation26–Citation28 we provided additional evidence for a compromised WM in FE and ARMS patients. The dysfunctional short-term memory storage might have been especially important in explaining a diminished encoding efficiency of list items into episodic memory.
In order to test this, we formulated a hypothesis in terms of a structural equation model. In support of our hypothesis, the latent exogenous variable WM was significantly and positively related to the rate of learning. Most importantly, the FE and ARMS patients showed worse WM performance than HC. However, the rate of learning was no longer statistically different between groups when corrected for the influence of WM. Therefore, we conclude that WM might essentially contribute to the deficits in the formation of a long-term episodic memory in both the FE and the ARMS patients (Hypothesis III).
However, an issue arises from theoretical considerations, and refers to the nature of the rec effect itself. There is a controversial discussion in psychological literature on whether the rec effect in verbal learning truly reflects WM capacity. Initially, this idea emerged from experiments that demonstrated dissociable effects on rec and pre-recency portions of word lists.Citation38–Citation40 However, the observation of a long-term rec effect in so-called continuous distractor free recall tasks posed a challenge to this point of view,Citation41 since these tasks are characterized by presenting memory items along with distracting tasks, prior to and after each item, such that interference with WM should abolish the rec effect. On the other hand, both continuous distracter free recall rec and immediate free recall rec might be manipulated by experimental conditions, such that a double dissociation is evident.Citation42 Thus, regarding this issue, an unequivocal conclusion cannot be drawn.
Overall, the evidence we reported grossly confirmed our hypotheses. However, the picture that emerged was not quite as uniform as the hypotheses implied. First, the impairment in episodic memory encoding spared the span of apprehension and was exclusively restricted to the rate of learning. Second, even though the N-back task indicated a reduced central executive component of WM in both ARMS and FE patients, the SCR was not different between the groups.
Evidence of an aberrant rec effect in schizophrenia is sparse and inconsistent. Although there are reports on a diminished rec effect in schizophrenia,Citation43,Citation44 some found an elevated rec effect compared to HC,Citation45 and yet some others found no difference at all.Citation23,Citation46,Citation47 And, finally, there is virtually no evidence regarding ARMS patients. Therefore, our unequivocal and clear-cut findings of a reduced rec recall probability in both FE and ARMS patients might add to a more concise picture of the cognitive deficit in these groups.
We not only provided evidence that the maintenance (rec effect) but also the central executive component of the WM was impaired in both ARMS and FE patients. A general impairment of WM has been demonstrated in both patients with fully developed schizophreniaCitation48,Citation49 and those experiencing a first episode of psychosis.Citation4 But it also occurs in prodromal patients (ie, ARMS patients with later transition), and ARMS patients in general.Citation7,Citation8,Citation15,Citation50 However, SCR was preserved, which is somewhat puzzling, given the general importance of the WM in semantic encodingCitation51,Citation52 and the large body of evidence indicating a reduced tendency in using semantic cues as to effectively improve memory performance in schizophrenia.Citation53–Citation58
The results from the structural equation model suggested that the impaired WM is sufficient in explaining a reduced rate of learning in ARMS and FE patients. Support for this finding is suggested by evidence emphasizing the role of WM for episodic memory encoding in schizophrenia.Citation59,Citation46,Citation60,Citation56,Citation58,Citation61 Thus, verbal memory encoding deficits are secondary to a primary WM impairment and, therefore, are contrary to assumptions of a generalized-deficit perspective.Citation11–Citation14
However, it appears that additional factors could have contributed to the observed encoding deficiencies in FE patients, as their particular low performance in pre-recency portions suggested.
This last issue surely warrants replication and a finer grained analysis. There is evidence that long-term memory encoding and the central executive component of the WM share considerable proportions of prefrontal resources and that the recruitment of these prefrontal areas is less behavioral efficient in patients with schizophrenia as compared to HC subjects.Citation60,Citation61 It remains to be shown whether and how this mechanism gradually applies to ARMS and FE patients and might, thus, correlate with a diminishing encoding efficiency in emerging psychosis.
Acknowledgments
The data on which this research is based were drawn from the FEPSY (Early Detection) Study, which is funded by project grants from the Swiss National Science Foundation (Nos. 3200-057216-99; 3200-057216/3). We thank all patients and volunteers who participated in the study as well as the referring specialists. We especially would like to thank Dr Christian Schindler for his support with statistical advices.
Supplementary materials
Estimation of learning curves
The graph of the average numbers of correctly recalled list items as a function of consecutive trials usually resembles a bounded growth curve, which can be formalized as follows:
where c is a group-specific constant and S is the growth limit, which can be set to 16, since no more than 16 words can be learned (actually, the growth limit was set to S=17 in order to avoid taking the logarithm of zero). Moreover, S – c represents the intercept (span of apprehension, ie, the maximum number of words that can be correctly assessed after the first list presentation) and k the learning slope (growth rate). The larger k is, the more and faster learning occurs. It determines how fast the amount of recalled list items converges toward the growth boundary S. Actually, the analysis resulted in a model with additional parameters, thus, extending the above formalization, as follows:
In expanding the expression, we obtain
Now the intercept becomes S − cesex etrx,where trx (tranquilizer use) and sex are dichotomously coded. It is important to note that the intercept is not dependent on group. Thus, the group difference in learning is exclusively restricted to the slope (a figure of the learning curves is provided in Figure S1).
Learning curves as derived from the mixed modeling approach
Black crosses denote fit values from the mixed model, as outlined in the results section. Red lines indicate mean fit values, and dashed lines indicate the 99% confidence intervals of the means. As can be seen, variance in learning increases as learning proceeds. Apparent differences between the intercepts are due to different proportions of men and women, and a different use of tranquilizers across the groups. Moreover, healthy control (HC) achieves an overall maximum number of items recalled during trial five, suggesting a reduced rate of learning in both the at-risk mental state (ARMS) and the first-episode psychosis (FE) patients.
Construction of the serial position curve and determination of the recency effect
Item-wise recall probabilities were computed by assigning 1.0 to a successful recall and 0.0 otherwise. By summing up the successes of recalling a particular word across trials and dividing it by 5 (total number of trials), probabilities were derived that ranged from 0 (no recall across the trials) to 1 (permanent recall). In order to calculate the primacy and recency (rec) effect, the complete 16-items word list was subdivided into groups of four adjacent list items. The aggregation of the first quarter yielded the primacy effect and the aggregation of the last quarter provided the rec effect, respectively. Therefore, each individual’s serial position curve was represented by a series of four averaged recall probabilities (primacy, middle 1, middle 2, and rec).
Variable transformations according to the multivariate analysis of variance and Structural Equation Modeling
As to satisfy residual normality and heteroscedasticity positional recall probabilities pR were arcsine transformed as follows (and additionally z-transformed):
For the structural equation modeling, additional variables were transformed in order to meet the above distribution requirements:
A working memory composite score was created by calculating the mean from z-transformed omission errors and logarithmized reaction times.
Cannabis use was dichotomized by collapsing the classes “daily” and “weekly” in “frequent use” and the classes “monthly,” “less then monthly,” and “no” in “less frequent use” ().
rec recall probabilities were corrected for gender by extracting the residuals from regressing gender on the recall probabilities and dividing them by the standard error of the regression model. This resulted in z-values corrected for gender.
Slope was corrected for cannabis use (see issue 2) in the same way as issue 3.
A somewhat different approach was used to preprocess the concept failures from the Wisconsin Card Sorting Test. Due to a large floor effect, the distribution of the concept failures was highly skewed. Therefore, the variable was dichotomized according to subjects who scored more than one and others who scored less.
The semantic cluster ratio was simply z-transformed by centering the values on the mean and dividing them by the standard deviation.
Variable imputation
Initially a small proportion of 0.6% data were missing, most frequently affecting cannabis use. In total, seven variables were affected by missing values (working memory omission errors and reaction time, Wisconsin Card Sorting Test concept failure, Brief Psychiatric Rating Scale global score, Scale for the Assessment of Negative Symptoms summary score, recall from trial 6 of the California Verbal Learning Test, and cannabis use).
The imputation of the missing values was achieved by using the Random Forest rfImpute procedure from the R package randomForest 4.6-12.
The algorithm starts by imputing “NA”s using “na. roughfix” (which is a starter function, likewise provided by the randomForest package). Then, the “randomForest” procedure is called with the completed data. The proximity matrix from the randomForest is used to update the imputation of the “NA”s. For continuous predictors, the imputed value is the weighted average of the nonmissing observations, where the weights are the proximities. For categorical predictors, the imputed value is the category with the largest average proximity. This process is iterated multiple times.
Figure S1 Learning curves of the CVLT word list for HC, ARMS, and FE as a function of trials 1 to 5.
Abbreviations: ARMS, at-risk mental state for psychosis; CVLT, California Verbal Learning Test; FE, first-episode psychosis; HC, healthy control.
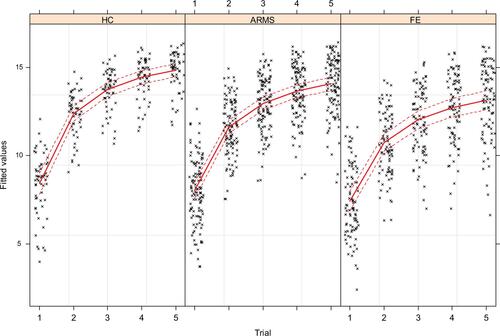
Table S1 Diagnostic criteria for ARMS and FE patients (Yung et al., 2003)Citation1
Reference
- YungARPhillipsLJYuenHPPsychosis prediction: 12-month follow up of a high-risk (“prodromal”) groupSchizophr Res2003601213212505135
Disclosure
The authors report no conflicts of interest in this work.
References
- NordentoftMMelauMIversenTFrom research to practice: how OPUS treatment was accepted and implemented throughout DenmarkEarly Interv Psychiatry20159215616224304658
- BuchananRWDavisMGoffDA summary of the FDA-NIMH-MATRICS workshop on clinical trial design for neurocognitive drugs for schizophreniaSchizophr Bull200531151915888422
- InselTRRethinking schizophreniaNature2010468732118719321068826
- Mesholam-GatelyRIGiulianoAJGoffKPFaraoneSVSeidmanLJNeurocognition in first-episode schizophrenia: a meta-analytic reviewNeuropsychology200923331533619413446
- SmieskovaRFusar-PoliPAllenPNeuroimaging predictors of transition to psychosis – A systematic review and meta-analysisNeurosci Biobehav Rev20103481207122220144653
- Fusar-PoliPBroomeMRMatthiassonPSpatial working memory in individuals at high risk for psychosis: longitudinal fMRI studySchizophr Res20101231455220688479
- Riecher-RösslerAPfluegerMOAstonJEfficacy of using cognitive status in predicting psychosis: a 7-year follow-upBiol PsychiatrIn press2009
- Fusar-PoliPDesteGSmieskovaRCognitive functioning in prodromal psychosis: a meta-analysisArch Gen Psychiatry201269656257122664547
- StuderusEPapmeyerMRiecher-RösslerANeurocognition and Motor Functioning in the Prediction of Psychosis181Karger Publishers2016 Available from: http://www.karger.com/Article/Abstract/440919Accessed February 19, 2016
- HauserMZhangJPSheridanEMNeuropsychological test performance to enhance identification of subjects at clinical high risk for psychosis and be most promising for predictive algorithms for conversion to psychosis: a meta-analysisJ Clin Psychiatr20177801e28e40
- BrewerWJWoodSJPhillipsLJGeneralized and specific cognitive performance in clinical high-risk cohorts: a review highlighting potential vulnerability markers for psychosisSchizophr Bull200632353855516782759
- LenczTSmithCWMcLaughlinDGeneralized and specific neurocognitive deficits in prodromal schizophreniaBiol Psychiatr2006599863871
- PukropRSchultze-LutterFRuhrmannSNeurocognitive functioning in subjects at risk for a first episode of psychosis compared with first-and multiple-episode schizophreniaJ Clin Exp Neuropsychol20062881388140717050266
- SeidmanLJGiulianoAJMeyerECNeuropsychology of the prodrome to psychosis in the NAPLS consortium: relationship to family history and conversion to psychosisArch Gen Psychiatry201067657858820530007
- PfluegerMOGschwandtnerUStieglitzRDRiecher-RösslerANeuropsychological deficits in individuals with an at risk mental state for psychosis – working memory as a potential trait markerSchizophr Res2007971–3142417936587
- BoraEMurrayRMMeta-analysis of cognitive deficits in ultrahigh risk to psychosis and first-episode psychosis: do the cognitive deficits progress over, or after, the onset of psychosis?Schizophr Bull201440474475523770934
- CastnerSGoldman-RakicPWilliamsGAnimal models of working memory: insights for targeting cognitive dysfunction in schizophreniaPsychopharmacology20041741
- ElvevagBGoldbergTECognitive impairment in schizophrenia is the core of the disorderCrit Rev Neurobiol200014112111253953
- GoldJMCarpenterCRandolphCGoldbergTEWeinbergerDRAuditory working memory and Wisconsin Card Sorting Test performance in schizophreniaArch Gen Psychiatry19975421599040284
- GottesmanIIGouldTDThe endophenotype concept in psychiatry: etymology and strategic intentionsAm J Psychiatry2003160463664512668349
- ParkSGoodingDCWorking memory impairment as an endophenotypic marker of a schizophrenia diathesisSchizophr Res Cogn20141312713625414816
- FlintJMunafòMRThe endophenotype concept in psychiatric geneticsPsychol Med2007370216316978446
- HillKSBeersSRKmiecJAKeshavanMSSweeneyJAImpairment of verbal memory and learning in antipsychotic-naïve patients with first-episode schizophreniaSchizophr Res2004682–312713615099597
- MurdockBBJrThe serial position effect of free recallJ Exp Psychol1962645482488
- CraikFLockhartRLevels of processing: a framework for memory researchJ Verbal Learn Verbal Behav1972116671684
- AndersonJRBothellDLebiereCMatessaMAn integrated theory of list memoryJ Memory Lang1998384341380
- GlanzerMStorage Mechanisms in RecallBowerGHThe Psychology of Learning and Motivation: Advances in Research and Theory5Academic Press1972129193 Available from: http://www.sciencedirect.com/science/article/B7J17-4S81B93-6/2/50dac4b99510365ee1a36d3afc8c655dAccessed June 15, 2010
- WaughNCNormanDAPrimary memoryPsychol Rev19657228910414282677
- DelisDKramerJKaplanEOberBCalifornia verbal learning testTest Critiq1984158
- Riecher-RösslerAGschwandtnerUAstonJThe Basel early-detection-of-psychosis (FEPSY)-study design and preliminary resultsActa Psychiatrica Scandinavica200711511412517244175
- LukoffDNuechterleinKHVenturaJManual for the expanded brief psychiatric rating scaleSchizophr Bull198612594602
- AndreasenNCThe Scale for the Assessment of Negative Symptoms (SANS): conceptual and theoretical foundationsBr J Psychiatry Suppl1989749582695141
- Riecher-RösslerAAckermannTUttingerMDas Basler Interview für Psychosen (BIP): Struktur, Reliabilität und ValiditätFortschritte der Neurologie · Psychiatrie201583029910825723774
- ZimmermannPFimmBTest for attentional performance (TAP)Herzogenrath, GermanyPsyTest1995
- Drühe-WienholtCMWienholtWCKV: Computergestütztes KartensortierverfahrenFrankfurt am MainSwets und Zeitlinger Testservices1998
- R Development Core TeamTeam R: A Language and Environment for Statistical ComputingVienna, AustriaR Foundation for Statistical Computing2015 Available from: http://www.R-project.org
- AlemanAHijmanRde HaanEHFKahnRSMemory impairment in schizophrenia: a meta-analysisAm J Psychiatry199915691358136610484945
- GlanzerMCunitzARTwo storage mechanisms in free recallJ Verbal Learn Verbal Behav196654351360
- PostmanLPhillipsLWShort-term temporal changes in free recallQuarter J Exp Psychol1965172132138
- UnsworthNEngleRWThe nature of individual differences in working memory capacity: active maintenance in primary memory and controlled search from secondary memoryPsychol Rev2007114110413217227183
- BjorkRAWhittenWBRecency-sensitive retrieval processes in long-term free recallCognit Psychol197462173189
- DavelaarEGoshen-GottsteinYAshkenaziAHaarmannHUsherMThe demise of short-term memory revisited: Empirical and computational investigations of recency effectsPsychol Rev2005112134215631586
- LandrøNIØrbeckALRundBRMemory functioning in chronic and non-chronic schizophrenics, affectively disturbed patients and normal controlsSchizophr Res199310185928369236
- StirlingJDHellewellJSEHewittJVerbal memory impairment in schizophrenia: no sparing of short-term recallSchizophr Res199725285959187007
- EgelandJSundetKRundBRSensitivity and specificity of memory dysfunction in schizophrenia: a comparison with major depressionJ Clin Exp Neuropsychol20032517912607174
- ChanASKwokICChiuHLamLPangAChowLMemory and organizational strategies in chronic and acute schizophrenic patientsSchizophr Res200041343144510728720
- PeuskensJde HertMJanssenFHulselmansJD’HaenensMSabbeBMemory disorders in schizophreniaDe DeynPPThieryED’HoogeRMemory: Basic Concepts, Disorders, and Treatment1st edLeuvenACCO2003488
- ForbesNFCarrickLAMcIntoshAMLawrieSMWorking memory in schizophrenia: a meta-analysisPsychol Med2009390688990518945379
- KimJGlahnDCNuechterleinKHCannonTDMaintenance and manipulation of information in schizophrenia: further evidence for impairment in the central executive component of working memorySchizophr Res2004682–317318715099601
- EastvoldADHeatonRKCadenheadKSNeurocognitive deficits in the (putative) prodrome and first episode of psychosisSchizophr Res2007931–326627717467955
- DembJBGloverHSemantic encodingJ Neurosci1995159587058787666172
- WagnerADParé-BlagoevEJClarkJPoldrackRARecovering meaning: left prefrontal cortex guides controlled semantic retrievalNeuron200131232933811502262
- Bonner-JacksonAYodkovikNCsernanskyJGBarchDMEpisodic memory in schizophrenia: the influence of strategy use on behavior and brain activationPsychiatr Res20081641115
- Bonner-JacksonAHautKCsernanskyJGBarchDMThe influence of encoding strategy on episodic memory and cortical activity in schizophreniaBiol Psychiatr20055814755
- WolfDHGurRCValdezJNAlterations of frontotemporal connectivity during word encoding in schizophreniaPsychiatr Res20071543221232
- BrébionGDavidASJonesHPilowskyLSSemantic organization and verbal memory efficiency in patients with schizophreniaNeuropsychology200418237838315099160
- RaglandJDGurRCValdezJNLevels-of-processing effect on frontotemporal function in schizophrenia during word encoding and recognitionAm J Psychiatry2005162101840184816199830
- AchimAMLepageMEpisodic memory-related activation in schizophrenia: meta-analysisBr J Psychiatry2005187650050916319401
- BrébionGAmadorXSmithMJGormanJMMechanisms underlying memory impairment in schizophreniaPsychol Med199727023833939089831
- BarchDMCsernanskyJGConturoTSnyderAZWorking and long-term memory deficits in schizophrenia: is there a common prefrontal mechanism?J Abnorm Psychol2002111347849412150424
- RaglandJDBlumenfeldRSRamsayISNeural correlates of relational and item-specific encoding during working and long-term memory in schizophreniaNeuroImage20125921719172621907293