
Abstract
Aims
The aims of this study were to assess the effectiveness of self-efficacy-focused education on health outcomes in persons with diabetes and review the strategies employed in the interventions.
Background
The traditional educational interventions for persons with diabetes were insufficient to achieve the desired outcomes. Self-efficacy-focused education has been used to regulate the blood sugar level, behaviors, and psychosocial indicators for persons with diabetes.
Design
This study is a systematic review and meta-analysis.
Methods
Studies on the effectiveness of self-efficacy-focused education in persons with diabetes were searched in six databases from inception until January 2018. The data were extracted and the quality of literature was assessed independently. Review Manager 5.3 was applied for the meta-analysis. Besides, the findings were summarized for narrative synthesis.
Results
Sixteen trials with 1,745 participants were included in the systematic review and ten trails with 1,308 participants in the meta-analysis. The meta-analysis for A1C, self-efficacy, self-management behaviors, knowledge, and quality of life (QOL) were represented in four, six, six, three, and three studies, respectively. The findings indicated that self-efficacy-focused education would probably reduce A1C, enhance self-efficacy, regulate self-management behaviors, increase knowledge, and improve the QOL for patients with diabetes. Weak quality studies, limited participants, and heterogeneity hindered the results pooled of the other secondary outcomes of fasting blood glucose, 2-hour plasma glucose, weight, weight circumference, body mass index, plasma lipid profile, and other psychological indicators. Goal setting, self-management skills practicing and recording, peer models, demonstration, persuasion by health providers, and positive feedback were the most commonly used strategies in the interventions. However, physiological/emotion arousal strategies were relatively less applied and varied significantly.
Conclusion
Individuals with diabetes may benefit a lot from the self-efficacy-focused education. However, insufficient high-quality studies, short-term follow-up period, relatively deficient physiological/emotion strategies, and incomplete outcome assessments were the drawbacks in most studies. Establishing satisfactory self-efficacy-focused education and better evaluating the effects were required in further studies.
Introduction
Nearly 425 million adults worldwide lived with diabetes in 2017, and it is projected that it will reach 629 million by 2045. Moreover, diabetes may lead to secondary complications, which accounted for 10.7% of the global all-cause mortality among the individuals aged between 20 and 79 years.Citation1 Diabetes education is a cornerstone of the diabetes care. Diabetes management is a complex daily work consisting of adjusting diet, performing exercise, conducting self-monitoring, and taking medicine. The traditional diabetes educational interventions, which merely provided the related knowledge, were inadequate to achieve the expected effects.Citation2,Citation3 Furthermore, the behavior change theories were applied in few studies on diabetes education.Citation4 A variety of research studies manifested that the self-care behaviors of persons with type 2 diabetes (T2DM) were suboptimal.Citation5–Citation9 Besides, poor self-efficacy was considered as an extreme disadvantage of managing diabetes.Citation10
The notion of self-efficacy originated from the social cognitive theory and developed into its related theory.Citation11,Citation12 According to the theory, self-efficacy is the individual’s belief that related to specific behavior in a special setting, which can be modified by four sources of information, including performance accomplishments, vicarious experience, verbal persuasion, and physiological/emotion arousal.Citation11,Citation12 Satisfactory results may be achieved when an educational intervention properly combined the above information. In addition, self-efficacy can regulate human behaviors based on the theory.
Diabetes educational interventions based on the self-efficacy theory were defined as self-efficacy-focused education.Citation13,Citation14 Literature reviews indicated that an educational intervention supported by the related theory may achieve more satisfactory results on reducing blood glucose levels.Citation15,Citation16 As far as we know, there was no literature review interpreting the effects of self-efficacy-focused education in patients with diabetes and the strategies used in the interventions. In addition, self-efficacy educational interventions for patients with diabetes on health outcomes were inconsistent.Citation14,Citation17–Citation20 As a consequence, the objectives of the review were to evaluate the effectiveness of self-efficacy-focused education on health outcomes in patients with diabetes and review the strategies employed in the self-efficacy educational interventions.
Methods
In this review, combined searching with screening the literature, the reporting was based upon PRISMA.Citation21
Eligibility
Types of studies
Studies using experimental designs included randomized controlled trials (RCTs), quasi-experimental approaches, or mixed method studies that included RCTs or quasi-experimental designs.
Types of participants
The ages of all the participants were ≥17 years, and all the participants were diagnosed with T2DM or T1DM unless the participants only included T1DM patients.
Types of interventions
The interventions should be developed and implemented based on the principle sources of information proposed by Bandura with detailed descriptions.Citation11,Citation12 Performance accomplishments referred to individuals’ direct experience originated from their own personal practices, which would play a crucial role in the establishment of self-efficacy under specific circumstances. Moreover, vicarious experience was defined as individual’s learning from observing and absorbing the successful behaviors or achievements from others. In addition, verbal persuasion indicated that individuals were convinced to believe that they can accomplish and succeed in a task by providing knowledge, instructions, and advice. Besides, physiological/emotion arousal was regarded as individuals’ psychological state adjustment. The contents of the self-efficacy-focused education for patients with diabetes mainly included education on any of the following aspects: diet adjustment, exercising, foot care, self-monitoring, and medication.
Types of outcome measures
The primary outcomes included A1C, diabetes self-efficacy, and diabetes self-management behaviors. Weight control (weight, body mass index [BMI], and weight circumference [WC]), other indicators of blood sugar level (fasting blood glucose [FBG] and 2-hour plasma glucose [2 h-PG]), plasma lipid profile (total cholesterol [TC], low-density lipoprotein cholesterol [LDL-C], high-density lipoprotein cholesterol [HDL-C], and triglycerides [TG]), and other psychosocial indicators (diabetes knowledge, diabetes distress, depression, and QOL belonged to the secondary outcomes.
Data source and search strategy
Six databases including PubMed, Web of Science, EBSCO, CNKI, Wanfang, and SinoMed were systematically searched for the articles published from inception until January 2018. The terms of “self efficacy,” “self-efficacy,” “efficacy, self,” “diabet*,” and “educat*” were combined for searching. Articles published in English or Chinese language were included. The additional articles were identified through the references of the included studies. The selection of articles were reviewed by two investigators independently. A discussion or an arbitration was arranged when the two investigators were inconsistent with the inclusion of studies.
Extraction and quality appraisal of studies
The study characteristics including study location, design, sample, strategies of intervention, instruments, outcome measures, and so on were extracted. The Quality Assessment Tool for Quantitative StudiesCitation22 was applied to conduct the quality appraisal. The components of the quality tool included six aspects of bias of selection, research design, confounders in studies, blinding issue, methods of data collection, and withdrawals/dropouts of participants. Each criteria was rated in 3, 2, or 1 point, corresponding to the quality of strong, moderate, or weak, respectively. The overall rating in the study was determined by the total of six-component rating points. To be specific, two or more weak ratings in a study were defined as weak quality, less than four strong ratings and one weak rating as moderate quality, and no weak ratings and at least four strong ratings as strong quality.
Data analysis
In terms of participants, interventions, and outcomes, the indicators of FBG, 2 h-PG, weight, WC, BMI, and plasma lipid profile were presented in a format of a textual summary of findings, while indicators of A1C, self-efficacy, behavior, knowledge, and QOL were pooled for meta-analysis. The mean difference (MD) was calculated when the indicators were measured in the same scale, whereas the standardized mean difference (SMD) was calculated. Chi-squared test was applied to evaluate the heterogeneity, and P<0.10 was considered as heterogeneity. The value I2 quantified the degree of heterogeneity. If I2 was above 50%, a random-effect model was employed, otherwise, a fixed-effect model was used. The sensitivity analysis was conducted by deleting the studies of high risk bias. Besides, Review Manager 5.3 was employed for the meta-analysis.
Results
Study selection and study quality evaluation
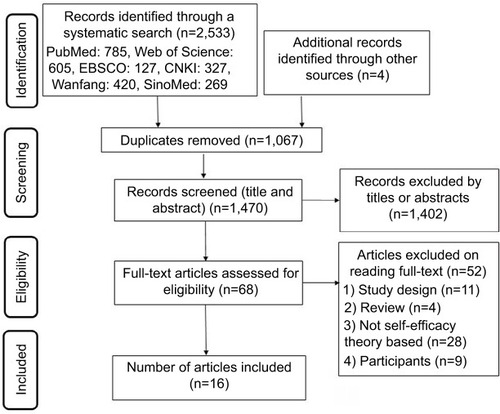
The selecting criteria of self-efficacy-focused education for adults with diabetes are shown in . Two thousand five hundred thirty-three abstracts were obtained via the systematic searches, and four additional articles were got through searching the references lists. To sum up, the total number of searched articles was 2,537. After deleting 1,067 duplicate articles and excluding 1,402 studies through reviewing titles and abstracts, there were 68 articles for full-text reading, and 16 studies were finally selected. The other 52 research studies were excluded because of the study population, review format, study design, the use of other theory, or a lack of detailed description regarding how educational interventions were developed and implemented based on the self-efficacy theory. Among the selected 16 studies, 6 were of strong quality, 9 of moderate quality, and 1 of weak quality. The blind outcome assessor or study participants were not reported in the above studies.
Figure 1 A PRISMA flow diagram describing the study selection criteria.
Characteristics of included studies
Various information including study location, date of publication, sample capacity, and study design is presented in . Among the 16 included studies, 2 were from Europe, 1 from Turkey, 2 from Thailand, 2 from Malaysia, 3 from Taiwan, and 6 from mainland China. The date of publications ranged from 2006 to 2017 and the sample capacity of studies from 8 to 228. RCT was employed in eight studies and the quasi-experimental design in the others (two pre-post design studies).
Table 1 Characteristics of included studies
In , verbal persuasion was used in all studies, performance accomplishments in 15 studies, vicarious experience in 15 studies, and physiological/emotion arousal in 5 studies. Five studies employed four sources of information when developing and implementing the educational interventions. Strategies such as goal-setting were predominately applied for performance accomplishments, followed by practicing diabetes self-management skills, recording behavior, patients’ return-demonstration, making diabetes-related plan, repetition, review and reinforcement, small and realistic steps, behavior contract, evaluation and feedback regarding behavior, and positive attribution. Successful experience provided by a live peer model was primarily applied in vicarious experience, followed by videos, booklets, other elements, such as demonstration and role-play. Verbal persuasion was mainly provided by nurses, followed by researchers, education booklets, group members, and psychologists. Besides, personal heath lectures and other healthy knowledge can be obtained through the Internet. Moreover, performance feedback, encouragement, and the identification of barriers and solutions were also employed in the verbal persuasion. For the physiological/emotion arousal aspects, the studies based on the strategy substantially varied and contained psychological consulting, discussion and identification of concerns, encouragement and reward, empathy and caring, reflective listening, mediation techniques, humor, relaxation therapy, and emotional support by nurses and family members.
Group format and face-to-face delivery were used in most of the studies. The durations of the interventions ranged from 4 to 16 weeks, the number of education modules from 3 to 12, the length of each module from 20 to 120 minutes, and the durations of research from 1 to 6 months. Nine studies measured self-efficacy, 13 studies measured the behavior of participants, 8 studies evaluated both of the above indicators, and 6 studies detected A1C.
Outcomes
The metabolic controls
The improvement of A1C 3 months post intervention was reported in one study.Citation23 In addition, the changes in A1C between two groups were represented in five studies shown in , but the follow-up period of one study was only 1 month.Citation19,Citation20,Citation24–Citation26 The overall pooled results (3–6 months) of 508 participants suggested that A1C reduced significantly (MD: −0.62%, 95% CI: −0.92% to −0.33%, P<0.001), with a heterogeneity of I2=21%, which favored the intervention group (). A study with high risk bias was deleted for the sensitivity analysis. The results of A1C remained effective (MD: −0.78%, 95% CI: −0.87% to −0.35%, P<0.001), with a heterogeneity of I2=0%. Another study conducted in Taiwan was excluded as well. The outcomes of A1C maintained statistically significant (MD: −0.55%, 95% CI: −0.84% to −0.27%, P<0.001) with a heterogeneity of I2=32%.
Figure 2 Efficacy of self-efficacy education interventions on A1C.
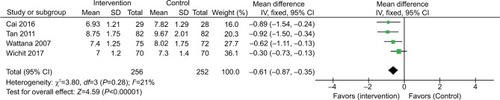
Table 2 Outcomes of included studies
The positive effects on FBG and 2 h-PG in the intervention group vs the control group were identified in three and two research studies, respectively, and these variables were improved at the end of the studies compared with the baseline.Citation27–Citation29 The weight of the patients was assessed in two studies; however, only one of them represented a significant difference between the groups.Citation25,Citation26 WC in the intervention group was found to be well-regulated compared with the control group in two studies.Citation24,Citation25 Among all the included studies, only one study involved in the positive result of BMI and a non-significant result of TC, TG, HDL-C, and LDL-C ().Citation24
Self-efficacy
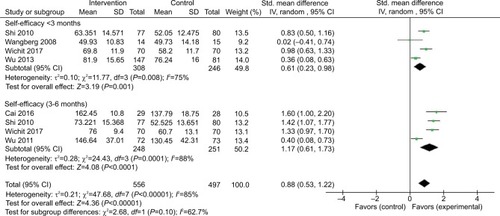
A positive impact on self-efficacy post intervention was reported in two studies.Citation13,Citation23 The foot care self-efficacy of the participants was examined and a significant difference was found. Another six studies reported the changes in self-efficacy between the two groups.Citation14,Citation17,Citation18,Citation20,Citation24,Citation25 However, the outcomes of self-efficacy were heterogeneous, namely the total self-efficacy of the participants was measured on different scales, including the Diabetes Management Self-Efficacy Scale (DMSES), the Perceived Competence Scales (PCS), and the Perceived Therapeutic Efficacy Scale (PTES) (). The pooled results (<3 months) of 554 participants revealed that self-efficacy can be improved significantly (SMD: 0.61, 95% CI: 0.23–0.98, P=0.001), and the results of 3–6 months also represented a positive effect (SMD: 1.17, 95% CI: 0.61–1.73, P<0.001) ().
Figure 3 Efficacy of self-efficacy education interventions on self-efficacy.
Behaviors
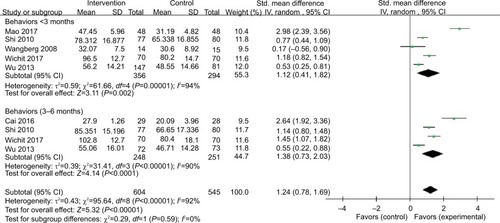
The positive self-management behavior improvements in the intervention group vs the control group were published in eleven studies,14,17,18,20,24,25,27–31 and one study identified a prominent improvement 3 months post intervention.Citation13 Similar to the results of self-efficacy, behavioral outcomes were heterogeneous, most studies employed the scale of Summary of Diabetes Self-Care Activities (SDSCA) to evaluate the self-management behaviors. The Revised Diabetes Self-Care Activity (RDSA), the Foot Self-Care Behavior Scale (FSCBC), and the Diabetes Foot Self-care Behavior Scale (DFSBS) were employed in one study, respectively. In addition, three studies examined the dietary self-management behaviors using the subscale of SDSCA (). The pooled results (<3 months) of 707 participants showed that self-management behaviors can be improve greatly (SMD: 1.12, 95% CI: 0.41–1.82, P<0.001), and the results of 3–6 months also revealed a positive effect (SMD: 1.38, 95% CI: 0.73–2.03, P<0.001) ().
Figure 4 Efficacy of self-efficacy education interventions on self-management behaviors.
Knowledge and other psychological indicators
The questionnaires employed to assess the outcome of knowledge varied substantially. The RDSA, the Diabetes Foot Knowledge Questionnaire-5 (DFKQ-5), and the Diabetes-related Knowledge Questions-24 (DKQ-24) were used in one, one, and two studies, respectively. While the remaining study employed a self-made questionnaire based on the literatures. Among the included studies, one study indicated the improvement of knowledge post intervention,Citation13 and another study assessed the foot care knowledge.Citation30 The other three studies reported changes in knowledge between the two groups ().Citation20,Citation24,Citation26 The pooled results (3–6 months) of diabetes knowledge showed a positive effect (SMD: 2.70, 95% CI: 0.63–4.78, P=0.01) ().
Figure 5 Efficacy of self-efficacy education interventions on knowledge.

For the aspect of other psychological indicators, three studies substantially varied (). Depression was measured by the Center for Epidemiology studies Short Depression scale (CES-D) in one study, but no remarkable difference between the two groups was found.Citation32 The short form version of the Depression, Anxiety and Stress Scale (DASS-21) was used in one study to evaluate the symptoms of depression, anxiety, and stress. The DASS-21 scores in the intervention group after intervention were much lower than that of the scores in the control group. In addition, the Five WHO Well-Being Index (WHO-5) was applied to inquire about the degree of depression during the past 2 weeks; however, the score of WHO-5 was not significant between the two groups.Citation25 In addition, the diabetes distress was assessed by the Diabetes Distress Scale (DDS) in one study, and the findings indicated that the DDS decreased much more in the intervention group than that in the control group.Citation31
QOL
QOL was estimated in five studies using three instruments, including the 36-item Short-Form health survey (SF-36), the Health-related quality of life Short Form-12 (SF-12), and Neuropathy and Foot Ulcer Specific Quality of Life (NFUS-QOL). Among the five studies, one study used the NFUS-QOL to assess the specific QOL of neuropathy and foot ulcer and reported significant improvements in the physical symptoms of the QOL after 3 months.Citation13 The others reported the changes in QOL between the two groups ().Citation19,Citation20,Citation24,Citation32 The pooled results (3–6 months) showed a significant improvement in QOL (SMD: 0.29, 95% CI: 0.08–0.50, P=0.008) ().
Figure 6 Efficacy of self-efficacy education interventions on quality of life.

Discussion
The present systematic review and meta-analysis were based upon 1,745 and 1,308 cases, respectively, which indicated self-efficacy-focused education was beneficial to the patients with diabetes. The self-efficacy-focused education would probably improve blood sugar level, enhance self-efficacy, promote self-management behaviors, increase knowledge, and improve the QOL. Learning strategies of self-efficacy theory including goal setting, self-management skills practicing and recording, peer models, demonstration, persuasion by health providers, and positive feedback were frequently applied in the enhancement of self-efficacy.
The effect of self-efficacy-focused education on blood sugar level in patients with diabetes was statistically positive (A1C reduced 0.61%), which approached a clinically significant level (A1C ≥0.5% was considered clinically significant).Citation33 This is superior than the previous meta-analysis of self-management interventions in T2DM patients with suboptimal blood sugar levels conducted by Li et al (A1C reduced 0.49% in 3–6 months),Citation15 and the other meta-analysis of the self-management education in T2DM patients by Norris et al (A1C decreased nearly 0.26% in 1–3 months and above).Citation34 In addition, the results of A1C by sensitivity analysis were relatively stable. It was mainly because the development and implementation of the interventions were on the basis of self-efficacy theory. Self-efficacy-focused education emphasized on improving self-efficacy of participants with diabetes, and promoting self-management behaviors which were critical for improving blood sugar levels.Citation35 There were predominant promotions of self-efficacy in <3 months and 3–6 months follow-up in the current meta-analysis, and improvements of self-management behaviors were also found. The results were unanimous with the previous reviews of diabetes self-management educationCitation36,Citation37 and psychological interventions.Citation38 However, the follow-up durations of the studies were relatively short and high-quality RCT was insufficient; thus, high-quality RCT design with long-term follow-up period should be taken into consideration for the further study. Although all studies were based on self-efficacy theory, only eight studies evaluated both self-efficacy and behaviors. It would be better to measure both self-efficacy and behavioral outcomes and to assess the linkage between them using causal modeling to help explain that self-efficacy was a crux mechanism in achieving behavioral and metabolic improvements.
Knowledge and QOL improved significantly in the current study. Nevertheless, the generalization of the findings should be careful because of the limited studies included. Knowledge provided by traditional education was necessary; however, other factors, for instance, self-efficacy, may be more effective to promote the establishment and maintenance of self-management behaviors. As a consequence, the interventions based on cognitive reframing techniques, which can preferably motivate patients, would produce better results.Citation36,Citation39 QOL was measured by SF-36 and SF-12 which were not specially designed for measuring QOL of persons with diabetes. In general, patients with diabetes often accompanied with other diseases (hypertension, hyperlipidemia, etc); hence, the scores of QOL could be easily affected and disturbed.Citation40 Consequently, a QOL instrument that is specific for patients with diabetes were urgently designed to accurately assess the effects of intervention on QOL.
The outcomes of FBG, 2 h-PG, weight, WC, BMI, plasma lipid profile, and other psychological indicators were expected to be well-analyzed by the meta-analysis, but were failed due to the lack of high-quality studies, limited studies, or heterogeneity. A positive change on the secondary outcomes of FBG and 2 h-PG through comparing the two groups was reported in several studies; however, the quality of one study was considered weak and the number of participants was limited. A meta-analysis manifested that group based self-management education can reduce the level of FBG,Citation37 but there was no strong proof supporting the effect of 2 h-PG. For other secondary outcomes, it was difficult to draw a conclusion on weight, WC, BMI, and plasma lipid profile because of the limited evidence. Likewise, it was quite difficult to determine the effects of self-efficacy-focused education on the other psychological indictors for the huge heterogeneity.
All the included studies were based on the self-efficacy theory, and almost all of them employed the performance accomplishments, vicarious experience, and verbal persuasion when developing and implementing diabetes educational interventions. The researchers of most studies were nurses rather than psychologists, which might be the main reason for the limited usage of physiological/emotion arousal and varied strategies to improve emotion state. Therefore, a multidisciplinary research group that comprised both nursing and psychology disciplines may be much better for developing and delivering the interventions based on self-efficacy theory. Strategies, such as goal setting, directly aroused and affected the motivation of behavior change.Citation12 Moreover, progressive and realistic goal setting step by step would provide a sense of successful experience for the patients. The self-management skills practicing and recording by patients may directly influence their behaviors and strengthened their experiences. The live peer models with mutual characteristics would promote the learning of patients by observing the success of others enhancing self-efficacy. What’s more, peer models may also combine with other media, such as videos and booklets, and it was noted that the experiences and characteristics of the models should be similar to the patients.Citation41 Self-management skills could be mastered through observing the demonstration from educators or group members. Verbal persuasion provided by health providers, mainly by nurses, might be related to the workforce nature of diabetes education, and a review indicated that diabetes education led by nurses could improve the blood glucose levels of patients.Citation42 Positive feedback was the critical means to guide the patients to conduct and persist the self-management behavior.
Limitations
The outcomes may be affected by several limitations. First, most included studies did not employ the RCT designs, which may influence the evidence level of pooled results. Secondly, the sample capacities of most studies were quite limited, and a number of trials had the following biases: blinding, withdrawal, or dropping out. Finally, the duration of the interventions varied greatly, and it was insufficient to determine the long-term effects of the interventions due to short durations of studies.
Conclusion
In this review, relevant data regarding self-efficacy-focused education effects were provided and mutual strategies in the self-efficacy-focused education to enhance self-efficacy, promote behavior change, and achieve optimal blood sugar level were summarized, which facilitated the studies on self-efficacy-focused education for patients with diabetes. In addition, individuals with diabetes mellitus would probably benefit from the self-efficacy-focused education. However, this review indicated that the research designs with high quality were insufficient and there existed several limitations, including short follow-up periods, deficient physiological/emotion arousal strategies, and incomplete outcome assessments. Future studies should emphasize on self-efficacy and employ the frequently used strategies including goal setting, self-management skills practicing and recording, peer models, demonstration, persuasion by health providers, positive feedback, and so on. It is high time to develop and deliver an educational intervention for patients with DM, as well as assess the outcome indicators with a high-quality study design.
Disclosure
The authors report no conflicts of interest in this work.
References
- International Diabetes FederationIDF Diabetes Atlas8th Edition2017 [updated 2018]. Available from: https://www.idf.org/our-activities/advocacy-awareness/resources-and-tools/134:idf-diabetes-atlas-8th-edition.htmlAccessed August 08, 2018
- GlasgowREOsteenVLEvaluating diabetes education. Are we measuring the most important outcomes?Diabetes Care19921510142314321425111
- BanduraAHealth promotion by social cognitive meansHealth Educ Behav200431214316415090118
- LouQWuLDaiXCaoMRuanYDiabetes education in mainland China – a systematic review of the literaturePatient Educ Couns201185333634721316898
- YuPXiaoXWangLWangLCorrelation between self-management behaviors and blood glucose control in patients with type 2 diabetes mellitus in communityZhong Nan Da Xue Xue Bao Yi Xue Ban201338442543123645245
- GuoXHYuanLLouQQA nationwide survey of diabetes education, self-management and glycemic control in patients with type 2 diabetes in ChinaChin Med J2012125234175418023217382
- WabeNTAngamoMTHusseinSMedication adherence in diabetes mellitus and self management practices among type-2 diabetics in EthiopiaN Am J Med Sci20113941842322362451
- YusuffKBObeOJosephBYAdherence to anti-diabetic drug therapy and self management practices among type-2 diabetics in NigeriaPharm World Sci200830687688318784982
- FormosaCMuscatRImproving diabetes knowledge and self-care practicesJ Am Podiatr Med Assoc2016106535235627762618
- GlasgowREToobertDJGilletteCDPsychosocial barriers to diabetes self-Management and quality of lifeDiabetes Spectrum20011413341
- BanduraASelf-efficacy: toward a unifying theory of behavioral changePsychol Rev1977842191215847061
- BanduraASocial Foundations of Thought and Action: A Social Cognitive TheoryNJPrentice Hall1986
- SharoniSKAAbdul RahmanHMinhatHSShariff GhazaliSAzman OngMHA self-efficacy education programme on foot self-care behaviour among older patients with diabetes in a public long-term care institution, Malaysia: a Quasi-experimental Pilot StudyBMJ Open201776e014393
- WuSFLeeMCLiangSYLuYYWangTJTungHHEffectiveness of a self-efficacy program for persons with diabetes: a randomized controlled trialNurs Health Sci201113333534321812879
- ChengLSitJWChoiKCChairSYLiXHeXLEffectiveness of interactive self-management interventions in individuals with poorly controlled type 2 diabetes: a meta-analysis of randomized controlled trialsWorldviews Evid Based Nurs2017141657327984672
- HampsonSESkinnerTCHartJBehavioral interventions for adolescents with type 1 diabetes: how effective are they?Diabetes Care20002391416142210977043
- ShiQOstwaldSKWangSImproving glycaemic control self-efficacy and glycaemic control behaviour in Chinese patients with type 2 diabetes mellitus: randomised controlled trialJ Clin Nurs2010193-439840420500279
- WangbergSCAn internet-based diabetes self-care intervention tailored to self-efficacyHealth Educ Res200823117017917412717
- WattanaCSrisuphanWPothibanLUpchurchSLEffects of a diabetes self-management program on glycemic control, coronary heart disease risk, and quality of life among Thai patients with type 2 diabetesNurs Health Sci20079213514117470188
- WichitNMnatzaganianGCourtneyMSchulzPJohnsonMRandomized controlled trial of a family-oriented self-management program to improve self-efficacy, glycemic control and quality of life among Thai individuals with Type 2 diabetesDiabetes Res Clin Pract2017123374827918976
- The PRISMA GroupTransparent Reporting Of Systematic Reviews and Meta-AnalysesPRISMA2018 [updated 2018]: 2018 update. Available from: http://www.prisma-statement.org/Accessed June 01, 2018
- National Collaborating Centre for Methods and ToolsQuality assessment tool for quantitative studies methodResource Details2018 [updated 2018]. Available from: http://www.nccmt.ca/knowledge-repositories/search/15Accessed June 01, 2018
- SturtJWhitlockSHearnshawHComplex intervention development for diabetes self-managementJ Adv Nurs200654329330316629914
- CaiCHuJEffectiveness of a family-based diabetes self-management educational intervention for Chinese adults with type 2 diabetes in Wuhan, ChinaDiabetes Educ201642669771127831523
- WuSFLiangSYLeeMCYuNCKaoMJThe efficacy of a self-management programme for people with diabetes, after a special training programme for healthcare workers in Taiwan: a quasi-experimental designJ Clin Nurs20142317-182515252324354787
- TanMYMagareyJMCheeSSLeeLFTanMHA brief structured education programme enhances self-care practices and improves gly-caemic control in Malaysians with poorly controlled diabetesHealth Educ Res201126589690721715653
- ZhangXAnZWangFXingFEffect analysis of the intervention by self-efficacy theory on self-management behavior of rural patients with type-2 diabetesMod Prev Med2014412138873889, 3900
- ZhaoCXingFLiHSelf-efficacy intervention on self-management actions in patients with type 2 diabetesMed J Chin PAP2016279874877
- LiDLiDXingFWangFEffect of dietary self-management of elderly diabetes using theory of serf-efficacyJ Health Psychol2013211117041706
- BiçerEKEnçNEvaluation of foot care and self-efficacy in patients with diabetes in Turkey: an interventional studyInt J Diabetes Dev Ctries2016363334344
- MaoDFangFPractice of self-efficacy intervention for elderly patients with diabetes mellitusJ Nurs Sci201732172528
- WuSFLiangSYWangTJChenMHJianYMChengKCA self-management intervention to improve quality of life and psychosocial impact for people with type 2 diabetesJ Clin Nurs20112017-182655266521605212
- UrrechagaEHigh-resolution HbA(1c) separation and hemoglobinopathy detection with capillary electrophoresisAm J Clin Pathol2012138344845622912363
- NorrisSLLauJSmithSJSchmidCHEngelgauMMSelf-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic controlDiabetes Care20022571159117112087014
- LinKParkCLiMEffects of depression, diabetes distress, diabetes self-efficacy, and diabetes self-management on glycemic control among Chinese population with type 2 diabetes mellitusDiabetes Res Clin Pract201713117918628756132
- Ricci-CabelloIRuiz-PérezIRojas-GarcíaAPastorGRodríguez-BarrancoMGonçalvesDCCharacteristics and effectiveness of diabetes self-management educational programs targeted to racial/ethnic minority groups: a systematic review, meta-analysis and meta-regressionBMC Endocr Disord20141416025037577
- SteinsbekkARyggLØLisuloMRiseMBFretheimAGroup based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysisBMC Health Serv Res20121221322824531
- ChewBHVosRCMetzendorfM-IScholtenRJPMRuttenGEHMCochrane Metabolic and Endocrine Disorders GroupPsychological interventions for diabetes-related distress in adults with type 2 diabetes mellitusCochrane Database Syst Rev2017394D11469
- EllisSESperoffTDittusRSBrownAPichertJWElasyTADiabetes patient education: a meta-analysis and meta-regressionPatient Educ Couns20045219710514729296
- SpeightJReaneyMDBarnardKDNot all roads lead to Rome – a review of quality of life measurement in adults with diabetesDiabet Med200926431532719388959
- BanduraASelf-Efficacy: The Exercise of ControlNew YorkW.H. Freeman and Company1997
- TshianangaJKKocherSWeberCErny-AlbrechtKBerndtKNeeserKThe effect of nurse-led diabetes self-management education on glycosylated hemoglobin and cardiovascular risk factors: a meta-analysisDiabetes Educ201238110812322116473