
Abstract
The importance of cultivating self-compassion is an often neglected issue among mental health professionals despite the risks to occupational well-being present in psychological care, such as burnout or compassion fatigue. In this context, this literature review has a twofold aim. Firstly, to contribute to raising awareness of the benefits of self-compassion among professionals, based on empirical research findings. Secondly, to coherently organize the available evidence on this topic, which to date appears scattered in a variety of articles. A systematic search on the APA PsycInfo database was conducted, and 24 empirical studies focused on the topic of the benefits of self-compassion in mental health professionals were finally selected. Concerning their methods, only 4 of the selected studies used experimental or quasi-experimental designs, 14 were cross-sectional studies, 3 presented qualitative research, and 3 were literature reviews. The research, regardless of methods used, points mainly to the benefits of self-compassion on the therapists’ mental health and well-being; prevention of occupational stress, burnout, compassion fatigue, and secondary traumatization as well as improvement of therapeutic competencies and professional efficacy-related aspects. In the review, self-compassion appeared as a process that could explain the benefits (eg on burnout) of cultivating other skills (eg mindfulness). To further explore this point, an additional review included 17 studies focused on the effects of mindfulness or compassion-based interventions on therapists’ self-compassion. In conclusion, our work joins those who have recommended the inclusion of self-compassion trainings in the curricula of mental health professionals.
Introduction
Self-compassion is a topic that is attracting great interest in current psychology. Following Neff’sCitation1 definition, self-compassion entails self-kindness, mindfulness, and feelings of common humanity. Self-kindness refers to an attitude of benevolence towards oneself, rather than self-criticism and self-judgment. Mindfulness involves being aware of one’s inner experiences from an open, accepting and non-judgmental perspective rather than being fused or over-identified with thoughts and emotions. Finally, the common humanity component is referred to the understanding of suffering and pain as universal aspects of the human shared experience, instead of feeling isolated, separate, strange, weird or marginalized when disturbing events occur or problematic emotions arise.
Self-compassion has been shown to be consistently associated with benefits for mental health and well-being across diverse populations.Citation2,Citation3 Specific interventions aimed to cultivate self-compassion skills, such as the Mindful Self-Compassion (MSC) programCitation4,Citation5 have even been designed. In addition, this particular training protocol, or adaptations of it, have been demonstrated as effective in several studies carried out in community samplesCitation6–8 and clinical settings.Citation9
However, the use of interventions and trainings aimed at cultivating mental health professionals’ self-compassion is not a widespread practice yet. This is rather unexpected for several reasons. First, as mentioned, self-compassion is connected with positive outcomes in the general population, and it would be similarly expected that mental health professionals would benefit from cultivating self-compassion. Second, experienced working health professionals as well as future therapists still in training and those who are in the initial stages of their professional career, are very vulnerable to psychosocial risks derived from the emotional demands implicit in their work.Citation10,Citation11 This makes them prone to burnout, compassion fatigue, and other forms of occupational stress, which are risks that self-compassion skills could contribute to prevent. Third, other interventions focused on training skills, such as mindfulness and compassion for others, have already shown that they produce benefits in mental health professionals (e.g.,Citation12–14). However, compassion towards oneself, or even a more general emphasis on self-care, seems to be often forgotten among therapists. Furthermore, as will be presented later, therapists themselves sometimes experience psychological barriers (eg, fear of stigma, irrational ideas opposed to self-care, etc.) that block the possibility of seeking help or engaging in self-compassionate practices.Citation15
Fourth, an emerging issue in the professional community is the need to “practice what is preached”.Citation16 Here, Bennett-Levy and Finlay-JonesCitation17 have emphasized that therapists in training should experience by themselves the techniques that they will later apply to their future patients or clients. This model of personal practice has at least two benefits: on a personal level, it promotes the growth of the future therapist while at a professional level it contributes to a better knowledge of the intervention strategies that are going to be used, and ultimately, it favors the development of therapeutic skills.
Why then is the topic of the need for self-compassion not more widespread as a self-care tool among therapists? A possibility is that self-compassion may be viewed as an emerging construct and self-compassion interventions are beginning just now to receive evidence-based support. However, as mentioned above, there is already a growing body of research supporting both the benefits of self-compassion and the possibility to effectively train this skill. Rather, we believe that the problem is a matter of sensitivity: mental health professionals may be not aware enough of the importance of preventing burnout and the need to protect their working life quality. The benefits of self-care, and particularly self-compassion, may have not received much attention and be unknown to many therapists. In addition, the information on these topics is sometimes scattered across a variety of sources, each looking at a particular benefit or aspect of self-compassion. It is therefore necessary to make an effort of clarification and integration of the available knowledge.
In this context, the present work aimed to carry out a systematic bibliographic review, with a twofold purpose. First, to contribute to making the benefits of a self-compassionate attitude visible among mental health professionals, based on the results obtained in empirical research. Second, to offer an integrated perspective on these benefits, identifying a series of aspects (for example, prevention of burnout, improvement of the professional’s mental health and well-being, benefits for the therapeutic relationship and for the professional’s effectiveness, etc.) where the cultivation of self-compassion has been shown to have beneficial effects or, at least, associations with positive outcomes.
Materials and Methods
A bibliography search was carried out in the abstracting and indexing database APA PsycInfo. This database contains more than five million interdisciplinary bibliographic records and it represents a major source for psychological, behavioral and social sciences research. The search was designed with the purpose of our review in mind, ie to ascertain the state of the art in research on the benefits of self-compassion in psychologists and other mental health professionals. An advanced search was carried out using the search term self-compassion OR loving-kindness to delimit the constructs of interest in the review. To delimit the professional group that represents the focus of the review, the string of terms psychologist OR counselor OR therapist OR psychiatrist OR psychiatrist OR mental health professional OR psychotherapist was used. The terms referring to constructs and professional groups were also associated with the Boolean operator AND. The complete search string had the following structure: (self-compassion OR loving-kindness) AND (psychologist OR counselor OR therapist OR psychiatrist OR mental health professional OR psychotherapist). This string was used to search in the title (TI), abstract (AB), subject (SU) and exact subject (DE) of the documents indexed in the document database. In addition, the option “apply equivalent subjects” was used as a search amplifier. As search limitations, only scientific articles published in peer-reviewed journals and in the English language be retrieved. Access to the APA PsycInfo database was carried out through the website of the library of the Pontifical University of Salamanca in May 2022.
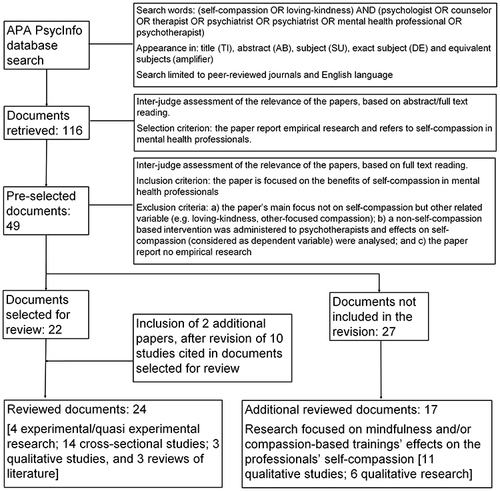
The search using these parameters yielded a total of 116 documents. Two researchers then independently carried out a first analysis to assess their relevance for the purposes of this paper based on reading the abstracts of the retrieved articles. There were only three cases of disagreement about the relevance of the records, and the researchers reached consensus after reading the full text of each document. A total of 67 papers were discarded where the focus was on self-compassion in patients, clients or the general population and not on the mental health professional community. There were 49 pre-selected documents. A second, independent filtering, based on a detailed reading of pre-selected papers’ full texts, was then carried out in order to discard papers that dealt with self-compassion only secondarily. Thus, 27 articles were discarded using the following exclusion criteria: a) the paper’s main focus was not self-compassion but another related variable (eg loving-kindness, other-focused compassion); b) a non-self-compassion based intervention was administered to psychotherapists and effects on self-compassion (considered as dependent variable) were analyzed; and c) the paper did not report empirical research (eg theoretical proposals, personal experience report, opinion article). There was no disagreement between the researchers about discarded papers in this second filtering of documents. Thus, 22 studies were finally selected from the initial PsycInfo database search. These studies were classified according to their methods, with 4 studies reporting experimental or quasi-experimental research involving the administration of a self-compassion intervention for psychotherapists or psychotherapists in training, 12 cross-sectional studies on self-compassion, conducted using samples of mental health professionals, 3 qualitative studies, and 3 literature reviews.
In addition to the documents retrieved from the PsycInfo database, 10 articles cited in papers already selected for review were also considered as candidates to be included in the literature review. A priori, these articles seemed relevant because they mentioned possible associations between self-compassion and other variables in mental health professionals. An inter-judge assessment of the relevance of these 10 new documents was carried out, based on an independent reading of full-texts. Finally, only 2 papers, reporting cross-sectional research, were selected for inclusion in the review, and 8 papers were discarded using the previously mentioned exclusion criteria. Therefore, the final sample of papers to be reviewed comprised a total of 24 empirical studies. However, we have also considered 17 out of the 27 articles that were not selected for review, in order to conduct an additional review on the effects of mindfulness and/or compassion-based interventions on therapists’ self-compassion. These studies do not address the main focus of our review (ie benefits of self-compassion), but they provide insights into how self-compassion can be increased among professionals. Although this is a topic that would merit a review in itself, we found it interesting to include these articles in our research for several reasons. First, they are studies that help contextualize the topic of self-compassion in therapists by connecting it to research on the antecedents of self-compassion. Second, these studies could provide a starting point for the identification of interesting relationships, such as the possible mediating role of self-compassion with respect to the effects of mindfulness or compassion-based training. Third, the knowledge derived from these studies may have practical and applied importance, as they identify ways to increase self-compassion in therapists. If, as hypothetically expected, the practice of self-compassion is potentially beneficial for mental health professionals, it may be equally interesting to have at least an initial idea of how therapists can become more self-compassionate. presents the systematic process followed for reviewing empirical research.
Figure 1 Systematic process followed for reviewing empirical research.
Results
Review Studies
The review studies show that the topic of the benefits of self-compassion in therapists has so far received little attention. Only three previous systematic reviews have been located, the studies by Boellinghaus et al.Citation18 Bibeau et alCitation19 and Rudaz et alCitation20 in which the possible effects of self-compassion in mental health professionals are mentioned.
The review by Boellinghaus et alCitation18 attempts to analyze the role of Mindfulness-based interventions (MBIs) and Loving-Kindness Meditation (LKM) in the cultivation of self-compassion and other-focused concern in health professionals. It focuses primarily on the effects of MBIs, since, as the authors say, at the time the review was conducted, there were no studies that included LKM or related practices in healthcare workers. However, they comment that the positive results obtained in non-clinical (non-healthcare) samples where the role of LKM is analyzed could be generalizable to healthcare personnel samples.
A similar conclusion is reached in the review by Bibeau et al,Citation19 who state that there are few studies on loving-kindness and self-compassion that focus on healthcare professionals and even fewer that focus on psychotherapists, so they take as a reference the research on the benefits of these practices in the general population. These authors call for further research on the protective effect of self-compassion and compassion meditation practices and their effects on empathy and burnout. Interestingly, they hypothesize that self-compassion meditation would reduce burnout linked to empathetic distress through better self-regulation of psychotherapists’ emotions while they are exposed to their patients’ suffering.
Rudaz et alCitation20 reviewed the effectiveness of Mindfulness-Based Stress Reduction (MBSR), Mindfulness-Based Cognitive Therapy (MBCT), Mindful Self-Compassion (MSC), and Acceptance and Commitment Therapy (ACT) to foster self-care and reduce stress in mental health professionals. They found only 2 studies, one by Finlay-Jones et alCitation16 and the other by Smeets et alCitation21 out of a total of 24 studies. The study by Smeets et alCitation21 uses a sample of first or second year psychology undergraduates, so it would not fit the aim of the present review. In any case, Smeets et alCitation21 found that the self-compassion intervention produced benefits in self-compassion, mindfulness, optimism, self-efficacy, life satisfaction and connectedness, and decreases in rumination. The study by Finlay-Jones et alCitation16 will be also mentioned in the next section (experimental and quasi-experimental research) of the present review. Among the benefits of self-compassion, Finlay-Jones et alCitation16 found that psychology trainees who participated in an online self-compassion cultivation program experienced gains in self-compassion and eudaimonic happiness, as well as reductions in stress emotion regulation difficulties. Interestingly, Rudaz et alCitation20 noted that there is potential for further investigation of the relatively young MSC program. Furthermore, they warn of the need for well-powered research, which includes randomization, active control groups, and long term follow-up that focuses on the study of mechanisms of change that are implicated in the benefits of the interventions.
Experimental and Quasi-Experimental Research on the Effects of Self-Compassion Training
The search yielded four publications in which self-compassion interventions were delivered to psychologists or graduate students and the trainings’ effects on a series of variables were analyzed.
Finlay‐Jones et alCitation16 performed pre-post comparisons and also included a 3-month follow-up. Yela et alCitation3 conducted a pre-post study using two groups with different adherence to MSC treatment. Eriksson et alCitation22 used a randomized control design. Finally, Jiménez-Gómez et alCitation23 used a randomized control design with CG active, and waitlist CG.
Two of these studies employed Internet-based programs. The “Self-compassion Online” program lasted for 6 weeks, with participants taking 1 to 2 hour per week to complete the online program and homework.Citation16 The “Internet Program Mindfulness and Compassion with Self and Others”, encompassed about 15 min of training per day, 6 days a week, for 6 weeks.Citation22 The other two studies employed the 8-week MSC protocol, with face-to-face sessions, 2.5 hours per week.Citation3,Citation23 The samples used in these intervention studies consisted of psychology graduate students,Citation16 psychologists attending graduate courses in clinical and health psychology,Citation3,Citation23 and practicing psychologists.Citation22
Significant improvements in self-compassion were obtained in all four studies (all using the 26-item SCS scale, except Eriksson et al,Citation22 that used the 12-item SCS). Two studies found pre-post improvements,Citation3,Citation16 and two studies reported improvements in relation to the waitlist CG.Citation22,Citation23 However, in the latter study the MBSR active CG did not significantly improve their self-compassion scores relative to the waitlist CG. More specifically, in the study by Eriksson et al,Citation22 a significant decrease in the SCS self-coldness factor scores was also observed in relation to the CG waitlist.
Concerning mindfulness, three trainings where this variable was assessed using the FFMQ scale reported statistically significant improvements on the participants’ levels. Eriksson et alCitation22 found significant improvements in the mindfulness total score in relation to the waitlist CG. Similarly, Yela et alCitation3 reported that graduate students with high adherence to MSC training improved their total mindfulness scores. Finally, Jiménez-Gómez et alCitation23 report that the MSC training produced significant improvements in mindfulness scores from pre- to post-training, compared with the CG waitlist.
Two papers studied the effect of self-compassion training on depression, showing a similar trend of improvement. Finlay-Jones et alCitation16 found a significant decrease in depression symptoms (using DASS-21) between pre- and post-training, with gains maintained at 3-month follow-up. Jiménez-Gómez et alCitation23 also found significant pre-to post- decreases in depression symptoms (using BDI), although such reductions did not significantly differ from the changes observed in the waitlist CG.
Two studies evaluated the effects of the self-compassion trainings on anxiety, reporting, however, less intense changes, probably due to a floor effect in the participants’ scores. Finlay-Jones et alCitation16 did not find significant pre- to post-intervention decreases (using DASS-21), although significant reductions in anxiety were observed from pre-test to 3-month follow-up. Jiménez-Gómez et alCitation23 found that the group that received MSC did not decrease their levels of anxiety (using STAI-S) from pre- to post-training. However, the waitlist CG experienced a significant increase in anxiety scores. Here, the MSC program could have had a protective effect against possible increases in anxiety during stressful periods.
The effects of training on psychologists’ perceived stress (assessed with PSS) were studied in two papers using online protocols, and beneficial effects were observed. For example, Finlay-Jones et alCitation16 found significant improvements in perceived stress symptoms from pre- to post-test, which were maintained at 3-month follow-up. Eriksson et alCitation22 also reported a significant decrease in perceived stress after the self-compassion training, in comparison with the CG waiting list. Regression analyses indicated that the SCS change-scores predicted 41.5% of the variance, and the FFMQ change-scores explained 16.1% of the additional variance.
Other benefits derived from self-compassion online interventions are the increase in emotional regulation capacity (using DERS) from pre- to post-intervention, gains that were maintained at 3-month follow-up.Citation16 Moreover, Eriksson et alCitation22 observed a significant improvement in burnout scores (using SMBQ) in relation to the waitlist CG. Remarkably, only this study assessed burnout using an experimental design. The changes in SCS accounted for 29% of the variance in burnout, whereas the FFMQ scores did not add any significant variance.
Only two studies evaluated the effects of self-compassion training on the therapists’ well-being. First, Finlay-Jones et alCitation16 found a significant pre-to post-intervention increase in happiness (measured by AHI) scores that were maintained at 3-month follow-up. Second, Yela et al,Citation3 using the PBWS, also observed significant pre-to post- changes in the global psychological well-being score in a group of psychologists with high adherence to MSC training.
It is also interesting to consider the “usability” and feedback from psychologists who received training, as reported in 2 papers. Finlay-Jones et alCitation16 informed that average ratings across the SCO program’s modules were high for enjoyableness, relevance, comprehension, and learning, with low to moderate perceived difficulty. Participants also described positive effects on their therapeutic work, including increased authenticity, responsiveness, and a greater capacity to “be present” and “practice what you preach”. Participants also reported increased resilience in the face of stress and expressed appreciation for the value of self-care practices. The main difficulty reported was the lack of time to complete the program as several participants suggested reducing the amount of content. The MSC group participants, in the study by Jiménez-Gómez et al,Citation23 reported an overall level of involvement and practice of 68.2%, high satisfaction with the program (7.7/10), and an average of 3 days per week dedicated to formal practices and 2.7 times a day doing informal practices. No differences between psychologists who received MSC and MBSR trainings were found concerning levels of satisfaction, involvement with their respective programs, and engagement with formal/informal practices.
The difference between self-compassion programs using face-to-face vs online format also deserve a comment. In general terms, the 4 studies reviewed reported significant improvements in self-compassion, mindfulness, anxiety and depression. However, if we consider the effect sizes, the increase in self-compassion was larger (Cohen’s d > 0.8) in the online programs in relation to the face-to-face training, in which intermediate effect sizes were observed (Cohen’s d > 0.50 and < 0.80). The effect sizes of mindfulness, anxiety and depression did not differ in face-to-face vs online formats. Overall, intervention studies found moderate effect-size increases for mindfulness, while improvements in anxiety and depression were mostly of small magnitude (Cohen’s d < 0.50). Concerning other effect-sizes reported in intervention studies, improvements in psychological well-beingCitation3 and stressCitation16 presented large effect sizes, and improvements in happiness, difficulty of emotional regulation and perceived stress had moderate effect sizes.Citation16,Citation22
Several meta-analysesCitation24–26 had previously indicated that self-compassion programs delivered to the general population produced overall significant moderate effect-size increases in self-compassion, mindfulness and depression, and improvements of close to moderate magnitude in anxiety. It should be noted that self-compassion programs produce changes with intermediate effect sizes on self-compassion when face-to-face sessions are used with psychologists and in the general population, while the effect size is large when working with psychologists in an online format. Effect-sizes of mindfulness are moderate in both the general population and psychologist samples. Effect-sizes of anxiety tend to be rather small in both psychologists and general population samples. Finally, changes in depression tend to be moderate in the general population but small in psychologists’ samples (probably due to a floor effect). summarizes the experimental and quasi-experimental research reviewed.
Table 1 Experimental and Quasi-Experimental Research on the Benefits of Self-Compassion
Cross-Sectional Research
The cross-sectional studies reviewed have analyzed self-compassion associations with a wide range of variables, in most cases suggesting that higher self-compassion is connected with beneficial psychological aspects. Obviously, as these are cross-sectional studies, it cannot be claimed that self-compassion causes these positive effects. However, this research serves to show that high levels of self-compassion may be linked in some way to numerous positive outcomes for mental health professionals.
In this regard, numerous studies have found a negative relationship between self-compassion and burnout scores, or burnout-related constructs such as compassion fatigue, in mental health professionals or trainees.Citation27–32 McCade et alCitation29 and Richardson et alCitation31 have used the 19-item Copenhagen Burnout Inventory (CBI)Citation33 scale, finding negative associations with self-compassion. Kotera et alCitation28 used a version of the Maslach Burnout Inventory,Citation34 with just two items to measure emotional exhaustion and depersonalization. Both components of burnout were found to be negatively related to levels of self-compassion. Some studies have used the Professional Quality of Life Scale (PROQOL) by Stamm,Citation35 which allows obtaining scores of compassion satisfaction and compassion fatigue, which in turn would include the components of burnout and secondary traumatic stress. Using this scale, Ondrejková and HalamováCitation30 found that compassion fatigue was negatively associated with total self-compassion scores and scores on two dimensions of self-compassion (ie, tolerating uncomfortable feelings and motivation to act), obtained using the Sussex-Oxford Compassion for the Self Scale (SOCS-S).Citation36 However, self-compassion was no longer a significant predictor of compassion fatigue when variables, such as self-criticism and compassion satisfaction, were included in the same regression model.Citation30 The studies by Beaumont et alCitation27 and Yip et alCitation32 also report negative associations of self-compassion with burnout and secondary traumatic stress. In these two studies, Neff’sCitation1 26-item SCS scale is used as a measure of self-compassion. From this scale Beaumont et alCitation27 and Yip et alCitation32 calculate scores for positive (self-warmth/self-kindness) and negative (self-coldness/self-judgment) components of self-compassion, which would be negatively and positively associated, respectively, with both burnout and secondary traumatic stress. Regarding compassion satisfaction, Beaumont et alCitation27 found no significant associations of this variable with self-compassion (total score), self-kindness or self-judgment. The study by Ondrejková and HalamováCitation30 does not provide information on this possible association, while Yip et alCitation32 did not use the compassion satisfaction subscale of the PROQOL.
Self-compassion has also been found to be a mediating variable in relation to professional characteristics associated with compassion fatigue or burnout. Thus, Ondrejková and HalamováCitation30 found that doctors, pedagogues, home nurses, nurses and psychologists reported higher levels of compassion fatigue, while psychotherapists and coaches reported the lowest levels. The relationship between different professions and compassion fatigue could be explained by the levels of self-criticism and self-compassion reported by different professionals. Also interesting is the result found by Kotera et alCitation28 regarding the relationship between work-life balance and emotional exhaustion -one of the dimensions of burnout-, which would be partially mediated by psychotherapists’ levels of self-compassion.
Self-compassion has also been analyzed in connection with another group of variables related to well-being and psychological symptoms that professionals may experience. Here, it has been found that higher levels of self-compassion are associated with better scores in well-being,Citation27,Citation37 while self-kindness and self-judgment are positively and negatively associated, respectively, with this construct.Citation27 Higher scores on self-compassion would further correspond with lower levels of depression,Citation29,Citation31 psychological distressCitation38 and stress.Citation39 Moreover, self-compassion could play a protective role against the onset of depressive symptoms in times of increased burnout risk. As McCade et alCitation29 reported, self-compassion acts as a moderating variable in the positive relationship between burnout and depression, finding that for psychologists with high levels of self-compassion, the connection between burnout and depression is not significant, while for those with low or moderate levels of self-compassion, a positive and significant association between burnout and depression is observed. Interestingly, Aruta et alCitation40 have informed of positive correlations between self-compassion and professionals’ attitudes and intentions towards help-seeking in case of experiencing mental health problems themselves, which may indicate that these self-compassionate professionals could better circumvent one of the barriers to help-seeking, ie the stigma attached to mental health among healthcare providers.Citation28 Especially, the connection between self-compassion and mental help-seeking attitudes seems to intensify with age, being stronger for older professionals -counselors in this case-.Citation40
Particularly interesting are the associations found in numerous studies between self-compassion and other variables that are in turn related to mental health. One of these variables is the practitioner’s mindfulness capacity, which is associated with levels of secondary traumatic stressCitation32 and psychological distress.Citation38 The studies reviewed consistently find a positive correlation between self-compassion and mindfulness.Citation38,Citation41–43 As expected, higher levels of mindfulness have been reported to be positively related to self-warmth and negatively related to self-coldness.Citation32 Moreover, the effects of mindfulness on secondary traumatic stress could be explained by considering the variables self-warmth and self-coldness in simple mediation models.Citation32 Self-critical perfectionism is another variable that has been positively associated with variables such as depression and burnout, while it would be negatively related to self-compassion.Citation31 In fact, the simple mediation models tested by Richardson et alCitation31 reveal that self-compassion would act as a partial mediator in the relationship between self-critical perfectionism and depression, and self-critical perfectionism and burnout.
Self-compassion is also associated with variables that reflect how professionals deal with potentially challenging situations. In this regard, FultonCitation42 has found a positive correlation between self-compassion and greater tolerance for ambiguity, as well as a negative correlation between self-compassion and levels of experiential avoidance. Similarly, Finlay-Jones et alCitation39 found that professional and trainee psychologists who reported higher levels of self-compassion also reported lower difficulties in emotional regulation, a construct that includes non-acceptance of emotions, difficulties engaging in goal directed behavior when upset, impulse control difficulties when upset, limited access to emotion regulation strategies, and lack of emotional clarity. Moreover, Finlay-Jones et alCitation39 found that difficulties in emotion regulation experienced by psychologists mediated the relationship between self-compassion and stress. This relationship is also interesting because it may offer a possible explanation for the mechanism through which self-compassion becomes associated with potential benefits, ie through an enhancement of emotion regulation processes.
Another group of variables analyzed in cross-sectional studies have to do with aspects that are involved in the therapeutic relationship. For example, using a sample of counseling and clinical psychology doctoral trainees, Latorre et alCitation41 found a positive association between self-compassion and self-evaluations of counselor self-efficacy and professional competency, which was maintained even controlling for other covariates such as age, gender, number of years in the doctoral program and mindfulness. In fact, this study found that self-compassion acted as a mediating variable in the relationship between mindfulness and counselor self-efficacy and self-assessed professional competency. Self-compassion is also associated with higher levels of therapeutic presence,Citation38 ie the capacity to bring one’s whole self into encounters with patients and being fully aware on multiple levels (physical, emotional, cognitive, spiritual). And again, self-compassion is found to be a variable involved in the relationship between the other two. In this regard, Bourgault & DionneCitation38 found that levels of self-compassion and psychological distress acted as parallel mediators in the relationship between mindfulness and therapeutic presence.
A separate question is whether higher levels of self-compassion on the part of the mental health professional also translate into self-perceived benefits for the patient. The results on this issue are more controversial. FultonCitation42 found that more self-compassionate counselor trainees had a perception that sessions with clients had greater depth, but practitioner levels of self-compassion did not correlate with client-rated perception of session depth or client-perceived empathy. In a similar vein, when analyzing the possible relationship between self-compassion and compassion for others in mental health professionals, the results are not entirely conclusive. For example, Beaumont et alCitation27 do not find a significant association between self-compassion and compassion for others. However, Fulton,Citation43 Roxas et alCitation37 and Yip et alCitation32 report positive correlations between self-compassion and compassion for others. FultonCitation43 further finds that levels of compassion for self mediate the relationship between mindfulness and compassion for others. Yip et alCitation32 elaborate further and report that the dimension of self-warmth, but not self-coldness, mediates the relationship between mindfulness and compassion for clients.
As presented, cross-sectional studies suggest that higher levels of self-compassion are generally associated with values indicative of better occupational health and mental health among professionals. However, the study by Tigranyan et alCitation44 found results contrary to expectations, with higher levels of self-compassion associated with greater experience of the imposter phenomenon, more perfectionism cognitions, higher anxiety, and lower achievement motives in clinical and counseling psychology doctoral students. Despite these results, the authors point to an interesting idea: self-compassion implies being kinder to oneself, but precisely that presupposes a high awareness of one’s imperfections and does not necessarily imply that one experiences lower levels of guilt or anxiety.
Finally, it is important to note that all these cross-sectional studies share some limitations derived from the methodology employed. As many of them acknowledge, a first caveat is that due to their correlational nature, the associations found between self-compassion and other variables do not imply a causal relationship, even in cases where mediational relationships are analyzed. Other widely acknowledged limitations of these studies are the difficulties in generalizing the results due to limitations in the size and/or representativeness of the sample, the use of self-report measures susceptible to being affected by the subjectivity of the participants themselves, difficulties in controlling for potential confounders, and the possible loss of nuance implied by the use of quantitative scores to analyze the professionals’ subjective experiences. In this sense, authors of the cross-sectional studies reviewed frequently recommend using experimental and longitudinal designs to clarify the relationships between variables, analyzing more complex relationships between variables, and incorporating qualitative perspectives, among other possible lines of research development.
Despite their limitations and shortcomings, these cross-sectional results are valuable in several ways. Several authors advocate the incorporation of self-compassion-based training in the curriculum of mental health professionals, in order to foster a greater awareness of the need for self-care in this group.Citation27,Citation29–32,Citation39–41,Citation43 Furthermore, they point to the possible role of self-compassion as a protective element against occupational hazards characteristic of mental health care, such as compassion fatigue, or more general problems related to stress, anxiety, and depressive symptoms. summarizes cross-sectional research on the benefits of self-compassion for mental health professionals.
Table 2 Cross-Sectional Research on the Benefits of Self-Compassion
Qualitative Research on the Benefits of Self-Compassion for Therapists
The topic of the benefits of self-compassion in mental health professionals emerged in three qualitative research studies, although in all cases the participants were counselors.Citation15,Citation45,Citation46
The participants in Barton’s studyCitation15 emphasized the demands and challenges involved in their work, especially with regard to the therapeutic relationship, and the possible risks arising from this, such as burnout. They also pointed out two interesting issues that aggravate the situation. First, therapists have the perception that their preparation and training to deal with such challenges is inadequate. In addition, therapists themselves experience barriers to self-care, for example, the idea that self-care may be selfish behavior. In this context, the need to prioritize self-care in the learning process of therapists and to have a greater awareness of the importance of self-compassion as an essential part of being a therapist is identified.
The studies by Patsiopoulos and BuchananCitation45 and Quaglia et alCitation46 agree in pointing out some benefits of self-compassion concerning the therapists’ well-being and their effectiveness in the therapeutic relationship with clients. In this regard, self-compassion would be related to a greater ability to self-observe with acceptance and kindness the therapist’s own emotional states.Citation46 This ability may offer protection against occupational stress, by identifying and coping with signs of burnout or complex therapeutic situations.Citation45 Self-compassion would also favor a greater capacity for emotional self-regulation, decreased self-criticism and perfectionism, and acceptance of one’s own limitations and uncertainty.Citation46 As a consequence, the cultivation of self-compassion would be associated with qualities such as “balance”, “clarity”, “groundedness”, “openness”, “wisdom”, “joy”, “creativity”, “freedom”, and with the perception of greater overall well-being, job satisfaction and burnout prevention.Citation45
In terms of the therapeutic relationship, the counselor’s self-compassion would also have benefits for the client. As Quaglia et alCitation46 point out, therapists’ self-compassion models self-compassion for clients. In addition, this study makes interesting contributions on how self-compassion influences compassion for others, on the maintenance of an appropriate balance between self-care and other-compassion, how elements such as the experience of shared humanity can establish a bridge between self-compassion and other-compassion. Patsiopoulos and BuchananCitation45 mention, along the same lines, broad benefits of therapists’ self-compassion in their effectiveness as professionals or in the therapeutic relationship. Basically, the therapists’ self-compassion is associated with behaviors (eg management of self-expectations, balance between counselor and client needs, proactive, preventative self-care, etc.) that derive benefits for the therapeutic relationship itself (eg greater ability to attune to their clients, a circular flow of compassion self/others, management of self- and other-directed judgment, etc.).
Finally, the qualitative research reviewed emphasizes once again the need for mental health professionals to receive training in self-compassion and self-care as elements of protection against the risks derived from professional practice. Positively, the benefits also extend to the therapist’s well-being and effectiveness as a professional. provides a summary of the qualitative studies on the benefits of self-compassion for mental health professionals reviewed.
Table 3 Qualitative Research on the Benefits of Self-Compassion for Mental Health Professionals
Additional Review. Research on the Effects of Mindfulness and Compassion-Based Interventions on the Therapists’ Self-Compassion
As presented in the Methods section, we initially discarded studies focused on the effects of mindfulness and/or compassion-based trainings on the professionals’ self-compassion. These papers analyzed the effects of interventions such as MBSR, MBCT, CCT, LKM, and other approaches, and considered self-compassion as an outcome variable. The focus of our review is rather the contrary, ie the analysis of potential effects of self-compassion. However, as the benefits of increasing the therapists’ self-compassion have been consistently identified, an additional review of interventions that likely enhance self-compassion may provide relevant information. Below, quantitative and qualitative research on such interventions is presented.
Quantitative Research on the Effects of Mindfulness and Compassion-Based Interventions on Self-Compassion
In this section we review the results of 11 publications that used quantitative methodologies to analyze the effects of different types of training on the improvement of self-compassion in psychologists/therapists in training.
A first group of studies is framed in the early years when the initial developments of mindfulness protocols were emerging. Specifically, they evaluate the effectiveness of the MBSR programCitation47 in samples of health professionals,Citation48 therapists in trainingCitation49 and a pilot study with mental healthcare professionals.Citation50 In all studies, in addition to effects on other variables, the program was found to produce significant increases in therapists’ self-compassion (SCS global scores). Moreover, Shapiro et alCitation49 found improvements in 4 of the 6 subscales of the SCS (ie, self-judgment, common humanity, isolation and over-identification). In these same early years of implementation of mindfulness programs, the pilot study by Rimes & WingroveCitation51 evaluated the effectiveness of MBCT trainingCitation52 in a group of trainee clinical psychologists. They found a significant increase in self-compassion and mindfulness scores, although not a decrease in rumination. In a qualitative section of the study, the authors identified that an increase in the acceptance of thoughts and emotions was frequently experienced as a result of the training (70%).
More recently, the effects on self-compassion produced by other types of mindfulness-based interventions have been analyzed. For instance, a quasi-experimental research using a Mindfulness for Stress Program with primary care health professionals,Citation53 a pilot study using an Intensive Mindfulness Training program with clinical psychology studentsCitation54 and a single case study using a mindfulness-based mobile intervention with a counselor.Citation55 Pizutti et alCitation53 and Schanche et alCitation54 reported, among other effects, significant improvements in the global levels of self-compassion assessed with the SCS, with the second study also finding improvements in 5 of the 6 SCS subscales (all self-compassion dimensions except common humanity). The single-case study found that the use of the Calm © app did not generate significant increases in self-compassion, although it did improve levels of burnout and mindfulness.Citation55
A second group of papers, published in 2016–2017, focused on the effects of compassion-based interventions on psychologists and therapists’ self-compassion. Here, Beaumont et alCitation13,Citation56 found a statistically significant overall increase in self-compassion scores (positive self-compassion) and a statistically significant reduction in self-critical judgment scores (negative self-compassion) after training compassion skills, using Compassion Focused Therapy (CFT)Citation56,Citation57 and Compassionate Mind Training (CMT).Citation13 Scarlet et alCitation58 conducted a pilot study where the Compassion Cultivation Training (CCT)Citation59 program was delivered to healthcare workers. Among other results, they found significant improvements in participants’ self-compassion were also found.Citation58
Finally, the study by Stafford-Brown and PakenhamCitation60 is also worth mentioning as it reported results from an ACT-informed intervention for stress management and improvement of therapist skills among clinical psychology trainees. This study showed significant differences in relation to a CG in work-related stress, distress, life satisfaction, counseling self-efficacy and therapeutic alliance, but not in self-compassion.
Qualitative Research on the Effects of Mindfulness and Compassion-Based Interventions on Self-Compassion
We found 6 publications that qualitatively analyzed the effect of various programs or strategies that produced beneficial effects on mental health professionals’ self-compassion. All these studies used small samples and relied on interpretative analysis strategies aimed at identifying emerging topics from the participants’ discourse. Interestingly, among other topics, increases in self-compassion are reported in these studies.
Two studies focused on Loving-Kindness Meditation (LKM) trainings. Boellinghaus et alCitation61 worked with twelve therapists-in-training who had previously attended a mindfulness-based cognitive therapy course and participated in a 6-week LKM course. Using interpretative phenomenological analysis, five main themes emerged from the participants’ responses to an interview. In particular, the beneficial impact of the training on the self (self-awareness, self-compassion, self-confidence) was identified as a relevant topic. The authors noted that LKM training could contribute, among other benefits, to enhance self-care and compassion. Bibeau et alCitation62 analyzed qualitative data from three psychotherapists who had already been practicing regular mindfulness meditation and engaged in a compassion meditation training over a 4-week period. The core content of these exercises was LKM. They carried out semi-structured interviews and conducted a phenomenological analysis of responses before, after and at 1-month follow-up. The therapists perceived that the compassion meditation training had an effect on their self-compassion skills. In their narratives, self-compassion appeared as the basis of their compassion for others, and as the key factor that enabled them to be more present, accepting and tolerant of their clients’ suffering. The narrative themes identified were very similar to those in the Boellinghaus et alCitation61 study. Among the conclusions, the authors proposed to include compassion meditation training in the psychotherapy training curricula, as well as in burnout prevention workshops.
Other two studies assessed the effects of mindfulness programs. Dorian and KillebrewCitation63 evaluated the impact of a 10-week mindfulness course delivered to 21 psychotherapists in training, using the Constant Comparative MethodCitation64 to analyze the participants’ self-reported experiences during those weeks. Most students stated that the mindfulness practice had helped them gain acceptance, compassion for self and others, and had increased their capacity for attention and awareness. Similarly, Felton et alCitation65 studied the impact of an MBSR-based program in a group of 41 students from a master’s degree in mental health counseling. They used conventional content analysis.Citation66 Participants described that, among other effects, they increased their capacity for self-compassion.
Finally, two studies evaluated the effects of the CFT program.Citation57 Gale et alCitation67 conducted an exploratory study in a sample of 10 therapists, aimed at assessing the effect of personal practice with the CFT program. Their responses to a semi-structured interview were analyzed using inductive thematic analysis and five main themes emerged. In particular, personal practice was said to improve both compassion for others and self-compassion. Although CFT was mainly designed to increase compassion, this protocol also produced improvements in self-compassion. The authors suggested using RCT designs and larger samples to further examine CFT-based training’s benefits. Similarly, Bell et alCitation68 studied the effect of an adaptation of the CFT program among 7 cognitive-behavioral therapists. The researchers used Interpretative Phenomenological Analysis to analyze the participants’ responses to an interview about their programs’ experiences. The enhancement of self-compassion and emotion regulation skills emerged, among other themes, as a benefit of the training. summarizes qualitative research on the effect of mindfulness and compassion-based interventions on the therapists’ self-compassion.
Table 4 Qualitative Research on the Effect of Mindfulness and Compassion-Based Interventions on the Therapists’ Self-Compassion
Discussion
Self-compassion may contribute to important benefits for mental health professionals, as the research reviewed highlights.
First, self-compassion may be a protective element against psychosocial risks that are present in therapeutic work, such as compassion fatigue, burnout, or secondary traumatic stress. In this regard, compassion is also a factor contributing to the quality of working life. Cross-sectional research is consistent in pointing to a negative relationship between self-compassion and these risks associated with therapeutic work (e.g.Citation27–32). Interestingly, self-compassion may act as a protective element against the development of depressive symptoms when the professional is exposed to high levels of burnout.Citation29 In addition, self-compassion appeared linked to a better balance between professional and personal life, with self-compassion mediating the relationship between work-life balance and emotional exhaustion.Citation28 From a qualitative perspective, Patsiopoulos and BuchananCitation45 have also mentioned, among the benefits of self-compassion, better management of occupational stress and challenges involved at therapeutic work. Here, compassion is a factor contributing to quality of working life. These results are consistent with intervention studies. For instance, Eriksson et alCitation22 found that an Internet-based program aimed at cultivating mindfulness and compassion for self and others produced significant decreases in perceived stress and burnout symptoms in practicing psychologists. In addition, changes in these variables were more strongly associated with self-coldness than self-warmth, ie the self-compassion’s negative and positive dimensions respectively. Finlay-Jones et alCitation16 found that psychology trainees who received online training in self-compassion described positive effects on their therapeutic work, increased resilience to stress, recognition of the value of self-care practices, increased authenticity, responsiveness, and an increased ability to “be present” and “practice what you preach”.
Second, self-compassion is also associated, in general, with numerous benefits for the psychological well-being and mental health of professionals. For example, cross-sectional research has negatively connected self-compassion with depression, psychological distress (e.g.,Citation29,Citation31,Citation38,Citation39) and positively with well-being.Citation27,Citation37 Again, qualitative research points in the same direction, finding that one of the benefits of self-compassion refers to the overall feeling of well-being and the perception of physical, psychological and emotional health.Citation45 There is also robust evidence from four experimental and quasi-experimental studiesCitation3,Citation16,Citation22,Citation23 indicating that training self-compassion not only significantly improves self-compassion and mindfulness skills but also reduces anxiety and depression. In addition, some intervention studies reported improvements in psychological well-being,3 happiness, and less stress and emotional regulation difficulties.Citation16
Third, self-compassion appeared related to experiential avoidance, acceptance, and tolerance of uncertainty or ambiguity. These results have been repeatedly obtained in cross-sectional research,Citation39,Citation42 and have been similarly echoed in qualitative research.Citation46 The connections between self-compassion and such processes (ie lower experiential avoidance, higher tolerance to uncertainty) could contribute to explain self-compassion beneficial effects. For instance, Yela et alCitation8 found that the reductions in experiential avoidance after a Mindful Self-Compassion (MSC) program delivered to a community sample accounted for changes in depression, anxiety and well-being in a study conducted. However, this suggestion is yet to be tested in a mental health professionals’ sample.
Fourth, self-compassion itself is a variable that has been frequently proposed as an explanatory variable for psychological benefits linked to other variables, such as the negative association between mindfulness and burnout. This is a result that has appeared several times in cross-sectional research that has conducted mediation analyses, finding that self-compassion would be involved in the processes that explain the salutary effects of mindfulness in mental health professionals. For example, self-compassion mediates the relationship between profession and compassion fatigue,Citation30 between self-critical perfectionism and burnout or depression,Citation31 and mindfulness and burnout-related variables.Citation32 Hence, self-compassion is revealed as a psychological mechanism that may underlie the positive effects derived from other variables.
Fifth, therapists who receive training in mindfulness or compassion-based programs also experience improvements in their levels of self-compassion. Here, evidence again comes from both quantitative and qualitative research. Training professionals in compassion skills (eg using CFT, CCT or other compassion-focused programs) has demonstrated benefits in self-compassion too.Citation13,Citation56,Citation58 The effect of mindfulness-based interventions (MBSR and MBCT) on increasing self-compassion scores has been widely reported.Citation48–51,Citation53–55 To date, only one controlled study has compared the effects of a mindfulness program (MBSR) with a self-compassion program (MSC) among psychotherapists in training.Citation23 This research found that mindfulness and self-compassion scores presented similar trajectories in MBSR and MSC groups from pre- to post-training, with participants in both the MBSR and in the MSC groups significantly improving their self-compassion scores. However, when the comparison with a control group was taken into account, each program appeared to produce effects on those skills more directly trained. The MBSR program produced significant effects on mindfulness but not on self-compassion, whereas the MSC program enhanced self-compassion and mindfulness, compared to CG.
Concerning qualitative studies, from the participants’ discourse emerges the idea that trainings in compassion,Citation62,Citation67,Citation68 mindfulnessCitation63,Citation65 and LKMCitation61 enhance the professionals’ self-compassion. These results must be interpreted with caution, as all qualitative studies used very small and non-representative samples. However, these studies may constitute a basis for designing new research and provide us with a subjective but valuable perspective often neglected, ie the access to the participants’ self-reported experiences prior, during and after this kind of training.
Sixth, the beneficial effects of being a self-compassionate therapist do not exclusively redound to the professional, but also have positive effects on the therapeutic relationship and the clients themselves. In fact, self-compassion is related to compassion towards clients, therapeutic efficacy and the competence of the practitioner. This result has repeatedly appeared in cross-sectional research (e.g.,Citation32,Citation37,Citation38,Citation41–43). In addition, self-compassion has been found to explain, to some extent, the association between mindfulness and self-efficacy, self-rated professional competence,Citation41 therapeutic presence,Citation38 compassion for others,Citation43 and compassion to clients.Citation32 However, the results cannot be said to be conclusive. Firstly, these are studies that rely on self-report measures and therapists’ perceptions have sometimes been found to be at odds with those of clients (e.g.Citation42). On other occasions, the association between self-compassion and compassion for others has not been found to be significant (e.g.27). Qualitative research has also pointed to beneficial effects of self-compassion on aspects related to therapeutic competence and the establishment of an effective therapeutic relationship.Citation45,Citation46 However, due to the characteristics of these studies, these findings are based on the subjective assessments of the practitioners, and the client’s perspective is yet to be incorporated.
Seventh, the positive effects derived from a self-compassionate attitude make it a priority to train this quality during the training of therapists. This idea was derived from the discourse of the participants in Barton’s qualitative study.Citation15 However, this recommendation is also frequently mentioned in cross-sectional research’s conclusions,Citation27,Citation30–32,Citation40,Citation41 especially when self-compassion is viewed as a protective element against potential occupational risks such as burnout or compassion fatigue. Similar recommendations are also shared by authors of the most rigorous experimental and quasi-experimental studies,Citation3,Citation16,Citation22,Citation23 who defend that future clinical psychologists should receive training in self-compassion during their education.
Eight, there are however psychological barriers among therapists that may make them wary of cultivating self-compassion. For example, the idea that being self-compassionate is selfish, as identified in the qualitative study by Barton.Citation15 However, when the therapist is self-compassionate, this disposition can lead to the breaking down of other barriers that mental health professionals sometimes encounter. For example, Aruta et alCitation40 found in a cross-sectional study that self-compassion is positively associated with mental-help seeking intentions and attitudes, thus contributing to the search for effective solutions to situations compromising the professionals’ mental health, an issue that even today is perceived as stigmatizing. The practice of self-compassion may also entail difficulties and may even be aversive for some individuals. For example, in the context of the MSC program, the backdraft effect has been identified,Citation3,Citation9 in which the practice of self-compassion elicits the activation of difficult emotions. Self-compassionate practices can make the person aware of wounds and fears that had remained hidden and that may painfully emerge during the training. This effect is not seen as necessarily negative;Citation3 on the contrary, it may be part of the process of generating a self-compassionate attitude. In any case, these possible effects lead us to emphasize the convenience that the trainings be supervised by experts.Citation9,Citation61
Limitations and Future Research
We have also identified some limitations in our review of previous literature. Research, in general, on the topic of the benefits of self-compassion in mental health professionals is scarce. For instance, only four studies used experimental or quasi-experimental designs to address the topic of the potential benefits of self-compassion interventions delivered to therapists. There has been an evolution, however, concerning this point. The first intervention studies agreed on the need to carry out RCT studies comparing the effect of self-compassion interventions with an alternative stress-management intervention and a waitlist control group.Citation3,Citation16,Citation22 Another remarkable development is the analysis of processes that may account for the effects of self-compassion interventions. For example, Finlay-Jones et alCitation39 conducted mediation analyses and found that difficulties in emotional regulation mediated the beneficial effect of self-compassion training on stress. However, as Finlay-Jones et alCitation16 and Jiménez-Gómez et alCitation23 suggested, more experimental research on mediation processes accounting for the beneficial effects of self-compassion interventions is needed.
As a conclusion, future research should conduct more RCT studies with active CG, using larger samples of mental health professionals, with follow-ups, and focused not only on self-compassion benefits but also on identifying possible mediating variables involved in the positive outcomes. In addition, using objective psychophysiological measures, such as cortisol,Citation16 is recommended.
Most of the research reviewed used cross-sectional designs, which allows identifying associations between self-compassion and other variables, but does not unequivocally determine whether self-compassion causes beneficial outcomes. However, cross-sectional research is valuable and may well serve to complement findings obtained using other research designs.
Qualitative research is also scarce. Although research using qualitative methods is sometimes mistakenly considered to provide lower quality results, we would like to highlight the value of this type of research. Qualitative designs allow a very direct access to the subjectivity of therapists, and allow us to know first-hand how professionals experience issues such as the need for self-compassion, difficulties in the therapeutic relationship, the emotional demands present in their work, etc. From this point of view, this type of research has an important heuristic value. For example, by suggesting hypotheses that can be further analyzed using other methods. In addition, qualitative research has an applied interest, providing information on how participants in self-compassion programs experience the different sessions and practices. They can even identify barriers to self-compassion, often based on inappropriate beliefs about self-compassion. For example, as BartonCitation15 identified, the idea that being self-compassionate is a form of selfishness.
The research reviewed involves a heterogeneous group of helping-professionals or mental health professionals in general, but there could be differences between specific groups (psychologists, therapists, counselors, psychiatrists, etc.), as Ondrejková & HalamováCitation30 have identified. Emotional demands at work may depend on the type of care the professionals provide, the type of problems they deal with, their previous training, etc. Therefore, research focused on particular professional collectives is encouraged. This point would allow us to better understand specific needs of different professionals and design self-care and self-compassion interventions focused on their concrete circumstances and objectives.
Concerning the samples used in previous studies, we noticed that many of them have been conducted among trainee therapists. Likely, this is due to this collective being more accessible to researchers working in university contexts. For instance, experimental and quasi-experimental studies of self-compassion training mostly relied on samples of psychologists in training, with only Eriksson et alCitation22 using a sample of practicing psychologists. Of course, delivering self-compassion interventions to psychologists in training is highly valuable. Psychologists may be especially vulnerable to burnout and professional risks in early stages of their career, and this sort of interventions may play a preventive role. In addition, participating in a self-compassion program and experiencing sessions, techniques, and procedures is a valuable method of learning. As presented, numerous researchers in the field of professional self-care have highlighted the importance of providing training in the cultivation of self-compassion to future therapists as part of their curriculum. These authors’ suggestions are consistent with recent proposals encouraging the need of personal practice as a means to promote personal development and enhance professional skills.Citation17
However, these points should not make us forget that more research involving practicing mental health professionals with professional experience is desirable, as working psychologists also face daily emotional challenges. Here, few studies have analyzed the effects of being a self-compassionate therapist on patients/clients and have measured the therapists’ effectiveness at work. It is therefore necessary to analyze, preferably using experimental designs, the effects of self-compassion trainings on professional performance, burnout, compassion fatigue, psychological flexibility, therapist’s empathy or client evaluation of the therapeutic relationship.
Finally, when conducting the present review of literature, we have also found a limitation of a conceptual nature, derived from the proximity of self-compassion and other constructs such as self-love, self-care, compassion for others, loving-kindness, etc. This sometimes makes it difficult to determine whether several studies are referring to the same or different constructs. In this regard, a work of reflection and concept clarification of the semantic domain of (self)compassion is yet to be done.
Conclusions
Our review contributes to highlight the importance of self-compassion among mental health professionals. Although this is an area on which research is currently emerging, the results of studies of different methodological nature seem to converge in pointing out the benefits of self-compassion in this collective. Being self-compassionate is associated, in general, with better levels of mental health and well-being. In addition, self-compassion may act as a protective factor against psychosocial occupational risks to which therapists are potentially exposed, such as burnout and secondary traumatic stress. A self-compassionate attitude could also have a positive effect on aspects such as the professionals’ self-efficacy and competence and the quality of the therapeutic relationship itself. All aspects mentioned above make it highly advisable to include training in self-compassion in the curriculum of mental health professionals, since, like any other skill, it needs to be well understood and practiced in order to overcome possible difficulties and obtain the greatest benefits. In any case, as mentioned, this is an area where much more research is still needed, especially of an experimental nature.
Disclosure
The authors report no conflicts of interest in this work.
References
- Neff KD. The development and validation of a scale to measure self-compassion. Self Identity. 2003;2(3):223–250. doi:10.1080/15298860309027
- Bluth K, Neff KD. New frontiers in understanding the benefits of self-compassion. Self Identity. 2018;17(6):605–608. doi:10.1080/15298868.2018.1508494
- Yela JR, Gómez-Martínez MÁ, Crego A, Jiménez L. Effects of the Mindful Self-Compassion programme on clinical and health psychology trainees’ well-being: a pilot study. Clin Psychol. 2020;24:41–54. doi:10.1111/cp.12204
- Germer CK, Neff K. Teaching the Mindful Self-Compassion Program: A Guide for Professionals. Guilford Press; 2019.
- Neff K, Germer CK. The Mindful Self-Compassion Workbook: A Proven Way to Accept Yourself, Build Inner Strength, and Thrive. Guilford Press; 2018.
- Kirby JN. Compassion interventions: the programmes, the evidence, and implications for research and practice. Psychol Psychother Theory Res Pract. 2017;90(3):432–455. doi:10.1111/papt.12104
- Neff KD, Germer CK. A Pilot Study and Randomized Controlled Trial of the Mindful Self-Compassion Program: a Pilot and Randomized Trial of MSC Program. J Clin Psychol. 2013;69(1):28–44. doi:10.1002/jclp.21923
- Yela JR, Crego A, Buz J, Sánchez‐Zaballos E, Gómez‐Martínez MÁ. Reductions in experiential avoidance explain changes in anxiety, depression and well‐being after a mindfulness and self‐compassion (MSC) training. Psychol Psychother Theory Res Pract. 2022;95(2):402–422. doi:10.1111/papt.12375
- Germer CK, Neff KD. Self-Compassion in Clinical Practice: self-Compassion. J Clin Psychol. 2013;69(8):856–867. doi:10.1002/jclp.22021
- Lim N, Kim EK, Kim H, Yang E, Lee SM. Individual and work-related factors influencing burnout of mental health professionals: a meta-analysis. J Employ Couns. 2010;47(2):86–96. doi:10.1002/j.2161-1920.2010.tb00093.x
- Volpe U, Luciano M, Palumbo C, Sampogna G, Del Vecchio V, Fiorillo A. Risk of burnout among early career mental health professionals: burnout in early career phases. J Psychiatr Ment Health Nurs. 2014;21(9):774–781. doi:10.1111/jpm.12137
- Askey-Jones R. Mindfulness-based cognitive therapy: an efficacy study for mental health care staff. J Psychiatr Ment Health Nurs. 2018;25(7):380–389. doi:10.1111/jpm.12472
- Beaumont E, Rayner G, Durkin M, Bowling G. The effects of compassionate mind training on student psychotherapists. J Ment Health Train Educ Pract. 2017;12(5):300–312. doi:10.1108/JMHTEP-06-2016-0030
- Lomas T, Medina JC, Ivtzan I, Rupprecht S, Eiroa-Orosa FJ. A systematic review of the impact of mindfulness on the well-being of healthcare professionals. J Clin Psychol. 2018;74(3):319–355. doi:10.1002/jclp.22515
- Barton H. An exploration of the experiences that counsellors have of taking care of their own mental, emotional and spiritual well‐being. Couns Psychother Res. 2020;20(3):516–524. doi:10.1002/capr.12280
- Finlay-Jones A, Kane R, Rees C. Self-Compassion Online: a Pilot Study of an Internet-Based Self-Compassion Cultivation Program for Psychology Trainees: pilot Study of Online Self-Compassion Training. J Clin Psychol. 2017;73(7):797–816. doi:10.1002/jclp.22375
- Bennett-Levy J, Finlay-Jones A. The role of personal practice in therapist skill development: a model to guide therapists, educators, supervisors and researchers. Cogn Behav Ther. 2018;47(3):185–205. doi:10.1080/16506073.2018.1434678
- Boellinghaus I, Jones FW, Hutton J. The role of mindfulness and loving-kindness meditation in cultivating self-compassion and other-focused concern in health care professionals. Mindfulness. 2014;5(2):129–138. doi:10.1007/s12671-012-0158-6
- Bibeau M, Dionne F, Leblanc J. Can Compassion Meditation Contribute to the Development of Psychotherapists’ Empathy? A Review. Mindfulness. 2016;7(1):255–263. doi:10.1007/s12671-015-0439-y
- Rudaz M, Twohig MP, Ong CW, Levin ME. Mindfulness and acceptance-based trainings for fostering self-care and reducing stress in mental health professionals: a systematic review. J Context Behav Sci. 2017;6(4):380–390. doi:10.1016/j.jcbs.2017.10.001
- Smeets E, Neff K, Alberts H, Peters M. Meeting Suffering With Kindness: effects of a Brief Self-Compassion Intervention for Female College Students: self-Compassion Intervention for Students. J Clin Psychol. 2014;70(9):794–807. doi:10.1002/jclp.22076
- Eriksson T, Germundsjö L, Åström E, Rönnlund M. Mindful Self-Compassion Training Reduces Stress and Burnout Symptoms Among Practicing Psychologists: a Randomized Controlled Trial of a Brief Web-Based Intervention. Front Psychol. 2018;9:2340. doi:10.3389/fpsyg.2018.02340
- Jiménez-Gómez L, Yela JR, Crego A, Melero-Ventola AR, Gómez-Martínez MÁ. Effectiveness of the Mindfulness-Based Stress Reduction (MBSR) vs. the Mindful Self-Compassion (MSC) Programs in Clinical and Health Psychologist Trainees. Mindfulness. 2022;13(3):584–599. doi:10.1007/s12671-021-01814-2
- Kirby JN, Tellegen CL, Steindl SR. A Meta-Analysis of Compassion-Based Interventions: current State of Knowledge and Future Directions. Behav Ther. 2017;48(6):778–792. doi:10.1016/j.beth.2017.06.003
- Ferrari M, Hunt C, Harrysunker A, Abbott MJ, Beath AP, Einstein DA. Self-Compassion Interventions and Psychosocial Outcomes: a Meta-Analysis of RCTs. Mindfulness. 2019;10(8):1455–1473. doi:10.1007/s12671-019-01134-6
- Wilson AC, Mackintosh K, Power K, Chan SWY. Effectiveness of Self-Compassion Related Therapies: a Systematic Review and Meta-analysis. Mindfulness. 2019;10(6):979–995. doi:10.1007/s12671-018-1037-6
- Beaumont E, Durkin M, Hollins Martin CJ, Carson J. Measuring relationships between self-compassion, compassion fatigue, burnout and well-being in student counsellors and student cognitive behavioural psychotherapists: a quantitative survey. Couns Psychother Res. 2016;16(1):15–23. doi:10.1002/capr.12054
- Kotera Y, Maxwell-Jones R, Edwards AM, Knutton N. Burnout in Professional Psychotherapists: relationships with Self-Compassion, Work–Life Balance, and Telepressure. Int J Environ Res Public Health. 2021;18(10):5308. doi:10.3390/ijerph18105308
- McCade D, Frewen A, Fassnacht DB. Burnout and depression in Australian psychologists: the moderating role of self-compassion. Aust Psychol. 2021;56(2):111–122. doi:10.1080/00050067.2021.1890979
- Ondrejková N, Halamová J. Prevalence of compassion fatigue among helping professions and relationship to compassion for others, self‐compassion and self‐criticism. Health Soc Care Community. 2022;hsc.13741. doi:10.1111/hsc.13741
- Richardson CME, Trusty WT, George KA. Trainee wellness: self-critical perfectionism, self-compassion, depression, and burnout among doctoral trainees in psychology. Couns Psychol Q. 2020;33(2):187–198. doi:10.1080/09515070.2018.1509839
- Yip SYC, Mak WWS, Chio FHN, Law RW. The Mediating Role of Self-Compassion Between Mindfulness and Compassion Fatigue Among Therapists in Hong Kong. Mindfulness. 2017;8(2):460–470. doi:10.1007/s12671-016-0618-5
- Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress. 2005;19(3):192–207. doi:10.1080/02678370500297720
- West CP, Dyrbye LN, Satele DV, Sloan JA, Shanafelt TD. Concurrent Validity of Single-Item Measures of Emotional Exhaustion and Depersonalization in Burnout Assessment. J Gen Intern Med. 2012;27(11):1445–1452. doi:10.1007/s11606-012-2015-7
- Stamm BH Profesional quality of life: compassion satisfaction and fatigue version 5 (ProQOL); 2009. Available from: proqol.org. Accessed September 9, 2022.
- Gu J, Baer R, Cavanagh K, Kuyken W, Strauss C. Development and Psychometric Properties of the Sussex-Oxford Compassion Scales (SOCS). Assessment. 2020;27(1):3–20. doi:10.1177/1073191119860911
- Roxas MM, David AP, Aruta JJBR. Compassion, Forgiveness and Subjective Well-Being among Filipino Counseling Professionals. Int J Adv Couns. 2019;41(2):272–283. doi:10.1007/s10447-019-09374-w
- Bourgault M, Dionne F. Therapeutic Presence and Mindfulness: mediating Role of Self-Compassion and Psychological Distress among Psychologists. Mindfulness. 2019;10(4):650–656. doi:10.1007/s12671-018-1015-z
- Finlay-Jones AL, Rees CS, Kane RT. Self-Compassion, Emotion Regulation and Stress among Australian Psychologists: testing an Emotion Regulation Model of Self-Compassion Using Structural Equation Modeling. PLoS One. 2015;10(7):e0133481. doi:10.1371/journal.pone.0133481
- Aruta JJBR, Maria A, Mascarenhas J. Self-compassion promotes mental help-seeking in older, not in younger, counselors. Curr Psychol. 2022. doi:10.1007/s12144-022-03054-6
- Latorre C, Leppma M, Platt LF, Shook N, Daniels J. The relationship between mindfulness and self-compassion for self-assessed competency and self-efficacy of psychologists-in-training. Train Educ Prof Psychol. 2021. doi:10.1037/tep0000395
- Fulton CL. Mindfulness, Self-Compassion, and Counselor Characteristics and Session Variables. J Ment Health Couns. 2016;38(4):360–374. doi:10.17744/mehc.38.4.06
- Fulton CL. Self-compassion as a mediator of mindfulness and compassion for others. Couns Values. 2018;63(1):45–56. doi:10.1002/cvj.12072
- Tigranyan S, Byington DR, Liupakorn D, et al. Factors related to the impostor phenomenon in psychology doctoral students. Train Educ Prof Psychol. 2021;15(4):298–305. doi:10.1037/tep0000321
- Patsiopoulos AT, Buchanan MJ. The practice of self-compassion in counseling: a narrative inquiry. Prof Psychol Res Pract. 2011;42(4):301–307. doi:10.1037/a0024482
- Quaglia JT, Cigrand C, Sallmann H. Caring for you, me, and us: the lived experience of compassion in counselors. Psychotherapy. 2021. doi:10.1037/pst0000412
- Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4(1):33–47. doi:10.1016/0163-8343(82
- Shapiro SL, Astin JA, Bishop SR, Cordova M. Mindfulness-Based Stress Reduction for Health Care Professionals: results From a Randomized Trial. Int J Stress Manag. 2005;12(2):164–176. doi:10.1037/1072-5245.12.2.164
- Shapiro SL, Brown KW, Biegel GM. Teaching self-care to caregivers: effects of mindfulness-based stress reduction on the mental health of therapists in training. Train Educ Prof Psychol. 2007;1(2):105–115. doi:10.1037/1931-3918.1.2.105
- Raab K, Sogge K, Parker N, Flament MF. Mindfulness-based stress reduction and self-compassion among mental healthcare professionals: a pilot study. Ment Health Relig Cult. 2015;18(6):503–512. doi:10.1080/13674676.2015.1081588
- Rimes KA, Wingrove J. Pilot Study of Mindfulness-Based Cognitive Therapy for Trainee Clinical Psychologists. Behav Cogn Psychother. 2011;39(2):235–241. doi:10.1017/S1352465810000731
- Segal ZV, Williams JMG, Teasdale JD. Mindfulness-Based Cognitive Therapy for Depression: A New Approach to Preventing Relapse. Guilford Press; 2002.
- Pizutti LT, Carissimi A, Valdivia LJ, et al. Evaluation of Breathworks’ Mindfulness for Stress 8‐week course: effects on depressive symptoms, psychiatric symptoms, affects, self‐compassion, and mindfulness facets in Brazilian health professionals. J Clin Psychol. 2019;75(6):970–984. doi:10.1002/jclp.22749
- Schanche E, Vøllestad J, Binder PE, et al. Can clinical psychology students benefit from brief and intensive mindfulness training? Couns Psychother Res. 2020;20(2):311–324. doi:10.1002/capr.12273
- Callender KA, Trustey CE, Alton L, Hao Y. Single Case Evaluation of a Mindfulness-Based Mobile Application with a Substance Abuse Counselor. Couns Outcome Res Eval. 2021;12(1):16–29. doi:10.1080/21501378.2019.1686353
- Beaumont E, Irons C, Rayner G, Dagnall N. Does Compassion-Focused Therapy Training for Health Care Educators and Providers Increase Self-Compassion and Reduce Self-Persecution and Self-Criticism? J Contin Educ Health Prof. 2016;36(1):4–10. doi:10.1097/CEH.0000000000000023
- Gilbert P. Compassion Focused Therapy: Distinctive Features. Routledge; 2010.
- Scarlet J, Altmeyer N, Knier S, Harpin RE. The effects of Compassion Cultivation Training (CCT) on health‐care workers. Clin Psychol. 2017;21(2):116–124. doi:10.1111/cp.12130
- Jazaieri H, Jinpa GT, McGonigal K, et al. Enhancing compassion: a randomized controlled trial of a compassion cultivation training program. J Happiness Stud. 2013;14(4):1113–1126. doi:10.1007/s10902-012-9373-z
- Stafford-Brown J, Pakenham KI. The Effectiveness of an ACT Informed Intervention for Managing Stress and Improving Therapist Qualities in Clinical Psychology Trainees: stress Management in Clinical Psychology Trainees. J Clin Psychol. 2012;68(6):592. doi:10.1002/jclp.21844
- Boellinghaus I, Jones FW, Hutton J. Cultivating self-care and compassion in psychological therapists in training: the experience of practicing loving-kindness meditation. Train Educ Prof Psychol. 2013;7(4):267–277. doi:10.1037/a0033092
- Bibeau M, Dionne F, Riera A, Leblanc J. The Influence of Compassion Meditation on the Psychotherapist’s Empathy and Clinical Practice: a Phenomenological Analysis. J Humanist Psychol. 2020;002216782095325. doi:10.1177/0022167820953258
- Dorian M, Killebrew JE. A Study of Mindfulness and Self-Care: a Path to Self-Compassion for Female Therapists in Training. Women Ther. 2014;37(1–2):155–163. doi:10.1080/02703149.2014.850345
- Glaser BG. The Constant Comparative Method of Qualitative Analysis. Soc Probl. 1965;12(4):436–445. doi:10.1525/sp.1965.12.4.03a00070
- Felton TM, Coates L, Christopher JC. Impact of Mindfulness Training on Counseling Students’ Perceptions of Stress. Mindfulness. 2015;6(2):159–169. doi:10.1007/s12671-013-0240-8
- Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
- Gale C, Schröder T, Gilbert P. ‘Do You Practice What You Preach?’ A Qualitative Exploration of Therapists’ Personal Practice of Compassion Focused Therapy: personal Practice and CFT. Clin Psychol Psychother. 2017;24(1):171–185. doi:10.1002/cpp.1993
- Bell T, Dixon A, Kolts R. Developing a compassionate internal supervisor: compassion-focused therapy for trainee therapists: developing a compassionate internal supervisor. Clin Psychol Psychother. 2017;24(3):632–648. doi:10.1002/cpp.2031