
Abstract
Background
Gestational diabetes mellitus (GDM) is a condition that causes poor glucose tolerance during pregnancy and usually resolves after birth. Having GDM impacts the mother and baby. Smartphone-based lifestyle interventions may offer innovative solutions.
Aim
To examine the effects of smartphone-based lifestyle interventions on compliance, Hemoglobin A1c (HbA1c), maternal outcomes, infant outcomes, psychological status, satisfaction, and cost effectiveness among women with GDM.
Methods
Randomized controlled trials (RCTs) of smartphone-based lifestyle interventions for women with GDM aged over 18 years were included. A systematic search of PubMed, Embase, Web of Science, CINAHL, and Cochrane Library for articles published from January 2007 to March 2022 and updated on 12 October 2022. Data were extracted independently by two researchers, and the risk of bias in individual trials was rated using the Cochrane risk-of-bias tool (RoB 2). Meta-analysis was conducted by using RevMan 5.3.
Results
Ten studies were included involving 1626 participants. The mean ages of the women were 32.42 ±4.68 years. Eight out of 10 studies were conducted in developed countries. Meta-analysis found that smartphone-based lifestyle interventions statistically improved compliance [SMD = 7.36, 95% CI = (4.05 to 10.68), P < 0.0001] and decreased the incidences of neonatal intensive care unit (NICU) admission [RR = 0.64, 95% CI = (0.47,0.86), P = 0.003], compared with controls. However, intervention effects on HbA1c, maternal outcomes, neonatal hypoglycemia, and infant birth weight were non significant. Moreover, the satisfaction of intervention is high in this review. Contrastingly, no significant effects were observed for psychological status and cost-effectiveness.
Conclusion
Smartphone-based lifestyle interventions may improve patient compliance and reduce NICU admissions. These findings may aid in developing future intervention strategies, help elucidate future research directions, and guide clinical practice for women with GDM. Future high-quality RCTs must be further studied at larger scales to examine smartphone-based lifestyle interventions’ long-term effects and cost-effectiveness.
Introductions
GDM refers to any degree of glucose intolerance that occurs or is first detected during pregnancy.Citation1 GDM is one of the most common pregnancy complications, with a global prevalence of 10.6%.Citation2 Women with GDM are seven times more likely to develop Type 2 diabetes mellitus (T2DM) later in life than women with normal glycemia during pregnancy.Citation3 Women with GDM are more likely to have adverse maternal and infant outcomes, including caesarean section, higher need for induced labor and pre-eclampsia, and congenital disabilities in infants.Citation4,Citation5 In addition, children exposed to chronic high blood sugar in utero have a higher risk of obesity, insulin resistance, metabolic syndrome, T2DM, or cardiovascular disease.Citation6 Thus, GDM must be managed effectively.
The current management model for GDM focuses on lifestyle interventions that aim to provide patients with the skills and strategies required to promote and change their behavior. Due to their low cost and potential for scalability with no side effects,Citation7 lifestyle interventions are recommended as a first-line approach to improve physical activity and dietary modification in women with GDM.Citation8 Lifestyle interventions for women with GDM during pregnancy and postpartum can normalize glycemic levels, reducing the incidence of adverse maternal and infant outcomesCitation5,Citation8–10 and improving diabetes-related risk factors (eg, insulin resistance and weight reduction).Citation11 Meanwhile, a meta-analysis of eight studies from seven countries unveiled that lifestyle interventions reduced T2DM incidence by 25% in women with GDM.Citation11 However, traditional lifestyle interventions often require intensive provider support, ongoing follow-ups, and frequent counselling for young mothers.Citation12 As a result, previous studies have reported implementation with a 54.1% recruitment response rate and 65.0% attendance rate,Citation13 well below the benchmark rate of over 80%.Citation14 Researchers reported challenges for women with GDM participating in lifestyle interventions in clinical practice, including guilt about leaving their children, work-life imbalance, time constraints, and the need for more flexible schedules.Citation12 These findings are consistent with reports that the main barriers to attending in-person health promotion programs are family/childcare responsibility and transportation.Citation15 These problems may be alleviated by using technology. As the COVID-19 pandemic spreads, the development of mobile health interventions as alternatives to traditional face-to-face approaches to providing real-time healthcare to patients is becoming increasingly popular.Citation16
Lifestyle interventions delivered through smartphones can be cost effective, innovative, secure, and user friendly.Citation17 The unique features of smartphone app or text message can be used to track and modify the patient’s diet, exercise or health behavior diet, weight, and physical activity.Citation18 The data collection function of smartphones can also be used to develop a tailored intervention.Citation19 Furthermore, smartphones can provide real-time feedback through a graphical display and encourage self-monitoring.Citation20 Smartphone-based interventions can be embedded with behavior change technologies, such as feedback, reminders, information delivery, self-monitoring, and tailoring to adjust an individual’s diet and physical activity.Citation21 A systematic review including 29 studies suggests that smartphone-based lifestyle interventions are feasible and acceptable for health care during pregnancy.Citation22 Many smartphone-based health lifestyle interventions have been applied in chronic disease management and have shown great potential in providing personalized guidance.Citation23,Citation24 Smartphone-based lifestyle interventions are promising in improving the management of maternal obesity and excessive gestational weight gain.Citation17,Citation22,Citation25 Women with GDM are interested in receiving health information on their smartphones and are willing to use them.Citation20,Citation26 These data suggest that smartphones are a promising medium for women with GDM to use in the behavior change.
Recently published systematic review has highlighted lifestyle-based interventions as practical strategies that delay the onset of T2DM among at-risk populations.Citation27 However, due to the scarcity of available studies, knowledge gaps were observed regarding the effect of lifestyle-based interventions on the health-related outcomes for GDM.Citation27 Meanwhile, several previous systematic reviews and meta-analyses have evaluated the effects of technology-based lifestyle interventions in managing diabetes (T1DM, T2DM, and GDM), most of which involve heterogeneous technologies. They examined the effectiveness of smartphone-based interventions combining other types of technology (eg, wearable devices and primarily web-based programs).Citation28–32 Moreover, a systematic review, which included six studies (n = 408), suggested that mHealth-apps may improve health-related outcomes among pregnant women with GDM.Citation33 However, this paper was a narrative synthesis and failed to draw solid conclusions for health-related outcomes due to heterogeneity, a small number of trials, the research design was not limited to RCT. Drawing reliable conclusions about the effectiveness of smartphone-based lifestyle interventions for patients with GDM is difficult. To a large extent, evidence is sparse on the impacts of smartphone-based lifestyle interventions on GDM. Thus, we performed a systematic review and meta-analysis of available evidence from RCT studies to quantify the evidence on smartphone-based lifestyle interventions for health-related outcomes and satisfaction and cost effectiveness for GDM. Therefore, this study aimed to assess the efficacy of smartphone-based lifestyle interventions in improving compliance, HbA1c, maternal outcomes, infant outcomes, and psychological status, as well as investigate the satisfaction and cost effectiveness in women with GDM compared to control groups.
Methods
Eligibility Criteria
Studies that were RCTs published in the English language and met the following criteria were included: 1) Study participants were adults who had GDM history or a confirmed diagnosis of GDM. 2) Smartphone-based lifestyle interventions were defined as interventions achieved through smartphones, for example real-time doctor-patient communication, activity/diet tracking, coaching, goal setting. Telemedicine portals or portals based on electronic medical records used for mobile phones are not eligible (eg, website). 3) Studies that examined at least one of the following outcomes: compliance, HbA1C, maternal outcomes (gestational weight gain, gestational age at delivery, normal vaginal delivery, and cesarean delivery), infant outcomes (infant birth weight (grams), neonatal hypoglycemia, NICU admission), and psychological status (depression and anxiety).
The exclusion criteria are as follows: 1) used qualitative data as an outcome measure, 2) were not written in English, and 3) did not use smartphone-based technology for GDM. A PRISMA checklist is outlined in .
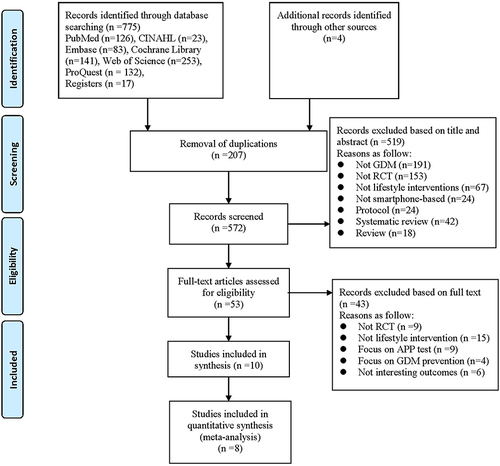
Figure 1 PRISMA flow diagram.
Data Source and Search Strategy
A systematic search of PubMed, Web of Science, Embase, CINAHL and Cochrane Library was carried out. These five databases were chosen because they contain a wealth of valuable biomedical literature that maximizes journal coverage and ensures the inclusion of all relevant research.Citation35,Citation36 ClinicalTrials.gov, Grey Literature (http://www.opengrey.eu), ProQuest Dissertations, and ongoing trials were also searched to find unpublished and ongoing trials. Smartphones with touch screens were popular among the population and rapidly developed from 2007.Citation37 Therefore, only studies published from January 2007 to March 2022 were included. The search was updated on 12 October 2022. Comprehensive search strategies were developed under the supervision of a medical librarian. Appendix 1 shows the detailed search strategies. Additional studies were identified for screening by manually retrieving the list of references and systematic reviews cited in eligible studies. Eligible studies’ citations were searched on the Web of Science to find potential studies and avoid missing eligible studies.
Study Selection and Data Extraction
Searched records were imported into Endnote X9.1 reference manager (Clarivate Analytics, PA, USA), and duplicated references were removed using the software and by hand. Two reviewers (HJW and YYJ) worked independently to screen titles, abstracts, and full texts to decide the eligibility of the studies. Any discrepancies were resolved by a third reviewer (LG). The consensus was achieved in all studies included.
Data were extracted by two reviewers (HJW, YYJ) independently from the 10 trials using a standardized data collection sheet. Any disagreements between two reviewers during the data collection were resolved through further discussion. If necessary, a third reviewer (LG) was invited to arbitrate until an agreement was reached.
Characteristics of each study included general information (authors, year, and country), methods (study design), participants’ characteristics (sample size, mean age, mean BMI, HbA1c at diagnosis, gestation week at recruitment, OGTT-2h, history of previous GDM, attrition rate) (see ), detailed descriptions of interventions (content of intervention, venue, provider, dosage and framework) (see ), outcome measures (compliance, HbA1c, gestational weight gain, gestational age at delivery, normal vaginal delivery, cesarean delivery, infant birth weight, neonatal hypoglycemia, NICU admission, depression, anxiety) (see ).
Table 1 Characteristics of Included Studies
Table 2 Content of Lifestyle Interventions of Included Studies
Table 3 Outcome Measures Available for Meta-Analysis
Risk of Bias Assessment
The Cochrane risk-of-bias tool (RoB 2) was utilized to evaluate the quality of the included
studies by two independent investigators.Citation38 This tool assessed the methodological quality of studies in five domains: (1) random allocation, (2) deviation from intended interventions, (3) management of missing data, (4) outcome measurement, and (5) data analysis. The risk of bias for each domain was categorized into three levels: low, some concerns, high. Any disagreements between the investigators were resolved through discussion or consultation with a senior reviewer (LG). The critical appraisal results are reported in narrative form and a table ().
Table 4 Summary of Quality Assessment of Studies by the Cochrane Risk-of-Bias Tool (RoB 2)
Data Analysis
The RevMan Version 5.3.5 was used to conduct the data analysis (available from the website for free: http://tech.cochrane.org/revman/download). Mean difference (MD)/standardized mean difference (SMD) was calculated for continuous outcomes, and dichotomous variables were presented as risk ratio (RR) with forest plots. I2 test was carried out to assess the heterogeneity, and a value of I2 >50% means high heterogeneity.Citation39 A fixed-effects model was considered to calculate the pooled effect size if the data were not significantly heterogeneous; otherwise, a random-effects model was used. A narrative synthesis was used for quantitative studies that do not extract data to be included in the meta-analysis. A sensitivity analysis was performed by excluding one study at a time to confirm the consistency of the findings. Given that number of reviewed studies is small, subgroup analysis was not conducted. The funnel plot was visually inspected to assess any publication bias.
Results
Search Results
A total of 779 articles were retrieved in the initial search of databases, of which 207 were duplicates. A total of 519 studies were excluded on the basis of the title and abstract. There were no eligible studies in the grey literature databases. A total of 53 studies were included in the full-text screening. Ultimately, 10 studies that met the inclusion criteria were included in this systematic review after the screening process. Eight studies were incorporated in the meta-analysis, whereas two studies that did not extract the required outcome data were not incorporated in the meta-analysis. The selection process is shown in . Two authors were contacted for more precise data points, but no additional information was received.
Risk of Bias
provides the risk of bias summary. Regarding the overall quality of the included studies, six studies had a high risk of bias, and four studies had some concerns about the risk of bias. For the randomization process, four studies reported a low risk of bias for allocation sequence random and allocation sequence concealed; four studies had some concerns, whereas two studies had a high risk of bias. Regarding deviations from intended interventions, most studies (n = 8) reported some concerns. The remaining studies had a high risk of bias for the blind participants and interventionists. In terms of missing outcome data, all studies had a low risk of bias. As for the measurement of the outcome, seven out of 10 studies reported a low-risk bias, whereas three studies had a high risk of bias. Concerning the selection of the reported result, four studies reported a low risk of bias; five studies had some concerns, and one study reported a high risk of bias. Appendix 2 presents the details on the risk of bias (graph).
Studies Characteristics
The included studies involved 1626 women with GDM, and sample sizes in each study ranged from 21 to 340 women. One study (n = 10%) was multi-center design. The mean age of the women was 32.42 ±4.68 years, excluding one study that reported age in a categorical variable.Citation40 Regarding research’s country, most were performed in developed countries: two in Singapore,Citation41,Citation42 one in Australia,Citation43 the UK,Citation44 Norway,Citation40 Korea,Citation45 Spain,Citation46 and Israel.Citation47 The remaining were conducted in developing countries: China (n = 2).Citation48,Citation49 Ten studies were conducted during gestation. With respect to GDM diagnosis criteria, three studies reported that GDM diagnosis was used on the basis of the World Health Organization 2013 criteria,Citation41,Citation42,Citation49 two studies were based on International Association of Diabetes and Pregnancy Study Group criteria,Citation43,Citation44 two studies were based on the American Diabetes Society criteria.Citation47,Citation48 However, the remaining three studies did not report the GDM diagnosis.Citation40,Citation45,Citation46 All of studies were conducted between 2018 and 2022.
Five studies reported a mean BMI of 27.08 ±4.97 kg/m2 at initial study enrollment,Citation41,Citation44,Citation45,Citation47,Citation48 whereas other studies did not extract data or did not report it.Citation40,Citation42,Citation43,Citation46,Citation49 Six studies reported a mean HbA1C of 5.43 ±0.36%.Citation41,Citation42,Citation44,Citation46–48 Six out of 10 studies said the mean gestational week of 27.58 ±2.79 weeks.Citation41–45,Citation48 Five studies reported a mean OGTT-2h of 8.7 ±1.48 mmol/L.Citation41,Citation42,Citation44,Citation48,Citation49 The majority of the included studies (n = 6) reported women we had with a GDM history.Citation40–44,Citation47,Citation48
Characteristics of Interventions
Intervention Group
Women with GDM in the intervention group received smartphone-based lifestyle interventions using a smartphone app (n = 8),Citation40–45,Citation47,Citation48 smart phone social media platform (WeChat) (n = 1),Citation49 or short message service (SMS) (N = 1).Citation46 Three studies reported research teams, including endocrinologists, diabetes nurse educators, and dietitians,Citation42–44 whereas another three studies included obstetricians and endocrinologists,Citation46,Citation47,Citation49 one including outpatient service doctors,Citation48 the remaining studies did not report the details of the research team.Citation40,Citation41,Citation45 The frequency of intervention was every day in eight studies.Citation40–43,Citation46–49 Two studies reported a frequency of twice a weekCitation45 and once a week,Citation44 respectively. Only two studies used intervention components that were based on a theoretical framework.Citation41,Citation42
The contents of interventions in our review can be categorized into four primary types: “health education” (provision of diabetes-related behavior education), “self-management behavior reminders” (reminders to conduct specified behavior activities), “data management” (monitoring and recording self-monitoring of blood glucose (SMBG), weight data obtained, data upload, visualization, trend report, and alerts), and “feedback” (system-generated automated messages, system-generated personalized feedback on the basis of pre-designed algorithms, and personalized feedback sent by health-care professionals on the basis of patient data and performance). All the studies incorporated individualized guidance, supervision, and feedback. Ten studies involved diet, eight involved blood glucose; seven performed health education, six included physical activity, and three monitored insulin treatment.Citation46–48 Only two studies tracked weightCitation41,Citation49 and SMBG.Citation41,Citation48
The attrition of the intervention group ranged from 0% to 7.7%, and the control groups were 0% to 12.7%. The attrition of lifestyle interventions that used a smartphone-based APP in the intervention group ranged from 0% to 7.7%, the control group varied from 0% to 12.1%,Citation40–45,Citation47,Citation48 and the WeChat platform was 0% in intervention and control group,Citation49 whereas SMS was 2% to 4%.Citation46 The reasons for dropout ranged from being too busy, time conflicts, work-related reasons, and spontaneous abortion.
Control Group
Women with GDM in the control group received “usual care”, which generally involved standard outpatient care and/or conventional clinic-based education classes. Six studies reported intervention recorded by paper diary, whereas the other four studies did not report.Citation41,Citation42,Citation45,Citation49
Effects on Compliance and HbA1C
Compliance
Compliance was evaluated in three RCTsCitation41,Citation47,Citation48 with two methods. A statistically significant difference in compliance existed between the two groups [n = 584, SMD = 7.36 95% CI = (4.05 to 10.68), z = 4.35, P < 0.0001, I2 = 99%, random-effects model] (see ). In two studies,Citation47,Citation48 compliance was calculated as the actual blood glucose measurements/instructed measurements×100, and one studyCitation41 was calculated by frequency of SMBG per week. Heterogeneity did not disappear when we removed study one by one. A high heterogeneity was observed, maybe due to the different measurement criteria of compliance.
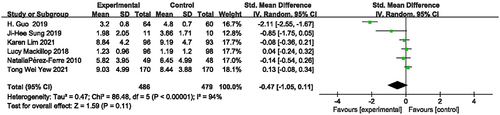
Figure 2 Forest plot of compliance.

HbA1C
HbA1C was assessed in three studies,Citation44,Citation46,Citation48 data available were indicated in two studies.Citation46,Citation48 As one study did not report the means and standard deviations of the HbA1C values.Citation44 Compared to the control group, a non significant difference was observed in two studies after the intervention [n = 221, SMD = −1.30, 95% CI = (−3.36, 0.77), z = 1.23, P = 0.22, I2 = 98%, random-effects model] (see ).
Figure 3 Forest plot of HbA1C.

Effects on Maternal Outcomes
Gestational Weight Gain
Six studiesCitation41,Citation42,Citation44–46,Citation48 reported the effectiveness of intervention on gestational weight gain. Meta-analysis results revealed non significant improvement in gestational weight gain [n = 905, SMD = −0.47, 95% CI = (−1.05, 0.11), z = 1.59, P = 0.11, I2 = 94%; random-effects model], compared to the control group (see ). Heterogeneity was reduced from 94% to 30% when Guo’s study was excluded [SMD = −0.02, 95% CI = (−0.19, 0.16), z = 0.18, P = 0.86] (figure not shown).
Figure 4 Forest plot of gestational weight gain.
Gestation Age at Delivery
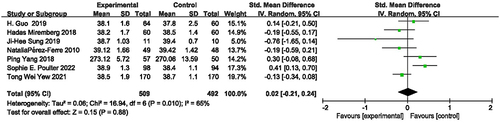
Week of gestation age at delivery was measured in seven RCTs.Citation41,Citation43,Citation45–49 Meta-analysis results indicated no beneficial effect on week of gestation age at delivery [n = 1001, SMD = 0.02, 95% CI = (−0.21, 0.24), z = 0.15, P = 0.88, I2 = 65%, random-effects model] (see ). When the Poulter’s study was removed for the analysis, no statistically significant difference was found between two groups with an acceptable heterogeneity (I2 = 40%, P = 0.14) [SMD = −0.06, 95% CI = (−0.25, 0.14), z = 0.59, P = 0.56] (figure not shown).
Figure 5 Forest plot of gestational age at delivery.
Normal Vaginal Delivery and Cesarean Birth
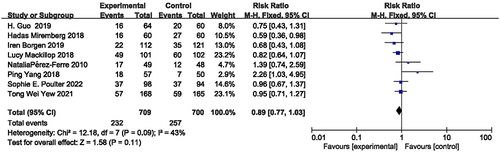
Eight studies reported normal vaginal delivery,Citation40,Citation41,Citation43,Citation44,Citation46–49 when pooling eight studies, no significant difference was revealed in the groups [n = 1409, RR = 1.19, 95% CI = [0.95,1.51], z = 1.51, P = 0.13, I2 = 35%, fixed-effects model] (see ). Similarly, regarding cesarean birth, insignificant differences between two groups were found in risks of cesarean birth as reported in eight studiesCitation40,Citation41,Citation43,Citation44,Citation46–49 [n=1409, RR = 0.89, 95% CI = [0.77,1.03], z = 1.58, P = 0.11, I2 = 43%, fixed-effects model] (see ).
Figure 6 Forest plot of normal vaginal delivery.
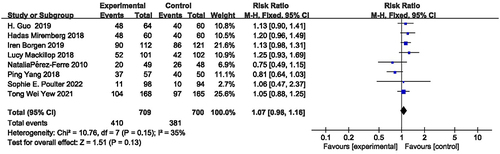
Figure 7 Forest plot of cesarean delivery.
Effects on Infant Outcomes
Infant Birth Weight
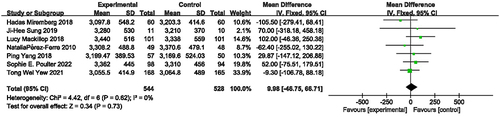
Infant birth weight was assessed in eight RCTs. Among which one study was excluded from the meta-analysis due to insufficient data.Citation40 Seven studies were performed a meta-analysis,Citation41,Citation43–47,Citation49 no statistically significant difference existed in infant birth weight between the intervention group and control group [n = 1072, MD = 9.98, 95% CI = (−46.75 to 66.71), z = 0.34, P = 0.73, I2 = 0%, fixed-effects model] (see ).
Figure 8 Forest plot of Infant birth weight.
Neonatal Hypoglycemia
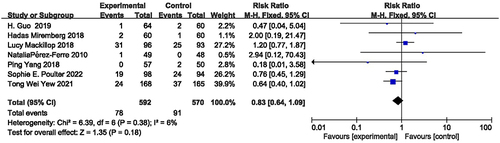
The overall prevalence of neonatal hypoglycemia was evaluated in eight studies. One out of eight studies could not be pooled for meta-analysis as they did not extract neonatal hypoglycemia values.Citation44 Thus, a meta-analysis including seven studies was conducted.Citation41,Citation43,Citation44,Citation46–49 The pooled results did not identify a statistically significant amelioration of neonatal hypoglycemia compared with controls [n = 1162, RR = 0.83, 95% CI = (0.64,1.09), z = 1.35, P = 0.18, I2 = 6%, fixed-effects model] (see ).
Figure 9 Forest plot of neonatal hypoglycemia.
NICU Admission
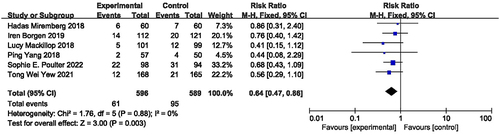
Six studiesCitation40,Citation41,Citation43,Citation44,Citation47,Citation49 reported NICU admission. The results showed that the participants in the intervention group had a significantly reduced risk for NICU admission compared with the control group [n = 1185, RR = 0.64, 95% CI = (0.47,0.86), z = 3.00, P = 0.003, I2 = 0%, fixed-effects model] (see ). Citation40,Citation41,Citation43,Citation44,Citation47,Citation49 summarizes the effect sizes for primary and secondary outcomes from RCTs.
Table 5 Effect Sizes for Primary and Secondary Outcomes from RCTs
Figure 10 Forest plot of NICU admission.
Psychological Status
Regarding psychology outcomes, one out of 10 studies reported psychological determinants of behavior change (depression and anxiety).Citation41 Findings revealed no significant difference between the two groups on depression and anxiety after intervention (P > 0.05).
Satisfaction Evaluation
Two studies evaluated satisfactionCitation43,Citation44 with the structured semiquantitative Oxford Maternity Diabetes Treatment Satisfaction Questionnaire (a 7-point Likert scale). Participants showed overall high satisfactions on smartphone based, due to the special focus on reducing contact and perceived time.
Cost Effectiveness
In terms of cost-effectiveness, two out of 10 studies reported the conflicting results. OneCitation43 indicated a significant reduction in resource use on the total cost during study period after smartphone-based intervention (P = 0.023) compared to the control group. Another studyCitation44 demonstrated no statistically significant cost differences between the two groups over the study period.
Publication Bias and Sensitivity Analyses
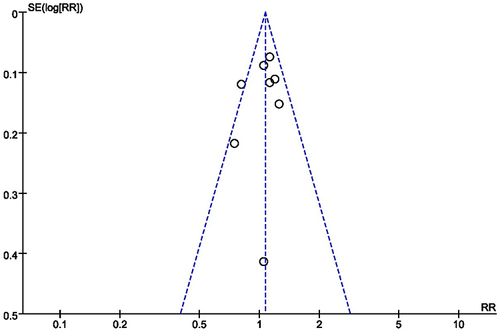
Visual inspection of the funnel plot did not find evidence of potential publication bias (see ). A sensitivity analysis was conducted to examine how the results changed with the removal studies and assessed the stability of the results. When we removed the study from the model and recalculated the combination estimate on the remaining studies, heterogeneity disappeared or decreased, and the pooled results were consistent, which indicated the robustness of our findings.
Figure 11 Funnel plot.
Discussion
This meta-analysis systematically evaluated the effectiveness of smartphone-based lifestyle interventions compared with the standard care on compliance, HbA1C, maternal and infant outcomes, psychological status, satisfaction, and cost effectiveness for women with GDM. This review indicated that smartphone-based lifestyle interventions can contribute to favorable impacts on compliance, and the incidences of NICU admission. Contrastingly, we did not observe significant improvements in HbA1c, neonatal hypoglycemia, infant birth weight, maternal outcomes, psychological status, and cost effectiveness. Moreover, participants’ satisfaction reported in the two studies was high, and higher level of satisfaction is conducive to obtain better outcomes.
Regarding compliance, the current meta-analysis showed that smartphone-based lifestyle interventions can improve compliance significantly (I2 = 99%). The heterogeneity did not disappear by sensitivity analysis when each study was deleted from the model one by one. This heterogeneity might have been due to different devices available to measure compliance from different countries. Guo’s study was conducted in a developing country (China),Citation48 whereas Yew’s studyCitation41 and Miremberg’s studyCitation47 were implemented in Singapore. Additionally, a high heterogeneity may be due to the different measurement criteria of compliance. Moreover, our finding is consistent with the effects of technology-based lifestyle interventions on patients by providing real-time reminders and guidance, which can improve participants’ compliance and increase positive health behaviors.Citation50,Citation51 Interestingly, although the compliance was improved, smartphone-based lifestyle interventions on HbA1C levels were non significant. The intervention effects observed in our analysis should be interpreted with caution due to the small number of studies and the high heterogeneity.
We observed no significant improvements of maternal outcomes. Regarding gestational weight gain, the current study observed no statistically significant difference between the two groups. Several reasons possibly explain the non significant effect of the smartphone-based lifestyle interventions on gestational weight gain. First, those studies that demonstrated that lifestyle interventions reduced gestational weight gain or improved other maternal outcome mainly targeted women with BMI of at least 31.3 kg/m2.Citation44 We included women with GDM with the average BMI at recruitment of roughly 26.53 kg/m2. Second, a recent study revealed that gestation week at baseline was associated with maternal outcomes.Citation52 Mean gestation at recruitment of 25 weeks showed decreased gestational weight gainCitation48 possibly because there was a longer intervention time from recruitment to. In our meta-analysis, the mean gestational week at baseline was 27.4 in included studies. Therefore, it was not surprising that our review did not identify improvements in the gestational weight gain.
Our finding is consistent with the current available evidence (n = 11 trails including 5658 participants, MD = 0.05 weeks, 95% CI: −0.05 to 0.15),Citation53 which has reported that no evidence of a difference in the gestational age at delivery exists between the lifestyle intervention and standard care groups. As for the rate of normal vaginal delivery and cesarean birth, the available literature has reported different results.Citation29,Citation30,Citation33 A recent review (n = 32 trial including 5108 participants)Citation29 reported that telemedicine interventions on women with GDM showed a significant improvement in incidences of caesarean section [relative risk (RR) = 0.82, P = 0.02] compared to the control group. Another review (n = 6 trials including 408 participants)Citation33 reported that mHealth-apps might improve vaginal deliveries showing improving trends. However, a recent meta-analysis in 2020 evaluated technology-supported lifestyle interventions for GDM covering 10 studies, demonstrated that no differences in normal vaginal delivery and cesarean birth were found in the two groups.Citation30
Our meta-analysis showed that smartphone-based lifestyle interventions were associated with lower incidences of NICU admission, which is in line with one systematic review demonstrating that lifestyle interventions were beneficial for NICU admission mainly due to a reduced risk of being born preterm (<37 weeks) (RR = 0.71, 95% CI = 0.53, 0.96) and of shoulder dystocia (RR = 0.38, 95% CI = 0.21, 0.66).Citation54 However, as for the infant birth weight and rate of neonatal hypoglycemia, the current study did not observe statistically significant differences between the two groups. These findings were consistent with two reviews of technology-based interventions that found no significant differences in infant outcomes between the two groups.Citation30,Citation33 The possible reason is that gestational weight gain and gestational age delivery were not improved. Higher quality and more adequately powered studies are warranted to investigate the effects of smartphone-based lifestyle interventions on maternal and fetal outcomes among women with GDM.
In our included studies, the psychological status of GDM receives little attention. One of 10 studies reported depression and anxiety, showing non significant improvements in psychological status. The psychological burden is also common in GDM.Citation55 The prevalence of anxiety was highest (39.9%), followed by depression (12.5%), among women with GDM.Citation56 Prior studies suggested that depression and anxiety can directly affect patients’ behavior and ability to self-management and indirectly affect HbA1c.Citation57 Moreover, the psychological status of pregnant women also has a certain impact on maternal and offspring outcomes.Citation55,Citation58,Citation59 Evidence suggests that strategies to tailor psychological interventions modules based on smartphone help adults with diabetes cope positively and achieve diabetes treatment goals.Citation60 Therefore, psychological intervention elements must be integrated into smartphone-based lifestyle interventions to investigate the effects on psychological status among women with GDM in future studies.
Strength and Limitations
The principal strength of this review is its inclusion of various outcomes that evaluated the effectiveness of smartphone-based lifestyle interventions on compliance, HbA1C, maternal and neonatal outcomes and psychological status, satisfaction, and cost effectiveness. In addition, we did not limit our systematic review to smartphones for developing/developed countries. The search strategy was comprehensive and inclusive, and this review reported outcomes according to PRISMA guidelines. Finally, the attrition of this review included studies in the intervention group was low, approximately 0% to 7.7%, especially in the WeChat group, which was 0%.
However, this study also has some limitations that must be considered while interpreting our findings. First, the lack of standardized intervention time and assessment time points prevented a direct comparison between trials due to the different GDM diagnosis criteria. Meanwhile, the insufficiency of existing data (eg, compliance, HbA1c) in included studies prevented us from drawing a solid conclusion about the effects of smartphone-based lifestyle interventions on women with GDM. Second, the included studies had suboptimal quality, and methodological weakness may decrease the internal validity of the results and increase the heterogeneity, which may have led to a biased estimate of the overall effect. Third, all studies for women with GDM were conducted during gestation; however, the effects of smartphone-based behavior intervention on women with GDM after postpartum remain unknown. Fourth, participants’ psychological outcomes (n = 1), satisfaction (n = 3), and cost effectiveness (n = 2) were reported in limited studies, making data synthesis extremely difficult.
Implications for Practice and Research
Implications for Practice
In clinical practice, smartphone-based lifestyle interventions are routinely under-recognized. This review found that smartphone-based lifestyle interventions affects the compliance and the incidences of NICU admission. Smartphone-based lifestyle interventions are promising for women with GDM during gestation and can be applied in clinical practice. According to the evidence in this systematic review, multidisciplinary collaboration involving dietitians, diabetes educators, obstetricians, and endocrinologists will help women with GDM improve their health outcomes.
Implications for Research
Considering the methodological weakness of some included studies, future RCTs must follow the guidelines of the Consolidated Standards of Reporting Trials statement to enhance the standard of reports.Citation61 In this review, most studies were conducted in developed countries; more research is warranted in developing and low-income countries. Most of the trials in the included studies were conducted during gestation, more research is required before pregnancy or postpartum or all-round. The effects of smartphone-based lifestyle intervention on HbA1c, maternal-fetal, and infant outcomes, as well as psychological status, are warranted in multi-center designs guided by a framework to investigate effects and possible intervention mechanisms. Thus far, APP/smart phone-based interventions have not performed well, and participants are unsure how to use the technology effectively. It would be preferable to involve participants more in the content development for smartphone-based interventions. Future researchers must try new strategies for using technology to promote healthy lifestyles. More rigorous cost-effective analyses of smartphone-based interventions are warranted to demonstrate the impact on public health. Future meta-analyses with a larger sample of RCT studies can perform subgroup analysis on the basis of the type of country, gestation or postpartum, and App, WeChat, or SMS.
Conclusion
The current systematic review fills the research gap regarding the effectiveness of smartphone-based lifestyle interventions among women with GDM. It provides further evidence to help elucidate future research directions and guide clinical practice. Smartphone-based lifestyle interventions as a practical strategy improve compliance and the incidences of NICU admission among women with GDM. However, the effectiveness appears to be non significant with respect to HbA1c, maternal outcomes, infant birth weight, and neonatal hypoglycemia. Future studies at larger scales are warranted to examine the long-term effects and cost effectiveness of smartphone-based lifestyle interventions.
Disclosure
The authors report no conflicts of interest in this work.
References
- Metzger BE, Coustan DR. Summary and recommendations of the fourth international workshop-conference on gestational diabetes mellitus. The organizing committee. Diabetes Care. 1998;21(Suppl 2):B161–B167.
- Behboudi-Gandevani S, Amiri M, Bidhendi Yarandi R, Ramezani Tehrani F. The impact of diagnostic criteria for gestational diabetes on its prevalence: a systematic review and meta-analysis. Diabetol Metab Syndr. 2019;11(1):11. doi:10.1186/s13098-019-0406-1
- Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet. 2009;373(9677):1773–1779. doi:10.1016/S0140-6736(09)60731-5
- Chiefari E, Arcidiacono B, Foti D, Brunetti A. Gestational diabetes mellitus: an updated overview. J Endocrinol Invest. 2017;40(9):899–909. doi:10.1007/s40618-016-0607-5
- Blumberg J, Ballares V, Durbin JL. Ethnic variations on gestational diabetes mellitus and evidence-based first-line interventions. J Matern Fetal Neonatal Med. 2018;31(19):2641–2647. doi:10.1080/14767058.2017.1344967
- Leybovitz-Haleluya N, Wainstock T, Landau D, Sheiner E. Maternal gestational diabetes mellitus and the risk of subsequent pediatric cardiovascular diseases of the offspring: a population-based cohort study with up to 18 years of follow up. Acta Diabetol. 2018;55(10):1037–1042. doi:10.1007/s00592-018-1176-1
- Albright AL, Gregg EW. Preventing type 2 diabetes in communities across the U.S.: the national diabetes prevention program. Am J Prev Med. 2013;44(4 Suppl 4):S346–S351. doi:10.1016/j.amepre.2012.12.009
- Brown J, Alwan NA, West J, et al. Lifestyle interventions for the treatment of women with gestational diabetes. Cochrane Database Syst Rev. 2017;5(5):CD011970. doi:10.1002/14651858.CD011970.pub2
- Brown J, Ceysens G, Boulvain M. Exercise for pregnant women with gestational diabetes for improving maternal and fetal outcomes. Cochrane Database Syst Rev. 2017;6(6):CD012202. doi:10.1002/14651858.CD012202.pub2
- Dhingra A, Ahuja K. Lifestyle modifications for GDM. J Pak Med Assoc. 2016;66(9 Suppl 1):S34–S38.
- Goveia P, Cañon-Montañez W, Santos DP, et al. Lifestyle intervention for the prevention of diabetes in women with previous gestational diabetes mellitus: a systematic review and meta-analysis. Front Endocrinol. 2018;9:583. doi:10.3389/fendo.2018.00583
- Jones EJ, Fraley HE, Mazzawi J. Appreciating recent motherhood and culture: a systematic review of multimodal postpartum lifestyle interventions to reduce diabetes risk in women with prior gestational diabetes. Matern Child Health J. 2017;21(1):45–57. doi:10.1007/s10995-016-2092-z
- Guo J, Tang Y, Wiley J, Whittemore R, Chen JL. Effectiveness of a diabetes prevention program for rural women with prior gestational diabetes mellitus: study protocol of a multi-site randomized clinical trial. BMC Public Health. 2018;18(1):809. doi:10.1186/s12889-018-5725-x
- Treweek S, Pitkethly M, Cook J, et al. Strategies to improve recruitment to randomised trials. Cochrane Database Syst Rev. 2018;2(2):Mr000013. doi:10.1002/14651858.MR000013.pub6
- Aziz Z, Mathews E, Absetz P, et al. A group-based lifestyle intervention for diabetes prevention in low- and middle-income country: implementation evaluation of the Kerala diabetes prevention program. Implement Sci. 2018;13(1):97. doi:10.1186/s13012-018-0791-0
- Lim SL, Ong KW, Johal J, et al. A smartphone app-based lifestyle change program for prediabetes (D’LITE study) in a multiethnic Asian population: a randomized controlled trial. Front Nutr. 2021;8:780567. doi:10.3389/fnut.2021.780567
- Farzandipour M, Nabovati E, Anvari S, Vahedpoor Z, Sharif R. Phone-based interventions to control gestational weight gain: a systematic review on features and effects. Inform Health Soc Care. 2020;45(1):15–30. doi:10.1080/17538157.2018.1540421
- World Health Organization. mHealth New horizons for health through mobile technologies. WHO Press; 2011. Available from: http://www.who.int/goe/publications/goe_mhealth_web.pdf. Accessed August 3, 2022.
- Jo A, Coronel BD, Coakes CE, Mainous AG 3rd. Is there a benefit to patients using wearable devices such as fitbit or health apps on mobiles? A systematic review. Am J Med. 2019;132(12):1394–1400.e1391. doi:10.1016/j.amjmed.2019.06.018
- Chen Q, Carbone ET. Functionality, implementation, impact, and the role of health literacy in mobile phone apps for gestational diabetes: scoping review. JMIR Diabetes. 2017;2(2):e25. doi:10.2196/diabetes.8045
- Direito A, Dale LP, Shields E, Dobson R, Whittaker R, Maddison R. Do physical activity and dietary smartphone applications incorporate evidence-based behaviour change techniques? BMC Public Health. 2014;14(1):646. doi:10.1186/1471-2458-14-646
- Overdijkink SB, Velu AV, Rosman AN, van Beukering MD, Kok M, Steegers-Theunissen RP. The usability and effectiveness of mobile health technology-based lifestyle and medical intervention apps supporting health care during pregnancy: systematic review. JMIR Mhealth Uhealth. 2018;6(4):e109. doi:10.2196/mhealth.8834
- Sieverdes JC, Treiber F, Jenkins C, Hermayer K. Improving diabetes management with mobile health technology. Am J Med Sci. 2013;345(4):289–295. doi:10.1097/MAJ.0b013e3182896cee
- Scott-Sheldon LA, Lantini R, Jennings EG, et al. Text messaging-based interventions for smoking cessation: a systematic review and meta-analysis. JMIR Mhealth Uhealth. 2016;4(2):e49. doi:10.2196/mhealth.5436
- Hussain T, Smith P, Yee LM. Mobile phone-based behavioral interventions in pregnancy to promote maternal and fetal health in high-income countries: systematic review. JMIR Mhealth Uhealth. 2020;8(5):e15111. doi:10.2196/15111
- Adesina N, Dogan H, Green S, Tsofliou F. Effectiveness and usability of digital tools to support dietary self-management of gestational diabetes mellitus: a systematic review. Nutrients. 2021;14(1):10. doi:10.3390/nu14010010
- Sagastume D, Siero I, Mertens E, Cottam J, Colizzi C, Peñalvo JL. The effectiveness of lifestyle interventions on type 2 diabetes and gestational diabetes incidence and cardiometabolic outcomes: a systematic review and meta-analysis of evidence from low- and middle-income countries. EClinicalMedicine. 2022;53:101650. doi:10.1016/j.eclinm.2022.101650
- Halligan J, Whelan ME, Roberts N, Farmer AJ. Reducing weight and BMI following gestational diabetes: a systematic review and meta-analysis of digital and telemedicine interventions. BMJ Open Diabetes Res Care. 2021;9(1):1. doi:10.1136/bmjdrc-2020-002077
- Xie W, Dai P, Qin Y, Wu M, Yang B, Yu X. Effectiveness of telemedicine for pregnant women with gestational diabetes mellitus: an updated meta-analysis of 32 randomized controlled trials with trial sequential analysis. BMC Pregnancy Childbirth. 2020;20(1):198. doi:10.1186/s12884-020-02892-1
- Li SY, Ouyang YQ, Qiao J, Shen Q. Technology-supported lifestyle interventions to improve maternal-fetal outcomes in women with gestational diabetes mellitus: a meta-analysis. Midwifery. 2020;85:102689. doi:10.1016/j.midw.2020.102689
- Leblalta B, Kebaili H, Sim R, Lee SWH. Digital health interventions for gestational diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. PLoS Digital Health. 2022;1(2):1–23. doi:10.1371/journal.pdig.0000015
- Wu Y, Yao X, Vespasiani G, et al. Mobile app-based interventions to support diabetes self-management: a systematic review of randomized controlled trials to identify functions associated with glycemic efficacy. JMIR Mhealth Uhealth. 2017;5(3):e35. doi:10.2196/mhealth.6522
- Eberle C, Loehnert M, Stichling S. Effectiveness of specific mobile health applications (mHealth-apps) in gestational diabetes mellitus: a systematic review. BMC Pregnancy Childbirth. 2021;21(1):808. doi:10.1186/s12884-021-04274-7
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339(jul21 1):b2700–b2700. doi:10.1136/bmj.b2700
- Bahaadinbeigy K, Yogesan K, Wootton R. MEDLINE versus EMBASE and CINAHL for telemedicine searches. Telemed J E Health. 2010;16(8):916–919. doi:10.1089/tmj.2010.0046
- Chapman D. Health-related databases. J Can Acad Child Adolesc Psychiatry. 2009;18(2):148–149.
- Cecere G, Corrocher N, Battaglia RD. Innovation and competition in the smartphone industry: is there a dominant design? Telecomm Policy. 2015;39(3–4):162–175. doi:10.1016/j.telpol.2014.07.002
- Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
- Higgins J, Thompson SG, Decks JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
- Borgen I, Småstuen MC, Jacobsen AF, et al. Effect of the pregnant+ smartphone application in women with gestational diabetes mellitus: a randomised controlled trial in Norway. BMJ Open. 2019;9(11):e030884. doi:10.1136/bmjopen-2019-030884
- Yew TW, Chi C, Chan SY, et al. A randomized controlled trial to evaluate the effects of a smartphone application-based lifestyle coaching program on gestational weight gain, glycemic control, and maternal and neonatal outcomes in women with gestational diabetes mellitus: the SMART-GDM study. Diabetes Care. 2021;44(2):456–463. doi:10.2337/dc20-1216
- Lim K, Chan SY, Lim SL, et al. A Smartphone App to Restore Optimal Weight (SPAROW) in women with recent gestational diabetes mellitus: randomized controlled trial. JMIR Mhealth Uhealth. 2021;9(3):e22147. doi:10.2196/22147
- Poulter SE, Meloncelli N, Mack M. Use of a smartphone-based, interactive blood glucose management system in women with gestational diabetes mellitus: a pilot study. Diabetes Res Clin Pract. 2022;185:109224. doi:10.1016/j.diabres.2022.109224
- Mackillop L, Hirst JE, Bartlett KJ, et al. Comparing the efficacy of a mobile phone-based blood glucose management system with standard clinic care in women with gestational diabetes: randomized controlled trial. JMIR Mhealth Uhealth. 2018;6(3):e71. doi:10.2196/mhealth.9512
- Sung JH, Lee DY, Min KP, Park CY. Peripartum management of gestational diabetes using a digital health care service: a pilot, randomized controlled study. Clin Ther. 2019;41(11):2426–2434. doi:10.1016/j.clinthera.2019.09.005
- Pérez-Ferre N, Galindo M, Fernández MD, et al. The outcomes of gestational diabetes mellitus after a telecare approach are not inferior to traditional outpatient clinic visits. Int J Endocrinol. 2010;2010:386941. doi:10.1155/2010/386941
- Miremberg H, Ben-Ari T, Betzer T, et al. The impact of a daily smartphone-based feedback system among women with gestational diabetes on compliance, glycemic control, satisfaction, and pregnancy outcome: a randomized controlled trial. Am J Obstet Gynecol. 2018;218(4):453e451–453 e457.
- Guo H, Zhang Y, Li P, Zhou P, Chen LM, Li SY. Evaluating the effects of mobile health intervention on weight management, glycemic control and pregnancy outcomes in patients with gestational diabetes mellitus. J Endocrinol Invest. 2019;42(6):709–714. doi:10.1007/s40618-018-0975-0
- Yang P, Lo W, He ZL, Xiao XM. Medical nutrition treatment of women with gestational diabetes mellitus by a telemedicine system based on smartphones. J Obstet Gynaecol Res. 2018;44(7):1228–1234. doi:10.1111/jog.13669
- Macharia WM, Leon G, Rowe BH, Stephenson BJ, Haynes RB. An overview of interventions to improve compliance with appointment keeping for medical services. JAMA. 1992;267(13):1813–1817. doi:10.1001/jama.1992.03480130129038
- van Dulmen S, Sluijs E, van Dijk L, de Ridder D, Heerdink R, Bensing J. Patient adherence to medical treatment: a review of reviews. BMC Health Serv Res. 2007;7(1):55. doi:10.1186/1472-6963-7-55
- Voerman E, Santos S, Inskip H, et al. Association of gestational weight gain with adverse maternal and infant outcomes. JAMA. 2019;321(17):1702–1715. doi:10.1001/jama.2019.3820
- Shepherd E, Gomersall JC, Tieu J, Han S, Crowther CA, Middleton P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst Rev. 2017;11(11):CD010443. doi:10.1002/14651858.CD010443.pub3
- Mitanchez D, Ciangura C, Jacqueminet S. How can maternal lifestyle interventions modify the effects of gestational diabetes in the neonate and the offspring? A systematic review of meta-analyses. Nutrients. 2020;12(2):353. doi:10.3390/nu12020353
- Packer CH, Pilliod RA, Chatroux LR, Caughey AB, Valent AM. Increased rates of adverse perinatal outcomes in women with gestational diabetes and depression. J Matern Fetal Neonatal Med. 2021;34(23):3862–3866. doi:10.1080/14767058.2019.1701647
- Lee KW, Ching SM, Hoo FK, et al. Prevalence and factors associated with depressive, anxiety and stress symptoms among women with gestational diabetes mellitus in tertiary care centres in Malaysia: a cross-sectional study. BMC Pregnancy Childbirth. 2019;19(1):367. doi:10.1186/s12884-019-2519-9
- Lin K, Park C, Li M, et al. Effects of depression, diabetes distress, diabetes self-efficacy, and diabetes self-management on glycemic control among Chinese population with type 2 diabetes mellitus. Diabetes Res Clin Pract. 2017;131:179–186. doi:10.1016/j.diabres.2017.03.013
- Schmitt A, Reimer A, Hermanns N, et al. Depression is linked to hyperglycaemia via suboptimal diabetes self-management: a cross-sectional mediation analysis. J Psychosom Res. 2017;94:17–23. doi:10.1016/j.jpsychores.2016.12.015
- Nazu NA, Wikström K, Lamidi ML, et al. Association of mental disorders and quality of diabetes care - a six-year follow-up study of type 2 diabetes patients in North Karelia, Finland. Diabetes Res Clin Pract. 2020;166:108312. doi:10.1016/j.diabres.2020.108312
- He Q, Zhao X, Wang Y, Xie Q, Cheng L. Effectiveness of smartphone application-based self-management interventions in patients with type 2 diabetes: a systematic review and meta-analysis of randomized controlled trials. J Adv Nurs. 2022;78(2):348–362. doi:10.1111/jan.14993
- Moher D, Schulz KF, Altman DG. The CONSORT statement: revised recommendations for improving the quality of reports of parallel-group randomised trials. Lancet. 2001;357(9263):1191–1194. doi:10.1016/S0140-6736(00)04337-3