
Abstract
Purpose
Sex differences in depression have been well recognized. However, sex differences in depression among Omicron-infected individuals have received little systematic study. This study compared sex differences in depression in infected individuals during the 2022 Omicron pandemic in China.
Patients and Methods
506 individuals infected with Omicron (males/females = 268/238) were recruited from Tianjin and Shanghai in China. Self-developed Scale of Demographics were used to collect demographic and clinical data, Zung Self-Rating Depression Scale (SDS), Zung Self-Rating Anxiety Scale (SAS), the Connor-Davidson Resilience Scale (CD-RISC), De Jong Gierveld Scale (DJGLS), and the Penn State Worry Questionnaire (PSWQ) were used to measure respondents’ depression, anxiety, resilience, loneliness and worry, respectively.
Results
The prevalence rate of depression in male patients was significantly higher than in female patients (42.2% versus 31.9%; χ2 = 5.64, p = 0.018). Regression analysis showed that in female patients, depression was associated with anxiety [OR = 1.26, 95% CI (1.16–1.36), p < 0.001], and resilience [OR = 0.98, 95% CI (0.96–1.00), p < 0.05], while in male patients, depression was associated with anxiety [OR = 1.24, 95% CI (1.15–1.33), p < 0.001].
Conclusion
This on-site study demonstrates that depression is more frequent in male than female Omicron-infected patients and suggests that sex differences should be considered in prevention and treatment strategies for depression during the Omicron pandemic.
Introduction
Background and Information Regarding the COVID-19 Pandemic
The coronavirus disease 2019 (COVID-19) is an infectious disease caused by the severe acute respiratory syndrome coronavirus, which has caused many infections and a rapidly increasing number of cases, posing a huge challenge to the global public health, research, and medical communities, and leading to serious and unanticipated biological, psychological, social, spiritual, and economic related issues.Citation1–3 As of May 1, 2023, more than 600 million cases of COVID-19 infection have been reported globally, with more than 6 million deaths. (COVID‐19 Map. Johns Hopkins Coronavirus Resource Center. https://coronavirus.jhu.edu/map.html.) It is well known that the damage and impact of the COVID-19 epidemic on our country and other countries in terms of social, healthcare, and mental health problems are enormous.Citation4–7
Impact of the COVID-19 Pandemic on Mental Health
In the three years since the outbreak, this panic and inconvenience caused by the novel coronavirus has been affecting people’s daily lives and mental health.Citation8,Citation9 People’s psychological problems are increasing and attracting the attention of many researchers.Citation10–12 Many studies have shown that people experience some psychological problems during the COVID-19 epidemic, such as depression, anxiety, insomnia, etc. A systematic review demonstrated that the rates of depression in the general population reached 14.6% to 48.3% across the globe during the COVID-19 pandemic.Citation13 The results of another meta-analysis showed that 45% of COVID-19 patients develop depression,Citation14 which is the evidence of a high prevalence of depression during the COVID-19 epidemic.
Depression is a major global health problem that will be the leading cause of the disease burden by 2030.Citation15 Research has shown that there are sex differences in depression, with most studies reporting twice the incidence of depression in female than in male.Citation16,Citation17 And some studies show that male are more likely to suffer from depression than female.Citation18
Gaps in the Literature
Many studies have now reported on the prevalence of depression during the COVID-19 epidemic, few studies have reported gender differences on the prevalence of depression. One study showed no sex difference were found,Citation19 and another study found depression is more frequent in female.Citation20 These studies were conducted in the non-infected population. Many studies have shown that anxiety, resilience, loneliness, and worry are associated with depression.Citation21–25 A person’s level of anxiety, resilience, loneliness, and worry may be risk or protective factors for depression.
Purpose and Significance of the Study
As seen above, sex differences in depression have been extensively studied in the general population. The purpose of our study was to investigate sex differences in depression among Omicron-infected individuals during the COVID-19 epidemic and whether there were sex differences in depression-related factors. Therefore, the current study aimed to investigate the sex differences in (1) demographic factors and clinical characteristics; (2) their associated factors of depression among male and female infected patients with Omicron in China.
Materials and Methods
Sampling
From 28th January to 28th March in 2022, 306 infected candidates from two Tianjin designated hospitals were interviewed, 6 refused to participate in the research, 33 incorrectly completed the assessment, 18 met the excluding criteria, and 249 were included in the analysis. From 26th April to 11th May 2022, 271 infected candidates from one of Shanghai makeshift hospitals were interviewed, 10 incorrectly completed the assessment, 4 met the exclusion criteria, and 257 were included in the analysis. In total, five hundred and six individuals infected with Omicron (males/females = 268/238) were recruited from Tianjin and Shanghai designated hospitals. All participants provided their written informed consent by a handwritten or electronic signature for participating in this study. This survey was anonymous and voluntary.
Eligibility Criteria
The inclusion criteria were as followings: (1) age must be older than 18; (2) no history of severe brain injury, significant brain disease, or major cognitive impairment; (3) no history of severe somatic illnesses; (4) no history of mental illness. If not, she/he would be excluded from the study.
Conduct of the Assessment
This is on-site self-rating study related to COVID-19. The interviewers included psychiatrists, psychiatric nurses, and students pursuing a master’s or doctoral degree in psychiatry or psychology. Five interviewers were involved in the on-site investigations using hard-copy and e-copy questionnaires in Tianjin designated hospital; 10 interviewers were involved in the on-site investigations using e-copy questionnaires in Shanghai makeshift hospitals.
After the interviewers introduce the study, the candidates should complete informed consent by a handwritten or electronic signature if she or he agrees to participate in the study. Each responder needs complete the scales by herself or himself. If she or he has questions, the interviewer provides a standardized answer but not an excessive explanation.
Demographic Characteristics Scale
A self-developed questionnaire was used to collect demographic data, including sex, age, educational level, marital status, living status, work status, ethnicity, economic level, etc. Besides, other questions included “Do you have any physical illnesses”, “Have you ever had any psychiatric/psychological problems”, and “COVID-19-infected status [1 = non-infection; 2 = asymptomatic; 3 = mild; 4 = common; 5 = severe; 6 = critical]”, etc.
Zung Self-Rating Depression Scale
The depression and severity was assessed using the Zung Self-rating Depression Scale (SDS).Citation26 This scale includes 20 items, the response options were: 1 = “none or a little of the time”, 2 = “small of the time”, 3 = “a good part of the time”, 4 = “most or all of the time”. The total score of SDS was computed by the sum of 20 items, with higher total scores indicating greater propensity of depression. The raw total scores were multiplied by 1.25 to yield the standard scores. In our study, the standard scores ≥ 53 as cutoff for diagnosing depression. The scale had good reliability and validity, which has been demonstrated in its prior Chinese version.Citation27 In the current study, the Cronbach’s alpha coefficient of the SDS was 0.83.
Zung Self-Rating Anxiety Scale
The Zung Self-rating Anxiety Scale (SAS)Citation28 was used to measure the severity of anxiety symptoms. It includes 20 items, the response options were: 1 = “none or a little of the time”, 2 = “small of the time”, 3 = “a good part of the time”, 4 = “most or all of the time”. The total score of SAS was computed by the sum of 20 items, with higher total scores indicating greater propensity of anxiety. The scale had good reliability and validity, which has been demonstrated in its prior Chinese version.Citation29 In the current study, the Cronbach’s alpha coefficient of the SAS was 0.83.
Connor-Davidson Resilience Scale
Psychological resilience was assessed using the Connor-Davidson Resilience Scale (CD-RISC).Citation30 The scale includes 25 items, the response options were: 0 = “not at all”, 1 = “rarely”, 2 = “sometimes”, 3 = “often”, 4 = “always”. The total score of CD-RISC was computed by the sum of 25 items, with higher total scores representing greater resilience. Previous Chinese editionCitation31 demonstrated good reliability and validity. In this study, the Cronbach’s alpha coefficient of the CD-RISC was 0.96.
De Jong Gierveld Scale
The De Jong Gierveld Scale (DJGLS)Citation32 was used to measure a person’s loneliness. It includes 11 items, the response options were: 0 = “never”, 1 = “seldom”, 2 = “sometimes”, 3 = “often”, 4 = “always”. On the 5 negatively worded items (items 1, 4, 7, 8, 11), the answers of “sometimes”, “often”, and “always” are scored as “1”; On the remaining 6 positively worded items, the answers of “never” and “seldom” are scored as “1”. The total score of DJGLS was computed by the sum of 11 items, with higher total scores representing greater propensity of loneliness. Previous Chinese editionCitation33 demonstrated good reliability and validity, and in this study, the Cronbach’s alpha coefficient of the DJGLS was 0.78.
Penn State Worry Questionnaire
Penn State Worry Questionnaire (PSWQ) was used to measure a person’s worry.Citation34 This scale includes 16 items, the response options were: 1 = “not at all typical of me”, 2 = “not really typical of me”, 3 = “a little of typical of me”, 4 = “really typical of me”, 5 = “very really typical of me”. The total score of PSWQ was computed by the sum of 16 items, with higher total scores representing greater propensity of worry. Previous Chinese editionCitation35 demonstrated good reliability and validity, and in the present study, Cronbach’s alpha coefficient for scores on this scale was 0.86.
Data Analysis
The data were prepared using double entry verification in EpiData 3.1. SPSS version 25.0 (SPSS Inc., Chicago, IL, USA) was used for data analysis. The Chi-square test was used for the categorical variables in the univariate analysis between male and female patients. In contrast, Wilcoxon’s test was used for the continuous variables after the Kolmogorov–Smirnov test. To compare the sex differences of clinical variables between Omicron-infected patients with or without depression, a nonparametric two-factor ANOVA (Scheirer-Ray-Hare test) was used to analyze clinical variables as dependent variables, taking sex (male vs female) and category (depression vs non-depression) as independent variables, with age, educational level, marital status, living status, working status, ethnicity, and economic level as covariates.
In addition, the differences in clinical variables between depression and non-depression subgroups were compared by Kruskal–Wallis H in male or female patients, respectively. Finally, the logistic regression analysis was used to identify the important variables associated with depression in each sex group after controlling all the demographic variables. Both the Step-forward method and Step-backward were tried. The odd ratio (OR) and 95% confidence interval (CI) were calculated. The statistical significance was set at p < 0.05 for all tests.
Results
Sex Difference in Prevalence of Depression in Omicron-Infected Individuals
The prevalence rate of depression in Omicron-infected individuals was 37.4%. Male patients (42.2%, 113/268) had higher prevalence rate of depression than female patients (31.9%, 76/238; χ2 = 5.64, p = 0.018), with the odds ratio (OR) of 1.55 [95% confidence interval (CI) 1.08–2.24].
Sex Differences in Demographic and Clinical Characteristics in Omicron-Infected Individuals
As shown in , SDS total scores for the male patients was significantly higher than that of the female patients. There were significantly differences in age, educational level, work status, economic level (all p < 0.01), marital status (p < 0.05), and the overall scores of DJGLS scale (p < 0.05) between male and female patients. Compared with female Omicron-infected patients, male patients were younger and poor, had lower educational level, had higher rates of unmarried, had other work status, and had higher probability of loneliness.
Table 1 Characteristics of Male and Female Infected Individuals with Omicron During Omicron Pandemic in China
Sex Differences in Demographic and Clinical Features in Omicron-Infected Individuals with and without Depression
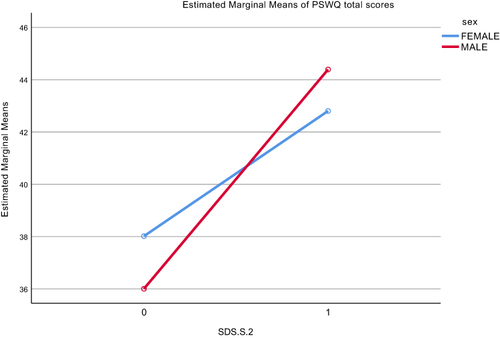
As shown in and , there was significant interaction between depression category and sex in PSWQ total scores (H = 3.96, p = 0.032). Then, we analyzed the demographic and clinical variables in male and female Omicron-infected individuals separately. In female patients, individuals with depression were significantly unemployed (χ2= 3.96, p = 0.047), rich (χ2 = 9.45, p = 0.009) and had higher probability of anxiety (Z = -8.48, p = 0.000), loneliness (Z = -1.98, p = 0.047), worry (Z = -2.82, p = 0.005), and had worse resilience (Z = -4.82, p = 0.000) than those without depression. In male patients, individuals with depression were significantly older (Z = -2.15, p = 0.031), poor (χ2 = 8.38, p = 0.015) and had lower educational level (χ2 = 18.05, p = 0.000), had higher probability of anxiety (Z = -10.34, p = 0.000), loneliness (Z = -3.97, p = 0.000), worry (Z = -6.50, p = 0.000), and had worse resilience (Z = -5.84, p = 0.000) than those without depression ().
Table 2 Demographic and Clinical Characteristics of Omicron-Infected Patients with and without Depression Grouped by Sex
Figure 1 Interactions between depression and sex on PSWQ total scores.
Factors Associated with Depression
In female patients, binary logistic regression analysis indicated compared to the respondents without depression, those with depression were more likely to be with higher overall scores of SAS [OR = 1.26, 95% CI (1.16–1.36), p < 0.001], and to be with lower overall scores of CD-RISC [OR = 0.98, 95% CI (0.96–1.00), p < 0.05]. In male patients, binary logistic regression analysis revealed that compared to the respondents without depression, those with depression more likely to be with higher overall scores of SAS [OR = 1.24, 95% CI (1.15–1.33), p < 0.001] ().
Table 3 Binary Logistic Analysis for Factors Associated with Depression in Female and Male Omicron-Infected Individuals
Discussion
There are three main findings in our study. First, male Omicron-infected individuals displayed a significantly higher rate of depression than female patients. Second, anxiety, resilience, loneliness, and worry were associated with depression in both female and male patients. Third, in female patients, depression was associated with anxiety and resilience, while in male patients, depression was associated with anxiety.
Sex Differences in Depression Rate
We found that depression was more prevalent in male than female infected patients with Omicron (42.2% vs 31.9%). Some epidemiological studies have found that sex differences in depression have been observed in the general populations.Citation16,Citation36,Citation37 However, till now, no studies find sex differences in the incidence of depression on Omicron-infected patients during COVID-19 pandemic. Relevant studies found sex differences in depression on general populations.Citation19,Citation20 Our findings on Omicron-infected patients showed that the incidence of depression in men was higher than that in women.
One possible explanation for the higher prevalence of depression in male Omicron-infected patients is that their infection rate and mortality rate were high and their infectious symptoms were more serious.Citation38–40 In this study, we found that the male patients were more than female patients, which may lead to a higher prevalence of depression in male than in female Omicron-infected patients during the COVID-19 pandemic.
Depression was Associated with Anxiety, Loneliness, Worry, and Resilience in Both Male and Female Omicron-Infected Patients
As most studies have reported that depression is associated with anxiety, loneliness, worry, and resilience,Citation21–24 we also observed the correlation between anxiety, loneliness, worry, resilience, and depression in Omicron-infected patients. However, this study was cross-sectional, and it could not determine the causal relationship between these associated factors and depression. Therefore, whether these associated factors will predict a greater depression in Omicron-infected patients during the COVID-19 will be worth exploring in future.
Sex Differences in Clinical Correlates of Depression
We observed that there were interactions between depression and sex. Our findings demonstrated that an interaction between depression and sex in terms of the PSWQ total scores. That is to say, depression may differentially affect the total scores of PSWQ in male and female Omicron-infected patients. However, no relevant studies have reported the potential mechanism of sex differences in the association between worry and depression in Omicron-infected patients, which is worthy of further exploration in future research.
We further found that there were sex differences in some associated factors of depression in infected patients with Omicron. In male patients, depression was associated with age and anxiety levels. However, in female patients, depression was associated with unemployed work status, high SAS total scores and low resilience CD-RISC total scores.
Symptoms of anxiety and depression are known to be highly correlated.Citation41 People who are often in a state of anxiety are also more likely to get depression. A systematic review found anxiety and depression to have a bidirectional relationship, especially over shorter periods, and reported that anxiety symptoms and disorders predicted depression;Citation42,Citation43 and, the worse resilience a woman is, the more likely she is to experience depression. Relevant study showed that negative association of resilience with depression. Participants with a higher level of depression had a worse resilience. Resilience reduces the impact of stressful life events on the formation of depression and resilience levels are significantly lower in people with depression.Citation44
Limitations
There are several limitations in the current study. First, depression was assessed by a self-rating scale rather than diagnoses. It means the results should be limited to the general population and could not be generalized to those with emotional disorders. Second, the sample was taken from only two cities (Tianjin and Shanghai), which may not represent Omicron-epidemic areas in China. Third, two cross-sectional surveys were independent and only reflected the psychological status of the subjects at that time, so the temporal changes and trajectories of the respondents’ mental health could not be observed longitudinal follow-up was lacking. Even with the above shortcoming, we explored the sex differences in depression among Chinese Omicron-infected patients during the COVID-19 pandemic, as well as associated factors in differences between factors associated with depression by gender.
Conclusion
This study found that sex differences existed in demographic, mental health, and psychological traits in Chinese Omicron-infected patients. Male Omicron-infected patients had a higher prevalence of depression as compared with female patients. And, there are differences in the clinical correlates of depression by sex, in female patients, depression was associated with anxiety and resilience, while in male patients, depression was associated with anxiety, suggesting that sex differences should be considered in prevention and treatment strategies for depression during Omicron pandemic.
Ethics Statement
This study was conducted in accordance with the Declaration of Helsinki. The study was approved by the Ethics Committee of Tianjin Anding Hospital, reference numbers: 2021-045 and 2021-046. All the participants provided their informed consent to participate in this study.
Implication
Given that this study is focused on the mental health of Omicron-infected individuals during the COVID-19 pandemic and elaborated on the significance of sex differences, we propose practical implications in the following three main areas: research, mental health, and services. In terms of the research area, our study fills an important and meaningful gap; in terms of the mental health area, COVID-19 pandemics have a very negative impact on the mental health of the general public, and the incidence of common mental illnesses has risen dramatically as a result of pandemics. This study reminds readers and other researchers to pay more attention to their own and others’ mental health and to seek formal help if they are unable to adjust it on their own; in terms of the services area, local governments, and mental health providers can provide effective services targeted to help people in need.
Disclosure
The authors declare that they have no conflicts of interest in this work.
Acknowledgments
The authors thank the staff members in the Yangliuqing Township Community Center in Xiqing County, Tianjin First Center Hospital, Tianjin Haihe Hospital, and Tianjin Anding Hospital for their assistance in the study.
Additional information
Funding
References
- Bao Y, Sun Y, Meng S, et al. 2019-nCoV epidemic: address mental health care to empower society. Lancet. 2020;395(10224):e37–e38.
- Tanhan A. Utilizing online photovoice (OPV) methodology to address biopsychosocialspiritual economic issues and wellbeing during COVID-19: Adapting OPV to Turkish. TurkishStudies. 2020;15(4):1029–1086. doi:10.7827/TurkishStudies.44451
- Doyumğaç İ, Tanhan A, Kiymaz MS. Understanding the most important facilitators and barriers for online education during COVID-19 through online photovoice methodology. IJHE. 2021;10(1):166. doi:10.5430/ijhe.v10n1p166
- Lippi G, Henry BM, Sanchis-Gomar F. Putative impact of the COVID-19 pandemic on anxiety, depression, insomnia and stress. Eur J Psychiatry. 2021;35(3):200–201. doi:10.1016/j.ejpsy.2020.11.006
- Mion G, Hamann P, Saleten M, et al. Psychological impact of the COVID-19 pandemic and burnout severity in French residents: a national study. Eur J Psychiatry. 2021;35(3):173–180. doi:10.1016/j.ejpsy.2021.03.005
- Sifat RI, Ahmed F, Miah MRA, et al. Effects of COVID-19 on livelihood, health, and psychology of Hijra Population: insights from Dhaka, Bangladesh. J Homosex. 2023;70(10):2096–2112. doi:10.1080/00918369.2022.2048162
- Sifat RI. COVID-19 and mental health challenges among the Hijra people in Bangladesh. Int J Soc Psychiatry. 2021;67(8):1072–1073. doi:10.1177/0020764020978684
- Haleem A, Javaid M, Vaishya R. Effects of COVID-19 pandemic in daily life. Curr Med Res Pract. 2020;10(2):78–79. doi:10.1016/j.cmrp.2020.03.011
- Barber RM, Sorensen RJ, Pigott DM, et al. Estimating global, regional, and national daily and cumulative infections with SARS-CoV-2 through Nov 14, 2021: a statistical analysis. Lancet. 2022;399(10344):2351–2380.
- Kuriyama A, Shikino K, Moriya M, et al. Burnout, depression, anxiety, and insomnia of internists and primary care physicians during the COVID-19 pandemic in Japan: a cross-sectional survey. Asian J Psychiatr. 2022;68:102956. doi:10.1016/j.ajp.2021.102956
- Nishimura Y, Miyoshi T, Hagiya H, et al. Prevalence of psychological distress on public health officials amid COVID-19 pandemic. Asian J Psychiatr. 2022;73:103160. doi:10.1016/j.ajp.2022.103160
- Zheng D, Liu P, Chen H, et al. Worse psychological traits associated with higher probability of emotional problems during the Omicron pandemic in Tianjin, China. Eur J Psychiatry. 2023;37(2):84–91. doi:10.1016/j.ejpsy.2022.09.002
- Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
- Deng J, Zhou F, Hou W, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. 2021;1486(1):90–111. doi:10.1111/nyas.14506
- Lépine JP, Briley M. The increasing burden of depression. Neuropsychiatr Dis Treat. 2011;7(Suppl 1):3–7. doi:10.2147/NDT.S19617
- Salk RH, Hyde JS, Abramson LY. Gender differences in depression in representative national samples: meta-analyses of diagnoses and symptoms. Psychol Bull. 2017;143(8):783–822. doi:10.1037/bul0000102
- Angst J, Gamma A, Gastpar M, et al. Gender differences in depression. Epidemiological findings from the European DEPRES I and II studies. Eur Arch Psychiatry Clin Neurosci. 2002;252(5):201–209. doi:10.1007/s00406-002-0381-6
- Faravelli C, Alessandra Scarpato M, Castellini G, et al. Gender differences in depression and anxiety: the role of age. Psychiatry Res. 2013;210(3):1301–1303. doi:10.1016/j.psychres.2013.09.027
- Olaseni AO, Akinsola OS, Agberotimi SF, et al. Psychological distress experiences of Nigerians during Covid-19 pandemic; the gender difference. Soc Sci Humanit Open. 2020;2(1):100052. doi:10.1016/j.ssaho.2020.100052
- Ulloa RE, Apiquian R, de la Peña FR, et al. Age and sex differences in the impact of the COVID-19 pandemic on mental health and coping mechanisms in Latin American youth. J Psychiatr Res. 2022;156:372–378. doi:10.1016/j.jpsychires.2022.10.005
- Amsalem D, Dixon LB, Neria Y. The Coronavirus Disease 2019 (COVID-19) outbreak and mental health: current risks and recommended actions. JAMA Psychiatry. 2021;78(1):9–10. doi:10.1001/jamapsychiatry.2020.1730
- Hwang T-J, Rabheru K, Peisah C, et al. Loneliness and social isolation during the COVID-19 pandemic. Int Psychogeriatr. 2020;32(10):1217–1220. doi:10.1017/S1041610220000988
- Golberstein E, Wen H, Miller BF. Coronavirus Disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatr. 2020;174(9):819–820. doi:10.1001/jamapediatrics.2020.1456
- Choi KW, Kim YK, Jeon HJ. Comorbid anxiety and depression: clinical and conceptual consideration and transdiagnostic treatment. Adv Exp Med Biol. 2020;1191:219–235.
- Benke C, Autenrieth LK, Asselmann E, et al. One year after the COVID-19 outbreak in Germany: long-term changes in depression, anxiety, loneliness, distress and life satisfaction. Eur Arch Psychiatry Clin Neurosci. 2022;2022;1–11.
- Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
- Zhang DX, Luo JH, Peng LZ, et al. Factor analysis on survey results of the Self Rating Depression Scale (SDS)in students. J Kunming Med Univ. 2012;5(33):61–63.
- Zung WW. A rating instrument for anxiety disorders. Psychosomatics. 1971;12(6):371–379. doi:10.1016/S0033-3182(71)71479-0
- Yu X, Cao S, Li J, et al. Applicability research of self-rating anxiety scale and self-rating depression scale in termination of pregnancy caused by fetal abnormality. J Nurs Rehabil. 2016;15(8):723.
- Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
- Yu X, Zhang J, Yu XN, et al. Factor analysis and psychometric evaluation of the Connor-Davidson resilience scale (CD-RISC) with Chinese people. Soc Behav Pers. 2007;35(1):19–30. doi:10.2224/sbp.2007.35.1.19
- de Jong-Gierveld J, Kamphuls F. The development of a rasch-type loneliness scale. Appl Psychol Meas. 1985;9(3):289–299. doi:10.1177/014662168500900307
- Leung GT, de Jong Gierveld J, Lam LC. Validation of the Chinese translation of the 6-item De Jong Gierveld Loneliness Scale in elderly Chinese. Int Psychogeriatr. 2008;20(6):1262–1272. doi:10.1017/S1041610208007552
- Meyer TJ, Miller ML, Metzger RL, et al. Development and validation of the Penn State Worry Questionnaire. Behav Res Ther. 1990;28(6):487–495. doi:10.1016/0005-7967(90)90135-6
- Zhong J, Wang C, Li J, et al. Penn State Worry Questionnaire: structure and psychometric properties of the Chinese version. J Zhejiang Univ Sci B. 2009;10(3):211–218. doi:10.1631/jzus.B0820189
- Holden C. Sex and the suffering brain. Science. 2005;308(5728):1574. doi:10.1126/science.308.5728.1574
- Kessler RC, Berglund P, Demler O, et al. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095–3105. doi:10.1001/jama.289.23.3095
- Wang L, Berger NA, Kaelber DC, et al. COVID infection rates, clinical outcomes, and racial/ethnic and gender disparities before and after Omicron emerged in the US. medRxiv. 2022. doi:10.1101/2022.02.21.22271300
- Gebhard C, Regitz-Zagrosek V, Neuhauser HK, et al. Impact of sex and gender on COVID-19 outcomes in Europe. Biol Sex Differ. 2020;11(1):29. doi:10.1186/s13293-020-00304-9
- Pérez-López FR, Tajada M, Savirón-Cornudella R, et al. Coronavirus disease 2019 and gender-related mortality in European countries: a meta-analysis. Maturitas. 2020;141:59–62. doi:10.1016/j.maturitas.2020.06.017
- Jacobson NS, Martell CR, Dimidjian S. Behavioral activation treatment for depression: returning to contextual roots. Clin Psychol. 2001;8(3):255–270.
- Jacobson NC, Newman MG. Anxiety and depression as bidirectional risk factors for one another: a meta-analysis of longitudinal studies. Psychol Bull. 2017;143(11):1155–1200. doi:10.1037/bul0000111
- Abas MA, Weiss HA, Simms V, et al. The effect of co-morbid anxiety on remission from depression for people participating in a randomised controlled trial of the Friendship Bench intervention in Zimbabwe. EClinicalMedicine. 2020;23:100333. doi:10.1016/j.eclinm.2020.100333
- Lim ML, Lim D, Gwee X, Nyunt MS, Kumar R, Ng TP. Resilience, stressful life events, and depressive symptomatology among older Chinese adults. Aging Ment Health. 2015;19(11):1005–1014.