
Abstract
Purpose
The drug classification system, as prescription or non-prescription drug category, has been utilized as a regulatory strategy to ensure patient safety. In Thailand, the same system has been used for decades, though the drug classification criteria were updated to accommodate drug re-classification in 2016. These new criteria, however, have not been applied retroactively. Inconsistency in drug classification has been observed leading to concerns regarding the drug classification system. This has prompted the need for a review of the drug classification system in Thailand. This study aims to explore Thailand and other selected countries’ regulatory management regarding the drug classification system, drug classification criteria, and drug classification itself.
Methods
The drug classification systems of the United States, the United Kingdom, Japan, Singapore, Malaysia, the Philippines, and Canada were selected to study alongside Thailand’s system. The regulatory review was conducted through each country’s drug regulatory agency website and available published research. Complementary interviews with drug regulatory authorities were conducted when written documentation was unclear and had limited access. Fifty-two common drugs were selected to compare their actual classifications across the different countries.
Results
All selected countries classified drugs into two major groups: prescription drugs and non-prescription drugs. The studied countries further sub-classified non-prescription drugs into 1–4 categories. Principles of drug classification criteria among countries are similar; they comprised of three themes: disease characteristics, drug safety profile, and other drug characteristics. Actual drug classification of antibiotics, dyslipidemia treatments, and hypertension treatments in Thailand are notedly different from other countries. Furthermore, 77.4% of drugs studied in Thailand fall into the behind-the-counter (dangerous) drug category, which varied from antihistamines to antibiotics, dyslipidemia treatments, and vaccines.
Conclusion
Thailand’s drug classification criteria are comparable with other nations; however, there is a need to review drug classification statuses as many drugs have been classified into improper drug categories.
Introduction
Regulators around the world impose different restrictions on drug availability, such as prescription status, to protect the health. Different drug categories, such as prescription and over-the-counter drugs, lead to different drug access, channel of drug distribution, and permitted advertisement.Citation1
Drugs are classified into different categories based on their characteristics. Major factors that affect drug classification are the self-diagnosis nature of diseases and safety profile of drugs. Drugs for catastrophic diseases and drugs for minor ailments are usually classified into different categories, which are prescription drugs and non-prescription drugs, respectively.Citation1 Drug status can be re-classified downward or upward depending mainly on the safety information being obtained from market experiences.Citation1,Citation2 For example, in the UK, diclofenac was re-classified upward from non-prescription to prescription status because an increased risk of cardiovascular diseases was found.Citation3 Conversely, to increase drug accessibility, in the US, loratadine was re-classified from prescription to non-prescription status when its safety information was confirmed after placing it on the market for nine years.Citation4 There is a precedent, then, that drug regulatory agencies make the final decision when assessing benefits and risks to re-classify drugs into appropriate categories in order to ensure patient safety while maximizing timely access to drugs.
Thailand has been internationally recognized for its successful health development and universal health coverage policy.Citation5 Currently, all Thai citizens are covered under one of the three public health insurance schemes: the National Health Security Office (NHSO), the Social Security Office (SSO) and the Civil Services Medical Benefits Scheme (CSMBS).Citation6 Thailand has approximately 13,405 public hospitals, 384 private hospitals, 13,510 clinics, 17,069 type 1 modern community pharmacies, and 2865 type 2 drugstores.Citation7,Citation8 Type 1 modern community pharmacies can distribute all types of drugs ranging from traditional to western medicines and from household remedies to specially controlled substances (equal to the prescription status). They require a pharmacist on duty during their operating hours; while type 2 drugstores sell limited non-prescription drug items and drug dispensers are certified non-pharmacists.Citation9 Since 2005, the Ministry of Public Health has no longer authorized new type 2 drugstore licensing; therefore, the number of type 2 drugstores have been predicted to decline. This was due to concerns regarding illegally dispensing of dangerous drugs, such as antibiotics or antihypertensive drugs, from the certified non-pharmacists.Citation10
The Thai Food and Drug Administration (Thai FDA) has classified drugs into four legal categories: specially controlled drugs, dangerous drugs, non-dangerous drugs and household remedies.Citation11 Regulatory details of each drug category are shown in .
Table 1 Current Legal Drug Categories and Their Regulatory Details in ThailandCitation11,Citation12
As of 2017, Thailand has more than 37,500 drugs registered with the Thai FDA.Citation13 Drugs in three categories, specially controlled drugs, dangerous drugs, and household remedies, must be formally designated by the Thai FDA. Drugs that are not included in the three mentioned categories are automatically classified as non-dangerous drugs. This drug classification system has been used in Thailand for more than five decades.Citation12,Citation14 Nonetheless; a study conducted in Thailand by Sriwiryanupab and her colleagues has proposed, along with various pharmacist groups in Thailand, that the non-dangerous drug category should be discontinued.Citation15,Citation16 In other words, the drug classification system in Thailand should be reformed. This is because non-dangerous drug category was initiated to support existence of type 2 drugstores where certified non-pharmacists can dispense non-dangerous drugs. As type 1 community pharmacies are now sufficient, type 2 drugstores and non-dangerous drug category can be deserted.
Several drugs in Thailand are classified differently when compared to other countries. Many of them are very easy to access, which evidently result in irrational drug use. Examples of the consequences of classic irrational drug use are antibiotic resistance from antibiotics overuse, addiction from tramadol overuse, misuse of hydrochlorothiazide for weight loss, and dextromethorphan and brown mixture (opium preparation) abuse when mixed with beverages or other illicit drugs for recreational purposes.Citation17–Citation20 At the same time, some other drugs in Thailand are more difficult to access than in other countries. In Thailand, cetirizine and ibuprofen are classified as dangerous drugs which need to be kept behind the counter and dispensed by pharmacists. However, these two drugs are classified as general sale list drugs in the US and the UK, and can be sold by non-pharmacy retailers.Citation4,Citation21,Citation22
The Thai Drug Act (No. 6) A.D. 2019 was announced in April 2019 as an addendum to the Thai Drug Act A.D. 1967. The main foci of the addendum were to change the renewal process for drug product licensing (from no re-licensing required to renewal every 7 years), to ensure timeline of the marketing authorization process, and to set up an official list of registered external experts or organizations.Citation12,Citation23 However, the revision of the drug classification system regarding the number of drug categories, classification criteria, and actual drug classification is an issue not yet resolved. Thus, a comprehensive review of the drug classification system is required to support the revision.
There have been few research studies published comparing drug classification systems worldwide.Citation15,Citation24–Citation26 Of these, just one includes Thailand, but this research still does not focus on a comprehensive review of drug classification systems among the countries in the study.Citation15 As prescription and non-prescription drug classification systems can be used as regulatory frameworks to ensure the rational use of drugs, this study aims to explore Thailand and other selected countries’ regulatory management regarding their respective drug classification systems, the different criteria of drug classification, and how drug regulatory agencies actually classify drugs into different categories. Findings from this study could be used to support the revision of the drug classification system in Thailand.
Methods
In this study, the focus was on eight countries: the US, the UK, Japan, Canada, Singapore, the Philippines, Malaysia, and Thailand. The first four were chosen as they are rated as having stringent drug regulatory agencies as defined by the World Health Organization (WHO). The remaining three countries are the regional neighbors of Thailand, all being members of Association of South East Asian Nations (ASEAN), and therefore were chosen for their comparability.Citation27–Citation29
A targeted review was used as a primary method to gather information regarding the drug classification system specific to each country, the drug classification criteria specific to each drug classification system, and comparative actual drug classification across selected countries. All data searching in this study was conducted up to February 2020.
Data searching was first run through each country’s official drug regulatory agency website. Then, complementary data search for further information was conducted through Google scholar with a combination of various search terms: “drug classification”, “drug reclassification”, “Rx-to-OTC”, “drug schedule”, “prescription”, “non-prescription”, “criteria” and each selected country name. The use of manual searching was also employed to ensure complete inclusion of necessary data sources. Grey literature, such as government reports and conference handouts presented by drug regulatory agencies, were also included. Drug regulatory agencies’ interviews would be performed when published information was ambiguous or when information was provided in local language.
In order to better understand the drug classification system and criteria of the selected countries, 52 common drugs used for treatment of both chronic and acute diseases were chosen along with various dosage forms to see how categorization affected drug classification. These drugs had been taken from 11 therapeutic groups: dyslipidemia, diabetes, hypertension, bacterial infection, fungal infection, pain, allergy, nausea and vomiting associated with chemotherapy, insomnia, smoking cessation, and vaccines. A targeted review was conducted through government websites and other credible sources, which are shown in .
Table 2 Sources of Actual Drug Classification Comparisons Across Different Drug Regulatory Agencies
Content analysis was performed to identify drug classification category and key criteria used to categorize drugs into different classes. We also investigated healthcare system, rate of education, and socioeconomic status of each country as these factors might affect drug classification system management. provides countries’ background regarding the healthcare system, country education levels and socioeconomic statuses. The healthcare context itself was separated into three different categories: physician density, pharmacist density, and pharmacists’ autonomy to respond to patients’ symptoms and vaccinate. Education attainment levels of each country were gaged using the learning-adjusted years of schooling (LAYS), a measurement combining both quantity and quality of schooling.Citation30 The socioeconomic status of each country was measured by the human development index (HDI).Citation31,Citation32
Table 3 Different System Contexts of the Eight Studied Countries
Results
The results themselves are comprised of three parts: the drug classification system specific to each country, the drug classification criteria specific to each drug classification system, and comparative drug classification across selected countries.
Drug Classification System
Our research found that, among the eight countries, drugs are universally classified into two major categories: prescription drugs and non-prescription drugs. Prescription drugs are consistently regulated across the eight studied countries. To access prescription drugs, physicians must diagnose a disease before providing prescriptions to patients. However, some regulations vary across countries. Within our sample, though excluding the US and Canada, prescription drugs cannot be directly advertised to consumers.Citation48–Citation56 Moreover, prescription drugs are mainly distributed through community pharmacies and hospitals. Online pharmacies are permitted to sell prescription drugs in the US, the UK, Singapore, the Philippines, and Canada, but not yet in Japan, Malaysia and Thailand.Citation12,Citation43,Citation45,Citation57–Citation67
On the other hand, non-prescription drugs are diversely regulated across countries. The numbers of these sub-categories ranged from one in the US to four in Japan (). Although the regulations of the non-prescription drug category varied, they could be grouped into the following four sub-categories ().
Figure 1 Drug classification categories among countries.
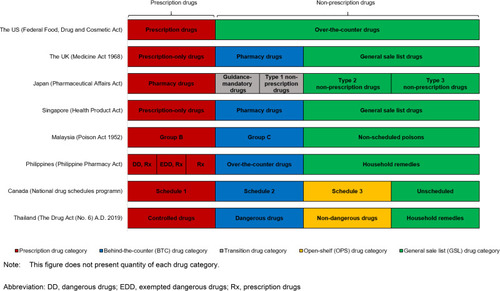
Table 4 Differences in Drug Regulation Among Each Drug CategoryCitation12,Citation43,Citation45,Citation48–Citation67
Behind-the-Counter (BTC) Drug Category
BTC drugs do not require prescriptions but do require dispensing under pharmacists’ supervision, and, as a result, these drugs are kept behind the pharmacy counters. Pharmacists must ask for patients’ symptoms before dispensing any drugs. Detailed instructions are also required to ensure that patients understand how to use the drug safely. Six countries have implemented BTC as an official drug category, though the official name of the category differs in each: pharmacy drugs (the UK and Singapore), group C (Malaysia), over-the-counter drugs (the Philippines), schedule 2 (Canada), and dangerous drugs (Thailand).Citation12,Citation43,Citation45,Citation58,Citation60,Citation61,Citation63–Citation67 These drugs are permitted to be sold via online pharmacies in most countries, except Malaysia and Thailand. Direct-to-consumer advertisements of BTC drugs are permitted only in the UK, Singapore and Canada; but not allowed in Malaysia, the Philippines and Thailand.Citation48–Citation56
Open-Shelf (OPS) Drug Category
OPS drugs have been deemed safe for consumers to practice self-medication; although drugs are still confined to distribution only in healthcare settings, and not in non-pharmacy retailers. This implies that patients could seek pharmacist advice if needed. Only Canada and Thailand have implemented the OPS drug category, which is called schedule 3 and non-dangerous drugs, respectively. In Thailand, OPS drugs can be sold in type 2 drugstores that are operated by certified non-pharmacists. OPS drugs are permitted to be sold via online pharmacies in Canada, but not in Thailand. Direct-to-consumer advertisements are permitted in both countries.Citation12,Citation50,Citation51,Citation61,Citation65
General Sale List (GSL) Drug Category
GSL drugs have been declared safe for self-medication. All studied countries have this drug category and they can be sold in non-pharmacy retailers and over the internet.Citation12,Citation43,Citation45,Citation57–Citation67 Direct-to-consumer advertisements of GSL drugs are also permitted in all sample countries.Citation48–Citation56 The GSL drug category has a different nomenclature across the eight countries: over-the-counter drugs (the US), general sale list drugs (the UK and Singapore), type 2 non-prescription drugs and type 3 non-prescription drugs (Japan), non-scheduled poisons (Malaysia), household remedies (the Philippines and Thailand) and unscheduled drugs (Canada).
Transitional Drug Category
We also found a transitional drug category in Japan. When drugs are re-classified from prescription to GSL drugs, they are then relegated to the guidance-mandatory drug category in order to examine the safety of the drug and to monitor consumer self-medication behavior. Drugs in the guidance-mandatory category required face-to-face pharmacist dispensing. It takes at least three years to monitor drugs under the guidance-mandatory label. Once evidence of drug safety is established and confirmed, guidance-mandatory drugs are then re-classified as type 1 non-prescription drugs and remain in this status for at least one year for safety monitoring purposes. Since the distribution of type 1 non-prescription drugs is more relaxed than guidance-mandatory drugs, they can be sold via internet, although pharmacists’ supervision is still required. Pharmacists must assess the necessity of drug use and instruct patients to appropriately use any dispensed drugs. Methods of contact other than face-to-face interaction, such as by email or telephone, can be used to ensure proper drug use. Having established the safety of a type 1 non-prescription drug, these can then be reclassified into type 2 and type 3 non-prescription drugs for self-medication without pharmacist supervision.Citation24,Citation59
Dissimilarities Between the Sample Countries’ Categorization
The similarities within the drug categories of the eight sample countries have been summarized above. Some unique dissention points are reviewed below.
The US is the only country with a two-drug classification system: prescription drugs and over-the-counter drugs (GSL drug category).Citation68 There is no BTC drug category in the US, although some OTC drugs under the GSL drug category, such as pseudoephedrine, need to be strictly kept behind the pharmacist’s counter and dispensed only by pharmacists.Citation69 This management process mimics the BTC drug category.Citation2
In Japan, it is not only the transitional drug category which is implemented to ensure safety when downward re-classification occurs. A strict self-medication handling mechanism is present wherein type 2 and 3 non-prescription drugs can be sold by non-pharmacy retailers, yet still require specially certified personnel to dispense them.Citation24,Citation59
In Canada, Health Canada and the National Association of Pharmacy Regulatory Authorities are responsible for drug classification in Canadian provinces and territories, and implement four drug categories nationwide. However, how drugs are placed into these centralized categories are not always uniform. The provinces of British Columbia, Newfoundland and Labrador, and Quebec all have their own drug regulatory agencies, wherein a drug which is classified under the BTC drug category in the province of British Columbia may be categorized as OPS drugs in Quebec. Inconsistency of drug classification has therefore been noted between provinces and territories in Canada.Citation70
In Malaysia, drugs are regulated under the “Poison Act” along with other poisonous substances, while in other countries, drugs are regulated under the drug act. The Poison Act has classified substances into four categories; group A, group B, group C, and group D. Group A poisons are highly toxic substances that are not allowed to be sold under any circumstances, while group D poisons are chemical substances used in a laboratory. Only group B (prescription drug category) and group C (BTC drug category) are considered drugs for medical consumption. Non-scheduled drugs exempted from the Poison Act 1952 are considered as “non-scheduled poisons” or GSL drugs.Citation43
In the Philippines, drugs which require prescriptions can be divided into three categories. The first category, called “dangerous drugs”, is made up of narcotic and psychotropic drugs listed in the Comprehensive Dangerous Drugs Act of 2000 and requires a special prescription form (yellow Rx) to supply. The second category, called “exempted dangerous drugs”, contains controlled substances that are exempt from dangerous drug category if they meet certain criteria. The third category is prescription-only medicines, which are general drugs that require prescriptions to be dispensed.Citation45,Citation71
This study found that drug re-classification across all sample countries can be divided into two types: re-classification by active pharmaceutical ingredient (API), which was found in Canada, Thailand, Malaysia, and the Philippines, and re-classification by specific product brand, which was found in the US, the UK, Japan, and Singapore. There are pros and cons to either system. The re-classification by API across all product brands is easier for management. Brand-specific re-classification, in contrast, tends to accommodate market exclusivity.Citation72 Under the market exclusivity period, a solicited company needs to undertake post-marketing surveillance to support re-classification and is also granted an exclusive period to make back their investment during the re-classification process. The exclusivity period can range from 1 year in the UK and Singapore to 3 years in the US and Japan.Citation72–Citation77
Drug Classification Criteria
The drug classification criteria from the eight sample countries were obtained mostly from drug regulatory agency websites. Half of the studied countries (the US, Japan, Malaysia, and the Philippines) published only the principles of their respective drug classification criteria in small detail, while the other half (the UK, Singapore, Canada, and Thailand) published detailed drug classification criteria. summarizes the degree of information which can be found for each country’s drug classification criteria. The table indicates “Yes” only when the criteria were explicitly mentioned, while blank cells mark a lack of explicitly published classification criteria.
Table 5 Drug Classification Criteria Among the Eight CountriesCitation11,Citation22,Citation58,Citation78–Citation87
This study found that the drug classification criteria are comprised of three themes: i) disease characteristics, ii) drug safety profiles, and iii) other drug characteristics.
The common criteria of drug classification explicitly mentioned across the eight countries were i) “Requires disease diagnosis from healthcare professional”, ii) “The drug requires evaluation or management by a healthcare professional”, and iii) “The drug resulted in potentially negative consequences, especially habit-forming drugs”. Among these three criteria, “Requires a disease diagnosis from a healthcare professional” is usually the first discriminating criteria to filter prescription from non-prescription drugs. If a layperson cannot accurately identify their illness, drugs indicated for that illness cannot be classified as non-prescription drugs. However, if a layperson can identify their illness, but indicated drugs require evaluation or management by a healthcare professional, then those drugs must be classified as prescription drugs. If a layperson can identify their illness and the corresponding drugs do not require a health professional’s evaluation or management, but those drugs could have potentially negative consequences, then those drugs must be considered as prescription drugs.
Other common criteria explicitly mentioned in at least half of the studied countries were “requires subsequent disease monitoring” (the US, the UK, Singapore, the Philippines, and Canada), “misuse” (the US, the UK, Japan, Canada, and Thailand), and “injection dosage form” (the UK, Singapore, Canada, and Thailand). The UK and Singapore classified injections as prescription status, while Canada and Thailand classified injections as either prescription or BTC drugs.
Other less commonly explicit criteria worth mentioning are “micro-organism resistant” (Canada), “masking serious diseases’ symptoms” (the UK, Singapore, Canada), “need special storage and handling” (Singapore), and “pack size” (the UK, Thailand). It should be noted that, though micro-organism resistance is a known global issue, as of this writing only one country lists it as an explicit criteria for drug classification.Citation11,Citation22,Citation58,Citation78–Citation87
Actual Drug Classification
Fifty-two common drugs for 11 indications were selected to compare their actual drug classification across different drug regulatory agencies. The actual drug classification is presented in . They were obtained from official drug regulatory sources between August 2019 and February 2020.
Table 6 Actual Drug Classification of Selected Drugs Across Different Drug Regulatory Agencies (Updated in February 2020)
Homogeneous drug classification was observed in some drug groups across eight countries. It was found that all countries classify drugs indicated for insomnia (alprazolam, lorazepam, and diazepam), and drugs indicated for nausea and vomiting associated with chemotherapy (ondansetron and granisetron) as prescription drugs. In addition, more than 75% of our sample countries consistently classify drugs for dyslipidemia, hypertension, diabetes, bacterial infection, and various vaccines as prescription drugs. The classification status of all these drugs as prescription drugs is consistent with drug classification criteria discussed above as they either i) require a disease diagnosis from a healthcare professional, ii) require subsequent disease monitoring from a healthcare professional, iii) can lead to habit formation, iv) contribute to micro-organism resistance, or v) have an injection dosage form.
A diverse drug classification status was found among some drug groups: topical antifungal, non-steroidal anti-inflammatory drugs, antihistamines, and drugs used for smoking cessation. Examples of drugs that had a wide range of drug classifications are clotrimazole and ketoconazole cream (prescription, BTC, OPS and GSL drug categories), ibuprofen tablets/capsules (prescription, BTC and GSL), loratadine tablets and cetirizine syrup (prescription, BTC, OPS and GSL), and nicotine patches (prescription, BTC, OPS and GSL).
It was worth noting that among the eight countries, Thailand classified most studied drugs (77.4%) as BTC drugs. Drugs classified into the prescription drug category in other countries, such as dyslipidemia, hypertension, diabetes, and antibiotics, are classified BTC in Thailand. Conversely, well-established and commonly used drugs like cetirizine tablets, loratadine tablets, and nicotine replacement therapy were classified GSL among countries with higher-incomes and higher rates of education (the US, the UK, Japan, Singapore, and Canada), while these drugs were classified as BTC drugs among middle-income and lesser-educated countries (Malaysia, the Philippines, and Thailand).
Discussion
This is the first comprehensive study exploring and comparing drug classification systems, drug classification criteria, and how drugs are actually classified across selected countries. The study confirmed that drug classification systems vary across countries, although classification principles are rather consistent. The design of each drug classification system is likely dependent on health professionals’ responsibility as the evidence suggests that pharmacists’ responsibility impacts the specific stipulations of the drug classification system. Countries which have the BTC drug category allow pharmacists to respond to patient’s symptoms themselves, while countries that do not allow pharmacists to respond to patient’s symptoms independently do not have this drug category.
Drug classification criteria are associated with the drug classification system, health professionals’ responsibility, and drug characteristics. Actual drug classification in each country is influenced by multiple factors, such as the drug classification system, different drug classification criteria, individual drug characteristics, the public need, and the public education level. Cetirizine, loratadine, and ibuprofen are examples of drugs that have well-established records of safe use for self-treatment, while nicotine replacement therapies have been found not suitable for self-treatment due to their complicated nature of use (for example, patients need to know the nicotine gums’ special chewing technique). Nevertheless, there are many examples of lowering the gatekeeper barrier between the patient and these products to encourage smoking cessation. However, drug regulatory agencies in each country need to evaluate the risk/benefit analysis of these types of therapies within the context of their own country to ensure citizen safety when given access to self-medicate. Thus, it was found that these drugs are less stringently regulated among higher educated countries but are more stringently regulated among lower educated countries.
Drug statuses are not static and can be changed over time. Drug re-classification may result from a drug’s safety profile, a health-consciousness trend, or a shift in the professional paradigm. In Thailand, nicotine replacement therapies have been switched from dangerous drugs (BTC drugs) to non-dangerous drugs (OPS drugs) to facilitate access for those who intend to stop smoking.Citation88 Likewise in Canada, many vaccines that are prescription products in countries, such as the UK are classified as schedule 2 (BTC drug category), which are under pharmacists’ control. This is congruent with the pharmacists’ country-specific role, as certified Canadian community pharmacists are responsible for providing routine immunization to their patients without prescriptions.
As for Thailand, the same four-drug classification system has been implemented for more than five decades. This drug classification system is considered appropriate for Thailand’s earlier healthcare system context, wherein type 2 pharmacies were designed to play a prominent role.Citation12 In the past, Thailand experienced healthcare professional shortages and inadequate type 1 modern community pharmacies. Moreover, public health insurance was limited only to government officers, their dependents and those working in the private sector. Many Thai citizens had difficulty gaining access to necessary healthcare services and medicines. Type 2 drugstores with trained personnel were one solution to this problem. Type 2 drugstores have been allowed to distribute non-dangerous drugs (OPS drugs) and household remedies (GSL drugs) to communities in order to ensure that people can gain access to drugs easily.
The regulations regarding drug classification have never been amended, even though Thailand’s healthcare system has changed tremendously over the past 20 years. Significant improvements in the Thai healthcare system have included the implementation of a universal health insurance system, increasing the pharmacist-to-population ratio, increasing numbers of type 1 community pharmacies, implementing pharmacy accreditation system, enforcing good pharmacy practice, and implementing continuing education for pharmacists and other healthcare professionals along with a professional re-licensing system.Citation5,Citation14 At the present, the Ministry of Public Health has ceased issuing type 2 drugstore licensure.Citation10 This is because the level of type 1 modern community pharmacies is adequate for the population, thus type 2 drugstores are expected to decrease and eventually become extinct.
Although our findings show that Thailand has similar drug classification criteria as other countries, the actual classification of individual drugs is notably different from other countries, especially for antibiotics, hypertension treatments, and dyslipidemia treatments. These drugs are classified as dangerous drugs (BTC drugs), and by law, they should be a pharmacist’s responsibility to dispense. Therefore, if these drugs continue to be in the BTC drug category, pharmacists must have a clear scope of practice when they provide care to patients who use these drugs.
Questions regarding the drug regulatory direction of Thailand were also raised, such as whether the four-drug classification system is still suitable, whether drug classification criteria are still valid, and whether current actual drug classification is still appropriate.
First, how many drug categories does Thailand need? Thailand can choose either a four- or three-drug classification categories (the current system and the new system wherein the OPS drug category will be collapsed into the GSL drug category). This decision should be made by regulators after taking into consideration all relevant medical, economic, and social aspects. If quality of service and patient safety are the main focuses for change, a three-drug classification system is preferable. Non-dangerous drugs (OPS drugs) should be subsumed into household remedies (GSL drugs) and type 1 modern community pharmacies will continue to sell BTC drugs. However, if easy access to OPS drugs is still the main focus, as in the past, then a four-drug classification system should continue. It should be noted that if the three-drug classification system is selected immediately, this will affect the viability of existing type 2 drugstores, and thus regulators should implement a fairness policy for these stakeholders before implementing any widespread change.
Second, are the drug classification criteria still valid? Thailand’s drug classification criteria are comparable to other countries. However, some actual drug classifications were found to conflict with other countries, especially hypertension treatments, dyslipidemia treatments, diabetes treatments, and antibiotics. It can be concluded that actual drug classification does not conform with the criteria. This is because the drug classification criteria in Thailand were updated for drug re-classification consideration in 2016. Drugs that were previously classified before 2016 were not harmoniously conformed with the updated criteria.Citation11 Considering the principles of drug classification criteria; hypertension treatments, dyslipidemia treatments, and diabetes treatments should be classified as prescription drugs since they require physicians’ involvement for disease diagnosis and monitoring. For antibiotics, bacterial resistance is one of the most concern issue of this era, and many countries are trying to limit distribution by classifying them as prescription drugs as is shown in . Although Canada is the only country that currently uses this as an actual criterion, the comparison of actual drug classification implies that most countries are concerned about this issue. Thus, it is crucial for Thai regulators to consider re-classifying these drugs as prescription drugs.
Although the healthcare system in Thailand has evolved enormously since 2003, many drugs which should require a prescription remain under the BTC drug category. Ignorance concerning the review and management of the drug statuses might result from multiple factors and from various stakeholders, such as pharmaceutical companies, community pharmacies, and physicians. One factor is that drug regulatory agencies do not have enough adverse event reports to support switching from BTC to prescription drug categories. In the past decade, only some drugs were upwardly recategorized based on supporting evidence, for example, anti-tuberculosis drugs were switched from dangerous drugs (BTC drugs) to specially controlled drugs (prescription drugs) because of a demonstrated antibiotic resistance.Citation89 This change was well known by healthcare professionals, but not realized by the consumers. However, some changes have had unintended consequences, such as when pseudoephedrine was reclassified from being a psychotropic substance that was non-prescription to being a prescription drug that could only be distributed by hospitals. This resulted in a block to direct access for those having nasal congestion.Citation69 Moreover, pharmaceutical companies were asked to replace pseudoephedrine with other drugs in combination preparations for nasal congestion in order to maintain a BTC status. This change has directly affected patients’ quality of life, ease of access to common drugs, and healthcare expenditures for many patients who suffer from nasal congestion.
In response to this, a few policy recommendations have been formulated. First, although the drug classification criteria in Thailand are well established, there is concern regarding injections. The current criteria imply that injections can be classified as prescription or BTC drugs. However, since pharmacists in Thailand cannot vaccinate or inject patients, injections should not be under pharmacists’ control, or, in other words, cannot be classified into the BTC drug category. Thus, the criteria should specify that injections must be classified only as prescription drugs.
Second, the Thai FDA should re-evaluate drugs listed under the dangerous drug (BTC drug) category to standardize which drugs should be switched to prescription drugs. If the status of these drugs remains unchanged, it is necessary to review the pharmacist’s role and responsibility over these drugs. There should be a pharmacy practice guideline, referral guideline, and continuing education that enhances pharmacists’ knowledge and skill to care for their patients. There could even be a certified system to ensure that pharmacists as providers are qualified to take care of those drugs.
Third, the general public should be empowered to better understand about association between drug classification and drug access. Prescription drugs must be dispensed in community pharmacies only when prescriptions are presented to the pharmacists. Thai citizens should not need to always visit hospitals for non-prescription drugs since these drugs are available for patients to self-medicate. It is important to empower Thai citizens by educating them about their responsibility for their own health, and to make sure the population understands which situations necessitate visits to hospitals. If their symptoms are minor ailments, they should self-medicate from pharmacies or non-pharmacy retailers first, and avoid excessive hospital visits. Patient information leaflets, labels, advertisements, and other developed digital media may be good options to educate citizens.
Some limitations to these suggestions have been observed. First, classification criteria are amended continuously, and therefore the information gathered in this study may not have captured all these changes. However, we believe that the core principles were captured and that the findings are robust enough to use as supporting evidence. Second, we found that the Philippines’ drug database that we used to compare actual drug status was not up to date. Drugs with the same active pharmaceutical ingredient should be in the same category, but various categories were observed. Nonetheless, we interviewed an expert who works in the Food and Drug Administration of the Philippines to confirm the status of these drugs. Third, the drug regulatory authorities of some countries provide information only in their local languages, such as Japan, Malaysia, and the Philippines. Therefore, information searching, gathering and comprehension from these countries was more difficult and required assistance from native speakers. Lastly, since the discussion of this study was based on gathered evidence from documents, several points, such as patients’ behavior, were not included in this study. Thus, further focus groups or public hearings from various stakeholders are necessary to conduct before any meaningful implementation.
Conclusion
In Thailand, drug classification systems should be updated to be more aligned with the country’s individual healthcare context, such as healthcare professionals’ scope of responsibility. A spotlight should be pointed on drugs intended to be prescription drugs (specially controlled drugs) misclassified as behind the counter drugs (dangerous drugs) as this misclassification could pose a higher risk to the public. Drug regulatory agencies should also educate the general public regarding drug classification systems to empower them to understand when they need to seek care from physicians or when they can practice self-medication.
Acknowledgments
The Scholarship from the Graduate School, Chulalongkorn University to commemorate the 72nd anniversary of his Majesty King Bhumibol Adulyadej is gratefully acknowledged.
We also would like to extend our appreciation to Assistant Professor Rungpetch Sakulbumringsil, Assistant Professor Suthira Taychakhoonavudh, and Associate Professor Susi Ari Kristina, for their recommendations, which helped to improve this study.
In addition, our sincere thanks also goes to Nattaporn Piensaknusorn and Sirisopa Nakawong, Nantarat Sukrod, Dr Mohd Shahezwan Abd Wahab, Mallenrose Kristine Marcelo Ofrecio, Taichi Hiraga, and Fumiya Seki for providing valuable information and translating several non-English documents. Last, but not least, we would like to thank Stephen Pinder and Laura Saxton for their dedicated English proofreading.
Disclosure
Noppadon Adjimatera is a committee of the Thailand Self Medication Industry Association and an employee of Reckitt Benckiser (Thailand) Ltd. Lawanworn Broese Van Groenou is an employee of DKSH (Thailand) Limited. The authors report no other potential conflicts of interest in this work.
References
- Sukrod N. Principle of Thailand medicine reclassification guidelines; 2015 Available from: http://www.tsmia.or.th/RTD2015/5-THAILAND%20(Sept%2017)%20Drug%20reclassification%20guideline%20(final).pdf. Accessed 423, 2020.
- Consumer Healthcare Product Association. Rx-to-OTC switch; 2019 Available from: https://www.chpa.org/switch.aspx. Accessed 1023, 2019.
- GOV.UK. Oral diclofenac presentations with legal status ‘P’ – reclassified to POM; 2015 Available from: https://www.gov.uk/drug-device-alerts/drug-alert-oral-diclofenac-presentations-with-legal-status-p-reclassified-to-pom. Accessed 1023, 2019.
- Consumer Healthcare Product Association. Rx-to-OTC switch: switch list; 2018 Available from: https://www.chpa.org/Switch.aspx. Accessed 1026, 2019.
- World Bank Group President Jim Yong Kim. Speech by World bank group president Jim Yong Kim on universal health coverage in emerging economies; 2014 Available from: https://www.worldbank.org/en/news/speech/2014/01/14/speech-world-bank-group-president-jim-yong-kim-health-emerging-economies. Accessed 82, 2020.
- Sakulbumrunsul R, Taychakhoonavudh S. Pricing and patient access framework to support universal coverage in Thailand. Available from: http://www.pharm.chula.ac.th/dept5/source/images/data/files/NHSO_PPA_Report_240317(2).pdf. Accessed 1217, 2020.
- Strategy and planning division: Office of the Permanent Secretary for Ministry of Public Health. Number of hospitals by category in Thailand; 2014 Available from: http://203.157.10.8/hcode_2014/query_02.php?p=3%20/. Accessed 412, 2020.
- Thai Food and Drug Administration. Number of pharmacies; 2017 Available from: http://www.fda.moph.go.th/sites/drug/Shared%20Documents/Statistic/establishment.pdf. Accessed 423, 2020.
- Saramunee K, Chaiyasong S, Krska J. Public health roles for community pharmacy: contrasts and similarities between England and Thailand. Isan J Pharm Sci. 2011;7(2):1–11.
- Thai Food and Drug Administration. Designation of number of type 2 community pharmacies; 2005 Available from: http://www.ratchakitcha.soc.go.th/DATA/PDF/2548/00155157.PDF?fbclid=IwAR2Qksp4wyeb5ZnkhGZXUNyigAjknzu92GMReDzdSdIfZGWjd6E32VwRwwE. Accessed 423, 2020.
- Thai Food and Drug Administration. Guideline of drug reclassification; 2016 Available from: http://www.fda.moph.go.th/sites/drug/Shared%20Documents/reclass/%E0%B8%A0%E0%B8%B2%E0%B8%84%E0%B8%9C%E0%B8%99%E0%B8%A7%E0%B8%81%20%E0%B8%84.pdf. Accessed 1023, 2019.
- The drug act (No. 6) B.E. 2562 (A.D. 2019). Available from: https://sme.go.th/upload/mod_download/download-20190508065825.PDF. Accessed 1218, 2019.
- World Health Organization. Thailand pharmaceutical profile; 2017 Available from: https://apps.who.int/iris/bitstream/handle/10665/274873/2017-Thailand-pharm-profile.pdf?sequence=1&isAllowed=y. Accessed 423, 2020.
- Chan RC, Ching PL. Pharmacy practice in Thailand. Am J Health Syst Pharm. 2005;62(13):1408–1411. doi:10.2146/ajhp04039315972385
- Sriviriyanupap W. Developing indicators and method of drug classification according to Thai law. Thai J Pharm Sci. 2016;40.
- MGR Online. The propose of new drug classification scheme; 2018 Available from: https://mgronline.com/qol/detail/9610000088655. Accessed 1025, 2019.
- Sumpradit N, Chongtrakul P, Anuwong K, et al. Antibiotics smart use: a workable model for promoting the rational use of medicines in Thailand. Bull World Health Organ. 2012;90(12):905–913. doi:10.2471/BLT.12.10544523284196
- Bangkok Post. Teens taking ‘taxi’ ride to drug addiction; 2018 Available from: https://www.bangkokpost.com/thailand/special-reports/1529006/teens-taking-taxi-ride-to-drug-addiction. Accessed 423, 2020.
- Thai Food and Drug Administration. Counterfeit drug manufacturing was found; 2018 Available from: http://pca.fda.moph.go.th/public_media_detail.php?id=2&cat=50&content_id=1671. Accessed 425, 2020.
- Thai Food and Drug Administration. Risks of 4x100 (pro drug); 2020 Available from: https://oryor.com/oryor_miniweb/knowledge_detail.php?cat=2&id=7. Accessed 423, 2020.
- Thai Food and Drug Administration. Drug database; 2019 Available from: http://pertento.fda.moph.go.th/FDA_SEARCH_DRUG/SEARCH_DRUG/FRM_SEARCH_DRUG.aspx. Accessed 114, 2019.
- GOV.UK. Medicines: reclassify your product; 2019 Available from: https://www.gov.uk/guidance/medicines-reclassify-your-product#classifications-of-medicines. Accessed 1023, 2019.
- Homhuan A. Amendments to Thailand’s drug act; 2019 Available from: https://www.tilleke.com/resources/amendments-thailand%E2%80%99s-drug-act. Accessed 82, 2020.
- Nomura K, Kitagawa Y, Yuda Y, Takano-Ohmuro H. Medicine reclassification processes and regulations for proper use of over-the-counter self-care medicines in Japan. Risk Manag Healthc Policy. 2016;9:173. doi:10.2147/RMHP.S9809927555801
- Gauld NJ, Kelly FS, Emmerton LM, Buetow SA. Widening consumer access to medicines: a comparison of prescription to non-prescription medicine switch in Australia and New Zealand. PLoS One. 2015;10(3):e0119011. doi:10.1371/journal.pone.011901125785589
- Gauld NJ, Kelly FS, Kurosawa N, Bryant LJ, Emmerton LM, Buetow SA. Widening consumer access to medicines through switching medicines to non-prescription: a six country comparison. PLoS One. 2014;9(9):e107726. doi:10.1371/journal.pone.010772625251434
- World Health Organization. Proposal for updating the definition of stringent regulatory authority; 2017 Available from: https://www.who.int/medicines/areas/quality_safety/quality_assurance/SRA_QAS17-728Rev1_31082017.pdf?ua=1. Accessed 1026, 2019.
- The International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use. Members & observers; 2019 Available from: https://www.ich.org/page/members-observers. Accessed 1026, 2019.
- Association of Southeast Asian Nations. ASEAN member states; 2019 Available from: https://asean.org/asean/asean-member-states/. Accessed 1210, 2019.
- Filmer D, Rogers H, Angrist N, Sabarwal S. Learning-Adjusted Years of Schooling (LAYS): Defining a New Macro Measure of Education. The World Bank; 2018.
- Human development index (HDI) by country; 2019 Available from: http://worldpopulationreview.com/countries/hdi-by-country/. Accessed 112, 2020.
- United Nations Development Programme. Global human development indicators; 2020 Available from: http://hdr.undp.org/en/countries/profiles/. Accessed 425, 2020.
- The World Bank. Education Statistics. 2019 Available from: https://databank.worldbank.org/indicator/UIS.SAP.CE?id=c755d342&report_name=EdStats_Indicators_Report&populartype=series. Accessed 112, 2020.
- World Health Organization. Density of physicians. Available from: https://www.who.int/gho/health_workforce/physicians_density/en/. Accessed 425, 2020.
- World Health Organization. Pharmacists (per 10,000 populations). Available from: https://www.who.int/data/gho/data/indicators/indicator-details/GHO/pharmacists-(per-10-000-population). Accessed 425, 2020.
- Collins S. A tale of two countries: the path to pharmacist prescribing in the United Kingdom and Canada; 2014 Available from: https://www.pharmacist.com/article/tale-two-countries-path-pharmacist-prescribing-united-kingdom-and-canada. Accessed 112, 2020.
- Deloitte Access Economics. Remuneration and regulation of community pharmacy; 2016 Available from: https://www1.health.gov.au/internet/main/publishing.nsf/Content/4E0B6EEE19F56A40CA2581470016D688/$File/deloitte-community-pharmacy-literature-review-2016.pdf. Accessed 112, 2020.
- Nakagawa S, Kume N. Pharmacy practice in Japan. Can J Hosp Pharm. 2017;70(3):232. doi:10.4212/cjhp.v70i3.166328680178
- Competency standards for Singapore pharmacists; 2010 Available from: https://www.healthprofessionals.gov.sg/docs/librariesprovider3/forms-publications/competency-standards-for-singapore-pharmacists-(march-2010).pdf. Accessed 1113, 2020.
- Chau A. Are pharmacists’ roles as primary health professionals underutilised in Singapore? 2016 Available from: https://today.mims.com/are-pharmacists’roles-as-primary-health-professionals-underutilised-in-singapore-?channel=GN-Local-News-SG. Accessed 112, 2020.
- General Pharmaceutical Council. What does a pharmacist do? 2019 Available from: https://www.pharmacyregulation.org/raising-concerns/raising-concerns-about-pharmacy-professional/what-expect-your-pharmacy/what-does-0. Accessed 112, 2020.
- Albanese NP, Rouse MJ, Schlaifer M. Pharmacy CoCi. Scope of contemporary pharmacy practice: roles, responsibilities, and functions of pharmacists and pharmacy technicians. J Am Pharm Assoc. 2010;50(2):e35–e69. doi:10.1331/JAPhA.2010.10510
- Poisons act 1952 and regulations; 2019 Available from: http://www.agc.gov.my/agcportal/uploads/files/Publications/LOM/EN/Act%20366%20online.pdf. Accessed 112, 2020.
- Annuar A. Counter-productive’ for pharmacists to administer vaccines, doctors’ body says; 2019 Available from: https://www.malaymail.com/news/malaysia/2019/02/25/counter-productive-for-pharmacists-to-administer-vaccines-doctors-body-says/1726723. Accessed 112, 2020.
- Philippine Pharmacy Act. 2015 Available from: https://www.lawphil.net/statutes/repacts/ra2016/ra_10918_2016.html. Accessed 112, 2020.
- International Pharmaceutical Federation. An overview of current pharmacy impact on immunisation; 2016 Available from: https://www.fip.org/www/streamfile.php?filename=fip/publications/FIP_report_on_Immunisation.pdf. Accessed 112, 2020.
- Pharmaceutical Profession Act (No.2). 2015 Available from: https://library2.parliament.go.th/giventake/content_nla2557/law21-260358-69.pdf. Accessed 112, 2020.
- U.S. Food and Drug Administration. Prescription drug advertising; 2019 Available from: https://www.fda.gov/drugs/drug-information-consumers/prescription-drug-advertising. Accessed 425, 2020.
- GOV.UK. Advertise your medicines; 2020 Available from: https://www.gov.uk/guidance/advertise-your-medicines#advertise-to-the-public. Accessed 425, 2020.
- Graham JS, Swanson R. Distribution and marketing of drugs in Canada: overview; 2018 Available from: https://ca.practicallaw.thomsonreuters.com/0-618-6695?transitionType=Default&contextData=(sc.Default)&firstPage=true&bhcp=1. Accessed 425, 2020.
- Government of Canada. Health products advertising on physician web sites – questions and answers; 2011 Available from: https://www.canada.ca/en/health-canada/services/drugs-health-products/regulatory-requirements-advertising/policies-guidance-documents/health-products-advertising-physician-questions-answers.html. Accessed 425, 2020.
- Health Sciences Authority. Advertisements and promotions of therapeutic products; 2019 Available from: https://www.hsa.gov.sg/therapeutic-products/advertisements. Accessed 425, 2020.
- The international comparative legal guide to: pharmaceutical advertising; 2016 Available from: https://www.jurists.co.jp/sites/default/files/tractate_pdf/en/PA16_Japan.pdf. Accessed 425, 2020.
- Thai Food and Drug Administration. Things to know for drug advertisements; 2020 Available from: http://www.fda.moph.go.th/sites/drug/SitePages/advertisement03.aspx. Accessed 425, 2020.
- Baker M. Promoting medical products globally; 2018 Available from: https://www.bakermckenzie.com/-/media/files/insight/publications/2018/03/healthcare/ap/promoting-medical-products-globally_malaysia.pdf?la=en. Accessed 425, 2020.
- The ministry of health in collaboration with the World Health Organization. Philippines pharmaceutical country profile; 2011 Available from: https://www.who.int/medicines/areas/coordination/Philippines_PSCPBNarrativeQuestionnaireEndorsement_13062012.pdf?ua=1. Accessed 425, 2020.
- The food, drug, and cosmetic act, code of federal regulations. 2019.
- Medicines act 1968. 2020.
- Japan Pharmaceutical Manufacturers Association. Pharmaceutical administration and regulations in Japan; 2019 Available from: http://www.jpma.or.jp/english/parj/pdf/2019.pdf. Accessed 112, 2020.
- Health Products Act. 2016 Available from: https://sso.agc.gov.sg/SL/HPA2007-S329-2016. Accessed 112, 2020.
- National Association of Pharmacy Regulatory Authorities. Drug scheduling in Canada – general overview; 2019 Available from: https://napra.ca/drug-scheduling-canada-general-overview. Accessed 1210, 2019.
- U.S. Food and Drug Administration. How to buy medicines safely from an online pharmacy; 2018 Available from: https://www.fda.gov/consumers/consumer-updates/how-buy-medicines-safely-online-pharmacy. Accessed 425, 2020.
- GOV.UK. Register for the distance selling logo; 2017 Available from: https://www.gov.uk/guidance/register-for-the-distance-selling-logo. Accessed 425, 2020.
- Ministry of Health Malaysia. Tips on how to buy medicines online; 2020 Available from: https://www.pharmacy.gov.my/v2/en/content/tips-how-buy-medicines-online.html. Accessed 425, 2020.
- Government of Canada. Choosing a safe online pharmacy; 2020 Available from: https://www.canada.ca/en/health-canada/topics/buying-using-drug-health-products-safely/safe-use-online-pharmacies.html. Accessed 425, 2020.
- Faculty of Medicine Ramathibodi Hospital. Online drug sale; 2018 Available from: https://med.mahidol.ac.th/ramapharmacy/th/knowledge/general/05192016-1800-th. Accessed 220, 2020.
- Health Sciences Authority. Explanation note for application of a pharmacy licence; 2016 Available from: https://www.hsa.gov.sg/docs/default-source/hprg-ald/phl_explanation-noteb201f748dd3a4a8ca9bd36f432a3fded.pdf. Accessed 425, 2020.
- Consumer Healthcare Product Association. FAQs about drug distribution in the United States; 2019 Available from: https://www.chpa.org/FAQDrugDistribution.aspx. Accessed 1023, 2019.
- U.S. Food and Drug Administration. Legal requirements for the sale and purchase of drug products containing pseudoephedrine, ephedrine, and phenylpropanolamine; 2017 Available from: https://www.fda.gov/drugs/information-drug-class/legal-requirements-sale-and-purchase-drug-products-containing-pseudoephedrine-ephedrine-and. Accessed 112, 2020.
- National Association of Pharmacy Regulatory Authorities. Implementation of the national drug schedules; 2019 Available from: https://napra.ca/implementation-national-drug-schedules. Accessed 112, 2020.
- Comprehensive Dangerous Drugs Act. 2002 Available from: https://www.ddb.gov.ph/images/Board_Regulation/2014/BD.REG1.14.pdf. Accessed 112, 2020.
- Gauld N, Bryant L, Emmerton L, Kelly F, Kurosawa N, Buetow S. Why does increasing public access to medicines differ between countries? Qualitative comparison of nine countries. J Health Serv Res Policy. 2015;20(4):231–239. doi:10.1177/135581961559330226152909
- Hennebry S. When a 20 year patent term just isn’t enough: market and data exclusivity; 2018 Available from: https://fpapatents.com/resource?id=483. Accessed 425, 2020.
- Medicines and Healthcare products Regulatory Agency. How to change the legal classification of a medicine in the UK; 2006 Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/277307/Legal_classification_changes.pdf. Accessed 425, 2020.
- Agency for Care Effectiveness. Drug evaluation methods and process guide; 2018 Available from: http://www.ace-hta.gov.sg/public-data/our-process-and-methods/ACE%20methods%20and%20process%20guide%20for%20drug%20evaluation%20(5%20Feb%202018).pdf. Accessed 425, 2020.
- Gauld NJ. How and Why Do Developed Countries Vary in Reclassifying Medicines from Prescription to Non-Prescription? University of Auckland; 2013.
- Camargo. Rx-to-OTC switch: expanding to the US over-the-counter market; 2017 Available from: https://camargopharma.com/resources/blog/rx-to-otc-switch-expanding-to-the-us-over-the-counter-market. Accessed 425, 2020.
- Mithun Raja. B, Raghavendra Rao. K. Regulatory and clinical requirements for prescription to OTC switches in USA and India; 2013 Available from: https://www.complianceonline.com/articlefiles/Regulatory_Requirements_Prescription_to_OTC_Switches_USA_India.pdf. Accessed 112, 2020.
- U.S. Food and Drug Administration. Bringing an over-the-counter (OTC) drugs to market; 2020 Available from: https://www.accessdata.fda.gov/scripts/cder/training/OTC/topic2/topic2/da_01_02_0080.htm. Accessed 425, 2020.
- Health Sciences Authority. Therapeutic products guidance; 2019 Available from: https://www.hsa.gov.sg/docs/default-source/hprg/therapeutic-products/guidance-documents/guidance-on-therapeutic-product-registration-in-singapore_jan2019.pdf. Accessed 425, 2020.
- Tago S, Ueda A, Kudo R, Guesdon L. Distribution and marketing of drugs in Japan: overview; 2019 Available from: https://uk.practicallaw.thomsonreuters.com/5-618-3562?transitionType=Default&contextData=(sc.Default)&firstPage=true&comp=pluk&bhcp=1. Accessed 425, 2020.
- National Association of Pharmacy Regulatory Authorities. National drug scheduling factors; 2017 Available from: https://napra.ca/sites/default/files/documents/NDSAC_Scheduling_Factors_website_September2017.pdf. Accessed 112, 2020.
- Katsura H. The approval standards for OTC drugs in Japan; 2015 Available from: http://www.tsmia.or.th/RTD2015/2-Japan%202nd%20self-CARER%20(PMDA%20Ehidemi%20Katsura).pdf. Accessed 117, 2020.
- Bakah SA. Regulation of OTC medicines in Malaysia; 2017 Available from: https://www.tga.gov.au/sites/default/files/international-over-counter-otc-medicines-regulators-forum-2017-malaysia.pdf. Accessed 1113, 2020.
- Official Portal of Pharmaceutical Services Programme, Ministry of Health Malaysia. Application for poisons classification guideline under the poisons act 1952; 2013 Available from: https://www.pharmacy.gov.my/v2/sites/default/files/document-upload/garispanduan.pdf. Accessed 112, 2020.
- Policies and guidelines on over-the-counter (OTC) drug products; 2000 Available from: https://ww2.fda.gov.ph/attachments/article/16557/ao%2023c%202000.pdf. Accessed 112, 2020.
- Republic of the Philippines DoH, Food and Drug Administration. Application process and requirements for post-approval changes of pharmaceutical products; 2014 Available from: https://ww2.fda.gov.ph/attachments/article/148395/FC2014-008%20-%20Application%20Process%20and%20Requirments%20for%20Post-Approval%20Changes%20of%20Pharmaceutical%20Products.pdf. Accessed 425, 2020.
- Ministry of Public Health. 30th notification of dangerous drugs; 2018 Available from: http://www.fda.moph.go.th/sites/drug/Shared%20Documents/Law03-TheMinistryOfHealth/Dangerousdrugs(30).PDF. Accessed 82, 2020.
- Ministry of Public Health. 53th notification of specially controlled drugs; 2019 Available from: http://www.fda.moph.go.th/sites/drug/Shared%20Documents/Law03-TheMinistryOfHealth/SPC(53).pdf. Accessed 82, 2020.