
Abstract
Background
The outbreak of coronavirus disease 2019 (COVID-19) in Wuhan, China, spreads globally, since its declaration by the World Health Organization (WHO) as a COVID-19 pandemic on March 11, 2020. COVID-19 vaccine is a crucial preventive approach that can halt this pandemic. The present systematic review was aimed to assess the level of willingness to receive COVID-19 vaccine and its associated factors.
Methods
A comprehensive literature search was conducted by using various online databases such as PubMed/MEDLINE, HINARI, EMBASE, Google Scholar, Web of Science, Scopus, African journals, and Google for grey literature which were used to search the related articles up to the period of May 08, 2021.
Results
The overall rate of participants’ willingness to receive the COVID-19 vaccine was ranged from 27.7% to 91.3%, which was from Congo and China, respectively. Factors such as age, educational status, gender, income, residency, occupation, marital status, race/ethnicity, perceived risk of COVID-19, trust in healthcare system, health insurance, norms, attitude towards vaccine, perceived benefit of vaccine, perceived vaccine barriers, self-efficacy, up-to-date on vaccinations, tested for COVID-19 in the past, perceived efficacy of the COVID-19 vaccination, recommended for vaccination, political leaning, perceived severity of COVID-19, perceived effectiveness of COVID-19 vaccine, belief that vaccination makes them feel less worried about COVID-19, believing in mandatory COVID-19 vaccination, perceived potential vaccine harms, presence of chronic disease, confidence, COVID-19 vaccine safety concern, working in healthcare field, believing vaccines can stop the pandemic, fear about COVID-19, cues to action, COVID-19 vaccine hesitancy, complacency, and receiving any vaccine in the past 5 years were associated with the willingness of receive COVID-19 vaccine.
Conclusion
There were insufficient levels of willingness to receive COVID-19 vaccine, and several factors were associated with it. Health education should be provided concerning this vaccine to improve the willingness of the community.
Introductions
The COVID-19 is caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).Citation1–Citation5 Since the first case was reported from Wuhan, China, the Chinese government has taken the emergency actions to control the outbreak and has performed preliminary steps in the diagnosis and treatment of this COVID-19 pandemic.Citation6 The commonly detected severe risk factors of COVID-19 include older age and with medical comorbidities like cancer and diabetes.Citation1 The outbreak of COVID-19 disease in China has been brought to global attention and declared as a pandemic by the WHO on March 11, 2020.Citation7 The COVID-19 pandemic remains a global challenge.Citation3 It is a highly contagious disease. The WHO has declared the ongoing outbreak to be a global public health emergency.Citation8 There is an obvious concern worldwide regarding the fact about the emerging 2019‐nCoV as a global public health threat.Citation5 The pandemic of COVID-19 is spreading rapidly.Citation9 The COVID-19 is spreading all over the world.Citation10,Citation11 Then, it has affected individuals of all nations, continents, races, and socioeconomic groups.Citation11 This pandemic COVID-19 has significant mortality and morbidity rate.Citation1,Citation9,Citation12 As per the report from WHO on 14 August 2020, there have been 20,730,456 confirmed cases of COVID-19, including 751,154 deaths worldwide.Citation13 Besides, the significant deaths and morbidities from the COVID-19 pandemic, there will also be a substantial economic crisis by far.Citation14 This large morbidity and socioeconomic influence have demanded extreme measures across all continents, comprising nationwide lockdowns and border closures.Citation15
Furthermore, the COVID-19 pandemic has the potential to overwhelmingly affect young children’s development worldwide, through rises in poverty and food insecurity, loss of caregivers, heightened stress, and decreased health care. These can affect not only the whole life course of the child but also the future generations through physiological, psychological, and epigenetic changes occurring in utero and during early development that can decelerate the gains made since the turn of the century.Citation16 Because of this COVID-19 pandemic, mental health is a major public issue.Citation17 It has an immense influence on youth mental health.Citation18 It has put considerable stress on patients, healthcare workers (HCWs), and healthcare systems. However, fetal diagnosis and pregnancy care must be maintained, and we must struggle to protect the susceptible population of pregnant women and their fetuses.Citation19 COVID-19 has a higher burden on the emotional wellbeing of pregnant women and women in the early postpartum period.Citation20 Probably, there is the potential for pregnant women to be vulnerable to mental ill health during this pandemic virus.Citation21 Besides, COVID-19 pandemic was significantly interrupted the childhood vaccination practices.Citation22
The COVID-19 pandemic is a serious public health emergency, it is particularly deadly in exposed populations and communities in which healthcare providers are inadequately ready to manage the infection.Citation15 The responses required for COVID-19 pandemic were such as quarantining of entire communities, closing of schools, social isolation, and shelter in-place orders which have abruptly changed daily life to control the disease.Citation11 The management of patients with severe COVID-19 status is significant in decreasing the mortality of the ongoing pandemic, but the truly essential measures include prevention, monitoring, and timely intervention. Besides, in addition to rapid medical responses, continuous efforts to better understand the pathogenesis of COVID-19 will certainly enlighten the optimal management of the increasing pandemic.Citation9 The social media has the potential to provide rapid and effective dissemination routes for key information to enhance awareness about COVID-19 pandemic of the population if used responsibly and appropriately.Citation23
To decrease the spread of COVID-19, contact tracing, testing, and social restrictions are among the most powerful approaches adopted globally due to the lack of a COVID-19 vaccine. This leads to major physical, psychological, and economic distress suffering of most countries’ citizens. Thus, a safe and effective COVID-19 vaccine is the most effective alternative to manage this pandemic.Citation24 The COVID-19 pandemic is anticipated to continue to put large impacts of morbidity and mortality, while harshly upsetting society and economies globally. Thus, governments must be ready to make certain large-scale distribution of a COVID-19 vaccine and equitable access when a safe and effective vaccine is available. This will need sufficient health system capacity and methods to improve trust in and acceptance of the vaccine and those who deliver it.Citation25 The study has found that information concerning the process of vaccine development, vaccine efficacy, and individual variety affects the proportion of participants reporting COVID-19 vaccination intentions. Behavioral economics offers an empirical scheme to approximate vaccine claims to target subpopulations resistant to vaccination.Citation26
Methods
Research Questions
What is the level of willingness to receive COVID-19 vaccine globally?
What are the factors associated with the willingness to receive COVID-19 vaccine?
Study Setting
The present systematic review includes all studies conducted in different countries globally.
Search Strategies
A comprehensive literature search was conducted. For instance, The search was conducted by using the following electronic databases: PubMed/MEDLINE, HINARI, EMBASE, Google Scholar, Web of Science, Scopus, African journals, and Google for grey literature. The search was done by using the following keywords; “willingness”, “acceptance”, “hesitancy”, “COVID-19”, “SARS-CoV-2”, “vaccine”, “associated factors”, and “determinant factors”. At this time, “AND” and “OR” Boolean operators were employed to integrate the keywords.
Eligibility Criteria
The inclusion criteria for the present systematic review were: all cross-sectional studies done among adults globally, published in English language, and articles published until May 08, 2021 duration, whereas the exclusion criteria were as follows: articles with poor quality and articles in which the outcome variable was not clearly defined and measured were excluded from the present systematic review.
Outcome of Interest
In the present systematic review, the primary outcome was the level of willingness to receive COVID-19 vaccine, which was reported within the original article. Likewise, the secondary outcome was factors associated with the willingness to receive COVID-19 vaccine, which was reported within the original study.
Data Extraction
All studies obtained from all databases were exported to Endnote version 8 software, and the duplicates were removed. Finally, all studies were exported to Microsoft Excel spreadsheet. The Titles and abstracts of studies retrieved using the search strategy and those from additional sources were screened to identify studies that satisfy the inclusion criteria. Then, studies that satisfied the inclusion criteria by title or abstract screening were undergone a full-text review for eligibility and data extraction. The Preferred Reporting Item for Systematic Review and Meta-Analyses (PRISMA) flowchart was used for the stepwise inclusion and exclusion of the articles. The first author, publication year, country, sample size, prevalence, and factors were included into the data extraction format.
Quality Assessment
The Newcastle–Ottawa Scale (NOS) quality assessment criteria for cross-sectional studies were used to include the studies into the present systematic review.Citation27,Citation28 The quality of each study was assessed using modified NOS for cross-sectional studies. It has 10 points in three domains of modified NOS components for observational studies. Thus, the studies which were scored ≥5 out of 10 points were included into the present systematic review.Citation29
Results
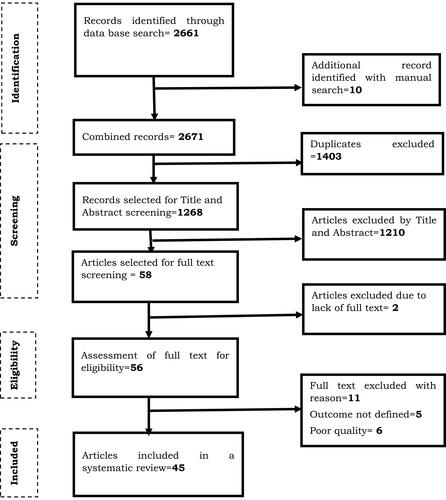
A total of 2671 articles were identified through the search strategies. They were retrieved from PubMed/MEDLINE, HINARI, EMBASE, Google Scholar, Web of Science, Scopus, African journals, and Google for grey literature. From the total of 2671, 1403 articles were excluded because of duplication. Of the remaining 1268 articles, 1210 articles were excluded after reviewing of the titles and abstracts because they were not related. Furthermore, out of 58 articles selected for full-text screening, 2 were excluded due to lack or inaccessible of full text. Then, 56 full-text articles were assessed for eligibility based on the pre-setted criteria and 11 articles were excluded with a reason. Finally, 45 articles were met the eligibility criteria and included into the present systematic review ().
Figure 1 PRISMA flowchart diagram of the study selection for systematic review on the willingness to receive COVID-19 vaccine and its associated factors. Note: Adapted from Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339 jul21 1:b2700–b2700. doi:10.1136/bmj.b2700.Citation95
Features of the Included Studies
Characteristics of the studies included in the present systematic review on the willingness to receive COVID-19 vaccine and its associated factors. Among the studies published up to May 08, 2021 globally, 45 studies were included in the present systematic review. The study design of all these studies were cross-sectional. Nine studies were done in the United States,Citation30–Citation38 nine studies were done in China,Citation39–Citation47 one study was done in Australia,Citation48 four studies were done in Saudi Arabia,Citation49–Citation52 one study was done in Kuwait,Citation53 one study was done in England,Citation54 one study was done in Congo,Citation55 one study was done in Greece,Citation56 two studies were done in UK,Citation57,Citation58 one study was done in Malaysia,Citation59 two studies were done in Japan,Citation60,Citation61 one study was done in Israel,Citation62 one study was done in Bangladesh,Citation63 one study was done in Jordan,Citation64 one study was done in Iran,Citation65 one study was done in Italy,Citation66 one study was done in Ethiopia,Citation67 two studies were done in France,Citation68,Citation69 one study was done in Vietnam,Citation70 one study was done in Uganda,Citation71 one study was done in Pakistan,Citation72 one study was done in Nigeria,Citation73 and one study was done in Latin America and the Caribbean (LAC).Citation74 The smallest sample size was 409 and the largest was 472,521, which was reported from Ethiopia,Citation67 and LAC,Citation74 respectively ().
Table 1 Characteristics of the Studies Included into the Present Systematic Review on the Level of Willingness to Receive COVID-19 Vaccine and Its Associated Factors
The Willingness to Receive COVID-19 Vaccine
As briefly displayed in (), 45 studies from various countries were included into the present systematic review. A large variability was stated on the level of willingness to receive COVID-19 vaccine in different countries. The highest level of willingness towards receiving the COVID-19 vaccine was reported from China, which was 91.3%,Citation47 whereas the lowest level of willingness towards receiving the COVID-19 vaccine was recorded in Congo, which was 27.7%.Citation55
Factors Associated with the Willingness to Receive COVID-19 Vaccine
From a total of 45 studies, 6 studies have not assessed the factors associated with the willingness of receiving COVID-19 vaccine. They were two studies from the United States,Citation33,Citation38 one study from Bangladesh,Citation63 one study from Jordan,Citation64 one study from Italy,Citation66 and one study from Ethiopia.Citation67 Generally, the present systematic review has briefly summarized factors associated with the willingness of receiving COVID-19 vaccine. They were; age, educational status, gender, income, residency, occupation, marital status, race/ethnicity, perceived risk of COVID-19, trust in healthcare system, health insurance, norms, attitude towards a vaccine, perceived benefit of vaccine, perceived vaccine barriers, self-efficacy, up-to-date on vaccinations, tested for COVID-19 in the past, responsibility, perceived efficacy of the COVID-19 vaccination, use of social media for COVID-19 vaccine-related information, recommended for vaccination, political leaning, perceived severity of COVID-19, perceived effectiveness of a COVID-19 vaccine, belief that vaccination makes them feel less worried about COVID-19, believing in mandatory COVID-19 vaccination, perceived potential vaccine harms, presence of chronic disease, previously received an influenza vaccine, confidence, having COVID-19 vaccine safety concern, working in the healthcare field, believing vaccines can stop the pandemic, relying on Centers for Disease Control and Prevention website for COVID-19 updates, fear about COVID-19, being HCWs, close attention to the latest news of the vaccine, cues to action, COVID-19 vaccine hesitancy, receiving any vaccine in the past 5 years, perception of disease can be prevented by vaccine, willingness to protect others by getting oneself vaccinated, taking direct care of COVID-19 patients, belief that only people who are at risk of serious illness should be vaccinated, trust in government, complacency, willingness to pay for and travel for a vaccine, themselves or a member of their household belonged to a vulnerable group, trust in public health authorities, believing COVID-19 virus was not developed in laboratories, believing COVID-19 is far more contagious and lethal relative to the H1N1 virus, compliance with community mitigation strategies, being in a private sector, encountering with suspected or confirmed COVID-19 patients, self-reported health outcomes, believing that next waves COVID-19 are coming, knowledge score regarding symptoms, transmission routes and prevention and control measures against COVID-19, and perception that COVID-19 will persist ().
Discussion
It is known that more than half of the world’s population faces long-term restrictions as the new normal to avoid the spread of COVID-19.Citation75 As the COVID-19 pandemic is extensive across the worldwide, there is an urgent requirement to develop effective vaccines as the most powerful approach to stop the pandemic.Citation76 Scientists are suffering to offer a verified treatment for COVID-19. This is due to that the development of vaccines against COVID-19 and their global access are a priority to end the pandemic. However, the success of this approach depends on individuals’ willingness of immunization. Questions like “what will happen if the individuals’ do not want the injection?” is what makes worry the experts. Because of this, numerous experts have warned against a worldwide for the decrease in community trust in immunization and the rise of vaccine hesitancy during the past decade.Citation77
The present systematic review has included all cross-sectional studies conducted on the willingness to receive COVID-19 vaccine and its associated factors. This is because understanding the level of willingness to receive and the associated factors of COVID-19 vaccine would provide valuable knowledge and direction for clinical implementation and intervention development. The present systematic review has reviewed all evidences on the willingness to receive COVID-19 vaccine and its associated factors. During this, 45 cross-sectional studies from different countries were included. The findings of the present systematic review revealed that there was a large variability on the level of willingness to receive COVID-19 vaccine in different countries. The overall rate of participants’ willingness to receive a COVID-19 vaccine was ranged from 27.7% to 91.3%, which was reported from Congo and China, respectively.Citation47,Citation55 This suggests that there is a serious problem to manage and control of the current COVID-19 pandemic. For the purpose of a permanent solution, vaccines are being developed by numerous countries for the safety of their populations for the current COVID-19 pandemic.Citation60 This is because, if a vaccine becomes available, it might be achievable to develop herd immunity and guard those who are most susceptible to the critical consequences of COVID-19.Citation75 However, with this level of willingness towards receiving COVID-19 vaccine, it would be extremely difficult to manage and control the current COVID-19 pandemic. By in turn, this might prolong the period of this pandemic affecting all populations of age category globally.
Concerning to the associated factors, from a total of 45 studies included in the present systematic review, 39 of the studies have assessed the associated factors with individuals’ willingness of receiving COVID-19 vaccine. From 39 studies assessed the associated factors with willingness of receiving COVID-19 vaccine, some of the studies have reported that sociodemographic factors such as age,Citation32,Citation35–Citation37,Citation39,Citation43,Citation48,Citation49,Citation56,Citation58,Citation60,Citation61,Citation65,Citation68,Citation69,Citation72,Citation73 educational status,Citation30–Citation32,Citation36,Citation43,Citation72 gender,Citation32,Citation35–Citation37,Citation47,Citation48,Citation52,Citation53,Citation55,Citation59–Citation61,Citation65,Citation68,Citation69,Citation71–Citation74 income,Citation36,Citation54,Citation61 residency,Citation36,Citation60,Citation74 occupation,Citation54,Citation62 marital status,Citation47,Citation49,Citation71 and race/ethnicityCitation32,Citation35,Citation37,Citation54 were factors associated with willingness of receiving COVID-19 vaccine. This might be due to that education is a powerful strategy to disseminate the essential information about the health of individuals. In fact, the level of education of people will affect the general knowledge and awareness of the individuals in particular, whereas residency has also an effect on information achievement since the urban population receives information more easily when compared to the rural population. Occupation could also affect the willingness of individuals towards receiving COVID-19 vaccine in many ways of which like being HCWs or being stressed for his/her work is among them while they are eager for vaccination relative to their contrary. Age has also an impact on the willingness of people towards this vaccine. Particularly, older age individuals might have a sense of responsibility and accountability for themselves and their families’ relative to the youngest age group individuals. The level of income also affects the willingness of an individual towards this vaccine. The possible justification would be that the expenses paid for the transport purpose. Concerning to the marital status; this could also affect the willingness of the individual towards this vaccine, while married individuals have relatively a feeling of more responsible because of their collective family responsibilities.
Furthermore, the study reported that factors such as perceived risk of COVID-19,Citation30,Citation31,Citation34,Citation44,Citation47,Citation50,Citation51,Citation53,Citation58,Citation59,Citation68–Citation71 trust in healthcare system,Citation46,Citation51 health insurance,Citation31,Citation48 norms,Citation31,Citation65 attitude towards a vaccine,Citation31,Citation55,Citation58 perceived benefit of vaccine,Citation31,Citation40,Citation46,Citation65,Citation70 perceived vaccine barriers,Citation31,Citation40,Citation70 self-efficacy,Citation31 up-to-date on vaccinations,Citation32 being tested for COVID-19 in the past,Citation32,Citation72 responsibility,Citation39 perceived efficacy of the COVID-19 vaccination,Citation41,Citation47 use of social media for COVID-19 vaccine-related information,Citation41 recommended for vaccination,Citation34 political leaning,Citation34 perceived severity of COVID-19,Citation34,Citation44,Citation46,Citation70,Citation74 perceived effectiveness of a COVID-19 vaccine,Citation34,Citation43,Citation59,Citation61 belief that vaccination makes them feel less worried about COVID-19,Citation59 believing in mandatory COVID-19 vaccination,Citation50 perceived potential vaccine harms,Citation34,Citation42,Citation53,Citation58 presence of chronic disease,Citation45,Citation48,Citation60 previously received an influenza vaccine,Citation43,Citation45,Citation47,Citation50,Citation53,Citation58,Citation69 confidence,Citation39,Citation42,Citation73 having COVID-19 vaccine safety concern,Citation52,Citation65 working in the healthcare field,Citation65 believing vaccines can stop the pandemic,Citation52 relying on Centers for Disease Control and Prevention website for COVID-19 updates,Citation52 fear about COVID-19,Citation68,Citation69 being HCWs,Citation68 close attention to the latest news of the vaccine,Citation43 cues to action,Citation46,Citation70 COVID-19 vaccine hesitancy,Citation71 receiving any vaccine in the past 5 years,Citation71 perception of disease can be prevented by vaccine,Citation44 willingness to protect others by getting oneself vaccinated,Citation61 taking direct care of COVID-19 patients,Citation72 belief that only people who are at risk of serious illness should be vaccinated,Citation58 trust in government,Citation73 complacency,Citation39,Citation42 willingness to pay for and travel for a vaccine,Citation73 themselves or a member of their household belonged to a vulnerable group,Citation56 trust in public health authorities,Citation73 believing COVID-19 virus was not developed in laboratories,Citation56 believing COVID-19 is far more contagious and lethal relative to the H1N1 virus,Citation56 compliance with community mitigation strategies,Citation74 being in a private sector,Citation45 encountering with suspected or confirmed COVID-19 patients,Citation45 self-reported health outcomes,Citation46 believing that next waves COVID-19 are coming,Citation56 knowledge score regarding symptoms, transmission routes and prevention and control measures against COVID-19,Citation56 and perception that COVID-19 will persistCitation57 were factors associated with the willingness of receiving COVID-19 vaccine.
This might be due to that behavioral factors have a critical influence on the newly developed things, particularly like that of vaccines. Perception or attitude towards COVID-19 vaccine might be due to lack of sufficient knowledge or awareness concerning to this vaccine. In fact, the information has a strong effect on the awareness of individuals because it would clarify the misunderstandings that make people confused. Besides, people might consider the personal protection behaviours as a substitute of vaccination in the prevention of COVID-19. They may believe commitment to these precautions is adequate for the prevention of this pandemic.Citation78 This evidence suggests that the community should be aware that personal protection behaviour could not be a substitute for vaccination to prevent COVID-19 infection. This might be because of the misinformation dissemination within the community. Furthermore, a pandemic is a community experience putting a substantial effect on all citizens and demanding a cooperative response.Citation79 However, vaccine hesitancy leftovers a barrier to community vaccination against extremely infectious diseases.Citation80 It is a key impending problem for this pandemic.Citation81 It remains insidious and multifactorial even in individuals of COVID-19 survivors, since most recovered patients revealed to be refusing or uncertain regarding SARS-CoV-2 vaccination.Citation79 COVID-19 vaccine hesitancy is common and can be a barrier to the distribution of vaccines.Citation82 This is because of that the community would be concerned for the safety of the vaccine, since COVID-19 vaccines were rapidly developed globally. This could contribute to vaccine hesitancy.Citation80
The Importance of Understanding the Level of Willingness to Receive COVID-19 Vaccine and Its Associated Factors
The COVID-19 pandemic has significantly harmed the lives of individuals globally. This is by affecting their economic welfare, their health, and changing the behavior of our society extensively. This condition may lead to a strong incentive for individuals to buy a COVID-19 vaccine.Citation83 However, there is controversy about the safety and efficacy of COVID-19 pandemic vaccines, which may contribute to low vaccination rates.Citation84 Besides, even though researchers have been working rapidly and collaboratively for the development of vaccines against this pandemic, the effort of the scientific community in searching a vaccine for COVID-19 may be hindered by a diffused vaccine hesitancy.Citation85 The actual effectiveness of vaccination against COVID-19 might be challenged by vaccine hesitancy.Citation86 The decline of participants’ willingness to vaccinate for COVID-19 may undermine the pandemic response and the public health advantages’ of an effective vaccine.Citation87 Besides, the low vaccination response could make the accomplishment of herd immunity to COVID-19 difficult and unnecessarily extend the pandemic.Citation88
Since HCWs are amongst the first to receive COVID-19 vaccines, their perception or attitude about the safety of these vaccines should be addressed as early as possible.Citation89 Therefore, advanced understanding of young adults’ willingness to take a COVID-19 vaccine and the possible factors affecting their vaccine intention will contribute to the development and implementation of effective methods to encourage COVID-19 vaccine uptake among this group.Citation90 This finding was supported by the study which reported that addressing sociodemographic determinants relating to the COVID-19 vaccination may support to augment the utilization of the worldwide vaccination program to tackle future pandemics.Citation49 Improving the understanding of vaccination hesitancy in the perspective of COVID-19 and finding and using policies to control it, may be as significant as discovering a safe and effective vaccine.Citation91
Besides, in order to improve attitudes towards COVID-19 vaccination, it is very vital to start providing community health education on the COVID-19 vaccine as soon as possible prior to an availability of this vaccine.Citation88 Overall, based on these evidences, targeted health education interventions are required to augment the uptake of the future COVID-19 vaccine.Citation49 In addition to this, by educating the general population about the safety, advantages, and efficacy of vaccines can we hope to prevent the needless delay of the COVID-19 pandemic.Citation88 It is crucial that the public communicate their understanding that the risk of unfavorable results from anything other than rigorous product development likely will reverberate throughout the population and possibly spill into the fear of vaccines. Swiftness is essential for this urgently required vaccine. However, ensuring it is safe is an ethical and humanistic responsibility even if no one in the community is inspecting.Citation92
Finally, in the present systematic review, the level of participants’ willingness towards COVID-19 vaccine and its associated factors throughout different countries have been briefly summarized. This showed that there were some countries that have very low levels of willingness towards COVID-19 vaccine. Furthermore, there were several factors that were found to have an association with the willingness to receive this vaccine (). This suggests that there is a critical problem. This is because if they have unfavorable attitude, perceptions, and hesitancy towards this vaccine, these would have a massive effect on the vaccination rate, particularly if they are HCWs. The study suggested that it is essential to ensure that both the HCWs and the public have access to reliable and sufficient information about vaccines to increase a vaccine acceptance rate.Citation93 This is due to that in fact, if HCWs will not eager to recommend the community to have COVID-19 vaccine, this would have a critical effect on the population’s utilization of this vaccine. Therefore, these could prolong the era of this COVID-19 pandemic. This is supported by the study which stated that future education must be prioritized for HCWs for vaccine acceptance by the population. This is due to that their attitude regarding the vaccines has proved to be a determining factor significant to their own use of the vaccine and their willingness to recommend a vaccine to their patients.Citation94
Conclusion
COVID-19 has been initially reported from China. Then after, rapidly crossed all borders by infecting people of all age groups globally. It is known that this pandemic puts a critical worldwide confrontation with large impacts and several undisclosed events. This pandemic has caused a considerable loss of life and developed into a historic danger to several healthcare systems globally. The crucial element in this initiative is the human behavior to accept a COVID-19 vaccine.
The overall rate of participants’ willingness to receive the COVID-19 vaccine was ranged from 27.7% to 91.3%, which was from Congo and China, respectively. Age, educational status, gender, income, residency, occupation, marital status, race/ethnicity, perceived risk of COVID-19, trust in healthcare system, health insurance, norms, attitude towards vaccine, perceived benefit of vaccine, perceived vaccine barriers, self-efficacy, up-to-date on vaccinations, tested for COVID-19 in the past, responsibility, perceived efficacy of the COVID-19 vaccination, use of social media for COVID-19 vaccine-related information, recommended for vaccination, political leaning, perceived severity of COVID-19, perceived effectiveness of a COVID-19 vaccine, belief that vaccination makes them feel less worried about COVID-19, believing in mandatory COVID-19 vaccination, perceived potential vaccine harms, presence of chronic disease, previously received an influenza vaccine, confidence, having COVID-19 vaccine safety concern, working in the healthcare field, believing vaccines can stop the pandemic, relying on Centers for Disease Control and Prevention website for COVID-19 updates, fear about COVID-19, being HCWs, close attention to the latest news of the vaccine, cues to action, COVID-19 vaccine hesitancy, receiving any vaccine in the past 5 years, perception of disease can be prevented by vaccine, willingness to protect others by getting oneself vaccinated, taking direct care of COVID-19 patients, belief that only people who are at risk of serious illness should be vaccinated, trust in government, complacency, willingness to pay for and travel for a vaccine, themselves or a member of their household belonged to a vulnerable group, trust in public health authorities, believing COVID-19 virus was not developed in laboratories, believing COVID-19 is far more contagious and lethal relative to the H1N1 virus, compliance with community mitigation strategies, being in a private sector, encountering with suspected or confirmed COVID-19 patients, self-reported health outcomes, believing that next waves COVID-19 are coming, knowledge score regarding symptoms, transmission routes and prevention and control measures against COVID-19, and perception that COVID-19 will persist were factors associated with the willingness of receiving COVID-19 vaccine.
The present systematic review has addressed crucial issues for healthcare providers, stakeholders, governments, health policy-makers and implementers, researchers, and for the community as a whole. The significant policy effort may be vital to improve the community willingness to accept a COVID-19 vaccine to have sufficient vaccination rates. It is very significant to start providing health education to the communities on the issue of COVID-19 vaccination as soon as possible in order to improve their willingness towards COVID-19 vaccination. The general public should be aware about the safety, benefits, and efficacy of a vaccine for COVID-19 to prevent the unnecessary prolongation of the COVID-19 pandemic. Lastly, since COVID-19 vaccine is found to be a crucial preventive approach that can halt this pandemic, all barriers that could influence the willingness of receiving COVID-19 vaccine should be urgently addressed by community health strategies.
Abbreviations
COVID-19, coronavirus disease 2019; WHO, World Health Organization; HCWs, healthcare workers; SARS-CoV-2, severe acute respiratory syndrome Coronavirus 2; PRISMA, Preferred Reporting Item for Systematic Review and Meta-Analyses; NOS, Newcastle–Ottawa Scale; HCP, healthcare personnel; CS, cross-sectional; MS, multiple sclerosis; UK, United Kingdom; CRD, chronic respiratory disease; NA, not applicable; LAC, Latin America and the Caribbean.
Data Sharing Statement
The data used to support the findings of this study are on the hands of the corresponding author.
Author Contributions
The author made a significant contribution to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; and agrees to be accountable for all aspects of the work.
Disclosure
The author declares no conflicts of interest for this work.
References
- Dariya B, Nagaraju GP. Understanding novel COVID-19: its impact on organ failure and risk assessment for diabetic and cancer patients. Cytokine Growth Factor Rev. 2020;53:43–52. doi:10.1016/j.cytogfr.2020.05.001
- Lake MA. What we know so far: COVID-19 current clinical knowledge and research. Clin Med. 2020;20(2):124–127. doi:10.7861/clinmed.2019-coron
- Lotfi M, Hamblin MR, Rezaei N. COVID-19: transmission, prevention, and potential therapeutic opportunities. Clin Chim Acta. 2020;508:254–266. doi:10.1016/j.cca.2020.05.044
- Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
- Dey SK, Rahman MM, Siddiqi UR, Howlader A. Analyzing the epidemiological outbreak of COVID-19: a visual exploratory data analysis approach. J Med Virol. 2020;92(6):632–638. doi:10.1002/jmv.25743
- Han Y, Yang H. The transmission and diagnosis of 2019 novel coronavirus infection disease (COVID‐19): a Chinese perspective. J Med Virol. 2020;92(6):639–644. doi:10.1002/jmv.25749
- Jin Y, Yang H, Ji W, et al. Virology, epidemiology, pathogenesis, and control of COVID-19. Viruses. 2020;12(4):372. doi:10.3390/v12040372
- Wang L, Wang Y, Ye D, Liu Q. Review of the 2019 novel coronavirus (SARS-CoV-2) based on current evidence. Int J Antimicrob Agents. 2020;55(6):105948. doi:10.1016/j.ijantimicag.2020.105948
- Cao W, Li T. COVID-19: towards understanding of pathogenesis. Cell Res. 2020;30(5):367–369. doi:10.1038/s41422-020-0327-4
- Sun P, Lu X, Xu C, Sun W, Pan B. Understanding of COVID‐19 based on current evidence. J Med Virol. 2020;92(6):548–551. doi:10.1002/jmv.25722
- Shanafelt T, Ripp J, Trockel M. Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA. 2020;323(21):2133. doi:10.1001/jama.2020.5893
- Lu Q, Shi Y. Coronavirus disease (COVID‐19) and neonate: what neonatologist need to know. J Med Virol. 2020;92(6):564–567. doi:10.1002/jmv.25740
- World Health Organization. Coronavirus disease (COVID-19) dashboard. Available from: https://covid19.who.int. Accessed August 15, 2020.
- Ataguba JE. COVID-19 pandemic, a war to be won: understanding its economic implications for Africa. Appl Health Econ Health Policy. 2020;18(3):325–328. doi:10.1007/s40258-020-00580-x
- Dashraath P, Wong JLJ, Lim MXK, et al. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. Am J Obstet Gynecol. 2020;222(6):521–531. doi:10.1016/j.ajog.2020.03.021
- Yoshikawa H, Wuermli AJ, Britto PR, et al. Effects of the global coronavirus disease-2019 pandemic on early childhood development: short- and long-term risks and mitigating program and policy actions. J Pediatr. 2020;223:188–193. doi:10.1016/j.jpeds.2020.05.020
- Kajdy A, Feduniw S, Ajdacka U, et al. Risk factors for anxiety and depression among pregnant women during the COVID-19 pandemic: a web-based cross-sectional survey. Medicine (Baltimore). 2020;99(30):e21279. doi:10.1097/MD.0000000000021279
- Liang L, Ren H, Cao R, et al. The effect of COVID-19 on youth mental health. Psychiatr Q. 2020;91(3):841–852. doi:10.1007/s11126-020-09744-3
- Deprest J, Choolani M, Chervenak F, et al. Fetal diagnosis and therapy during the COVID-19 pandemic: guidance on behalf of the international fetal medicine and surgery society. Fetal Diagn Ther. 2020:1–10. doi:10.1159/000508254
- Ceulemans M, Hompes T, Foulon V. Mental health status of pregnant and breastfeeding women during the COVID‐19 pandemic: a call for action. Int J Gynecol Obstet. 2020;229(6):ijgo.13295. doi:10.1002/ijgo.13295
- Thapa SB, Mainali A, Schwank SE, Acharya G. Maternal mental health in the time of the COVID‐19 pandemic. Acta Obstet Gynecol Scand. 2020;99(7):817–818. doi:10.1111/aogs.13894
- Fahriani M, Anwar S, Yufika A, et al. Disruption of childhood vaccination during the COVID-19 pandemic in Indonesia. Narra J. 2021;1. doi:10.52225/narraj.v1i1.7
- Chan AKM, Nickson CP, Rudolph JW, Lee A, Joynt GM. Social media for rapid knowledge dissemination: early experience from the COVID −19 pandemic. Anaesthesia. 2020;75(12):1579–1582. doi:10.1111/anae.15057
- Borriello A, Master D, Pellegrini A, Rose JM. Preferences for a COVID-19 vaccine in Australia. Vaccine. 2021;39(3):473–479. doi:10.1016/j.vaccine.2020.12.032
- Lazarus JV, Ratzan SC, Palayew A, et al. A global survey of potential acceptance of a COVID-19 vaccine. Nat Med. 2021;27(2):225–228. doi:10.1038/s41591-020-1124-9
- Hursh SR, Strickland JC, Schwartz LP, Reed DD. Quantifying the impact of public perceptions on vaccine acceptance using behavioral economics. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.608852
- Modesti PA, Reboldi G, Cappuccio FP, et al. Panethnic differences in blood pressure in Europe: a systematic review and meta-analysis. PLoS One. 2016;11(1):e0147601. doi:10.1371/journal.pone.0147601
- Wells GA, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomized studies in meta-analyses, Ottawa Hospital Research Institute, Ottawa, Canada. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed May 21, 2021.
- Shiferaw WS, Akalu TY, Work Y, Aynalem YA. Prevalence of diabetic peripheral neuropathy in Africa: a systematic review and meta-analysis. BMC Endocr Disord. 2020;20(1):49. doi:10.1186/s12902-020-0534-5
- Ehde DM, Roberts MK, Herring TE, Alschuler KN. Willingness to obtain COVID-19 vaccination in adults with multiple sclerosis in the United States. Mult Scler Relat Disord. 2021;49:102788. doi:10.1016/j.msard.2021.102788
- Guidry JPD, Laestadius LI, Vraga EK, et al. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am J Infect Control. 2021;49(2):137–142. doi:10.1016/j.ajic.2020.11.018
- Kuter BJ, Browne S, Momplaisir FM, et al. Perspectives on the receipt of a COVID-19 vaccine: a survey of employees in two large hospitals in Philadelphia. Vaccine. 2021;39(12):1693–1700. doi:10.1016/j.vaccine.2021.02.029
- Malik AA, McFadden SM, Elharake J, Omer SB. Determinants of COVID-19 vaccine acceptance in the US. EClinicalMedicine. 2020;26:100495. doi:10.1016/j.eclinm.2020.100495
- Reiter PL, Pennell ML, Katz ML. Acceptability of a COVID-19 vaccine among adults in the United States: how many people would get vaccinated? Vaccine. 2020;38(42):6500–6507. doi:10.1016/j.vaccine.2020.08.043
- Shaw J, Stewart T, Anderson KB, et al. Assessment of U.S. health care personnel (HCP) attitudes towards COVID-19 vaccination in a large university health care system. Clin Infect Dis. 2021:ciab054. doi:10.1093/cid/ciab054
- Shekhar R, Sheikh AB, Upadhyay S, et al. COVID-19 vaccine acceptance among health care workers in the United States. Vaccines. 2021;9(2):119. doi:10.3390/vaccines9020119
- Unroe KT, Evans R, Weaver L, Rusyniak D, Blackburn J. Willingness of long-term care staff to receive a COVID-19 vaccine: a single state survey. J Am Geriatr Soc. 2021;69(3):593–599. doi:10.1111/jgs.17022
- Fisher KA, Bloomstone SJ, Walder J, Crawford S, Fouayzi H, Mazor KM. Attitudes toward a potential SARS-CoV-2 vaccine: a survey of U.S. adults. Ann Intern Med. 2020;173(12):964–973. doi:10.7326/M20-3569
- Kwok KO, Li -K-K, Wei WI, Tang A, Wong SYS, Lee SS. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: a survey. Int J Nurs Stud. 2021;114:103854. doi:10.1016/j.ijnurstu.2020.103854
- Lin Y, Hu Z, Zhao Q, Alias H, Danaee M, Wong LP. Understanding COVID-19 vaccine demand and hesitancy: a nationwide online survey in China. PLoS Negl Trop Dis. 2020;14(12):e0008961. doi:10.1371/journal.pntd.0008961
- Mo PK, Luo S, Wang S, et al. Intention to receive the COVID-19 vaccination in China: application of the diffusion of innovations theory and the moderating role of openness to experience. Vaccines. 2021;9(2):129. doi:10.3390/vaccines9020129
- Chen M, Li Y, Chen J, et al. An online survey of the attitude and willingness of Chinese adults to receive COVID-19 vaccination. Hum Vaccines Immunother. 2021;17(1–10):2279–2288. doi:10.1080/21645515.2020.1853449
- Gan L, Chen Y, Hu P, et al. Willingness to receive SARS-CoV-2 vaccination and associated factors among Chinese adults: a cross sectional survey. Int J Environ Res Public Health. 2021;18(4):1993. doi:10.3390/ijerph18041993
- Luodan S, Rui M, Zhongzhan W, et al. Perception to COVID-19 epidemic and acceptance of vaccination among healthcare workers in Beijing: a survey before the completion of COVID-19 vaccine Phase III clinical trials. preprint. In Review. 2020. doi:10.21203/rs.3.rs-110888/v1.
- Wang K, Wong ELY, Ho KF, et al. Intention of nurses to accept coronavirus disease 2019 vaccination and change of intention to accept seasonal influenza vaccination during the coronavirus disease 2019 pandemic: a cross-sectional survey. Vaccine. 2020:38. doi:10.1016/j.vaccine.2020.09.021
- Wong MCS, Wong ELY, Huang J, et al. Acceptance of the COVID-19 vaccine based on the health belief model: a population-based survey in Hong Kong. Vaccine. 2021;39(7):1148–1156. doi:10.1016/j.vaccine.2020.12.083
- Wang J, Jing R, Lai X, et al. Acceptance of COVID-19 vaccination during the COVID-19 pandemic in China. Vaccines. 2020;8(3):482. doi:10.3390/vaccines8030482
- Seale H, Heywood AE, Leask J, et al. Examining Australian public perceptions and behaviors towards a future COVID-19 vaccine. BMC Infect Dis. 2021;21(1):21. doi:10.1186/s12879-021-05833-1
- Al-Mohaithef M, Padhi BK. Determinants of COVID-19 vaccine acceptance in Saudi Arabia: a web-based national survey. J Multidiscip Healthc. 2020;13:1657–1663. doi:10.2147/JMDH.S276771
- Alfageeh EI, Alshareef N, Angawi K, Alhazmi F, Chirwa GC. Acceptability of a COVID-19 vaccine among the Saudi population. Vaccines. 2021;9(3):226. doi:10.3390/vaccines9030226
- Al-Mohaithef M, Padhi BK, Ennaceur SA. Demographics of COVID19 vaccine hesitancy during the second wave of COVID-19 pandemic: a cross-sectional web-based survey in Saudi Arabia. medRxiv. 2021;2021.04.20.21255781. doi:10.1101/2021.04.20.21255781
- Barry M, Temsah M-H, Alhuzaimi A, et al. COVID-19 vaccine confidence and hesitancy among healthcare workers: a cross-sectional survey from a MERS-CoV experienced nation. medRxiv. 2020:2020.12.09.20246447. doi:10.1101/2020.12.09.20246447
- Alqudeimat Y, Alenezi D, AlHajri B, et al. Acceptance of a COVID-19 vaccine and its related determinants among the general adult population in Kuwait. Med Princ Pract. 2021. doi:10.1159/000514636
- Bell S, Clarke R, Mounier-Jack S, Walker JL, Paterson P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: a multi-methods study in England. Vaccine. 2020;38(49):7789–7798. doi:10.1016/j.vaccine.2020.10.027
- Nzaji MK, Ngombe LK, Mwamba GN, et al. Acceptability of vaccination against COVID-19 among healthcare workers in the Democratic Republic of the Congo. Pragmatic Obs Res. 2020;11:103–109. doi:10.2147/POR.S271096
- Kourlaba G, Kourkouni E, Maistreli S, et al. Willingness of Greek general population to get a COVID-19 vaccine. Glob Health Res Policy. 2021;6(1). doi:10.1186/s41256-021-00188-1
- Williams L, Gallant AJ, Rasmussen S, et al. Towards intervention development to increase the uptake of COVID-19 vaccination among those at high risk: outlining evidence-based and theoretically informed future intervention content. Br J Health Psychol. 2020;25(4):1039–1054. doi:10.1111/bjhp.12468
- Sherman SM, Smith LE, Sim J, et al. COVID-19 vaccination intention in the UK: results from the COVID-19 vaccination acceptability study (CoVAccS), a nationally representative cross-sectional survey. Hum Vaccines Immunother. 2021;17(6):1612–1621. doi:10.1080/21645515.2020.1846397
- Wong LP, Alias H, Wong P-F, Lee HY, AbuBakar S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum Vaccines Immunother. 2020;16(9):2204–2214. doi:10.1080/21645515.2020.1790279
- Yoda T, Katsuyama H. Willingness to receive COVID-19 vaccination in Japan. Vaccines. 2021;9(1):48. doi:10.3390/vaccines9010048
- Machida M, Nakamura I, Kojima T, et al. Acceptance of a COVID-19 vaccine in Japan during the COVID-19 pandemic. Vaccines. 2021;9(3):210. doi:10.3390/vaccines9030210
- Zigron A, Dror AA, Morozov NG, et al. COVID-19 vaccine acceptance among dental professionals based on employment status during the pandemic. Front Med. 2021;8. doi:10.3389/fmed.2021.618403
- Abedin M, Islam MA, Rahman FN, et al. Willingness to vaccinate against COVID-19 among Bangladeshi adults: understanding the strategies to optimize vaccination coverage. PLoS One. 2021;16(4):e0250495. doi:10.1371/journal.pone.0250495
- Al-Qerem WA, Jarab AS. COVID-19 vaccination acceptance and its associated factors among a middle eastern population. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.632914
- Askarian M, Fu L, Taghrir MH, et al. Factors affecting covid-19 vaccination intent among Iranians: COVID-19 vaccination acceptance. SSRN scholarly paper. Rochester, NY: Social Science Research Network; 2020. Available from: https://papers.ssrn.com/abstract=3741968. Accessed May 8, 2021.
- Barello S, Nania T, Dellafiore F, Graffigna G, Caruso R. ‘Vaccine hesitancy’ among university students in Italy during the COVID-19 pandemic. Eur J Epidemiol. 2020;35(8):781–783. doi:10.1007/s10654-020-00670-z
- Dereje N, Tesfaye A, Tamene B, et al. COVID-19 vaccine hesitancy in Addis Ababa, Ethiopia: a Mixed-Methods Study. medRxiv preprint. Public Glob Health. 2021. doi:10.1101/2021.02.25.21252443
- Detoc M, Bruel S, Frappe P, Tardy B, Botelho-Nevers E, Gagneux-Brunon A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine. 2020;38(45):7002–7006. doi:10.1016/j.vaccine.2020.09.041
- Gagneux-Brunon A, Detoc M, Bruel S, et al. Intention to get vaccinations against COVID-19 in French healthcare workers during the first pandemic wave: a cross-sectional survey. J Hosp Infect. 2021;108:168–173. doi:10.1016/j.jhin.2020.11.020
- Huynh G, Tran TT, Nguyen HTN, Pham LA. COVID-19 vaccination intention among healthcare workers in Vietnam. Asian Pac J Trop Med. 2021;14(4):159. doi:10.4103/1995-7645.312513
- Kanyike AM, Olum R, Kajjimu J, et al. Acceptability of the coronavirus disease-2019 vaccine among medical students in Uganda: a Cross Sectional Study. Trop Med Health. 2021;49(1):1. doi:10.21203/rs.3.rs-425207/v1.
- Malik A, Malik J, Ishaq U. Acceptance of COVID-19 vaccine in Pakistan among health care workers. medRxiv. 2021;2021.02.23.21252271. doi:10.1101/2021.02.23.21252271
- Tobin EA, Okonofua M, Adeke A, Obi A. Willingness to accept a COVID-19 vaccine in Nigeria: a Population-Based Cross-Sectional Study. Cent Afr J Public Health. 2021;7(2):53. doi:10.11648/j.cajph.20210702.12
- Urrunaga-Pastor D, Bendezu-Quispe G, Herrera-Añazco P, et al. Cross-sectional analysis of COVID-19 vaccine intention, perceptions and hesitancy across Latin America and the Caribbean. Travel Med Infect Dis. 2021;41:102059. doi:10.1016/j.tmaid.2021.102059
- Dodd RH, Cvejic E, Bonner C, et al. Willingness to vaccinate against COVID-19 in Australia. Lancet Infect Dis. 2021;21(3):318–319. doi:10.1016/S1473-3099(20)30559-4
- Dong D, Xu RH, Wong EL, et al. Public preference for COVID‐19 vaccines in China: a discrete choice experiment. Health Expect Int J Public Particip Health Care Health Policy. 2020;23:1543–1578. doi:10.1111/hex.13140
- Peretti-Watel P, Seror V, Cortaredona S, et al. A future vaccination campaign against COVID-19 at risk of vaccine hesitancy and politicisation. Lancet Infect Dis. 2020;20(7):769–770. doi:10.1016/S1473-3099(20)30426-6
- Wang K, Wong EL-Y, Ho K-F, et al. Change of willingness to accept COVID-19 vaccine and reasons of vaccine hesitancy of working people at different waves of local epidemic in hong kong, china: repeated cross-sectional surveys. Vaccines. 2021;9(1):62. doi:10.3390/vaccines9010062
- Gerussi V, Peghin M, Palese A, et al. Vaccine hesitancy among Italian patients recovered from COVID-19 infection towards influenza and Sars-Cov-2 vaccination. Vaccines. 2021;9(2):172. doi:10.3390/vaccines9020172
- Dror AA, Eisenbach N, Taiber S, et al. Vaccine hesitancy: the next challenge in the fight against COVID-19. Eur J Epidemiol. 2020;35(8):775–779. doi:10.1007/s10654-020-00671-y
- Taylor S, Landry CA, Paluszek MM, Groenewoud R, Rachor GS, Asmundson GJG. A proactive approach for managing COVID-19: the importance of understanding the motivational roots of vaccination hesitancy for SARS-CoV2. Front Psychol. 2020;11:575950. doi:10.3389/fpsyg.2020.575950
- Longchamps C, Ducarroz S, Crouzet L, et al. COVID-19 vaccine hesitancy among persons living in homeless shelters in France. medRxiv. 2021:2021.04.29.21256256. doi:10.1101/2021.04.29.21256256
- Cerda AA, García LY. Willingness to pay for a COVID-19 vaccine. Appl Health Econ Health Policy. 2021;1–9. doi:10.1007/s40258-021-00644-6
- Alley SJ, Stanton R, Browne M, et al. As the pandemic progresses, how does willingness to vaccinate against COVID-19 evolve? Int J Environ Res Public Health. 2021:18. doi:10.3390/ijerph18020797
- Palamenghi L, Barello S, Boccia S, Graffigna G. Mistrust in biomedical research and vaccine hesitancy: the forefront challenge in the battle against COVID-19 in Italy. Eur J Epidemiol. 2020;35(8):785–788. doi:10.1007/s10654-020-00675-8
- Graffigna G, Palamenghi L, Boccia S, Barello S. Relationship between citizens’ health engagement and intention to take the COVID-19 vaccine in Italy: a mediation analysis. Vaccines. 2020;8(4):576. doi:10.3390/vaccines8040576
- Daly M, Robinson E. Willingness to vaccinate against COVID-19 in the US: longitudinal evidence from a nationally representative sample of adults from April–October 2020. medRxiv. 2020. doi:10.1101/2020.11.27.20239970
- Marcec R, Majta M, Likic R. Will vaccination refusal prolong the war on SARS-CoV-2? Postgrad Med J. 2021;97(1145):143–149. doi:10.1136/postgradmedj-2020-138903
- Verger P, Scronias D, Dauby N, et al. Attitudes of healthcare workers towards COVID-19 vaccination: a survey in France and French-speaking parts of Belgium and Canada, 2020. Eurosurveillance. 2021;26(3):26. doi:10.2807/1560-7917.ES.2021.26.3.2002047
- Qiao S, Tam CC, Li X. Risk exposures, risk perceptions, negative attitudes toward general vaccination, and COVID-19 vaccine acceptance among college students in South Carolina. preprint. Infect Dis. 2020. doi:10.1101/2020.11.26.20239483
- Neumann-Böhme S, Varghese NE, Sabat I, et al. Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19. Eur J Health Econ. 2020;21(7):977–982. doi:10.1007/s10198-020-01208-6
- Kuppalli K, Brett-Major DM, Smith TC. COVID-19 vaccine acceptance: we need to start now. Open Forum Infect Dis. 2021;8(2):ofaa658. doi:10.1093/ofid/ofaa658
- Küçükkarapınar M, Karadağ R, Budakoğlu I, Aslan S, Uçar S, Yay A. COVID-19 vaccine hesitancy and its relationship with illness risk perceptions, affect, worry, and public trust: an online serial cross-sectional survey from Turkey. Psychiatry Clin Psychopharmacol. 2021;31(1):98–109. doi:10.5152/pcp.2021.21017
- Ngoyi JM, Mbuyu LK, Kibwe DN, et al., Covid-19 vaccination acceptance among students of the higher institute of medical techniques of Lubumbashi, Democratic Republic of Congo. Rev L’Infirmier Congo. 2020;4:48–52.
- Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JPA, et al., he PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. 2009;339 jul21 1:b2700–b2700. doi:10.1136/bmj.b2700