
Abstract
Objective
This study aims to evaluate the impact of COVID-19 prevention and control policies on the frequency of emergency department (ED) visits in a large tertiary hospital in central China, from January 2018 to September 2023.
Methods
We conducted a multi-stage interrupted time series analysis to investigate the impact of various epidemic control policies on weekly ED visits at a tertiary hospital in Hunan Province, China. The study period ranged from January 1, 2018, to September 30, 2023, and was divided into four distinct periods: pre-epidemic, pandemic, normalized control, and end of control. Using a quasi-Poisson regression model, we examined the specific effects of these policies on emergency visits, with a particular focus on stratifying patients based on respiratory versus non-respiratory diseases.
Results
Compared to the pre-pandemic period, the number of ED visits in a tertiary hospital decreased by 38.5% (95% CI: 25.1% to 49.8%) during the COVID-19 pandemic, of which the number of ED visits for respiratory diseases increased by 79.4% (95% CI: 13.2% to 177.2%) and the number of ED visits for non-respiratory diseases decreased by 45.9% (95% CI: −55.7% to −34.2%). After the end of the epidemic control, the total number of ED visits increased by 31.5% (95% CI: 19.1% to 45.0%), with the number of ED visits for respiratory diseases rising by 379.2% (95% CI: 275.9% to 511.8%), but with no significant change in the number of ED visits for non-respiratory emergencies.
Conclusion
Control policies were associated with people avoiding emergency care for non-respiratory related reasons during the pandemic, while the end of control policies was associated with a sharp rise in emergency care for respiratory diseases. This study provides a scientific basis for the different changes in ED visits under the implementation of varying epidemic prevention and control policies.
Introduction
In December 2019 and January 2020, an outbreak of pneumonia with unknown causes occurred in Wuhan, China, with evidence of human-to-human transmission.Citation1 The novel coronavirus disease, later known to be coronavirus disease 2019 (COVID-19), quickly spread across Hubei Province and even across China. On Jan 20, 2020, China classified the disease as a second-class infectious disease, which generally warrants less intensive control than first-class diseases. Nevertheless, due to the urgent public health concern, China adopted management measures on par with those for high-risk, first-class infectious diseases.Citation2 Subsequently, unprecedented rigorous public health interventions were implemented, including quarantines, stay-at-home orders, and travel restrictions.Citation3 Until the end of April 2020, China’s response to the COVID-19 epidemic had transitioned into a phase of normalized prevention and control. This phase marked a shift towards a “dynamic zero” approach, emphasizing precise, whole-chain prevention and control measures. This approach aimed to maintain a low level of transmission by quickly identifying and isolating cases, implementing targeted measures in affected areas, and closely monitoring the situation to prevent resurgences.Citation4 After more than two years of implementing normalized prevention and control measures, China announced the termination of COVID-19 policies on December 7, 2022, with the Introduction of the “Ten New Measures”, effectively lifting nearly all restrictions on social mobility across most regions.Citation5
Changes in the epidemic policy have brought challenges to the allocation of medical resources,Citation6 as well as impacts on hospital visits,Citation7 such as several reports of sharp declines in hospital attendance following the COVID-19 outbreak. For example, a national study in the US showed a 42% reduction in emergency department (ED) visits early in the pandemic compared to the same period last year.Citation8 A study in Australia found that the number of ED visits at public hospitals in Queensland during the four-month COVID-19 lockdown was 19.4% lower than predicted by pre-pandemic visit patterns.Citation9 A study in Portugal found a 45.7% reduction in ED visits during the pandemic.Citation10 An interrupted time-series analysis in Ningbo, China, also showed a 45.7% reduction in ED visits during the COVID-19 pandemic.Citation11 Considering the particularity of China’s epidemic prevention policy, there is still a lack of studies that examine the changes in medical resources in the post-epidemic era.
As one of the top medical centers, our hospital is the most sensitive and representative of emergency visits in central South China. Critically, this hospital is located in Changsha, which is the adjacent provincial capital to Wuhan (the first outbreak of COVID-19). Therefore, we analyzed the data of ED visits at this tertiary hospital from January 2018 to September 2023, using the interrupt time series (ITS) method, a powerful quasi-experimental design that uses regression models to assess the longitudinal impact of an intervention.Citation12 The purpose of this study was to evaluate the short- and long-term effects of important changes in epidemic policy on ED visits. This study provides a more comprehensive scientific basis for the rational allocation of hospital medical resources in the post-COVID-19 era.
Materials and Methods
Data Collection
We conducted a multi-stage ITS analysis of emergency information from January 1, 2018, to September 30, 2023, based on the hospital information system (HIS) of the Emergency Department of a tertiary hospital. The HIS recorded basic patient information in emergency departments and observation rooms, including patient identifier, date of visit, and main diagnosis, which were used for the analysis. Patient information from various wards and observation rooms was aggregated and duplicate visits by the same patient within a single day were excluded. The patients were then categorized into 16 groups based on their primary diagnoses, following a classification of common diagnoses. Subsequently, the number of hospital visits was grouped according to the calendar week of each year. This study was approved by the Institutional Review Board of Xiangya Hospital, Central South University (#202002024). Informed consent was not required because anonymized and deidentified information was used in our analysis, and no individual patient information was presented. The study was conducted by the 1964 Helsinki Declaration or comparable standards.
Interventions
The first intervention was the first-level public health emergency response launched by Hunan province on 23 January 2020. The second intervention was the normalized control on April 29, 2020. The third intervention was marked by announcing the end of the epidemic with the release of the “Ten New Measures” on December 7, 2022. T represents the number of weeks since the start of the observation period. Thus, the pre-intervention period was from 1 January 2018 to 22 January 2020 (T=1 to 107), the pandemic period was from January 23, 2020, to September 2020 (T=108 to 121), the normalized control period was from April 29, 2020, to December 6, 2022 (T=121 to 257), and the end control period was from December 7, 2022 to September, 2023 (T=258 to 299).
Outcome Variables
The number of ED visits was the primary outcome. To observe changes in ED visits for respiratory and non-respiratory diseases during the epidemic, a stratified analysis was conducted based on whether patients were primarily diagnosed with respiratory or non-respiratory diseases. All of these outcomes were measured by the total number of ED visits per week.
Statistical Analysis
Owing to the overdispersion of the outcomes, we used a multi-stage ITS quasi-Poisson regression model for analysis. Using the number of weeks as a variable, we assumed that the pandemic would have an immediate impact and that usage would slowly increase over time, so we added level and slope changes to the model. The level change represents the short-term change corresponding to the impact of the epidemic policy, and the slope change represents the long-term change corresponding to the comparison of the weekly trend before and after the policy, the seasonality was considered by Fourier term modeling,Citation13 and the autocorrelation was considered by adding first-order lag residuals. Finally, we used the following segmented regression model:
In the above equation, Yt is the total number of visits or the number of visits by specific factors, β is the intercept term, and β1 represents the trend in the incidence of infectious diseases in the pre-epidemic period. The previous intervention period serves as the reference: β2 is the level change after the epidemic began; β3 was the slope after the epidemic began; β4 was the level change after normalized control; β5 was the slope after normalized control; β6 was the level change after the end of epidemic control; β7 was the slope after the end of epidemic control. Fourier terms were determined by auto Arima models, and ε was determined by the models without residuals. In this study, we used the incidence rate ratio (IRR) and its 95% confidence interval (95% CI) as effect estimates, and the calculation formula was: IRR = exp (βj).
To facilitate interpretation, we discussed the results as a percentage increase or decrease. Diagnostics were performed for each regression model, plotting residuals, autocorrelation, and partial autocorrelation functions. All statistical analyses were performed in R 4.0.2. A P value less than 0.05 was considered statistically significant.
Results
Number of ED Visits Over Time
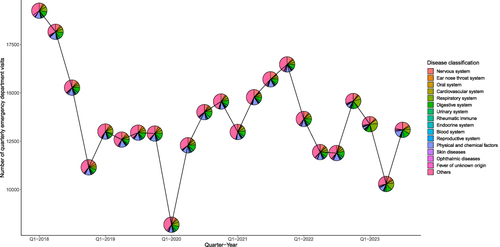
Our study included 313,080 ED visits between January 1, 2018, and September 30, 2023, including 117,745 in the pre-pandemic period (1100 per week), 9117 during the pandemic period (651 per week), 142,260 during the normalization of the epidemic period (1046 per week), and 43,035 at the end of the control period (1025 per week) (). During the pandemic period, the average number of emergency visits per week was the lowest, which can also be observed in the distribution of ED visits by disease type in each quarter, with the lowest number of ED visits in the first quarter of 2020 (). For specific diseases, the proportion of diseases caused by physical or chemical factors was the highest during the pre-pandemic period (12.6%) and normalized control period (11.9%), while the proportion of neurological diseases was the highest (12.1%) during the pandemic period, and the proportion of respiratory diseases was the highest (18.7%) at the end of the epidemic control period.
Table 1 Description of Total and Cause-Specific Emergency Visits During Pre- and Post-Pandemic Periods
Figure 1 Change in the number of emergency visits and the composition of diseases in each quarter from January 2018 to September 2023.
Impact of Policies on ED Visits
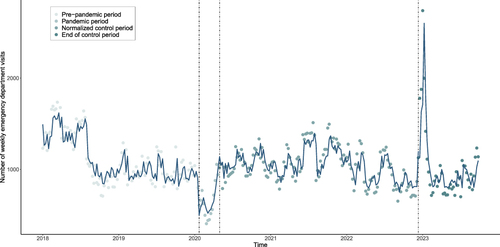
The multi-stage interrupted time series analysis indicated a decreasing trend (−0.5%; 95% CI: −0.6% to −0.4%) in the number of ED visits in the pre-epidemic period (). Compared with the pre-epidemic period, ED visits during the pandemic decreased by 38.5% (95% CI: 25.1% to 49.8%) in the short term, but the slope/trend of ED visits increased by 5.1% (95% CI: 2.8% to 7.6%), indicating both short-term and long-term impacts on ED visits. Upon the implementation of normalized control, the slope/trend of ED visits decreased by 4.5% (95% CI: −6.7% to −2.3%), indicating a long-term impact. After the end of epidemic control, the ED visits increased by 31.5% (95% CI: 19.1% to 45.0%), and its slope/trend showed a decreasing trend (−0.9%; 95% CI: −1.3% to −0.6%), indicating that both short-term and long-term impacts ().
Table 2 Results of Parameter Estimation for the Interrupted Time Series Model of Emergency Department Visits
Figure 2 Trend of the weekly emergency visits for all diseases from January 2018 to September 2023.
Impact of Policies on ED Visits for Respiratory Diseases Vs Non-Respiratory Diseases
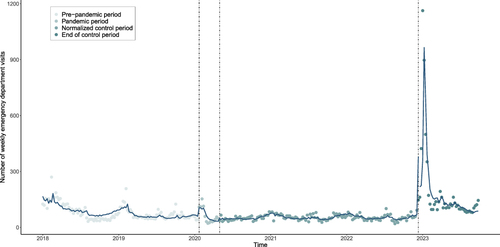
The policy changes significantly impacted the number of ED visits for respiratory diseases (). With the onset of the pandemic, ED visits for respiratory diseases increased by 79.4% (95% CI: 13.2% to 177.2%), indicating a strong short-term impact. Upon the implementation of normalized control measures, the slope/trend of ED visits for respiratory diseases showed a moderate increasing trend (7.3%; 95% CI: 0.7% to 14.8%), indicating a significant long-term impact. After the end of epidemic control, the ED visits for respiratory diseases sharply increased by 379.2% (95% CI: 275.9% to 511.8%) in the short term, and its slope/trend showed a decreasing trend (−2.8%; 95% CI: −3.7% to −1.9%) ().
Figure 3 Trend of weekly emergency visits for respiratory diseases from January 2018 to September 2023.
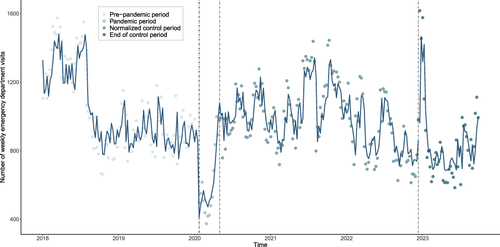
In contrast, the ED visits for non-respiratory diseases during the pandemic experienced a short-term decrease of 45.9% (95% CI: −55.7% to −34.2%) alongside an increasing slope/trend (6.3%; 95% CI: 4.0% to 8.7%) (). Following the implementation of normalized control, the slope/trend of ED visits for non-respiratory diseases demonstrated a gradual downward trend (−5.6%; 95% CI: −7.7% to −3.5%), suggesting the enduring impact of normalization policies on ED visits. It is noteworthy that at the end of the COVID-19 control period, changes in non-respiratory diseases remained relatively stable, with observed changes not achieving statistical significance ().
Figure 4 Trend of weekly emergency visits for non-respiratory diseases from January 2018 to September 2023.
Discussion
In this study of 313,080 ED visits to a tertiary hospital from January 2018 to September 2023, we observed a short-term rapid decline in total ED visits during the pandemic period owing to the strict policy on maintaining social distance, with a decrease in non-respiratory disease but a rapid increase in respiratory disease, indicating that emergency service was occupied by respiratory diseases. After the end of the control, a great increase in ED visits for respiratory diseases, accompanied by unchanged ED visits for non-respiratory diseases, was observed, indicating a severe overload of emergency service provision caused by respiratory diseases in the short term.
COVID-19 poses a serious threat to the lives and health of people around the world, so effective and strict prevention and control policies are crucial to halting the epidemic.Citation14 In the early stages of the epidemic, countries mainly used containment and mitigation strategies.Citation15 Containment focuses on stopping the spread of COVID-19, while mitigation aims to reduce the impact of the pandemic and ease the burden on healthcare resources. Countries have responded to the epidemic with different Interventions according to their circumstances, with the containment strategy represented by China and Italy,Citation16 which adopted strict lockdown measures, while the United States and most European countries adopted mitigation strategies. In the later stage of the epidemic, with the increase in vaccination rates and the development of strain mutations, the risk of serious consequences has been far lower than in the early stages.Citation17 Therefore, most countries, including China, have gradually lifted the epidemic control policies.
Changes in epidemic prevention and control policies have challenged medical resources, with emergency resources as valuable medical resources being significantly affected by policy changes. A study in Italy showed that ED visits during the pandemic decreased by 66.2% compared to the same period the previous year.Citation18 A study on tertiary hospitals in Foshan, China found a significant decrease of 37.75% in emergency department visits in 2020.Citation7 In addition, a hospital study in Ningbo, China also found a 22.6% decrease in total emergency department visits after the implementation of the epidemic prevention and control policies.Citation11 A study in the US found that ED visits decreased by 30.9% to 45% from March to April 2020.Citation19 These studies demonstrate that both containment and mitigation strategies have had an impact on emergency resources during the pandemic, which is also consistent with our findings, but current research mostly focuses on evaluating the impact of single policy changes and lacks analysis that combines multi-stage policy changes. In addition, some studies reported that the policy of normalized control had both short- and long-term restrictive effects on respiratory diseases.Citation20 Therefore, our study considers multi-stage policy changes and combines short - and long-term effects, which to some extent makes the Results different from other studies, but provides more valuable insights into the rational allocation of health care resources.
In the current study, we considered both the short- and long-term effects of different epidemic policies. At the beginning of the pandemic, as a result of delayed healthcare utilization owing to social distance policy and the fear of infection,Citation21 the total of ED visits decreased rapidly in the short term and then increased slowly. During the period of normalized control, the number of visits almost recover to the pre-pandemic level. With the end of control policies in China, the infection rate of COVID-19 has increased rapidly in a short period, bringing a heavy burden to medical staff.Citation22 In the post-epidemic era, with the end of the peak of the first wave of infections, the number of emergency visits has begun to return to relatively normal changes, but with the complete liberalization of policies, we need to be vigilant against the disease burden caused by the re-outbreak of respiratory diseases, rationally allocate medical resources, reduce the burden on medical staff, and improve emergency treatment capacity.
Our study has several limitations. First, although we used Fourier terms for fitting seasonality, there are still some time-varying confounders that may affect hospital visits, such as air pollution and meteorological factors, that were not included in our models. Second, to maintain data integrity, we retained some information about medical visits for which the primary diagnosis could not be clarified, which may have biased the subcomponents. Finally, the observational nature of our study suggests more association than causation between COVID-19 prevention and control policies and ED visits.
In summary, this study offers a scientific foundation for understanding the effects of policy changes on emergency visits during the COVID-19 pandemic through quasi-experimental analysis. It demonstrates that ED visits have shown varying patterns under different epidemic prevention and control policies. In addition, a global burden study reported that COVID-19 has greatly disrupted the referral of patients to emergency medical care, partly related to limited ED resources.Citation23 Therefore, it is crucial to prioritize the advancement of ED infrastructure, enhance epidemic prevention and control systems, and strengthen emergency response capabilities. This will ensure effective readiness to tackle future unknown epidemic challenges.
Disclosure
The authors report no conflicts of interest in this work.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Additional information
Funding
References
- Li Q, Guan X, Wu P, et al. Early transmission dynamics in Wuhan, china, of novel coronavirus–infected pneumonia. N Engl J Med. 2020;382(13):1199–1207. doi:10.1056/NEJMoa2001316
- Xiao Y, Torok ME. Taking the right measures to control COVID-19. Lancet Infect Dis. 2020;20(5):523–524. doi:10.1016/S1473-3099(20)30152-3
- Parmet WE, Sinha MS. Covid-19 - The law and limits of quarantine. N Engl J Med. 2020;382(15):e28. doi:10.1056/NEJMp2004211
- Liang WN, Liu M, Liu J, et al. The dynamic COVID-zero strategy on prevention and control of COVID-19 in China. Zhonghua Yi Xue Za Zhi. 2022;102(4):239–242. doi:10.3760/cma.j.cn112137-20211205-02710
- Lan D, Ren W, Ni K, et al. Topic and trend analysis of weibo discussions about covid-19 medications before and after china’s exit from the zero-COVID Policy: retrospective infoveillance study. J Med Internet Res. 2023;25: e48789. doi:10.2196/48789.
- Emanuel EJ, Persad G, Upshur R, et al. Fair allocation of scarce medical resources in the time of covid-19. N Engl J Med. 2020;382(21):2049–2055. doi:10.1056/NEJMsb2005114
- Shen B, Chen B, Li K, et al. The impact of COVID-19 pandemic lockdown on emergency department visits in a tertiary hospital. Risk Manag Healthc Policy. 2023;16:1309–1316. doi:10.2147/RMHP.S415704
- Hartnett KP, Kite-Powell A, Devies J, et al. Impact of the COVID-19 pandemic on emergency department visits — United States, January 1, 2019–May 30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(23):699–704. doi:10.15585/mmwr.mm6923e1
- Sweeny AL, Keijzers G, Marshall A, et al. Emergency department presentations during the Covid‐19 pandemic in Queensland (to June 2021): interrupted time series analysis. Med J Aust. 2023;218(3):120–125. doi:10.5694/mja2.51819
- Lopes S, Soares P, Santos Sousa J, et al. Effect of the COVID‐19 pandemic on the frequency of emergency department visits in Portugal: an interrupted time series analysis until July 2021. J Am Coll Emerg Physicians Open. 2023;4(1):E12864. doi:10.1002/emp2.12864
- ming YZ, Yin WM, Ming LJ, et al. Effect of COVID-19 on hospital visits in Ningbo, China: an interrupted time-series analysis. Int J Qual Health Care. 2021;33(2):mzab078. doi:10.1093/intqhc/mzab078
- Kontopantelis E, Doran T, Springate DA, et al. Regression based quasi-experimental approach when randomisation is not an option: interrupted time series analysis. BMJ. 2015;350:h2750. doi:10.1136/bmj.h2750.
- Bhaskaran K, Gasparrini A, Hajat S, et al. Time series regression studies in environmental epidemiology. Int J Epidemiol. 2013;42(4):1187–1195. doi:10.1093/ije/dyt092
- Nouvellet P, Bhatia S, Cori A, et al. Reduction in mobility and COVID-19 transmission. Nat Commun. 2021;12(1):1090. doi:10.1038/s41467-021-21358-2
- Walensky RP, Del Rio C. From mitigation to containment of the COVID-19 pandemic: putting the SARS-CoV-2 genie back in the bottle. JAMA. 2020;323(19):1889. doi:10.1001/jama.2020.6572
- Wang X, Shi L, Zhang Y, et al. Policy disparities in fighting COVID-19 among Japan, Italy, Singapore and China. Int J Equity Health. 2021;20:33. doi:10.1186/s12939-020-01374-2
- Nyberg T, Ferguson NM, Nash SG, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet Lond Engl. 2022;399(10332):1303–1312. doi:10.1016/S0140-6736(22)00462-7
- Santi L, Golinelli D, Tampieri A, et al. Non-COVID-19 patients in times of pandemic: emergency department visits, hospitalizations and cause-specific mortality in Northern Italy. PLoS One. 2021;16(3):e0248995. doi:10.1371/journal.pone.0248995
- Boserup B, McKenney M, Elkbuli A. The impact of the COVID-19 pandemic on emergency department visits and patient safety in the United States. Am J Emerg Med. 2020;38(9):1732–1736. doi:10.1016/j.ajem.2020.06.007
- Shi T, Zhang X, Meng L, et al. Immediate and long-term changes in infectious diseases in China at the “first-level-response”, “normalized-control” and “Dynamic-COVID-zero” stages from 2020 to 2022: a multistage interrupted-time-series-analysis. BMC Public Health. 2023;23(1):1381. doi:10.1186/s12889-023-16318-y
- Lazzerini M, Barbi E, Apicella A, et al. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc Health. 2020;4(5):e10–e11. doi:10.1016/S2352-4642(20)30108-5
- Cheng Z, Tao Y, Liu T, et al. Psychology, stress, insomnia, and resilience of medical staff in china during the covid-19 policy opening: a cross-sectional survey. Front Public Health. 2023;11:1249255. doi:10.3389/fpubh.2023.1249255
- Mogharab V, Ostovar M, Ruszkowski J, et al. Global burden of the Covid-19 associated patient-related delay in emergency healthcare: a panel of systematic review and meta-analyses. Glob Health. 2022;18(1):58. doi:10.1186/s12992-022-00836-2