
Abstract
Purpose
This study aims to identify medical care transformations during the COVID-19 pandemic and to assess the economic efficiency of these care transformations.
Methods
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviewing and Meta-Analysis (PRISMA) guidelines. The databases used in the search protocol included PubMed, RSCI, and Google Scholar.
Results
Ten eligible studies in English and one publication in Russian were identified. In general, the following changes in organization of health care processes since 2020 are observed: hospital at home, telemedicine (physician-to-patient), and the adoption of new information communication technologies within physician-to-physician and physician-to-nurse communication. Earlier trends, such as (a) wider use of electronic devices, (b) adoption of Lean techniques, (c) the incorporation of patient and other customer experience feedback, and (d) the implementation of clinical decision support systems and automation of workflow, tend to be preserved.
Conclusion
The most common changes in hospital care organization and the respective impacts of workflow changes (ie, workflow interventions, redesign, and transformations) on the efficiency of hospital care were summarized and avenues for future research and policy implications were discussed. The pandemic demonstrated a need for building more resilient and adaptive healthcare systems, enhancing crisis preparedness along with rapid and effective responses.
Introduction
Motivation
According to a recent news report,
inefficient clinical workflows in healthcare result in considerable waste. […] A hospital doctor typically wastes around 45 minutes every day as a result of inefficient communication systems.Citation1
In hospitals, examples of these inefficiencies include the duplication of tasks and poor communication among physicians. Such bottleneck inefficiencies have particularly striking effects on patient survival in severe infectious diseases due to their acute clinical course and immediate need for accurate diagnostics and treatment.Citation2 Health facilities, which manage to optimize their workflows through interventions, increase their return on investment due to the more efficient work of physicians and nurses and improved patient experience. Improvements of patient workflow can be made through, for example, automation, such as having patients use check-in kiosks and/or appointment scheduling and reminders. Other key areas of automation include patient record management, billing and claims processing, prescription management, lab test processing, and hospital inventory management.Citation3 In general, major strategies for enhancing hospital processes include establishing a real-time communication system, streamlining documentation processes, and tracking patient flow in real-time.Citation4 Inputs to hospital efficiency, such as environmental setting and access to drinking water,Citation5 while being assumed across the industrialized Northern Hemisphere remain a core challenge in an array of low and middle-income countries of the Global South.Citation6 Certain redesigns were specifically caused by epidemics. For example, during the H1N1 pandemic, hospital care transformations included segregating H1N1 patients, restricting visitors, using personal protective equipment, and modifying prophylactic protocols to mitigate viral transmission risks.Citation7 Fresh air, sunlight, hygiene standards, and reusable masks at open-air hospitals reduced deaths and infections, suggesting the importance of such measures in hospital care redesign.Citation8 However, there is limited evidence on economic efficiency of these transformations, especially in the context of the most recent pandemic.
Research Questions
This study aims to address the following research questions. First: How did medical care transform during the COVID-19 pandemic and which transformations were most common? Second: What was the economic efficiency of these care transformations?
Defining Key Terms
This review covers the following key concepts. The first concept is ‘healthcare processes’, defined as
the activities that constitute healthcare – including diagnosis, treatment, rehabilitation, prevention, and patient education – usually carried out by professional personnel, but also including other contributions to care, particularly by patients and their families
(Donabedian, 2003, p. 46).Citation9 In our context, a concept of “care process management” (CPM), which is the use of business process automation and optimization techniques in clinical care in the healthcare environment, is also relevant. CPM helps the subjects of healthcare to change delivery processes. The second concept is “process redesign” (or “process reengineering”), defined as “any methodology that focuses on creating new processes or changing existing ones in major ways”.Citation10 The purpose of process reengineering consists in improving overall work efficiency through optimizing the process(es) via equipment renewal, material substitution, step simplification, time sequence adjustment, etc. In this review, process redesign is closely related to the concepts of “workflow intervention” and “workflow improvement”. In organization of medical care, this can include, but is not limited to changes in the functions (actions, activities) performed by the subjects (actors, participants) of medical care: doctors, paramedical personnel, other categories of employees of medical organizations; changes in the methods (mechanisms, rules) and intensity of interaction of medical care subjects with each other (doctors with paramedical staff and other workers; general practitioners and narrow specialists, outpatient doctors and hospitals, etc.); changes in the way and frequency of interaction between patients and medical professionals; changes in information flows in the healthcare system. Following the Cochrane-EPOC classification for organizational interventions,Citation11 interventions were categorized into two groups. First, “changes in structure” include
changes in physical structure, facilities and equipment; changes in the setting/site of service delivery; cooperation with external services or communication and case discussion with offsite health professionals; integration of services; staff organization; clinical multidisciplinary teams; and revision of professional roles / skill mix changes.
Second changes in processes and process management” refer to “changes in process sequences and organization of processes; changes in capacity planning; and presence and organization of quality-monitoring mechanisms.
All other categories represent a combination of the above-mentioned interventions.
Last, but not least, the “economic efficiency” of hospitals is considered as a situation in which nothing can be improved without someone or something else being hurt. Farrell (1957) defined efficiency as
the firm’s success to produce the maximum feasible amount of output from a given amount of input or producing a given amount of output using the minimum level of inputs where both the inputs and the outputs are correctly measured’.Citation12
One of the following two concepts is typically used: (1) “allocative” (or “Pareto efficiency”) and (2) “productive efficiency”. Allocative efficiency assumes that any changes made to assist one person cannot be made without harming another. Productive efficiency refers to a situation, in which
no additional output of one good can be obtained without decreasing the output of another good, and production proceeds at the lowest possible average total cost.Citation13
The following methods are typically used to measure hospital efficiency: Data Envelopment Analysis (DEA), Stochastic Frontier Analysis (SFA), and measures of performance, such as Pabon Lasso’s model. DEA is a non-parametric linear programming method used to evaluate the efficiency of decision-making units.Citation9,Citation10,Citation14 SFA is a parametric method, which calculates the difference between the organization’s predicted and actual outputs.Citation15 Pabon Lasso’s model (1986) assesses hospital performance using three indicators: bed occupancy ratio, bed turnover ratio, and average length of stay.Citation16 These and similar methods to assess hospitals’ ability to deliver desired outputs, such as hospital admission episodes, number of prevented mortality cases, and outpatient examinations are widely explored in health economics.Citation17,Citation18
Overview of the Relevant Reviews
General reviews consider redesign strategies and approaches at hospital or industry level within current trends, such as process automation, digitalization, and implementation of computerized clinical decision support systems (CDSS). Elkhuizen et al reviewed the literature on business process redesign in hospital care.Citation19 Wang et al outlined the avenues of clinical information extraction applications.Citation20 Shahid et al reviewed applications of artificial neural networks (ANN) in decision-making of healthcare entities.Citation21 They identified key characteristics and drivers for ANN market uptake to guide their further use in health care. Janssen et al found that the most frequently reported workflow intervention categories referred to anesthetic management, in-hospital patient transfer management, and prehospital management.Citation22 In their empirical study on improving emergency departments, Pereira et al reviewed previous studies on the application of redesigned heuristics in healthcare.Citation23 Zayas-Cabán et al synthesized current approaches of workflow automation across industries and prospects of applying workflow automation in healthcare.Citation24 Eljiz et al provided a scoping review of the empirical studies on the large-scale redevelopment of healthcare facilities as a strategy for the transformation of care systems.Citation25 Hung et al analyzed three distinct transformational performance improvement approaches, which are commonly used to redesign work processes in medical organizations.Citation26 Ozkaynak et al introduced relevant theories, principles, and techniques to guide analysis of clinical workflows, methods and processes for workflows improvements, and organizational interventions aimed at workflow redesign.Citation27
The second group of studies focus on the quality of care and effectiveness associated with the reviewed organizational changes. Van Leijen-Zeelenberg et al reviewed the impact of care processes redesign on care quality. Their results suggest that process redesign interventions have positive effects on several quality aspects.Citation28 Buljac-Samardzic et al reviewed interventions that improve team's effectiveness in health care. The following types of interventions were distinguished: (a) “training” (eg, crew resource management, simulation, or general team training); (b) “tools” that “structure, facilitate (through communication technology), or trigger (through monitoring and feedback) teamwork”; (c) “organizational (re)design” is about (re)designing structures to stimulate team processes and team functioning; and (d) “programme”, which represents a combination of the previous types.Citation29 Blakeney et al provided a scoping review of new implementations of interprofessional bedside rounding models aimed at improving teamwork, care, and outcomes in hospitals. Their findings suggest that the majority of the reviewed studies reported positive impacts of IBR implementation across an array of team, patient, and care quality/delivery outcomes.Citation30 Chowdhury et al analyzed the effect of prehospital workflow optimization on treatment delays and clinical outcomes in acute ischemic stroke. The results of their systematic review and meta-analysis found that prehospital stroke workflow optimizations significantly improved several time metrics related to stroke treatment leading to improvement in intravenous thrombolysis reperfusion rates.Citation31 Dupuis et al reviewed several effective strategies aimed at reducing waiting times in outpatient rehabilitation services for adults with physical disabilities.Citation32
The last group of articles assessed the monetary effects of workflow changes. Evans et al reviewed the empirical studies on how hospitals capture financial benefits of process improvement and the impact of examined redesigns on hospital financial performance.Citation33 Von Schudnat et al analyzed the economic impact of standardization and digitalization in operating rooms. Only selected standardization methods and introduced digital support systems for intraoperative surgical workflows effectively increased efficiency while maintaining or even improving quality.Citation34
Thus, despite having the same or very similar object of the study, these reviews focused on the general or specific issues related to workflow redesigns and their efficiency without considering the impact of the COVID-19 pandemic.
Method
Following the PRISMA reporting guidelines (Page et al),Citation35 a systematic review was conducted to identify and classify all the literature that is related to our research questions. The databases used in the study included PubMed, RSCI, and Google Scholar. In the search, the following key terms and/or MeSH terms were used: for example, {“redesign” OR “re-engineering” OR “transformation” OR “workflow intervention” OR “process improvement” OR “workflow optimisation”} AND {“care”} AND {“hospital” OR “health facility” OR “medical organization”} AND {“efficiency” OR “effectiveness” OR “efficacy”} AND {“regression” OR “correlation”}. Our search was focused on articles in English and Russian, published between January 2020 and June 2023. For RSCI, Russian synonyms of the key terms were added to account for the nuances of Russian terminology.
Inclusion and Exclusion Criteria
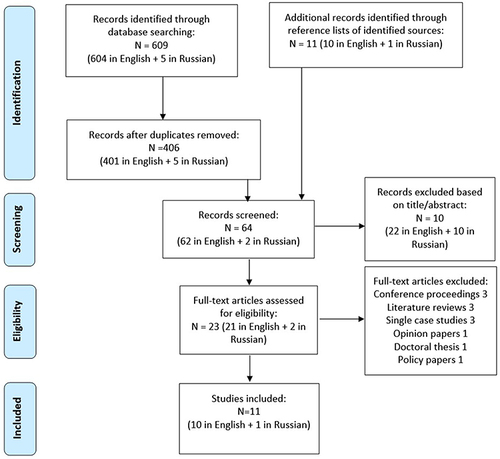
Publications were included, if they included empirical data; they were peer reviewed; they had extractable data related to hospital or medical care; and they represented “research article” or “original research” type. Publications of the following types were excluded: expert opinion, single-case study, conceptual theoretical study, editorial, commentary, qualitative study, study protocol. Quantitative studies based on either patients’, physicians’, or nurses’ perceptions via survey data, and any studies based on data collected before 2020, were also excluded. The PRISMA diagram demonstrates the details of our search for eligible studies (see ). Similarly to Elkhuizen et al, process changes could be supported by the introduction or redesign of IT solutions, and there may be organizational restructuring needed for implementing improved process designs.Citation19
Figure 1 Flow diagram of systematic review.
Typology of Study Designs
Similar to Shojania and Grimshaw (2005), study designs were assessed according to the following classification: randomized controlled trial, non-randomized control group design, interrupted time series design, controlled before-after design, and before-after design.Citation36
Screening and Quality Appraisal
Retrieved publications were reviewed independently by two researchers (TZ and YT) according to the criteria outlined above, and initial disagreements on the suitability of individual studies were resolved with a third expert (MJ). Reference lists of eligible publications were screened for any further potentially relevant sources.
Results
The initial search yielded 609 publications after the removal of duplicates. See for details. The selected articles were screened by title and subsequently screened on their abstract or full text. A total of N = 11 studies were selected for review based on the inclusion and exclusion criteria listed above: five from the US; two from China; and one each from Australia, Germany, Spain, and Russia. summarizes the articles, which were included in the analysis. The majority of eligible studies (8 out of 11 articles; 73%) used before-after design. The remaining three studies employed interventional study with a control group.
Table 1 Summary of Empirical Research on Hospital Care Redesign and Transformation
The Most Common Transformations of Care
Three out of 11 studies (27%), including Rock et alCitation45 Horn et alCitation46 and Chen et alCitation47 considered changes in facilities and equipment. Another three studies (27%), namely, Laurie et alCitation39 LeupoldCitation40 and ParodiCitation43 described changes in the setting/site of service delivery. One study (9%) by Lindsay and Lytle (2022) documented changes in process sequences and organization of processes.Citation41 One study (9%) by Song et al (2020) referred to changes in the physical structure of the care environment.Citation44 And, one study by Kulikova and Moskvina (2022) documented changes in staff organization.Citation37 Two other categories represent a combination of the above-mentioned interventions, such as changes in physical structure, changes in facilities and equipment, revision of professional roles/skill mix changes, integration of services.Citation38,Citation42
Economic Efficiency of Care Transformations
In this section, the diverse effects of the reviewed workflow redesigns and transformations are summarized. The studies are grouped by country, starting with the US.
Lindsay and Lytle (2022) report on a successful workflow redesign, which decreased documentation time, redundancy, and click burden for nurses.Citation41 Specifically, a few segments of nursing documentation were optimized, including the number of visible rows on access to and duplication of information noted elsewhere in the electronic health record (EHR). This redesign resulted in 18.5% decrease time in the EHR; decrease of 7% to 12% of total time in flowsheets; time savings of 1.5 to 6.5 minutes per reassessment per patient; and a decrease of 88% to 97% in number of steps to perform reassessment documentation, ie there is clear evidence of productivity improvement, since time savings could be reallocated to value-added patient care activities.Citation41 Larsen et al report on workflow improvements in their additive manufacturing lab consisted in the re-design and implementation of the internal project scorecard to standardize evaluation of requests, and the distribution of the responsibility of submission evaluation across lab members. As a result, the time to review new submissions was reduced from an average of 58 days to 4 days, allowing the Lab Manager to devote more time to engineering rather than administrative/decision-making tasks.Citation42 Parodi et al assessed the impact on readmission rates for CMS (Centers for Medicare and Medicaid Services) core measures (CCM) patients and patients receiving care under the Bundled Payment for Care Improvement (BPCI) Advanced Model resulting from implementing pharmacist-led transitions of care. Pharmacist-driven transitions of care were associated with significant reductions in 30-day CCM and 90-day BPCI hospital readmissions.Citation43
Rock et al aimed to reduce unnecessary Clostridioides difficile testing implemented computerized clinical decision support (CCDS) systems (hard stop or soft stop) in the EHR. As a result, in nine hospitals implementing hard-stop CCDS and four hospitals implementing soft-stop CCDS, C. Difficile testing incidence rate (IR) reduction was 33% and 23%, respectively. CCDS systems reduced unnecessary C. Difficile testing and were perceived positively by healthcare professionals when integrated into their workflow and when displaying relevant patient-specific information needed for decision making.Citation45 Horn et al implemented a pediatric essential clinical dataset (ECD) tool that positively affected nursing documentation time, dataset completion rate, and satisfaction. In particular, nursing admission history documentation time decreased by 91 seconds and the number of clicks decreased by 38%.Citation46
The next group refers to the studies originating in Europe. In their study on digital redesign of hypertension management in Germany, Leupold et al report that the analyzed intervention increased the blood pressure control rate significantly by 23.1% points, while systolic blood pressure decreased by 21.1 mmHg in the intervention group compared to 15.5 mmHg in their control group.Citation40 Bernabeu-Wittel et al conclude that a coordinated on-site medical program of Spanish nursing homes with COVID-19 outbreaks achieved a higher survival (97% versus 77% before the program) and optimal palliative care rate (84% versus 73% before the program), and a reduction in referrals to hospital (17% versus 29% before the program), thus ensuring rigorous but humanistic and gentle care to residents.Citation38 Kulikova and Moskvina (2022) studied the work of ambulance services in Russian regions before and after the COVID-19 pandemic and found that in regions of the Central Federal District, where the ambulance service was represented by a single legal entity during the pandemic, excess mortality was lower in comparison with those in the regions where the ambulance service was represented by departments within hospitals. This means a single legal entity has advantages in terms of the quality of healthcare services and the efficiency of the use of financial resources of the institution.Citation37
The last group provides the results from Asia and Oceania. According to Song et al, who studied the effect of optimization of the intravenous infusion workflow in isolation wards for patients with COVID-19 in China. The optimization of this workflow included five main steps: establishing the process improvement team, identifying the process steps to be improved, re-optimising the process, implementing the optimized process, and evaluating the new process. It effectively decreased the cost of personal protective equipment and improved the efficiency of infusion and patients’ satisfaction. In particular, after the infusion workflow was optimized, average times for preparation drugs and intravenous admixture, and patients’ waiting time decreased from 4.84 minutes, 4.03 minutes, and 34.33 minutes to 3.50 minutes, 2.60 minutes, and 30.87 minutes, respectively. Patients’ satisfaction increased from 66.7% to 93.3%, and the number and cost of personal protective equipment decreased from 46.67 sets and 186.6 CNY per day to 36.17 sets and 144.6 CNY, respectively.Citation44 Chen et al conducted a study in China as well, aimed to shorten door-to-needle time via multidisciplinary and workflow optimization in prehospital, in-hospital, and feedback stages. The major implemented changes were a hospital notification system via the establishment of a secure web communication platform, and monthly training to stroke and emergency nurses. The authors report that after the implementation of these changes the median (interquartile range) door-to-needle time decreased significantly from 57.0 (45.3–77.8) to 37.0 (29.0–49.0) minutes. They conclude that the multidisciplinary collaboration and continuous process optimization can result in overall shortened door-to-needle time despite the challenges incurred by the COVID-19 pandemic.Citation47 Findings by Laurie et al suggest that the analyzed pragmatic service redesign in Australia, which included the implementation of a digital model of care, demonstrates reassuring clinical outcomes in a culturally diverse gestational diabetes mellitus (GDM) cohort. The novel model of care included, for example, (a) initial midwife phone call informing the patient of the diagnosis; (b) delivery via email of a link to a GDM education video and registration for the use of a specialized app; (c) a Bluetooth capable blood glucose meter couriered to the patient’s home address; and (d) a scheduled face-to-face appointment with the dietitian.Citation39
Discussion
It seems beneficial to compare our findings with the results of recent studies published after 2019, and based on pre-pandemic data from Australia, Canada, China, the Netherlands, Singapore, Spain, the UK, and the US. For example, Janssen et al assessed the effect of 20 relevant workflow improvement strategies aimed at minimizing the time between onset of ischemic stroke and start of endovascular thrombectomy in the Netherlands.Citation53 Lai et al compared patients admitted under the integrated general hospital model and patients receiving usual care in public hospitals in Singapore.Citation54 Luu et al assessed the impact of using an EHR-based messaging system for nonemergent communication between nurses and physicians in US emergency departments.Citation55 Nether et al assessed implementation of a robust process improvement training program by the hospital neonatal intensive care units in the US.Citation56 Swedlund et al examined a primary care redesign process aimed at reducing refill requests made outside of office visits in the US.Citation57 Hung et al examined the impact of Lean redesign implementation, such as the standardization of exam room equipment and supplies, the streamlining of call management processes, care team co-location, and team management of the electronic inbox, on the amount of time taken for physicians to complete routine clinical tasks in the US.Citation58 Subbe et al explored the usage of participatory engagement in patient-created and co-designed medical records for emergency admission to the British hospital.Citation59 Bhayana et al created an electronic list of computed tomography (CT) requests that radiology residents would monitor to optimize after-hours workflow of CT orders.Citation60 Brooks et al assessed a novel payor-focused strategy to efficiently navigate the prior authorization process while eliminating physician burden and reducing inappropriate denials.Citation61 Chalwin et al examined the impact of re-design of an existing rapid response system in an Australian metropolitan hospital, including the addition of: (a) regular rapid response team (RRT) meetings (b) RRT role badges, and (c) a structured member-to-user patient care responsibility “hand-off” process.Citation62 Nguyen et al examined recommended cancer screening rates associated with a US primary care transformation initiative that established team-based care.Citation63 Mueller et al assessed the initiative to improve advanced notification of inter-hospital transfers in the US. During implementation of the interventions, an advance notification page was sent to the admitting clinicians to minimize inefficiencies caused by poor communication during the transfer of patients between hospitals.Citation64 Deng et al provided calculations on location optimization for emergency medical service (EMS) facilities in a Chinese megapolis, Chengdu, aiming to optimize the time required for emergency care physicians to reach patients by adding a minimum number of EMS facilities to achieve a given population coverage.Citation65 Sather et al identified significant improvements in timeliness outcomes driven by application of scripted quality improvement interventions, which included clinical practice guideline dissemination, interhospital transfer (IHT) process redesign, and improvement related to electronic patient arrival notification, electronic imaging exchange, and EHR. The application of scripted quality improvement interventions as part of the IHT process was feasible and effective at improving the timeliness of care and communication of critical information in patients with nontraumatic intracerebral and subarachnoid hemorrhage in the US.Citation66 Esteban et al, who studied the application of the telemonitoring system in Spain, reported no differences between the intervention group with telemonitoring and the control group (with standard care) in terms of cost-effectiveness, however the intervention program was less expensive than routine clinical practice.Citation67 In line with the reviewed care transformations, these redesign initiatives were typically associated with increased efficiency and/or workflow improvements.
In low resource settings, four unique health systems adaptations/interventions for restoring, maintaining, and ensuring continuity of care for people living with non-communicable diseases during COVID-19 were identified: telemedicine and teleconsultation strategies, the decentralization of hypertension follow-up services, diabetic retinopathy screening with a handheld smartphone-based retinal camera, and non-communicable diseases medicine drop-off points. The first three redesigns were associated with positive effects.Citation68
Policy Implications and Conclusions
In the observed period, apart from the essential changes in health expenditure and policy,Citation69 a lot of novel workflow redesigns occurred, which predictably included pandemic-related changes in the physical structures of hospital environments. Other improvements mostly referred to the changes in facilities or equipment, such as implementing a new clinical decision support system, telemonitoring or electronic notification system. The later changes basically are driven by the current trends in and challenges for medical care.Citation70 Similar to earlier redesigns, each of the examined workflow transformations was associated with improved workflow efficiency and/or improved patient satisfaction. In the long-term, further improvements can potentially be based on hospital workflow optimization via either the more extensive implementation of best practices in workflow innovations or through less known instruments, such as, for example, k-means clustering.Citation71 In addition, policy-makers should ideally consider the roots of healthcare system inefficienciesCitation72 to build more resilient and adaptive systems, enhancing crisis preparedness along with rapid and effective responses.Citation73,Citation74
The COVID-19 pandemic had a significant impact on healthcare systems worldwide, highlighting the need for increased patient and family engagement, enhanced use of health information technologies, a strengthened safety culture, and more reliable medical organizations. Key elements of an improved global pandemic response framework include: (a) data-driven decision making, leveraging robust global disease surveillance and data-sharing; (b) strengthened global public health infrastructure and technology systems; (c) strengthened social protection, equity, and inclusiveness; (d) enhanced international cooperation and the coordination of policies, resources, and response measures; and (e) ongoing public health education and preparedness efforts at the global level.Citation73,Citation74 Summing up, pandemic management in a globalized world requires an internationally coordinated public health approach to effectively detect, respond to, and mitigate future pandemics.
The major potential biases of the reviewed studies referred to relatively small sample size,Citation39,Citation41,Citation43,Citation44,Citation46,Citation47 retrospectiveCitation38,Citation42,Citation47 or remoteCitation42,Citation45 data collection, pre-post differences in the baseline characteristics for each sample,Citation43,Citation46 and the voluntary recruitment of participants.Citation45 As for additional drawbacks of the examined studies, it is important to note that the absolute majority of the studies (8 out of 11) use a before-and-after design. The findings of before-and-after studies should be treated with caution as they do not have respective control groups by definition.Citation50 In other words, the results might be different in the contexts of other samples. In some cases, the level of econometrics is low, for example, the use of Pearson correlation in Kulikova and Moskvina,Citation37 which means it is hard to make conclusions in terms of causality. Second, only the frequencies of redesign measures are observed in the selected papers, but there is no information about which, if any, of the redesign measures are used in practice in different regions and with what frequency. This is an important avenue for future research. Third, most research concerns only staff costs (wasted time, etc), not changes in mortality rates. It is hard to discuss efficiency ignoring the effect of staff costs on the decrease in mortality. Future research should explore this effect. Patient satisfaction, widely used in the examined studies, is a weak criterion for improving the effectiveness of hospital care; it should be supplemented by data on mortality, diagnostic and treatment errors, side effects, and repeated visits. Although there are many avenues for future research, policy implications can be drawn from the results of this review. Firstly, healthcare systems will be more efficient and responsive to potential future epidemics, if hospitals implement relevant changes in their physical structure, such as separating potentially infected patients. Secondly, healthcare facilities will benefit from having high-speed Internet connections to ensure the effective performance of telemedicine. Thirdly, hospital care will benefit from multidisciplinary collaboration and continuous process optimization.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception (YT), study design (YT), execution (YT and TZ), acquisition of data (YT and TZ), analysis and interpretation (MJ, YT and TZ), or in all these areas; took part in drafting (YT and TZ), revising or critically reviewing the article (MJ, YT, and TZ); gave final approval of the version to be published (MJ, YT, and TZ); have agreed on the journal to which the article has been submitted (MJ, YT, and TZ); and agree to be accountable for all aspects of the work (MJ, YT, and TZ).
Disclosure
The authors report no conflicts of interest related to this study.
Additional information
Funding
References
- Optimizing clinical workflows in healthcare. HIPAA J; Available from: https://www.hipaajournal.com/optimizing-clinical-workflows-in-healthcare/. Accessed May 27, 2024.
- Local Burden of Disease HIV Collaborators. Mapping subnational HIV mortality in six Latin American countries with incomplete vital registration systems. BMC Med. 2021;19:1–25. doi:10.1186/s12916-020-01876-4
- Arkenea. Guide to healthcare workflow automation; Available from: https://arkenea.com/blog/guide-to-healthcare-workflow-automation. Accessed May 27, 2024
- Sharepowered. Workflow optimization: 4 strategies to enhance hospital processes. 2020; Available from: https://sharepowered.com/workflow-optimization-4-strategies-to-enhance-hospital-processes.html. Accessed May 27, 2024
- Deshpande A, Miller-Petrie MK, Lindstedt PA, et al. Mapping geographical inequalities in access to drinking water and sanitation facilities in low-income and middle-income countries, 2000–17. Lancet Glob Health. 2020;8(9):e1162–85. doi:10.1016/S2214-109X(20)30278-3
- Jakovljevic M, Timofeyev Y, Ekkert NV, et al. The impact of health expenditures on public health in BRICS nations. J Sport Health Sci. 2019;8(6):516–519. doi:10.1016/j.jshs.2019.09.002
- Patel M, Dennis A, Flutter C, Thornton S, D’mello O, Sherwood N. Pandemic (H1N1) 2009 influenza: experience from the critical care unit. Anaesthesia. 2009;64(11):1241–1245. doi:10.1111/j.1365-2044.2009.06128.x
- Hobday RA, Cason JW. The open-air treatment of pandemic influenza. Am J Public Health. 2009;99(S2):S236–42. doi:10.2105/AJPH.2008.134627
- Donabedian A. An Introduction to Quality Assurance in Health Care. Oxford University Press; 2002.
- Harmon P. Business Process Change: A Manager’s Guide to Improving, Redesigning, and Automating Processes. Morgan Kaufmann; 2003.
- The Data Collection Checklist. Effective Practice and Organisation of Care Collaborative Review Group. 2002; Available from: http://www.epoc.uottawa.ca/checklist2002.doc. Accessed May 27, 2024.
- Farrell MJ. The measurement of productive efficiency. J R Stat Soc. 1957;120(3):253–281. doi:10.2307/2343100
- Different Types of Efficiencies; Available from: https://Courses.lumenlearning.com/Suny-Oldwestbury-Publicfinanceandpublicpolicy/Chapter/Different-Types-of-Efficiencies/. Accessed May 27, 2024
- Jakovljevic MB, Vukovic M, Fontanesi J. Life expectancy and health expenditure evolution in Eastern Europe—DiD and DEA analysis. Expert Rev Pharm Out. 2016;16(4):537–546. doi:10.1586/14737167.2016.1125293
- Aigner D, Lovell CK, Schmidt P. Formulation and estimation of stochastic frontier production function models. J Econom. 1977;6(1):21–37. doi:10.1016/0304-4076(77)90052-5
- Pabon Lasso H. Evaluating hospital performance through simultaneous application of several indicators. Bul Pan Am Health Org. 1986;20(4):341–357.
- Micah AE, Cogswell IE, Meretoja A, Meretoja TJ. Tracking development assistance for health and for COVID-19: a review of development assistance, government, out-of-pocket, and other private spending on health for 204 countries and territories, 1990-2050. Lancet. 2021;398:1317–1343. doi:10.1016/S0140-6736(21)01258-7
- Tyrovolas S, Kassebaum NJ, Stergachis A, et al. The burden of disease in Greece, health loss, risk factors, and health financing, 2000–16: an analysis of the Global Burden of Disease Study 2016. Lancet Public Health. 2018;3(8):e395–406. doi:10.1016/S2468-2667(18)30130-0
- Elkhuizen SG, Limburg M, Bakker PJ, Klazinga NS. Evidence‐based re‐engineering: re‐engineering the evidence: a systematic review of the literature on business process redesign (BPR) in hospital care. Int J Health Care Qual Assur. 2006;19(6):477–499. doi:10.1108/09526860610686980
- Wang Y, Wang L, Rastegar-Mojarad M, et al. Clinical information extraction applications: a literature review. J Biomed Inform. 2018;77:34–49. doi:10.1016/j.jbi.2017.11.011
- Shahid N, Rappon T, Berta W, Uthman O. Applications of artificial neural networks in health care organizational decision-making: a scoping review. PLoS One. 2019;14(2):e0212356. doi:10.1016/j.jbi.2017.11.011
- Janssen PM, Venema E, Dippel DW. Effect of workflow improvements in endovascular stroke treatment: a systematic review and meta-analysis. Stroke. 2019;50(3):665–674. doi:10.1161/STROKEAHA.118.021633
- Pereira R, Lapão LV, Bianchi IS, Amaral D. Improving emergency department through business process redesign. Australas J Inf Syst. 2020. doi:10.3127/ajis.v24i0.2679
- Zayas-Cabán T, Haque SN, Kemper N. Identifying opportunities for workflow automation in health care: lessons learned from other industries. Appl Clin Inform. 2021;12(03):686–697. doi:10.1055/s-0041-1731744
- Eljiz K, Greenfield D, Vrklevski L, Derrett A, Ryan D. Large scale healthcare facility redevelopment: a scoping review. Int J Health Plann Manag. 2022;37(2):691–714. doi:10.1002/hpm.3378
- Hung DY, Lee J, Rundall TG. Transformational Performance Improvement: why Is Progress so Slow? In: Responding to the Grand Challenges in Health Care via Organizational Innovation: Needed Advances in Management Research. 2022. Emerald Publishing Limited:23–46
- Ozkaynak M, Unertl K, Johnson S, Brixey J, Haque SN. Clinical workflow analysis, process redesign, and quality improvement. In: Clinical Informatics Study Guide: Text and Review. 2022. Cham: Springer International Publishing; 103–118. doi:10.1007/978-3-030-93765-2_8
- van Leijen-Zeelenberg JE, Elissen AM, Grube K, et al. The impact of redesigning care processes on quality of care: a systematic review. BMC Health Serv Res. 2015;16:1–24. doi:10.1186/s12913-016-1266-0
- Buljac-Samardzic M, Doekhie KD, van Wijngaarden JD. Interventions to improve team effectiveness within health care: a systematic review of the past decade. Hum Resour Health. 2020;18(1):1–42. doi:10.1186/s12960-019-0411-3
- Blakeney EA, Chu F, White AA, et al. A scoping review of new implementations of interprofessional bedside rounding models to improve teamwork, care, and outcomes in hospitals. J Interprof Care. 2021;1–16. doi:10.1080/13561820.2021.1980379
- Chowdhury SZ, Baskar PS, Bhaskar S, Panagos P. Effect of prehospital workflow optimization on treatment delays and clinical outcomes in acute ischemic stroke: a systematic review and meta‐analysis. Acad Emerg Med. 2021;28(7):781–801. doi:10.1111/acem.14204
- Dupuis F, Dery J, de Oliveira FC L, et al. Strategies to reduce waiting times in outpatient rehabilitation services for adults with physical disabilities: a systematic literature review. J Health Serv Res Policy. 2022;27(2):157–167. doi:10.1177/13558196211065707
- Evans J, Leggat SG, Samson D. A systematic review of the evidence of how hospitals capture financial benefits of process improvement and the impact on hospital financial performance. BMC Health Serv Res. 2023;23(1):1–13. doi:10.1186/s12913-023-09258-1
- von Schudnat C, Schoeneberg KP, Albors-Garrigos J, Lahmann B, De-Miguel-Molina M. The economic impact of standardization and digitalization in the operating room: A systematic literature review. J Med Syst. 2023;47(1):55. doi:10.1007/s10916-023-01945-0
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021;88:105906. doi:10.1016/j.ijsu.2021.105906
- Shojania KG, Grimshaw JM. Evidence-based quality improvement: the state of the science. Health Aff. 2005;24(1):138–150. doi:10.1377/hlthaff.24.1.138
- Kulikova IB, Moskvina SS. Transformation of the ambulance service during the COVID-19 pandemic: correlation and thematic analysis. Russ Med. 2022;28(3):193–199. doi:10.17816/medjrf108938
- Bernabeu-Wittel M, Ternero-Vega JE, Nieto-Martín MD, et al. Effectiveness of a on-site medicalization program for nursing homes with COVID-19 outbreaks. J Gerontol. 2021;76(3):e19–27. doi:10.1093/gerona/glaa192
- Laurie JG, Wilkinson SA, Griffin A, McIntyre HD. GDM care re-imagined: maternal and neonatal outcomes following a major model of care change for gestational diabetes mellitus at a large metropolitan hospital. Aust N Z J Obstet Gynaecol. 2023;63:681–688. doi:10.1111/ajo.13691
- Leupold F, Karimzadeh A, Breitkreuz T, et al. Digital redesign of hypertension management with practice and patient apps for blood pressure control (PIA study): a cluster-randomised controlled trial in general practices. EClinicalMedicine. 2023;55. doi:10.1016/j.eclinm.2022.101712
- Lindsay MR, Lytle K. Implementing best practices to redesign workflow and optimize nursing documentation in the electronic health record. Appl Clin Inform. 2022;13(03):711–719. doi:10.1055/a-1868-6431
- Larsen EP, Silvestro E, Ferro DF, et al. Using human factors principles to redesign a 3D lab workflow during the COVID-19 pandemic. 3D Print Med. 2022;8(1):1–10. doi:10.1186/s41205-022-00161-9
- Parodi M, Feeley B, Sanchez M. Impact of a pharmacist-driven transitions of care clinic for a multisite integrated delivery network. Am J Health-Syst Pharm. 2022;79(11):844–851. doi:10.1093/ajhp/zxac029
- Song Y, Wang W, Zhang L, Sha L, Lu G. Optimization of the intravenous infusion workflow in the isolation ward for patients with coronavirus disease 2019. Int J Nurs. 2020;7(2):148–152. doi:10.1016/j.ijnss.2020.03.009
- Rock C, Abosi O, Bleasdale S, et al. Clinical decision support systems to reduce unnecessary Clostridioides difficile testing across multiple hospitals. Clin Infect Dis. 2022;75(7):1187–1193. doi:10.1093/cid/ciac074
- Horn JJ, Doucette JN, Sweeney NL. An essential clinical dataset intervention for nursing documentation of a pediatric admission history database. J Pediatr Nurs. 2021;59:110–114. doi:10.1016/j.pedn.2021.03.022
- Chen Y, Nguyen TN, Wellington J, et al. Shortening door-to-needle time by multidisciplinary collaboration and workflow optimization during the COVID-19 pandemic. J Stroke Cerebrovasc Dis. 2022;31(1):106179. doi:10.1016/j.jstrokecerebrovasdis.2021.106179
- CFF. Interventional versus observational studies: what’s the difference?; Available from: https://www.cff.org/research-clinical-trials/interventional-versus-observational-studies-whats-difference. Accessed May 27, 2024
- Healthknowledge. Introduction to study designs – intervention studies and randomised controlled trials; Available from: https://www.healthknowledge.org.uk/e-learning/epidemiology/practitioners/introduction-study-design-is-rct. Accessed May 27, 2024
- Examine. Before-and-after study; Available from: https://examine.com/glossary/before-and-after-study/. Accessed May 27, 2024
- Berner ES. Clinical Decision Support Systems. New York: Springer; 2007.
- Matricardi PM, Potapova E, Forchert L, Dramburg S, Tripodi S. Digital allergology: towards a clinical decision support system for allergen immunotherapy. Pediatr Allergy Immunol. 2020;31:61–64. doi:10.1111/pai.13165
- Janssen PM, Roozenbeek B, Coutinho JM, et al. MR CLEAN Registry Investigators. Effect of workflow improvements on time to endovascular thrombectomy for acute ischemic stroke in the MR CLEAN Registry. Stroke: Vasc Interv Neurol. 2023;e000733. doi:10.1161/SVIN.122.000733
- Lai YF, Lee SQ, Tan YR, et al. One-bed-one-team—does an integrated general hospital inpatient model improve care outcomes and productivity: an observational study. Front Public Health. 2022;10:779910. doi:10.3389/fpubh.2022.779910
- Luu T, Spiegelman L, Nykin D, et al. Implementation of an electronic health record–based messaging system in the emergency department: effects on physician workflow and resident burnout. J Patient Saf. 2022;18(2):e542–e546. doi:10.1097/PTS.0000000000000869
- Nether KG, Thomas EJ, Khan A, Ottosen MJ, Yager L. Implementing a robust process improvement program in the neonatal intensive care unit to reduce harm. J Healthc Qual. 2022;44(1):23. doi:10.1097/JHQ.0000000000000310
- Swedlund M, Kamnetz S, Birstler J, et al. Reduction in medication refill encounters through primary care redesign workflow changes. J Ambul Care Manag. 2022;45(1):36–41. doi:10.1097/jac.0000000000000398
- Hung DY, Truong QA, Liang SY. Implementing lean quality improvement in primary care: impact on efficiency in performing common clinical tasks. J Gen Intern Med. 2021;36:274–279. doi:10.1007/s11606-020-06317-9
- Subbe CP, Tomos H, Jones GM, Barach P. Express check-in: developing a personal health record for patients admitted to hospital with medical emergencies: a mixed-method feasibility study. Int J Qual Health Care. 2021;33(3):mzab121. doi:10.1093/intqhc/mzab121
- Bhayana R, Wang CD, Menezes RJ, Bartlett ES, Choi J. Optimising after-hours workflow of computed tomography orders in the emergency department. BMJ Open Qual. 2020;9(3):e000969. doi:10.1136/bmjoq-2020-000969
- Brooks ED, Ning MS, Palmer MB, Gunn GB, Frank SJ, Shah AK. Strategic operational redesign for successfully navigating prior authorization barriers at a large-volume proton therapy center. JCO Oncol Pract. 2020;16(10):e1067–77. doi:10.1200/jop.19.00533
- Chalwin R, Giles L, Salter A, Kapitola K, Karnon J. Re-designing a rapid response system: effect on staff experiences and perceptions of rapid response team calls. BMC Health Serv Res. 2020;20:1–9. doi:10.1186/s12913-020-05260-z
- Nguyen KH, Chien AT, Meyers DJ, Li Z, Singer SJ, Rosenthal MB. Team-based primary care practice transformation initiative and changes in patient experience and recommended cancer screening rates. Inquiry. 2020;57:0046958020952911. doi:10.1177/0046958020952911
- Mueller S, Murray M, Schnipper J, Goralnick E. An initiative to improve advanced notification of inter-hospital transfers. In Healthcare. 2020;8(2):100423. doi:10.1016/j.hjdsi.2020.100423
- Deng Y, Zhang Y, Pan J. Optimization for locating emergency medical service facilities: a case study for health planning from China. Risk Manag Healthc Policy. 2021;1791–1802. doi:10.2147/RMHP.S304475
- Sather J, Littauer R, Finn E, et al. A multimodal intervention to improve the quality and safety of interhospital care transitions for nontraumatic intracerebral and subarachnoid hemorrhage. Jt Comm J Qual Patient Saf. 2021;47(2):99–106. doi:10.1016/j.jcjq.2020.10.003
- Esteban C, Antón A, Moraza J, et al. telEPOC group. Cost-effectiveness of a telemonitoring program (telEPOC program) in frequently admitted chronic obstructive pulmonary disease patients. J Telemed Telecare. 2021. doi:10.1177/1357633X211037207
- Baatiema L, Sanuade OA, Allen LN, et al. Health system adaptions to improve care for people living with non-communicable diseases during COVID-19 in low-middle income countries: a scoping review. J Glob Health. 2023;13:06006. doi:10.7189/iogh.13.06006
- Jin H, Li B, Jakovljevic M. How China controls the Covid-19 epidemic through public health expenditure and policy? J Med Econ. 2022;25(1):437–449. doi:10.1080/13696998.2022.2054202
- Timofeyev Y, Kaneva M, Jakovljevic M. Current questions and challenges in healthcare of the post-socialist countries. Front Public Health. 2023;11. doi:10.3389/fpubh.2023.1254898
- Spini G, van Heesch M, Veugen T, Chatterjea S. Private hospital workflow optimization via secure k-means clustering. J Med Syst. 2020;44. doi:10.1007/s10916-019-1473-4
- Jakovljevic M, Sugahara T, Timofeyev Y, Rancic N. Predictors of (in) efficiencies of healthcare expenditure among the leading Asian economies–comparison of OECD and non-OECD nations. Risk Manag Healthc Policy. 2020;Volume 13:2261–2280. doi:10.2147/RMHP.S266386
- Khorram-Manesh A, Goniewicz K, Burkle FM Jr. Unleashing the global potential of public health: a framework for future pandemic response. J Infect Public Health. 2024;17:82–95. doi:10.1016/j.jiph.2023.10.038
- Goniewicz K, Khorram-Manesh A, Burkle FM, Hertelendy AJ, Goniewicz M. The European Union’s post-pandemic strategies for public health, economic recovery, and social resilience. Global Transitions. 2023;5:201–209. doi:10.1016/j.glt.2023.10.003